Embed Size (px)
Citation preview

U
s
Fate of Patients With Prehospital Resuscitation for ST-ElevationMyocardial Infarction and a High Rate of Early ReperfusionTherapy (Results from the PREMIR [Prehospital Myocardial
Infarction Registry])
Oliver Koeth, MDa, Lutz Nibbe, MDb, Hans-Richard Arntz, MDc, Burkhard Dirks, MDd,Klaus Ellinger, MDe, Harald Genzwürker, MDf, Ulrich Tebbe, MDg, Steffen Schneider, PhDh,
Jörg Friedrich, MDi, Ralf Zahn, MDi, and Uwe Zeymer, MDh,i,*; for the PREMIR Investigators
Patients with acute ST-segment elevation myocardial infarction (STEMI) needing prehos-pital cardiopulmonary resuscitation (CPR) have a very high adverse-event rate. However,little is known about the fate of these patients and predictors of mortality in the era of earlyreperfusion therapy. From March 2003 through December 2004, 2,317 patients withprehospital diagnosed STEMI were enrolled in the Prehospital Myocardial InfarctionRegistry. One hundred ninety patients (8.2%) underwent prehospital CPR and wereincluded in our analysis. Overall 90% of patients were treated with early reperfusiontherapy, 56.3% received prehospital thrombolysis and 1/2 of these patients received earlypercutaneous coronary intervention after thrombolysis, 28.4% of patients were treated withprimary percutaneous coronary intervention, and 5.3% received in-hospital thrombolysis.Total mortality was 40.0%. The highest mortality was seen in patients with asystole (63%)or pulseless electric activity (64%). Independent predictors of mortality were need forendotracheal intubation and older age, whereas ventricular fibrillation as initial heartrhythm was associated with survival. In conclusion, in this large registry with prehospitaldiagnosed STEMI, incidence of prehospital CPR was about 8%. Even with a very high rateof early reperfusion therapy, in-hospital mortality was high. Especially in elderly patientswith asystole as initial heart rhythm and with need for endotracheal intubation, prognosisis poor despite aggressive reperfusion therapy. © 2012 Elsevier Inc. All rights reserved.
(Am J Cardiol 2012;109:1733–1737)Acute myocardial infarction is one of the main reasonsfor out-of-hospital cardiac arrest and need for prehospitalresuscitation.1 Patients with acute ST-segment elevationmyocardial infarction (STEMI) and prehospital cardiopul-monary resuscitation (CPR) represent a selected subgroupwith a very high adverse-event rate. Predictors of mortalityin these patients are of great interest to optimize prehospitaland hospital sequences. In patients with STEMI withoutCPR, primary percutaneous coronary intervention (PCI) andfibrinolysis are most effective within the first golden hourafter onset of symptoms.2,3 Therefore, especially patients atvery high risk, namely patients with STEMI and prehos-
aKlinikum Worms, Worms, Germany; Campuses bVirchow and cBen-jamin Franklin, Charite Berlin, Berlin, Germany; dUniversitätsklinikum
lm, Ulm, Germany; eKlinikum Ravensburg, Ravensburg, Germany; fKre-iskrankenhaus Buchen, Buchen, Germany; gKlinikum Lippe-Detmold,Lippe-Detmold, Germany; hInstitut für Herzinfarktforschung Ludwig-hafen an der Universität, Heidelberg, Germany; iKlinikum Ludwigshafen,
Ludwigshafen, Germany. Manuscript received December 9, 2011; revisedmanuscript received and accepted February 5, 2012.
The registry was supported by unrestricted funding from BoehringerIngelheim, Ingelheim, Germany. Dr. Zeymer, Dr. Arntz, Dr. Nibbe, andDr. Ellinger were or are members of the speakers bureau of BoehringerIngelheim.
*Corresponding author: Tel: 49-621-503-2941; fax: 49-621-503-4002.
E-mail address: [email protected] (U. Zeymer).0002-9149/12/$ – see front matter © 2012 Elsevier Inc. All rights reserved.doi:10.1016/j.amjcard.2012.02.013
pital CPR, may benefit from an early and aggressivereperfusion strategy.1,4,5 Therefore, we analyzed the Pre-hospital Myocardial Infarction Registry (PREMIR),which included patients with STEMI diagnosed in theprehospital phase and evaluated the subgroup of patientswith need for prehospital CPR.
Methods
The PREMIR was a collaboration of the Arbeitsgemein-schaft Leitende Kardiologische Krankenhausärzte and theBundesverband der Arbeitsgemeinschaft der NotärzteDeutschlands. The design of the registry is reported in moredetail elsewhere.6,7 In brief, consecutive patients were in-cluded who presented with typical chest pain or equivalentsymptoms �20 minutes within 24 hours after symptomonset, prehospital 12-lead electrocardiogram with STE in�2 contiguous leads (�2 mm precordial leads, �1 mmlimb leads) or left bundle branch block (LBBB) and pre-hospital diagnosis, and treatment by an emergency physi-cian. The present analysis includes consecutive patientswith STEMI and prehospital resuscitation. Data on patients’characteristics were recorded, including age, gender, car-diovascular risk factors, concomitant diseases, previous MI,previous stroke, and previous cardiovascular interventionsand data on onset of symptoms, time to call, time to arrival
of ambulance, prehospital delay, and time to start of reper-www.ajconline.org

/188)
1734 The American Journal of Cardiology (www.ajconline.org)
fusion therapy. Major cardiovascular and cerebrovascularadverse events until hospital discharge were also recorded.Those data were analyzed and processed centrally in theInstitut für Herzinfarktforschung, Ludwigshafen. Sourcedata verification was performed by comparison of the reg-istry data to ambulance and hospital records in randomlyselected 230 patients in randomly selected participatingcenters. Ambulance protocols of all patients with STEMIand prehospital CPR also were reviewed by 3 independentinvestigators. Initial heart rhythm, electrocardiograms, du-ration of cardiac massage, number of defibrillations, use ofcatecholamines, and need for endotracheal intubation wereevaluated in those patients. The registry was approved bythe ethical committee of the Landesärztekammer Mainz.STEMI was diagnosed in the presence of the 3 followingcriteria: persistent angina pectoris for �20 minutes, elec-trocardiographic criteria described earlier or presence ofLBBB, and increases of cardiac markers creatine ki-nase-MB or troponins. Reinfarction was diagnosed in caseof recurrent angina pectoris with re-elevation of creatinekinase-MB or angiographic demonstration of occlusion ofthe infarct vessel. Stroke was defined as the occurrence ofpersistent specific neurologic deficits. Major bleeding wasdefined as any intracranial bleeding, bleeding associatedwith need for blood transfusion, or any other clinicallyrelevant bleeding with need for intervention as judged bythe investigator. Data are presented as absolute numbers,percentages, or medians with 25th and 75th percentiles asappropriate. Categorical values were compared by chi-square test and continuous variables were compared by2-tailed Wilcoxon rank-sum test. A p value �0.05 wasconsidered statistically significant. For identifying indepen-dent predictors of mortality, logistic regression analysis wasperformed using forward parameter selection. All statisticalanalyses were performed using SAS 9.1 (SAS Institute,
Table 1Baseline characteristics
Baseline Characteristics Patients With STPrehospit
(n � 1
DemographicsAge (years) 64.0 (53Men 74.2% (14Body weight (kg) 83.0 (75Height (cm) 175 (17
Medical historyPrevious myocardial infarction 14.5% (27Previous percutaneous coronary intervention 7.0% (13Previous coronary artery bypass grafting 5.4% (10
Coronary risk factorsHypercholesterolemia 24.7% (46Smoker 31.7% (59Hypertension 53.8% (10Diabetes mellitus 18.8% (35
Prehospital findingsAnterior myocardial infarction 54.3% (10Posterior myocardial infarction 37.8% (71Left bundle branch block 8.5% (16
Cary, North Carolina).
Results
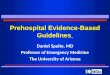
From March 2003 through December 2004, 2,317 pa-tients with prehospital diagnosed STEMI were enrolled inthe PREMIR. One hundred ninety patients (8.2%) neededprehospital CPR. Baseline characteristics and prehospitalfindings of patients with and without CPR are listed in Table1. Patients with STEMI and prehospital resuscitation wereyounger and more often had an anterior MI or LBBB com-pared to patients with STEMI without prehospital resusci-tation. Table 2 presents adjunctive prehospital medications.Patients with STEMI and prehospital CPR received aspirinless often. Median intervals are listed in Table 3. Intervalsfrom symptom onset to emergency call and from symptomonset to 12-lead electrocardiography were shorter in pa-tients with STEMI and prehospital CPR. Main reasons forCPR in patients with STEMI were ventricular fibrillationand asystole. Initial therapies applied in the prehospitalphase are listed in Table 4. Planned primary PCI and oralanticoagulation were the main reasons for withholding pre-hospital fibrinolysis. Figure 1 depicts initial prehospital andhospital reperfusion strategies and prehospital and hospitalmortalities according to different reperfusion therapies in
ceiving Patients With STEMI Not ReceivingPrehospital CPR
p Value
(n � 2,127)
66.0 (55–75) �0.0570.0% (1,489/2,127) 0.22
80.0 (70–90) �0.001172 (165–178) �0.01
19.4% (410/2,113) 0.110.0% (211/2,113) 0.194.2% (89/2,113) 0.45
36.1% (762/2,113) �0.0139.0% (824/2,113) 0.0560.6% (1,281/2,113) 0.0722.9% (484/2,113) 0.2
44.9% (940/2,093) �0.0551.3% (1,073/2,093) �0.0014.3% (90/2,093) �0.01
Table 2Antithrombotic treatment in prehospital phase
Patients WithSTEMI
ReceivingPrehospital CPR
Patients WithSTEMI NotReceiving
Prehospital CPR
p Value
(n � 190) (n � 2,127)
Aspirin 81.2% (151/186) 90.5% (1,924/2,125) �0.0001Clopidogrel 0.6% (1/178) 2.1% (42/2,045) 0.17Heparin 82.7% (153/185) 84.9% (1,796/2,116) 0.43Glycoprotein IIb/IIIa
inhibitors4.0% (7/176) 3.2% (65/2,040) 0.57
EMI Real CPR90)
–72)1/190)–90)0–180)
/186)/186)/186)
/186)/186)0/186)/186)
2/188)/188)
patients with STEMI and prehospital CPR. Overall rate of

taIp
eactc
carg
c
0–51.0)
1735Coronary Artery Disease/Prehospital CPR in STEMI
reperfusion therapy in patients with STEMI and CPR was90%. Prehospital mortality did not differ between patientswith STEMI receiving prehospital fibrinolysis and patientsnot receiving prehospital fibrinolysis (5.6% vs 4.8%, p �0.81). Overall mortality in patients with STEMI and pre-hospital resuscitation was 37.1% (66 of 178), reinfarctionoccurred in 8.5% (15 of 176), stroke in 2.3% (4 of 175), andmajor bleeding in 3.4% (6 of 175). Figure 2 shows hospitalmortality according to initial heart rhythm. To identify pre-dictors for mortality, a stepwise multivariate analysis wasperformed. Need for endotracheal intubation (odds ratio[OR] 16.8, 95% confidence interval [CI] 2.2 to 131.4) andolder age per year (OR 1.037, 95% CI 1.006 to 1.069) wereindependent predictors for mortality. Ventricular fibrillation(OR 0.313, 95% CI 0.128 to 0.766) as initial heart rhythmwas associated with survival, whereas mode of reperfusiontherapy had no significant impact on prognosis.
Discussion
This is 1 of the largest reports of consecutive patientswith STEMI and prehospital CPR. Incidence of prehospitalresuscitation in patients with STEMI diagnosed in the pre-hospital phase was about 8% in our study. Only a fewspecific data in patients with STEMI and prehospital CPRare currently available.1,4,5,8 These reports have revealedhat 10% to 21% of patients with STEMI need defibrillationnd CPR.9–11 An analysis of the American Nationwidenpatient Sample database has shown that the mean age of
Table 3Median time intervals
Patients With STPrehospi
(n �
Symptom onset to call 14.0 (4.0Symptom onset to 12-lead electrocardiography 45 (30.Call to arrival of ambulance on scene 8.0 (6.0Electrocardiography until admission to hospital 35.0 (20.
Table 4Reasons for resuscitation and acute therapy
Patients With STEMI ReceivingPrehospital CPR
(n � 190)
Reasons for resuscitationAsystole 10.3% (18/175)Pulseless electromechanical activity 7.4% (13/175)Ventricular fibrillation 80.0% (140/175)Ventricular tachycardia 2.9% (5/175)
Acute therapyDefibrillation 87.9% (167/190)Median number of defibrillations 3 (2–6)Chest compression 85.6% (160/187)Duration of cardiac massage (min) 20 (15–40)Intubation 86.1% (161/187)Catecholamines 78.6% (147/187)
atients with STEMI is 66 years.12 In our analysis patients b
with STEMI needing prehospital CPR were younger (64 vs66 years) and more often had anterior MI or LBBB com-pared to patients with STEMI without prehospital CPR.Intervals from symptom onset to emergency call and fromsymptom onset to 12-lead electrocardiography were shorterin patients with STEMI and prehospital resuscitation. Meandelay from symptom onset to 12-lead electrocardiographyin patients with STEMI and prehospital CPR was about 45minutes. These data suggest that patients needing CPR oftenhave larger infarcts, which have been shown to be associ-ated with shorter time to call.
Predictors of mortality in patients with prehospital CPRare of great interest to optimize prehospital and hospitalsequences. In our study older age and need for intubationwere independent predictors for a higher mortality rate,whereas ventricular fibrillation as initial heart rhythm wasassociated with survival. The highest mortality was seen inpatients with asystole or pulseless electric activity. Theseresults are in line with several previous studies. Roberts etal13 reported that unwitnessed events (p � 0.0316), need forpinephrine (p � 0.0003), identification of pulseless electricctivity or asystole as initial heart rhythm (p �0.0001), andardiac versus respiratory mechanism of arrest were predic-ors of higher hospital mortality in hospitalized patients withardiopulmonary arrest. In a study by Hosmane et al,14
shorter time to return of spontaneous circulation, youngerage, neurologic status after resuscitation (alert or mini-mally responsive), and male gender predicted survival. Inour study the overall rate of reperfusion therapy in pa-tients with STEMI and prehospital CPR was 90%, leav-ing only 10% of the patients without early reperfusiontherapy. Despite this high rate of reperfusion therapy,total mortality of those patients was 40%. Most patients(56.3%) with prehospital diagnosed STEMI and CPRreceived prehospital fibrinolysis.
The role of thrombolytic therapy in patients with STEMIand prehospital resuscitation has not been fully explored. Inrecent European guidelines,15 successful resuscitation is noontraindication to fibrinolytic therapy, but fibrinolytic ther-py should not be given to patients who are refractory toesuscitation. Current European Resuscitation Counciluidelines for resuscitation16 advise that fibrinolysis should
not be used routinely in cardiac arrest. When fibrinolyticagents have been given, CPR should be performed for up to60 to 90 minutes before termination of resuscitation at-tempts. Böttiger et al17 showed that after initially unsuc-essful out-of-hospital CPR, thrombolytic therapy com-
Median Intervals (min) p Value
eceiving Patients With STEMI Not ReceivingPrehospital CPR
(n � 2,127)
78.0 (32.0–233.0) �0.0001100.0 (51.0–253.0) �0.0001
9.0 (6.0–13.0) 0.1832.0 (23.5–45.0) 0.05
EMI Rtal CPR190)
–40.0)0–73.0)–12.0)
ined with heparin is safe and may improve patient

ttovc
ahrHnsplhsfiwtmetrhPos
3tpaMt
differen
1736 The American Journal of Cardiology (www.ajconline.org)
outcome. In addition, Ruiz-Bailén et al18 demonstrated thatadministration of fibrinolysis to patients with acute MI whorequire CPR is efficacious in decreasing mortality with noincrease in hemorrhagic complications. The Thrombolysisduring Resuscitation for Out-of-Hospital Cardiac Arrest(TROICA) trial investigators and the European Resuscita-tion Council study group19 presented conflicting results. Inhe TROICA trial fibrinolysis in patients with out-of-hospi-al cardiac arrest did not improve in 30-day survival, returnf spontaneous circulation, hospital admission, 24-hour sur-ival, survival to hospital discharge, and neurologic out-ome compared to placebo.
190 patients with Spre-hospital resu
107 patients received pre-hospitalthrombolysis
6 (5.6 %) patients died before hospital admission
101 patients survived pre-hospital phase
52 (51.5 %) patients received early PCI
49 (48.5 %) patients received no additional
reperfusion therapy
54 (68.4 %p
Hospital mortality was 26.9 % (14/52)
Hospital mortality was 46.9 % (23/49)
Hoswas
Figure 1. Mortality according to
0
10
20
30
40
50
60
70
Mortalityin %
Asystole Pulseless electricalactivity
Ventricular fibrillation Ventricular tachycardia
Initial heart rhythm
Figure 2. Mortality according to initial heart rhythm.
Our study was not randomized and not designed to ex- d
mine the benefits of revascularization in patients with pre-ospital CPR and STEMI. In addition, our sample waselatively small, despite being 1 of the largest to date.owever, in our study a lower prehospital mortality couldot be observed in patients receiving prehospital fibrinoly-is, even if or although the early diagnosis of STEMI in therehospital phase offered the opportunity to initiate fibrino-ysis therapy within the golden first hour. In addition, pre-ospital fibrinolysis was not an independent predictor ofurvival. In our study 51.5% of patients with STEMI andbrinolysis as initial reperfusion therapy received early PCIithin 12 hours. In these patients mortality was as low as in
hose treated with primary PCI. Median time from firstedical contact to primary PCI was 77 minutes. This is an
xcellent time delay enabled by the diagnosis of STEMI inhe prehospital phase. Numerically the lowest mortalityates were observed in patients with a combination of pre-ospital thrombolysis and subsequent PCI and with primaryCI. However, selection bias may play a major role for eachf these groups because the worst cases may not have beenelected for or did not survive to catheterization.
Our registry has several limitations. We did not collect0-day mortality, a measurement often used in randomizedrials. The reason to decide on 1 reperfusion strategy, i.e.,rehospital fibrinolysis, primary PCI, or early angiographynd PCI after fibrinolysis, was left to the treating physicians.oreover, data on use of therapeutic hypothermia and fur-
her procedures after resuscitation are not available. In ad-
d
83 patients received no pre-hospitalthrombolysis
.8 %) patients died before hospital admission
79 patients survived pre-hospital phase
ts received I
15 (19.0 %) patients receivedno reperfusion therapy
10 (12.6 %) patients received hospital thrombolysis
tality 6/52)
Hospital mortalitywas 66.7% (10/15)
Hospital mortality was 30 % (3/10)
t reperfusion therapy strategies.
TEMI anscitation
4 (4
) patienrimary PC
pital mor30.8 % (1
ition, data on cause of death are not available.

1737Coronary Artery Disease/Prehospital CPR in STEMI
1. Arntz HR, Wenzel V, Dissmann R, Marschalk A, Breckwoldt J,Müller D. Out-of-hospital thrombolysis during cardiopulmonary re-suscitation in patients with high likelihood of ST-elevation myocardialinfarction. Resuscitation 2008;76:180–184.
2. De Luca G, Suryapranata H, Ottervanger JP, Antman EM. Time delayto treatment and mortality in primary angioplasty for acute myocardialinfarction: every minute of delay counts. Circulation 2004;109:1223–1225.
3. Boersma E, Maas AC, Deckers JW, Simoons ML. Early thrombolytictreatment in acute myocardial infarction: reappraisal of the goldenhour. Lancet 1996;348:771–775.
4. Spaulding CM, Joly LM, Rosenberg A, Monchi M, Weber SN, Dhain-aut JF, Carli P. Immediate coronary angiography in survivors ofout-of-hospital cardiac arrest. N Engl J Med 1997;336:1629–1633.
5. Garot P, Lefevre T, Eltchaninoff H, Morice MC, Tamion F, Abry B,Lesault PF, Le Tarnec JY, Pouges C, Margenet A, Monchi M, LaurentI, Dumas P, Garot J, Louvard Y. Six-month outcome of emergencypercutaneous coronary intervention in resuscitated patients after car-diac arrest complicating ST-elevation myocardial infarction. Circula-tion 2007;115:1354–1362.
6. Zeymer U, Arntz H, Dirks HR, Ellinger K, Genzwürker H, Nibbe L,Tebbe U, Senges J, Schneider S. Aktueller Stand der prähospitalen Thera-pie des akuten ST-Streckenhebungs-Myokardinfarkts in Deutschland. De-sign und Basisdaten von PREMIR. Intensiv Notfallbehandlung 2007;32:159–166.
7. Zeymer U, Arntz HR, Dirks B, Ellinger K, Genzwürker H, Nibbe L,Tebbe U, Senges J, Schneider S. Reperfusion rate and inhospitalmortality of patients with ST segment elevation myocardial infarctiondiagnosed already in the prehospital phase: results of the GermanPrehospital Myocardial Infarction Registry (PREMIR). Resuscitation2009;80:402–406.
8. Müller D, Schnitzer L, Brandt J, Arntz HR. The accuracy of anout-of-hospital 12-lead ECG for the detection of ST-elevation myo-cardial infarction immediately after resuscitation. Ann Emerg Med2008;52:658–664.
9. van Campen LC, van Leeuwen GR, Verheugt FW. Safety and efficacyof thrombolysis for acute myocardial infarction in patients with pro-longed out-of-hospital cardiopulmonary resuscitation. Am J Cardiol1994;73:953–955.
10. Tenaglia AN, Califf RM, Candela RJ, Kereiakes DJ, Berrios E, Young
SY, Stack RS, Topol EJ. Thrombolytic therapy in patients requiringcardiopulmonary resuscitation. Am J Cardiol 1991;68:1015–1019.11. Scholz KH, Tebbe U, Hermann C, Wojcik J, Lingen R, ChemnitiusJM, Brune S, Kreuzer H. Frequency of complications of cardiopulmo-nary resuscitation after thrombolysis during acute myocardial infarc-tion. Am J Cardiol 1991;69:724–728.
12. Movahed MR, Ramaraj R, Hashemzadeh M, Jamal MM, Hashemza-deh M. Rate of acute ST-Elevation myocardial infarction in the UnitedStates from 1988 to 2004 (from the Nationwide Inpatient Sample).Am J Cardiol 2009;104:5–8.
13. Roberts D, Landolfo K, Light RB, Dobson K. Early predictors ofmortality for hospitalized patients suffering cardiopulmonary arrest.Chest 1990;97:413–419.
14. Hosmane VR, Mustafa NG, Reddy VK, Reese CL IV, DiSabatino A,Kolm P, Hopkins JT, Weintraub WS, Rahman E. Survival and neuro-logic recovery in patients with ST-segment elevation myocardial in-farction resuscitated from cardiac arrest. J Am Coll Cardiol 2009;53:409–415.
15. Van de Werf F, Bax J, Betriu A, Blomstrom-Lundqvist C, Crea F, FalkV, Filippatos G, Fox K, Huber K, Kastrati A, Rosengren A, Steg PG,Tubaro M, Verheugt F, Weidinger F, Weis M; ESC Committee forPractice Guidelines (CPG). Management of acute myocardial infarc-tion in patients presenting with persistent ST-segment elevation: theTask Force on the Management of ST-Segment Elevation Acute Myo-cardial Infarction of the European Society of Cardiology. Eur Heart J2008;29:2909–2945.
16. Nolan JP, Soar J, Zideman DA, Biarent D, Bossaert LL, Deakin C,Koster RW, Wyllie J, Böttiger B; ERC Guidelines Writing Group.European Resuscitation Council Guidelines for Resuscitation 2010Section 1. Executive summary. Resuscitation 2010;81:1219–1276.
17. Böttiger BW, Bode C, Kern S, Gries A, Gust R, Glätzer R, Bauer H,Motsch J, Martin E. Efficacy and safety of thrombolytic therapy afterinitially unsuccessful cardiopulmonary resuscitation: a prospectiveclinical trial. Lancet 2001;357:1583–1585.
18. Ruiz-Bailén M, Aguayo de Hoyos E, Serrano-Córcoles MC, Diáz-Castellanos MA, Ramos-Cuadra JA, Reina-Toral A. Efficacy ofthrombolysis in patients with acute myocardial infarction requiringcardiopulmonary resuscitation. Intensive Care Med 2001;27:1050–1057.
19. Böttiger BW, Arntz HR, Chamberlain DA, Bluhmki E, Belmans A,Danays T, Carli PA, Adgey JA, Bode C, Wenzel V; TROICA TrialInvestigators, European Resuscitation Council Study Group. Throm-
bolysis during resuscitation for out-of-hospital cardiac arrest. N EnglJ Med 2008;359:2651–2662.