Embed Size (px)
Citation preview

Fatal cholestatic hepatitis in aninfant: An unusual etiology
MARK R OLIVER MBBS, ALFREDO PINTO MD, R BRENT SCOTT MDCM
OBSTRUCTIVE JAUNDICE REQUIRES
prompt investigation to identifyan etiology and institute specific sup-portive and/or therapeutic measures toprevent morbidity and mortality. Wereport a three-month-old infant girlwho presented with cholestatic jaun-dice and hepatitis that progressed tofulminant hepatic failure due to adeno-
virus type 5 infection. Postmortem di-agnosis of severe combinedimmunodeficiency syndrome (SCIDS)was made. Infection, viral or bacterial,can be a recognized but less commoncause of this clinical picture in infancy(1,2). However, neither adenovirus in-fection nor immunodeficiency hasbeen included as a cause of hepatitis or
cholestasis during infancy in compre-hensive summaries of the differentialdiagnosis (1-3).
CASE PRESENTATIONClinical history: A three-month-oldfemale born to unrelated Mennoniteparents was transferred from a regionalcentre (following a one-week admis-sion) to the Alberta Children’s Hospi-tal in Calgary, Alberta with cholestaticjaundice and hepatitis as indicated bytotal bilirubin of 68 �mol/L (normalless than 32) with a conjugated biliru-bin of 57 �mol/L and elevated liver en-zymes (aspartate aminotransferase 542U/L [normal 0 to 30] and alkaline phos-phate 1721 U/L [normal 75 to 400]). Atentative diagnosis of biliary atresia hadbeen made at the referring institutionon the basis of absent excretion of bileinto the small intestine during a nuclearmedical hepatobiliary scan. However,there were some unusual features thatweighed against the transfer diagnosisand suggested an infectious etiology.First, the child had also presented withfever, leukopenia (total white bloodcell count 3.2x109 cells/L, normal 5 to18.5) and microcytic, hypochromicanemia (hemoglobin 59 g/L, normal 95to 155). Second, the infant also had ahistory of failure to thrive, with a recentonset of otitis externa. Before transferthe infant commenced a course of bothbroad spectrum intravenous antibioticsand an oral antifungal agent. Cultures ofurine and blood obtained before treat-ment was initiated did not subsequently
BRIEF COMMUNICATION – HEPATOLOGY
MR OLIVER, A PINTO, RB SCOTT. Fatal cholestatic hepatitis in an infant: Anunusual etiology. Can J Gastroenterol 1995;9(4):217-220. An infant girl whopresented with cholestasis and hepatitis that rapidly progressed to fulminant liverfailure is reported. Postmortem examination yielded a diagnosis of demonstratedextensive hepatic necrosis due to adenovirus type 5 infection which had devel-oped in the setting of an occult primary immunodeficiency (severe combined im-munodeficiency). The aim of this report is to alert the physician to a rare cause ofcholestasis and hepatitis in infancy. Recognition of the combination of adenovi-ral infection with underlying primary immunodeficiency is a prerequisite tothe provision of genetic counselling.
Key Words: Adenovirus, Cholestasis, Hepatitis, Immunodeficiency
Hépatite choléstatique fatale chez un nourrisson : étiologieinhabituelle
RÉSUMÉ : Le cas d’un nourrisson de sexe féminin qui a présenté une choléstaseet une hépatite ayant progressé vers une insuffisance hépatique fulminante estrésumé ici. L’autopsie a permis de poser un diagnostic de nécrose hépatique éten-due attribuable à une infection à adénovirus de type 5 qui s’était développée dansle contexte d’une immunodéficience primitive occulte (immunodéficience com-binée grave). Le but de ce rapport est de sensibiliser les médecins à une cause rarede choléstase et d’hépatite chez les nourrissons. L’observation d’une infectionadénovirale combinée à une immunodéficience primitive sous-jacente est essen-tielle à tout counselling génétique.
Department of Pediatrics and Pathology, Alberta Children’s Hospital and University ofCalgary, Calgary, Alberta
Correspondence and reprints: Dr R Brent Scott, Department of Pediatrics, Health ScienceCentre, 3330 Hospital Drive NW, Calgary, Alberta T2N 4N1. Telephone 403-220-4556,Fax 403-283-3028, e-mail [email protected]
CAN J GASTROENTEROL VOL 9 NO 4 JUNE 1995 217

grow either bacterial or fungal patho-gens.
On admission to the Alberta Chil-dren’s Hospital, the following addi-tional information was obtained. Thepatient had been born at term (weight2.8 kg) and at home, in a Mennonite
colony in Mexico. She had been exclu-sively bottle-fed with Enfalac (MeadJohnson Canada) since birth and apartfrom poor weight gain, which the par-ents attributed to ‘difficult feeding’, shehad been relatively well until twoweeks before admission to the referring
hospital, at which time she was jaun-diced and passing both acholic stoolsand dark urine. These symptoms wereaccompanied by a discharging right earand pallor. She had never been immu-nized or been given any prescribed ornonprescribed medications. The pati-ent’s 19-month-old sibling was well.Several unexplained deaths in the firstyears of life were reported on the mater-nal side of the family.
Physical examination confirmedfailure to thrive; both the patient’sheight and weight were below the fifthpercentile. She was afebrile, and ap-peared pale, jaundiced and poorlynourished. There was a yellow dis-charge from her right ear due to otitisexterna and mild oral candidiasis. Bothtonsillar and lymphoid tissue wereclinically present. She was noticeablyirritable on stimulation; however,there was no evidence of focal neuro-logical signs. Her liver was 7 cm in spanand her spleen was palpable 2 cm belowthe left costal margin. There was noother clinical evidence of chronic liverdisease.
Laboratory investigations per-formed on admission are summarized inTable 1. Within 12 h of admission thepatient suffered a significant deteriora-tion characterized by the clinical find-ings of shock, bleeding diathesis anddeteriorating liver function. She re-ceived supportive care including vol-ume expansion with fresh frozenplasma, antibiotics, pooled immuno-globulin and vitamin K. Serologicalinvestigations for hepatitis A, B and C,cytomegalovirus, toxoplasmosis, herpessimplex and human immunodeficiencyvirus-1 were negative. Plasma aminoacids and urinary organic acid profilefailed to detect an underlying meta-bolic disorder. Repeat blood and urinecultures were negative for bacterial orfungal organisms. Rotavirus was iso-lated from the stools and adenoviruscultured from the patient’s nasopha-rynx eight days following admission tothe Children’s Hospital. Despite allsupportive efforts the patient’s coagu-lopathy persisted (uncorrected byblood products and vitamin K) andher liver function continued to deterio-rate (Table 1). In addition, she devel-
TABLE 1Laboratory investigations
On admission Before death Normal values
Hemoglobin (g/L) 94 75 110-147
White blood cells (x109/L) 3 4.9 6-18
Lymphocytes (x109/L) 0.5 1.8 2.8-14.4
Platelets (x109/L) 167 75 150-550
Prothrombin time (s) 15.1 28 11.9-17.7
Activated partial thromboplastin time
(s)
33 >150 23.7-37.9
Fibrinogen (g/L) 2.0 1.4 2-4
D-dimers (fibrinogen equivalent units) <0.05 <0.05 <0.5
Total bilirubin (�mol/L) 55 108 5-23
Conjugated bilirubin (�mol/L) 25 76 0-10
Gamma glutamyltransferase (U/L) 1518 652 16-43
Aspartate aminotransferase (U/L) 1656 23,250 12-50
Alanine transaminase (U/L) 480 1740 5-40
Albumin (g/L) 24 22 35-50
Immunoglobulin G (U/L) 0.73 – 3.45-12.36
Immunoglobulin A (U/L) <0.07 – 0. 14-1.23
Immunoglobulin M (U/L) 0.17 – 0.43-1.73
Alpha-1 antitrypsin (U/L) – 3.48 0.85-2.65
Urinary reducing substances Negative
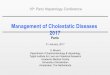
Figure 1) Light microscopy demonstrates extensive necrosis of the hepatocytes without a significantinflammatory response. Some hepatocytes contain intranuclear inclusions consistent with viral infec-tion (hematoxylin and eosin x262)
218 CAN J GASTROENTEROL VOL 9 NO 4 JUNE 1995
OLIVER et al

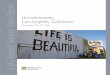
oped significant neurological dysfunc-tion characterized by irritability,opisthotonos, apnea and seizures in theabsence of evidence of an intracranialbleed on cerebral computed tomo-graphic scan (or later at autopsy). Shedied eight days following admission.Autopsy findings: Autopsy revealed adiffuse granular liver, which on his-tological assessment showed exten-sive areas of necrosis with minimal in-flammation and normal portal tracts.Hepatocytes at the periphery of ne-crotic areas contained round nucleiwith acidophilic inclusions sugges-tive of viral infection (Figure 1). Elec-tron microscopic examination of livertissue revealed the presence of adenovi-rus particles (Figure 2). The adenoviruswas serotyped as type 5 by standard neu-tralization tests using adenovirus type 5reference antisera (4). At the time ofautopsy, adenovirus was cultured fromstools, heart, lungs, liver, cerebrospinalfluid and throat, reflecting terminalviremia. There was no evidence of in-flammation or viral inclusion bodiesdetected in other organs apart from theliver. Examination of the reticuloendo-thelial system disclosed a small thymuswith complete depletion of lympho-cytes, dysplastic epithelium and ab-sence of Hassall’s corpuscles. Thelymph nodes, spleen and Peyer’spatches were depleted in lymphocytesand showed no evidence of germinalcentres. These histological findings arecharacteristic of severe combined im-munodeficiency (5).
DISCUSSIONA diagnosis of SCIDS, a heteroge-
nous group of disorders characterizedby a gross functional impairment ofboth T and B lymphocytes, was madein our patient. This diagnosis is sup-ported by both laboratory and autopsyfindings including the presence of lym-phocytopenia, hypogammaglobuline-mia, thymic dysplasia and generalizedlymphoid hypoplasia. There is usually apositive family history obtained in 50%of patients with SCIDS which may re-flect an autosomal recessive, dominantor X-linked pattern of inheritance (6).It is possible that in this patient’s Men-nonite background there is an unrecog-
nized basis for recessive inheritance;however, the precise inheritance of herdisease remains to be elucidated.
Adenovirus can, like many other vi-ruses, take advantage of an abnormalimmune system and produce either per-sistent or generalized infections(4,7-11). In the immunocompromisedpatient with adenoviral infection thereis a case fatality rate of over 50% inthose who present with hepatitiscompared with less than 10% in theimmunocompetent patient (9). Whenadenoviral infection occurs as a resultof a primary immunodeficiency, over90% of cases are associated with SCIDS
(9). Of the 19 reported adenoviral in-duced fatalities in patients with SCIDS,there has been only one previously re-ported case with adenovirus type 5 in-fection, and in that patient the clinicalpicture and outcome was similar to thatdescribed for our patient (10).
There is no specific treatment forSCIDS although a variety of natural andsynthetic products have been used withminimal success, including thymic hu-moral factor, pooled immunoglobulinG (which was used unsuccessfully inour patient) and interferon (9). Morerecently ganciclovir has shown somepromise in disseminated adenoviral in-fection after liver transplantation (12).
Lastly, successful treatment of fulmi-nant viral hepatitis (ECHO virus type11) by orothotopic liver transplanta-tion has been reported in an infant(13). Despite post-transplant immu-nosuppressive drug therapy, this latterpatient’s ECHO viral hepatitis did notrecur. Such aggressive treatment war-rants further assessment in the case ofcertain viral-induced hepatic infec-tions. However, because of our pati-ent’s underlying severe immunodefi-ciency syndrome we do not believe thatliver transplantation would have beenan appropriate therapeutic option.
CONCLUSIONSThe aim of this report was to alert
the physician to a rare cause of cho-lestasis and hepatitis in infancy. Whileadenoviral hepatitis and cholestasis ininfants with SCIDS is rare, and usuallylethal even with early recognition andtreatment, it should not go unrecog-nized because of the need to providegenetic counselling to the family.
ACKNOWLEDGEMENTS: The authorsthank Roberta Funk for typing the manu-script. Mark Oliver is a recipient of an Al-berta Children’s Hospital FoundationFellowship.
Figure 2) Hepatocyte showing the typical crystalline array of adenovirus particles withinthe nucleus (uranyl acetate-lead citrate x5216)
CAN J GASTROENTEROL VOL 9 NO 4 JUNE 1995 217
Fatal cholestatic hepatitis

REFERENCES1. Balistreri WF. Neonatal cholestasis:
lessons from the past, issues for thefuture. Semin Liver Dis 1987;7:61-6.
2. Felber S, Sinatra F. Systemic disordersassociated with neonatal cholestasis.Semin Liver Dis 1987;7:108-18.
3. Moyers MS, Balistreri WF. Prolongedneonatal obstructive jaundice. In:Walker WA, Durie PR, Hamilton JR,Walker-Smith JA, Watkin JB, eds.Pediatric Gastrointestinal Disease.Pathophysiology, Diagnosis andManagement, vol 2. Toronto:BC Decker, 1991:835-48.
4. Washington K, Gossage DL, GottfriedMR. Pathology of the liver in severecombined immunodeficiency and DiGeorge syndrome. Pediatr Pathol1993;13:485-504.
5. Linder J, Purtillo DT. Current concepts
of immunodeficiency disorders. ModPathol 1990;3:524-44.
6. Waldmann TA. Immunodeficiencydiseases: primary and acquired. In:Samter M, Talmage DW, Frank MM,Austen KF, Claman HN, eds. Immuno-logical Diseases, 4th edn. Toronto:Little, Brown & Co, 1988:411-67.
7. Ohbu M, Sasaki K, Okudaira M, IidakaK, Aoyama Y. Adenovirus hepatitis ina patient with severe combinedimmunodeficiency. Acta Pathol Jpn1987;37:655-64.
8. Wigger HJ, Blanc WA. Fatal hepaticand bronchial necrosis and adenovirusinfection with thymic alymphoplasia.N Engl J Med 1966;275:870-4.
9. Heirholzer JC. Adenovirus in theimmunocompromised host. ClinMicrobiol Rev 1992;5:262-74.
10. South MA, Dolen J, Beach DK, Mirkovic
RR. Fatal adenovirus hepatic necrosisin severe combined immunodeficiency.Pediatr Infect Dis J 1982;1:416-9.
11. Spencer MJ, Cherry JD. Adenoviralinfections. In: Feigin KD, Cherry JD,eds. Pediatric Infectious Disease, 3rdedn. Philadelphia: WB Saunders Co,1992:1670-87.
12. Wreghitt TG, Gray JJ, Ward KN, et al.Disseminated adenoviral infection afterliver transplantation and its possibletreatment with ganciclovir.J Infect 1989;19:88-9.
13. Chuang E, Maller ES, Hoffman MA,Hodinka RL, Altschuler SM.Successful treatment and fulminantEchovirus 11 infection in a neonatal byorthotopic liver transplantation.J Pediatr Gastroenterol Nutr1993;17:211-4.
220 CAN J GASTROENTEROL VOL 9 NO 4 JUNE 1995
OLIVER et al

Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com





![Current and future therapies for inherited cholestatic …...using an isolated jejunal loop as a conduit from gall bladder to mid ascending colon[26-28]. At present, only a few reports](https://img.pdfslide.us/doc/110x75/5f7a227db72e4d5f0e42d856/current-and-future-therapies-for-inherited-cholestatic-using-an-isolated-jejunal.jpg)