Embed Size (px)
Citation preview

Thorax (1953), 8, 195.
FATAL BRONCHIAL ASTHMAA SERIES OF FIFTEEN CASES WITH A REVIEW OF THE LITERATURE
BY
B. V. EARLEFrom the Westminster Hospital, London
(RECEIVED FOR PUBLICATION DECEMBER 8, 1952)
The chief object of this study is to investigatethe cause and incidence of death from asthma.The records of 15 cases of fatal asthma have beencollected. Three were observed personally at theWestminster Hospital and at the Willesden GeneralHospital, London, and the others obtained from thecase records of these hospitals and of LlandoughHospital, Cardiff, the Cardiff Royal Infirmary, theHospital for Sick Children, London, and Grayling-well Hospital, Chichester.
There is a widespread impression that deathnever results from uncomplicated bronchial asthma,and this view is supported by the older authorities.Trousseau described it as " le brevet de longue vie."Osler quotes Oliver Wendell Holmes as callingasthma " the slightest ailment that promoteslongevity." Modern textbooks make little referenceto death ensuing from this condition, and in thiscountry only one case with post-mortem findingshas been recorded (Thomson, 1945). It is nowbecoming recognized that asthma may be fatal,but death in hospital remains rare because mostcases are treated at home by their own doctors.
LITERATURE OF FATAL CASES
Tables 1, lI, and III contain a summary of 160cases so far reported in the world literature. Caseswithout adequate post-mortem studies and clinicalhistories have not been included, but otherwise thelist is as complete as possible.The pathological findings in most cases were as
follows: (1) Gross emphysema; (2) the bronchialtree plugged with sticky mucus; (3) the bronchialwalls thickened by muscular hypertrophy, wideningof the basement membrane, and oedema of alllayers; (4) infiltration of the bronchial walls byeosinophils; (5) hyperactivity of the bronchialmucous glands. The above features are listed asusual " in the Tables.The cases have been classified under three
headings: (1) Uncomplicated fatal asthma, (2)asthma the chiefcause of death, (3) death from othercauses. There were altogether 90 cases in which
asthma had been the only or chief cause of death.Forty-one of these were male and 49 female. Morethan half of the deaths took place between tht
TABLE INECROPSY REPORTS IN CASES OF ASTHMA RECORDED'
IN THE WORLD LITERATURE
Total Uncom- Asthma DeathYear Author No. plicated theCChief fromof Fatal Cause of Other
Cases Asthma Death Causes
1922 Huber and Koessler 21 5 3 131923 Lemierre, Leon-Kind- 1 1
berg, and Levesque1926 Rackemann .. 1 11927 Alexander, Luten, and I I
Kountz1927 Dehner .. .. .. 1 11928 Steinberg and Figley . . 2 1 11928 Kountz and Alexander 3 2 11930 Harkavy .. 2 1 11930 Clarke . . 1 11930 Fisher and Beck 1 11930 Wright I.. 11933 Macdonald .. 8 1 2 51933 Riopelle 1 11933 D'Antoniazzi .. 1 11935 Bubert and Warner 1 11936 MAimer, Eiman, and I I
Miller1935 Waldbott .. 2 21935 Michael and Rowe 2 21936 Hansen .. I 11935 Brul6, Hillemand, I I
Delarue, and Netter1936 Colton and Ziskin 6 3 1 21938 Thieme and Sheldon 17 2 5 101937 Fowler 2 1 11939 Facquet and Claisse 1 11941 Traisman .. I 11941 Harkavy .. 4 41941 Craige.7 5 21942 Chafee, Ross, and Gunn 6 3 31943 Fourestier .. 11943 Brul6, Hillemand, 1
Delarue, and Audoly1945 Unger.5 3 21945 Thomson I...1946 Massachusetts General I I
Hospital1946 Gay.24 2 4 181946 Bergstrand .. . 4 41946 Cummings .. 1 11947 Peterson .. 1 11947 Tichenor and Lafsky . . 1 11947 Wilson and Alexander I 11947 Wakefield ..1 11948 Lennox .. 1 11948 Benson and Perlman 3 2 11949 Schwartz .. 1 11949 Blanton and Sutphin 1 11950 Mitchell and Bacal 2 1 11951 Walton et al. 13 10 2 1
Total .. .. 160 56 (35%) 34 (21%) 70(44%)
on July 18, 2020 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.8.3.195 on 1 Septem
ber 1953. Dow
nloaded from

TABLE IISUMMARY OF 56 DEATHS DUE TO UNCOMPLICATED ASTHMA RECORDED IN THE LITERATURE
Authors
Huber and Koessler
Iemierre and o:hersRackemannAlexander and othersDehner
Kountz and Alexander
Clarke
WrightMacdonaldRiopelleAntoniazziBubert and Warner
Waldbott
Michael and Rowe
Brul6 and othersHansen
Colton and Ziskin
Fowler
Thieme and Sheldon..
Facquet and Claisse..
Craige
Traisman
Fourestier and others
Ungvr.
Thomson
Gay.
Age
{48 vrs.485515 mths.53 yrs.
58396551
{60\48
53
6743623869
6 mths.
3 ,
g 48 yrs.
t574556{56
434368
T18 mths.
L2! yrs.59
r4553
450
L491 yr.
38 yrs.
43 -
yr.31 yrs.
47
52_62 ,
Cummings .. 58Wilson and Alexander 65Blanton and Sutphin.. 57
4454
Walton and others 57
62
61
1611 41
Sex
.NIM
FM
FM
M
M
M
F
M
F
F
F
M
M
F
F
F
M
M
M
M
F
M
F
F
F
FMF
F
FFF
F
F
F
F
F
M
M
F
M
F
M
FFM
FM
F
M
Durationof Asthma
5 yrs.2,,5,,5 mths.
23 yrs.
3 mths13 yrs.
I yr.
3,,254012
8,,5,,3,,I yr.
2 yrs.
Few days
6 wks.15 yrs.
3,,3,'6 mths.lo
yr.S yrs.
8 ,,
11 mths.
14 yrs.
5 ,,
6 mths14 yrs.2,,7,,
9,,6 mths.
I mth.1 yr.9 mths.4 yrs.
20
203,,
5015 mths.
32 yrs.
29
393,,
8,,yr.
,,
1 ,,No details
I yr.8 yrs.
P.M. Findingsin Lungs
Usual
No mucous plugsUsual, but mucus scantyUsualUsual; no emphysemaUsual
1,,
Usual, but few eosinophilsUsual; little mucusUsualUsual; patchy atelectasis
Usual; no emphysemaUsual
,,Usual; pulmonary oedemaUsual; pulmonary congestion
Pulmonary congestion andoedema
Usual'
Usual: oedema of lungsUsual
Oedema; emphysema; thicken-
ing of bronchial. walls
Usual
Emphysema and eosinophilia of
bronchial walls onlyUsual
Dilated alveoli with haemor-
rhages into them
Usual; areas of atelectasis
Usual
Usual; patchy collapse
Usual
Usual; squamous metaplasiaof bronchial mucosa; collapseleft lower lobe
Usual with active mucous glandsbut no plugs
Usual
,,
..
.,
.,
..
Special Features
Many eosinophils in liver, spleen
Pethidine just before deathRight ventricular hypertrophy
Right ventricle hypertrophiedModerate general hypertrophy of
heart; thymus+Aspirin-sensitive
Blood pressure considerably raisedin attacks
Aspirin-sensitive; thymus, 6 g,atrophy of adrenals
Thymus, 7 g.
Right ventricle much hypertrophied
Right ventricle slightly hyper-trophied
Thymus, 23 g.
Persistent thymus; eosinophil reac-tion in ovarian dermoid
Right ventricular hypertrophyDeath after skin test; adrenaline-
sensitivePersistent thymus; splenic eosino-
philiaPersistent thymusPersistent thymus; splenic eosino-
philia; right heart hypertrophySplenic eosinophiliaRight heart hypertrophyRight heart hypertrophy; splenic
eosinophilia
Splenic eosinophilia; right hearthypertrophy; persistent thymus;splenic eosinophilia
Year
1922
1923192619271927
1928
1930
19301932193319331935
1935
1935
19351936
1936
1937
1933
1939
1941
1941
1943
1945
1945
1946
194619471 949
1951
I1 --I-1-1 -1-
,
I
-
on July 18, 2020 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.8.3.195 on 1 Septem
ber 1953. Dow
nloaded from

FATAL BRONCHIAL ASTHMA 197
TABLE HIISUMMARY OF 34 CASES OF ASTHMA AS CHIEF CAUSE OF DEATH RECORDED IN THE LITERATURE
Year Au&hors Age Sex Duration P.M. Findings Special Featuresof Asthma in Lungs SeilFaue
Huber and Kozssler . .
Kountz and Alexander
Steinberg and Figley.Harkavy
Macdona'd
Colton and Ziskin
Thieme and Sheldon
Craige
Chafee and others
Chafee and others
Brule and others
Unger.
Gay.
Gay.
Peterson
Wakefield
Benson and Perlman..
Lennox
Mitchell and Bacal
Walton and others . .
48 yrs.< 53 ,,L27 ,,52 ,
60 ,
23 ,
53 ,
3645 ,,
r14.13747 ,,
51 ,,,59 ,,
{23 ,
67 ,
27 ,
r38
L41 ,
58 ,
r34 ,
L46 .,46
rt4 ,,. 50 ,52 ,
L20 ,
34 ,
28 ,
51 ,
38 ,
r14 mths.
i58 yrs.
FFM
FFM
MM
F
M
M
M
MF
FF
M
FF
F
FM
M
FF
F
F
M
F
F
M
M
1 yr.23 yrs.
1 yr.2 yrs.
18 ,
6 mths.I yr.
14 yrs.3 ,,
18 mths.
35 yrs.
30 ,
38 ,
1 yr.7 yrs.
7,,20 ,
10 ,
12 ,
8 ,,
25 ,
2,,21 ,,
6,,
1 yr.2 yrs.
8 ,,
2,,
23 ,
20 ,
4,,
2,,
1 yr.
40 yrs.
Usual; also bronchopneumoniaUsual; also acute bronchitis
Usual; also pulmonary tuber-culosis
Usual; also acute bronchitisUsualUsual; plugs incomplete; acute
bronchitisUsual; also bronchopneumoniaUsual; adhesive paricarditis,no histology reported
Usual with early broncho-pneumonia
No mucous plugs; very earlybronchopneumonia
Usual; also left pneumothorax,early bronchopneumonia
Usual; also bronchopneumonia
Usual; also early broncho-pneumonia
Usual; also bronchopneumoniaUsual, with bronchopneumonia
Emphysema, chronic bronchitis,bronchopneumonia; a feweosinophils only
Usual with bronchopneumoniaUsual; patchy pulmonaryoedema
Emphysema; patchy collapsecomplete of left lower lobe;oedema; purulent bronchio-litis; a few eosinophils inalveoli and near bronchi
Emphysema; no histologyUsual; left lung collapsed;
tuberculosis, probable pneumo-thorax
Usual with pneumonia;squamous metaplasia
Usual with pneumoniabIsual with atelectasis, pneu-
monia; squamous metaplasiaUsual; subcutaneous and
mediastinal emphysemaUsual; left lower lobe broncho-pneumonia; patchy atelecta-sis right lower lobe
Purulent bronchitis and broncho-pneumonia; squamous meta-plasia of bronchial epithelium
Usual; also early broncho-pneumonia
Usual
9,,
Usual; also terminal broncho-pneumonia
Usual; also pneumonia
Right heart slightly hypertrophiedRight ventricle hypertrophied
Reaction to typhoid vaccineRight ventricular hypertrophy
Death 2 days after transpleuralneurectomy; right ventriclemoderately hypertrophied
Right ventricle considerably hyper-trophied
Myocardial degeneration witheosinophil infiltration
Right ventricular hypertrophySudden death after stellate ganglion
block
Aspirin-sensitiveRight ventricular hypertrophy
Generalized cardiac hypertrophy
Patient 4 months pregnant at death
Myocardial and pericardial fibrosis;heart failure
Acute pulmonary emphysema withleft (drained) pneumothorex;subcutaneous emphysema
Splenic eosinophilia
Right heart hypertrophy; spleniceosinophi.ia
1922
1928
19281930
1933
1936
1938
1941
1942
1942
1943
1945
1946
1946
1947
1947
1948
1948
1950
1951
-I_~l X Il1
on July 18, 2020 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.8.3.195 on 1 Septem
ber 1953. Dow
nloaded from

B. V. EARLE
ages of 40 and 60 years. There were seven deathsbefore the age of 5, but only eight deaths between5 and 30 years. Forty-nine patients had diedwithin five years and 62 within 10 years of theonset of asthma.The chief complication was found to be broncho-
pneumonia (20 cases). Inflammatory changes hadnot usually been enough to obliterate the under-lying pathological picture of asthma. Mediastinalemphysema with pneumothorax was seen in fourcases. A persistent or overweight thymus wasnoted nine times. Right ventricular hypertrophyof moderate to considerable degree was found in
TABLE IVSUMMARY OF SEVEN CASES WITH DEATH DUE TO
UNCOMPLICATED ASTHMA IN PRESENT SERIES
Cas Duration P.M. SpecialNos Age Sex of Findings FeaturesAsthma in Lungs
1 43 yrs. F 23 yrs. Usual Thymus 23 g.2 48 ,, F 40 ,, Usual, but no
eosinophilia;some oedema oflung
3 30 ., F 25 ,, Usual; some oed-ema and atelec-tasis
4 6 mths. M 3 mths. Usual Patent ductus;thymus 40 g.
5 42 yrs. F 41 yrs. ,Slight yper-trophy ofright ven-tricle
6 62 ,. F 53 ,, Peribronchialeosinophilia only
7 55 ,, M yr. Usual
TABLE VSUMMARY OF EIGHT CASES WITH ASTHMA AS THE
CHIEF CAUSE OF DEATH
Case Duration P.M. specialNo. Age Sex of Findings Features.Asthma in Lungs
8 2 yrs. F 5 mths. Subcutaneous andmediastinal em-physema, patchyemphysema andoedema; puru-lent bronchitis
9 52 ,, M 5 yrs. Right lung col- Right ventricu-lapsed with lar hyper-pneumothorax trophy
10 50 ,, M 20 ,, Usual; also pul-monary embolus
11 47 ,, M 9 ,. Emphysema, somecollapse of leftlung; very eariybronchopneu-monia
12 53 ,, F 17 ,, Emphysema andbronchopneu-monia
13 62 ,, M 4 ,. Emphysema only Generalizedcardiachyigpertrophy14 65 ,, F 60 ,, Usual ht aorticincompe-tence; smallmeningoma
15 21 ,, F 1 yr. Usual; also bron-chitis and areasof collapse
nine of the uncomplicated and five of the com-plicated cases. Eosinophilia was found in thespleen in 10 cases, in the heart in one, and in theliver and an ovarian dermoid in one.
PRESENT SERIES OF FATAL CASESTables IV and V contain an analysis of the main
features of fatal cases (15 in all). Case historiesare given at the end of this paper (those personallyobserved in greater detail).There were nine female and six male patients.
Ten died between the ages of 35 and 60 years. Fourdeaths took place before the age of 5. There wasonly one death between the ages of 5 and 35 years.Eight patients out of 15 were dead within ten yearsof the onset of asthma.
Pathological findings approximate to those foundin previously reported cases. Nine of the 15 casesshowed the basic changes of asthma already des-cribed. Four had emphysema only. Two werecomplicated by bronchitis, one by early broncho-pneumonia, and one by a pulmonary embolus.Considerable enlargement of the right ventricle wasseen in one, slight enlargement in another, while athird had hypertrophy of both ventricles. Pneumo-thorax and mediastinal emphysema were eachfound once.
THE CAUSE OF DEATH IN ASTHMAMECHANISM OF DEATH.-MOSt writers are agreed
that the chief cause of death is asphyxia due tobronchial obstruction, but not all are agreed as tothe cause of the obstruction. The two principaltheories are spasm of the bronchial musculatureand swelling of the mucous membrane with increasedbronchial secretion and the formation of mucousplugs. Most authors attach much more importanceto bronchial secretion than to bronchospasm.THE ROLE OF DRUGS.-Morphine is generally
incriminated as a precipitating cause of death.Clarke (1930), Thieme and Sheldon (1938), Craige(1941), Thomson (1945), Unger (1945), and Serafini(1950) all describe patients dying within a fewhours of having morphine. Facquet and Claisse'spatients (1939) died a few mihutes after having beengiven the drug. Morphine was of great importancein Case 3 of the present series. The patient becamesemi-comatose soon after j grain (30 mg.) hadbeen given. In Case 1 also morphine was a con-tributory factor.
Aspirin appears to initiate the attack in thesmall group of asthmatics which is sensitive to thedrug. Coke and Coke (1939), Wright (1930),Macdonald (1933), Michael and Rowe (1935), andUnger (1945) all describe deaths in cases sensitive
198
on July 18, 2020 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.8.3.195 on 1 Septem
ber 1953. Dow
nloaded from

FATAL BRONCHIAL ASTHMA
TABLE VIRESPONSE TO DRUGS AND CAUSE OF DEATH IN CASES OF PRESENT SERIES
Case Duration of Response to DrugsNo. Age Sex Fatal Attack during Fatal Attack Remarks
1 43 F 18 hours Morphine 12 hrs. before death. Unrespon- Death from asphyxia. Morphine may havesive to adrenaline subcutaneously (600 played a partminims in all)
2 48 F Not known Gave herself adrenaline just before death May have died from accidental intravenousinjection of adrenaline
3 30 F 36 hours Morphine, gr. i, a few hours before death; Death from asphyxia; morphine anadrenaline-resistant (260 minims); no important aggravating factorimprovement from ether and olive oilenema
4 6 mths. M 24 ,, Resistant to adrenaline subcutaneously Fatal attack precipitated by attempteddesensitization
5 42 F 8 days No response to adrenaline; became rapidly Fairly sudden death in a patient exhaustedresistant to intravenous aminophylline and anoxic from status asthmaticus
6 62 F 36 hours No response to subcutaneous adrenaline or Death from progressive asphyxiaintravenous aminophylline
7 55 M 24 ,, No response to subcutaneous adrenaline; Death from asphyxia. Patient was alreadytemporary improvement with amino- semi-comatose on admission to hospitalphylline
8 21 F Less than No record Mediastinal emphysema may have been an12 hours important cause of death
9 52 M 12 hours Adrenaline subcutaneously gave no relief A left-sided pneumothorax was a contri-butory cause of the asphyxial death
10 50 M 6 days Unrelieved by intravenous aminophylline; A small pulmonary embolus was the precipi-morphine, gr. J, on the day before death tating cause of death in a patient exhausted
and partially asphyxiated by statusasthmaticus
11 47 M 6 ,, No response to 05 ml. of /1000 adrenaline Death from asphyxia complicated by verysubcutaneously, ephedrine orally, or early bronchopneumonia. Patient hadatropine gr. 1/ 100 subcutaneously; some suffered from recurrent episodes of con-benefit from 0 25 g. aminophylline i.v. gestive heart failure as a result of right
heart strain. There was no evidence ofheart failure during the terminal asthmaticattack
12 53 F 2 ,, No response to adrenaline Death from asphyxia complicated bybronchopneumonia; a schizophrenic,whose mental condition improved whenshe had asthma
13 62 M Mild asthma No response to adrenaline subcutaneously Sudden death after emotional shock duringfor 3 wks. a mild but prolonged asthmatic bout; some
degree of congestive heart failure14 65 F 24 hours ,, ., ,, ,. History of a number of attacks shortly before
the fatal one becoming increasinglyresistant to adrenaline; progressiveasphyxia with terminal circulatory collapse
15 2+ F 2 days Very large doses of adrenaline (25 minims Purulent bronchitis an important contribu-subcutaneously at one time) without benefit tory cause of death
to aspirin. In the case described by Wright therewas a violent fatal paroxysm of asthma a fewminutes after taking a tablet.
Adrenaline may be dangerous. Very rarely itmay produce a generalized reaction with urticaria.This appeared to be fatal in one case (Frankland,personal communication). Over-dosage may be acause of death, especially in children. ThusTraisman (1941) describes a child of 1 year dyingafter being given 10 min. (0.6 ml.) of 1 in 1,000adrenaline, and Blanton and Sutphin (1949) reportsudden death in an asthmatic after 1 ml. of 1 in1,000 adrenaline. Case 2 of the present seriesdied after an injection of adrenaline, probablygiven intravenously. In cases of heart diseaseadrenaline is naturally dangerous, while in somepeople with normal hearts it seems to cause anexcessive rise of blood pressure. Gay (1946)describes a patient developing coma and lefthemiparesis after 5 ml. of 1 in 1,000 adrenaline.Benson and Perlman (1948) believe that adrenaline
inhalers are very dangerous because they damagethe epithelium of the respiratory tract allowing easyaccess of pyogenic organisms. They noted 48 deathsin 649 patients using sprays (7.4%). In 1,588patients who did not use them there were 72 deaths(4.5%). Facquet and Claisse (1939) and Hamburger,Milliez, and Halpern (1947) believe that repeateduse of adrenaline may result in increased bronchialsecretion of mucus and cause adrenaline " resist-ance " during an attack. Moulis (1950) noted threedeaths in patients who had been taking largeamounts of adrenaline.
Villanova (1948) describes fatal cases afterintravenous procaine. Intravenous tetraethyl-ammonium bromide has only recently been usedfor treating asthma, but has already given rise toone death and a number of non-fatal reactions(Schwartz, 1949). According to Vaughan (1948)digitalis may be dangerous in asthma, but he doesnot offer evidence to support this statement, nor isit substantiated by others.
199
on July 18, 2020 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.8.3.195 on 1 Septem
ber 1953. Dow
nloaded from

B. V. EARLE
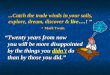
Uncomplicatedfatal asthma.
3 -
L 2 -
u
o5 1 _z
2..~~s:ThtlAsthma chief cause
of de-ath.
I I I I I I
5 10 15 20 25 305 4 4 I I I6
35 40 45 50 55 60 65AGE AT DEATH
5
4-
3
2
I I I I I I I I I
5 10 15 20 25 30 35 40 45 50 55 60 65 70
AGE AT DEATH
Fiei. 1. -Age at death in fatal cases of asthma. Above, 15 cases of present series. Below, 90 cases recorded in the literature.
13 -
12 -
11 -
10-
9-
8-
7-
U-0 6,
6z
200
on July 18, 2020 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.8.3.195 on 1 Septem
ber 1953. Dow
nloaded from

FATAL BRONCHIAL ASTHMA
Pethidine is blamed by Wilson and Alexander(1947) and by Walton, Penner, and Wilt (1951) foraltogether four deaths.ANAPHYLACTIC SHOCK AND FATAL ASTHMA.-
The changes found in the lungs of asthmatics andothers who have died from anaphylactic shock mayresemble very closely those found in uncomplicatedfatal asthma (Meakins, 1944; Vance and Strass-mann, 1942; Huber and Koessler, 1922).
50
45
40 -
35-
< 30 -
U-
625z
20
15 -
10 -
5 -
9
5 10 15 20 25 30DURAT:ON Or HISTORY
FIG. 2.-Duration of history of asthma at death. Cases re4
Anaphylactic shock is usually rapidly fatalwithin minutes to an hour or so, and althoughassociated with bronchospasm is a generalizcdreaction. There is usually peripheral circulatoryfailure and sometimes convulsions or other evidenceof its widespread nature. This is quite a differentpicture from the gradual suffocation of statusasthmaticus. Asthmatics are abnormally liable tohorse serum reactions. They may sometimes getover the initial shock only to pass into statusasthmaticus. Skin testing in an asthmatic may
provoke either a rapidly fatal anaphylactic shock
or a prolonged attack of asthma. The dangersare discussed by Blanton and Sutphin (1949).Case 4 of the present series was an example of this.Waldbott (1935) believes that all asthmatic
deaths in infancy arise from a kind of anaphylacticshock, i.e., a different process from the mechanismin adults. This concept is supported by the frequentfinding of pulmonary oedema without mucousplugging in the lungs of infants dying from asthma.This is the picture of death from anaphylacticshock in the experimental rabbit.
MEDIASTINAL EMPHYSEMA AND SPONTANEOUSPNEUMOTHORAX.-Trowbridge (1944) found in theliterature seven fatal cases of bronchial asthmacomplicated by pneumothorax. Mitchell and Bacal(1950) added one more. Schwartz, Mcllroy, andWarren (1945) described 25 cases of pneumothoraxand subcutaneous emphysema in asthmatics withno mortality. The course of 18 cases with media-stinal and subcutaneous emphysema only wassimilarly benign (Rosenberg and Rosenberg, 1938).Case 9 of the present series was complicated by alarge right-sided pneumothorax which appeared tobe an important contributory cause of death.
Thus, pneumothorax accompanying asthma maybe dangerous if a severe asthmatic attack occurs,but is not usually of grave significance.PSYCHOLOGICAL FACTORS AND SUDDEN DEATH.--
Magee (1949) described two patients dying inattacks following an emotional shock, but no post-mortem findings were available. Vagal inhibitionof the heart by sudden fear was postulated. Thisseems to be a possible mechanism in some of therecorded cases in which death has occurred very
rapidly during a slight ormoderate attack. Kayssi(1948) showed that stimu-lation of the vagus nervemay produce sudden
35 40 45 50 death in experimentalanimals; this may be
corded in the literature, the mechais mai methe mechanism in manwhen death has followed very slight trauma tocertain regions (e.g., larynx, abdomen). In rareinstances the vagal overactivity accompanyingasthma perhaps produces the same result.THE HEART AND FATAL ASTHMA.-Cardiac failure
is rarely a primary cause of death in uncomplicatedasthma. Indeed in a number of fatal cases theheart has continued to beat for a minute or soafter respiration has ceased (Thieme and Sheldon,1938; Bubert and Warner, 1935). In the opinionof most authors significant right ventricular hyper-trophy or congestive heart failure are relatively
201
on July 18, 2020 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.8.3.195 on 1 Septem
ber 1953. Dow
nloaded from

B. V. EARLE
uncommon findings in uncomplicated asthma(Kountz and Alexander, 1928; Michael and Rowe,1935; Vaughan, 1948; Villanova, 1948). Gay(1946) found congestive heart failure in only twoof 24 asthmatics dying from various causes. Par-kinson and Hoyle in 1937, describing the conditionof the heart in 80 cases of emphysema, did notfind it more frequently affected in those casescomplicated by asthma.
Three cases of the present series had evidence ofright heart strain as shown by right ventricularhypertrophy at necropsy. Only in Case 13 wasthere any degree of congestive failure at death.Case 11 suffered several bouts of heart failure, butwhen he died during an attack of asthma theheart appeared normal. At necropsy the heartwas found to be of normal size with a healthymyocardium. During episodes of failure theelectrocardiogram had shown right ventricularpreponderance, afterwards returning to normal.Thus the weight of evidence is against heart
failure as an important cause of death in asthma.But in some long-standing cases with muchemphysema it may be so.
THE ROLE OF PULMONARY INFECTIONS.-In manyfatal cases of status asthmaticus very early broncho-pneumonic changes are found after death. Oftenthere has been little or no fever and no clinicalevidence of bronchopneumonia, the course of thedisease having been identical with uncomplicatedfatal asthma. In most instances it seems reasonableto assume that the inflammatory changes wereincidental and that death resulted from asphyxia.In infancy and old age, however, the part playedby infection is difficult to assess, since in these agegroups a relatively slight infection may be fatal.It is uncertain why these early bronchopneumonicchanges should be found. The cases do not presentthe clinical or pathological picture of terminalbronchopneumonia. In a severe prolonged attackof asthma the patient is often exhausted and unableto take nourishment, but he is not as ill as thepatient with malignant disease, uraemia, or similarconditions in whom bronchopneumonia is acommon terminal event. In such cases the pneu-monia is usually confluent, quite unlike the minimalpneumonic changes found in fatal asthma. It hasbeen suggested that infection arises in the minuteatelectatic patches produced by mucous plugs inthe smaller bronchioles (Huber and Koessler, 1922;Clarke, 1930). In elderly people the infection mayprogress and finally dominate the picture, but thisdoes not generally happen.The part attributed to adrenaline inhalers in
reducing the resistance of the bronchial walls to
infection has already been referred to. Furtherwork is needed to ascertain how far this is true.
Cases 8, 11, 12, and 15 of the present seriesshowed evidence of bronchitis or very earlybronchopneumonic change, but in all the clinicalpicture was one of status asthmaticus.
PROGNOSISLittle information can be gathered from the
literature about the prognosis of asthma. Old(1933) analysed life insurance statistics in theU.S.A. and found that among 274 asthmatics theratio of expected to actual deaths was 100 to 121;the death rate from heart disease was three and aquarter times the normal of the population. Dublinand Marks (1933), quoted by Lamson and Butt(1937), found the death rate to be 27% above normalin a series of mixed patients in the U.S.A. Theyalso found a high rate of heart disease. Diagnosesare not always accurate in life insurance statistics,and the unusually high incidence of heart diseasemay reflect confusion between cardiac and bronchialasthma. Williams and Williams (1949) followed up64 cases ofasthma over seven to 12 years in Englandand found that 19.4% had recovered and 17.2%had died. Unfortunately, as they point out, theirseries is too small to warrant statistical analysis.There is no conclusive statistical information avail-able, but the papers quoted suggest that the deathrate is higher among asthmatics than among thepopulation as a whole. Most deaths from uncom-plicated asthma occur between the ages of 40and 65 years. A small percentage take place ininfancy. Death in a young adult is very rare.Nearly half the total number of fatal cases of asthmahave had the disease for less than five years. Thereis an equal mortality in males and females.
SUMMARYDeath from uncomplicated bronchial asthma is
not as rare as was once supposed. Fatal cases arerare in hospital because status asthmaticus isusually treated at home. A series of 15 fatal caseshas been collected and 160 fatal cases publishedin the world literature have been reviewed.Death usually results from asphyxia, produced
by excessive mucous secretion blocking the airpassages. Bronchospasm plays a minor role.Morphine is dangerous because it depresses therespiratory centre and cough reflex so that ithinders expectoration of mucus. Aspirin mayprovoke violent, even fatal, attacks in asthmaticswho are sensitive to it. Adrenaline may be fatalif accidentally or deliberately injected intravenously.Some asthmatics die suddenly without sufficient
-20-2
on July 18, 2020 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.8.3.195 on 1 Septem
ber 1953. Dow
nloaded from

FATAL BRONCHIAL ASTHMA
cause being demonstrated at necropsy; vagalinhibition of the heart by physical or psychologicalstimuli is a possible mechanism.
Heart failure has little importance as an imme-diate cause of death in asthma. Failure of the rightheart takes place only as a result of the emphysemawhich complicates long-standing asthma. Onepatient (No. 11) in the reported series developedcongestive heart failure secondarily to emphysemaand recurrent bronchopneumonia. The heartreturned to normal when the pneumonia clearedup. The patient died a year later in status asthma-ticus; but even during this fatal attack the heartremained normal, and at necropsy there was no
hypertrophy of the right ventricle.Pulmonary infection is a common complication
which tends to prolong the asthmatic attack andmay be difficult to diagnose. Resistance to infec-tion may be lowered by the prolonged use ofadrenaline inhalers.On the whole prognosis is good during an attack
of status asthmaticus. Death in a young adult isvery rare. There is a slight but definite risk tolife in the patient aged between 40 and 65 years.
CASE RECORDS
CASE 1: FATAL UNCOMPLICATED ASTHMA (from therecords of Llandough Hospital).-A woman aged 43had suffered from asthma since pneumonia at the age
of 20. She developed a severe attack which did notrespond to adrenaline or morphine i grain (15 mg.) andwas admitted to hospital the same day. There she was
given 1 in 1,000 adrenaline at five to 10 minute intervalsin doses of 35 minims (2 ml.), to a total of 600 minims(35 ml.). This produced no relief and she died earlynext morning. At necropsy both lungs were found tobe very emphysematous and moderately congested,with oedema at the bases; there were tenacious mucousplugs in the bronchi and extensive pleural adhesions on
the left. Microscopically there was emphysema withoedema and congestion of the alveolar walls, and thebronchi showed disintegration of the mucous membrane,hypertrophy of the muscle layer, and prominent elasticlamina. The right heart was dilated and the abdominalviscera congested. Other findings were normal.
CASE 2: FATAL UNCOMPLICATED ASTHMA (from therecords of the Cardiff Royal Infirmary).-A woman
aged 48 had suffered from asthma since childhood. Atjust before midnight she called another occupant ofher house and said, " I am dying," then rapidly becameunconscious and was dead before the doctor arrived.A hypodermic syringe containing adrenaline was foundbeside her. At necropsy needle punctures were foundon the outer surfaces of both thighs. The trachea andlarge bronchi were filled with sticky mucus and therewere small petechiae at the lower end of the trachea.Both lungs were very emphysematous; the bronchihad thickened walls and contained thick mucous plugs.
The left lung had several small, well-encapsulatedcaseous areas in the subpleural part of the upper lobeand old adhesions over the greater part of this area.Microscopically there was some lung oedema, thebronchial walls were thickened with prominent muscles,and section through the caseous area showed tuber-culosis. There was a persistent thymus, weighing 23 g.Other organs were normal.
CASE 3: FATAL UNCOMPLICATED AsTHMA (from therecords of Llandough Hospital).-This 30-year-oldwoman had had asthma since childhood. She wasadmitted to hospital in an attack which had started theprevious day. Shortly before admission she had beengiven morphine j grain (20 mg.) subcutaneously. Shewas semiconscious, very dyspnoeic and cyanosed, withvery active accessory muscles of respiration and loudexpiratory rhonchi. The pulse rate was 135 per minute,regular, of poor volume. Over two and a half hoursshe was given a total of 440 minims (26 ml.) of 1 in 1,000adrenaline in divided doses and then an enema of 1 oz.(30 ml.) each of ether and olive oil, but she died threehours after admission. At necropsy the lungs showedlarge areas of atelectasis with surrounding emphysema,bronchioles plugged with thick, tenacious mucus, andhypertrophied small bronchi and bronchioles. Thealveolar walls were thickened with eosinophilic materialand some alveoli contained eosinophilic strands. Otherorgans showed no significant change.CASE 4: FATAL UNCOMPLICATED ASTHMA (from the
records of the Hospital for Sick Children, London).-This baby was well till the age of 3 months when hedeveloped asthma and eczema. He was breast-fed till4 months of age when cow's milk precipitated a severeattack. At six months desensitization with a solutionderived from milk protein was begun; the third injectionwas followed after an hour by a severe asthmatic attack.On admission to hospital next day he was moribundand cyanosed. There was very poor air entry, extremerib recession, and high-pitched expiratory rhonchi. Hewas given 2 minims (0.12 ml.) of 1 in 1,000 adrenaline,but died an hour later. At necropsy the lungs showedsome emphysema, small areas of collapse throughout,and a bronchial tree filled with thick, greenish-yellowmucus. Microscopically the trachea showed somedesquamation of the epithelium, active mucous glands,and its wall infiltrated with eosinophils, plasma cells,and lymphocytes. The mucus filling the bronchi andlarger bronchioles contained numerous eosinophils,neutrophils, and lymphocytes, and the same cells infil-trated the walls. The smaller bronchioles showedemphysema, collapse, oedema, and wide dilatation.There was histiocytic infiltration of the alveoli, andincreased lymphocytes and polymorphs in the pulmonarysepta. Other organs showed no significant change.CASE 5: FATAL UNCOMPLICATED ASTHMA (from the
records of Llandough Hospital).-This 42-year-oldwoman had had asthma since she was a year old. Ninedays before admission she developed pneumonia whichresponded to a sulphonamide, but was followed byasthmatic paroxysms unrelieved by adrenaline. On
203
on July 18, 2020 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.8.3.195 on 1 Septem
ber 1953. Dow
nloaded from

B. V. EARLE
admission she was pale and anxious; respirations were30 per minute, chest expansion was poor with generalizedrhonchi and a loud expiratory wheeze. She did notrespond to aminophylline intravenously, or later to thesame drug rectally, and died a week after admissionafter being in status asthmaticus for a week andremaining apyrexial throughout. At necropsy the lungsshowed thickened bronchi with tenacious plugs ofmucus and no evidence of infection; the heart wasnormal except for slight hypertrophy of the rightventricle; the only other abnormality found was auterine fibroid.
CASE 6: FATAL UNCOMPLICATED ASTHMA (from therecords of Llandough Hospital).-This 62-year-oldwoman had had asthma since the age of 9. She developedan asthmatic attack which failed to respond to adren-aline, and was admitted the same day. On admissionshe was drowsy and cyanosed with a temperature of990 F. (37.20 C.) and respiration rate of 40 per min.,with difficult and prolonged expiration; the lungs wereresonant throughout with numerous rales and rhonchi;the pulse was feeble (150 per minute); blood pressure was120/65 mm. Hg. In spite of adrenaline and intravenousaminophylline she became progressively worse and diednext day. At necropsy the walls of the bronchi wereinfiltrated with eosinophils and the muscle layer hyper-trophied, and they were filled with mucus containingeosinophils. There was moderate atheroma of theaorta and coronary arteries. Other findings were withinnormal limits.
CASE 7: FATAL UNCOMPLICATED ASTHMA (from therecords of Llandough Hospital).-This 55-year-old manhad a history of asthma for one year. A sudden severeattack began on the day of admission. On examinationhe was very cyanosed, semi-comatose, and pulseless withcold extremities. Expiration was very difficult with ageneralized wheeze. Temperature was 990 F. (37.20 C.),heart rate 130 per min.; blood pressure 130/70. Hewas treated with 1 g. aminophylline intravenously(which produced some improvement) three-hourlypenicillin, and continuous oxygen. He died next day.At necropsy the lungs showed slight emphysema; themedium-sized bronchi were thickened and containedvery tenacious mucous plugs. Microscopically thebronchi and bronchioles contained mucous plugs withpolymorphs, eosinophils, and macrophages, but relativelyfew pus cells. Some bronchi were distended. Thebronchial walls were infiltrated by polymorphs andmany eosinophils, the basement membrane thickenedand hyaline, and the mucous glands active. Otherorgans were normal.CASE 8: ASTHMA THE CHIEF CAUSE OF DEATH (from
the records of the Hospital for Sick Children, London).-This 2-year-old girl had had asthmatic attacks forfive months. On admission she was in an acute asthmaticattack, semi-comatose with difficult, rapid, gruntingirespirations. The face, neck, chest, and arms wereemphysematous, and air in the subcutaneous tiswnesobscured the lung fields in a radiograph. She died afew hours after admission. At necropsy the chest,
shoulders, and proximal parts of both arms werethickened and the whole face blown up; these partsfelt crepitant. In the thorax the connective tissue inthe anterior mediastinum was permeated with air fromheart to neck; there were subpleural emphysematousbullae in the left upper lobe, air in the subpleural tissuearound both hila; and in the lung there were areas ofover-inflation and of collapse. Microscopically manybronchi and bronchioles contained purulent exudate,areas of emphysema alternated with areas in whichalveoli were lined with eosinophilic material and filledwith pale-staining, oedematous fluid. The brain wascongested and other organs were normal.
CASE 9: ASTHMA THE CHIEF CAUSE OF DEATH (fromthe records of the Westminster Hospital).-This 52-year-old man had had asthma for five years and wasadmitted to hospital in a very severe attack which hadstarted that day. He was cyanosed, in acute respiratorydistress, with very poor chest expansion, and generalizedexpiratory rhonchi. His blood pressure was 124/70 mm.Hg; the cardiovascular system was normal. Oxygenand adrenaline produced no relief and he died earlynext morning. At necropsy the right lung was found tobe collapsed by a pneumothorax except at the apexwhere there were two fibrous adhesions, and the leftlung was distended by emphysema. A small tear nearone of the adhesions was thought to have been thecause of the pneumothorax. In the heart there wasright ventricular hypertrophy. Other organs werenormal.CASE 10: ASTHMA THE CHIEF CAUSE OF DEATH (from
the records of Llandough Hospital).-This 50-year-oldman had had asthma for 20 years. He was admittedto hospital in status asthmaticus and responded wellto intravenous aminophylline. Two months later hewas readmitted, cyanosed, breathless with loud expiratoryrhonchi. This time he failed to respond to amino-phylline or adrenaline and two days later becameconfused, then stuporose, and died the same day. Atnecropsy the lungs were voluminous and soft with tena-cious mucus in the bronchi. One of the major branchesof the right pulmonary artery contained a recent throm-bus. Microscopically there was squamous metaplasiaof the lining of many bronchi; in some there wasmuscular hypertrophy. Eosinophils infiltrated theepithelium and walls. The alveoli were distended, themucous glands not prominent.
CASE 11: ASTHMA THE CHIEF CAUSE OF DEATH (per-sonally observed at the Westminster Hospital).-This47-year-old man had been well until seven years beforeadmission when he developed bronchopneumoniaaccompanied by bronchospasm. Four similar episodesoccurred between the first illness and his first hospitaladmission. He was then found to have the physicalsigns ofemphysema with bronchospasm; blood pressurewas 130/80; temperature 1020 F., and respirations40 per min.; radiologically patchy consolidation ofboth lower lobes. A few days after admission hedeveloped signs of congestive heart failure with anenlarged and tender liver and moderate oedema of the
204
on July 18, 2020 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.8.3.195 on 1 Septem
ber 1953. Dow
nloaded from

FATAL BRONCHIAL ASTHMA
lower limbs. An E.C.G. showed right axis deviationand tall P waves in leads IL and III. The pneumoniaresponded slowly to sulphadimidine and the heart failureslowly subsided with digitalis and mersalyl. After twomonths he was fit for discharge and the E.C.G. hadbecome normal. The following year he had a similarattack with congestive heart failure and pulmonaryinfection, and six months later an attack of the sametype but much less severe and with no E.C.G. changes.Later that year-nine years after his first illness-hebegan to have asthmatic attacks relieved by adrenalineand partially prevented by sublingual isoprenaline;an E.C.G. at this time was normal. For six weeks hisattacks became more frequent and failed to respond toisoprenaline; he was admitted to hospital, cyanosedwith loud expiratory rhonchi but without signs of lungconsolidation or of heart failure. Adrenaline andintravenous theophylline with ethylene diamine producedsome relief; treatment was continued with continuousoxygen and four-hourly ephedrine. Early next morninghe became more dyspnoeic and semi-comatose, did notimprove with an atropine injection, and died at 8 a.m.During this admission he was apyrexial; respirations35 per min. and pulse rate rising to 115 per min. shortlybefore death. At necropsy the right lung was grosslyemphysematous with bullae along the free margin;the left felt somewhat collapsed and there was adherentpleura. Microscopically there was gross emphysemawith very early bronchopneumonic changes, no thick-ening of the muscle layer or basement membrane ofthe bronchioles, and the predominant cells were poly-morphs with very few eosinophils. The heart wasnormal. The liver was congested. Other organs werenormal.
CASE 12: ASTHMA THE CHIEF CAUSE OF DEATH (fromthe records of Graylingwell Hospital).-This 53-year-old woman was a paranoid schizophrenic who had hadasthma for 17 years. When her asthma was bad hermental symptoms improved, and, conversely, in schizo-phrenic exacerbations she was free of asthma. Whilein a mental hospital she developed a severe asthmaticattack, with great difficulty in expiration, cyanosedextremities but no fever or evidence of pulmonaryinfection or heart failure. Intermittent oxygen, andephedrine and aminophylline orally, produced tem-porarily some relief; she then improved considerablywith continuous oxygen and adrenaline but becameworse again and died two days after the onset of theattack. At necropsy the significant findings wereemphysema and bronchopneumonia; no histologicalstudies were done.
CASE 13: ASTHMA THE CHIEF CAUSE OF DEATH (per-sonally observed at the Westminster Hospital).-This62-year-old man had had two or three attacks of noc-turnal dyspnoea a week, better in summer, since anattack of bronchitis four years previously. He had hadhay fever as a child and had a sister with asthma.Ephedrine afforded relief. He attended the out-patientdepartment, as for a month the attacks had lasted
several hours every night. On examination he had aloud expiratory wheeze, basal rales, and gross emphy-sema; blood pressure was 150/100 mm. Hg. The liverwas tender 2 in. below the costal margin. There wasslight oedema of the ankles, but pulse and heart soundswere normal. Next day he went to sleep after lunch,and on waking asked the time. He had an appointmentat the hospital for 2 p.m., and on being told that itwas 3.30 p.m. fell back dead. At necropsy, the larynxwas slightly oedematous. The bronchi and trachea wereinflamed and filled with glairy, green mucopus. Bothlungs were ballooned by emphysema and microscopicallyshowed chronic emphysema with some interstitial fibrosisand collections of chronic inflammatory cells near thebronchioles. Some small bronchi were occluded bymuco-cellular exudate, but there was no sign of bronchialmuscular hypertrophy or eosinophilia. The heartshowed generalized hypertrophy only. There was grossatheroma of the aorta; and the coronary vessels, thoughatheromatous, were patent throughout. The liver wasenlarged and showed a mottling of the early " nutmeg "type. The spleen was congested and the adrenals hada curious mottled appearance on section. Micro-scopically the liver and adrenal changes were seen tobe due more to fatty change than to congestion.
CASE 14: ASTHMA THE CHIEF CAUSE OF DEATH (per-sonally observed at the Willesden General Hospital).This 65-year-old woman had had asthma between theages of 5 and 15 years and had then been free of ituntil three years previously. For 10 years she had hadwinter bronchitis. Her asthmatic attacks had respondedto adrenaline until a few weeks before admission, andshe was admitted in one which had failed to respondto several injections. On examination she was thin,dyspnoeic, and cyanosed. The chest was fixed inexpiration with accessory muscles working, loud expira-tory stridor and rhonchi in all areas. Blood pressure was210/110 mm. Hg. There was no evidence of heartfailure. She did not respond to adrenaline and threehours after admission suddenly collapsed with a weakpulse, inaudible heart sounds, deep cyanosis, andprofuse sweating, and died five minutes later. Atnecropsy both lungs were found to be very emphysema-tous and the bronchi almost completely blocked byvery tenacious mucopus adherent to the bronchial wall.Microscopically many bronchioles showed round-cellinfiltration, mucous plugs containing macrophages,desquamated bronchial epithelium and eosinophilsblocked many smaller bronchi, the walls of which wereinfiltrated by eosinophils, and eosinophils were seenin smaller numbers between the muscle layers. Theright side of the heart was dilated and slightly hyper-trophied and there was left ventricular enlargement.The aortic valves were distorted and incompetent dueto old rheumatic carditis, and the mitral valve wasslightly thickened. The coronary arteries showed earlyatheromatous changes. The abdominal viscera werenormal apart from moderate eosinophilia of the spleen.A meningioma the size of an acorn was found hangingfrom the left side of the front of the falx.
205
on July 18, 2020 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.8.3.195 on 1 Septem
ber 1953. Dow
nloaded from

B. V. EARLE
CASE 15: ASTHmA THE CHIEF CAUSE OF DEATH (fromthe records of the Hospital for Sick Children).-This2j-year-old girl had had asthma since the age of 18months. She was admitted in an attack which hadstarted 24 hours previodsly. She was dyspnoeic andcyanosed, with signs of severe bronchospasm but noneof consolidation. In spite of adrenaline she died 16hours later. At necropsy the lungs were pale anddistended; there were two areas of collapse-of half theright middle lobe and the anterior parts of the leftupper lobe, but no evidence of consolidation. Thetrachea was congested; the bronchi and bronchioleswere plugged with thick, tenacious mucopus and theirmucosae were congested. The heart and other organswere normal. Microscopically there were many eosino-phils in the mucous plugs and bronchial walls, andthere was thickening of the muscle layer of the bronchi.
I have to thank Dr. C. J. Gavey for suggesting thisinvestigation, and for his very helpful criticism; Dr.D. A. Williams for his kind help; and the medicalstaffs of the Westminster Hospital, the Hospital for SickChildren, Great Ormond Street, London, LlandoughHospital, Cardiff, the Royal Infirmary Cardiff, Gray-lingwell Hospital, Chichester, and the Willesden GeneralHospital for allowing access to case records.
REFERENCESAlexander, H. L., Luten, D., and Kountz, W. B. (1927). J. Amer.
med. Ass., 83, 882.Antoniazzi, E. (1933). Pollclinico, Sez. med., 40, 345.Benson, R. L., and Perlman, F. (1948). J. Allergy, 13, 129.Bergstrand, H. (1946). J. Path. Bact., 56, 399.Blanton, W. B., and Sutphin, A. K. (1949). Amer. J. med. Se., 217,
169.
Bru16, M., HUlemand, P., Delarue, J., and Netter, A. (1935). Bull.Soc. mdd. H6p. Paris., p. 981.
and Audoly, J. (1943). Ibid, 53, 40.Bubert, H. M., and Warner, C. Gardner(1935). J. Amer. med. Ass.,
104, 1469.Chafee, F. H., Ross, J. R., and Gunn, E. M. (1942). Ann. Intern.
Med., 17, 45.Clarke, J. A. (1930). Arch. intern. mod., 45, 624.Coke, F., and Coke, H. (1939). Asthma, p. 237. Wright, Bristol.Colton, W. A., and Ziskin, T. (1936). Med. Bull. Veterans' Adm., 13,
117.Craige, B. (1941). Arch. intern. Med., 67, 399.
Cummings, G. 0. (1946). Ann. Otol., St. Louis, 55, 136.Dehner, W. (1927). Kiln. Wschr., 6, 1412.Facquet, J., and Claisse, R. (1939). Paris mdd., 2, 113.Fowler, K. (1937). Penn. med. J., 40, 720.Gay, L. N. (1946). The Diagnosis and Treatment of Bronchial
Asthma. Bailli6re, Tindall and Cox, London.Hamburger, J., Milliez, P., and Halpern, B. (1947). Bull. Soc. mid.
H6p. Paris, 63, 432.Hansen, 0. S. (1936). Minn. Med., 19, 445.Harkavy, J. (1930). J. ilergy, 1, 136.-(1941). Arch. Intern. Med., 67, 709.Huber, H. L., and Koessler, K. K. (1922). Ibid., 30, 689.Kayssi, A. I. (1948). Brit. med. J., 2, 131.Kountz, W. B., and Alexander, H. L. (1928). Arch. Path. Lab. Med.,
S, 1003.Lamson, R. W., and Butt, E. M. (1937). J. Amer. med. Ass., 106,
1843.Lemierre, A., Leon-Kindberg, M., and L6vesque, J. (1923). Presse
mid., 31, 613.
Lennox, B. (1948). J. Path. Bact., 60, 620.Macdonald, I. G. (1933). Ann. intern. Med., 6, 253.Magee, A. V. (1949). Practitioner, 163, 134.Massachusetts General Hospital Reports (1946). Case record No.
32192. New Engl. J. Med., 233, 639.Meakins, J. C. (1944). The Practice ofMedicine, 4th edit. Kimpton,
London.Michael, P. P., and Rowe, A. H. (1935). J. Allergy, 6, 150.Mitchell, H. S., and Bacal, H. L. (1950). Canad. med. Ass. J., 63,
467.Moulis, A. (1950). J. franp. med. Chir. thorac., 4, 273.Old, H. (1933). J. Alergy, 4, 122.Peterson, H. (1947). Ibid., 16, 413.Rackemann, F. M. (1926). Boston med. surg. J., 164, 531.Riopelle, J. L. (1933). Ann. Anat. path. med.-chfr., 10, 1179.Rosenberg, J., and Rosenberg, L. (1938). Amer. J. med. Sd., 195,
682.Schwartz, B. M., Mcllroy, G. H., and Warren, H. A. (1945). Air
Surgeon's Bull., 2, 146.Schwartz, M. (1949). Lancet, 1, 1001.Serafini, U. (1950). Policlinico, Sez. prat., 57, 33.Steinberg, B., and Figley, K. D. (1928). J. Lab. clin. Med., 13, 921.Thieme, E. T., and Sheldon, J. M. (1938). J. Allergy, 246.Thomson, J. G. (1945). J Path. Bact., 57, 213.Tichenor, C. J., and Lafsky, B. P. (1947). Clin. Proc. Child. Hosp.
Wash., 3, 50.Traisman, A. S. (1941). Arch. Pediat., 56, 407.Trowbridge, M. (1944). Arch. intern. Med, 73, 460.Unger, L. (1945). Sth med. J., Bgham, Ala., 38, 513.Vance, B. M., and Strassmann, G. (1942). Arch. Path., Chicago, 34,
849.Vaughan, W. T. (1948). Practice of Allergy, 2nd edit. Kimpton,
London.Villanova, P. (1948). Presse med., 56, 828.Waldbott, G. L. (1935). Amer. J. Dis. Child., 4, 1531.Walton, C. H. A., Penner, D. W., and Wilt, J. C. (1951). Canad.
med. Ass. J., 64, 95.Williams. E. O., andWilliams, G.E. O. (1949). Brit. med. J., 2,897.Wilmer, H. B., Eiman, J., and Miller, M. M. (1936). J. Allergy, 7,
156.Wilson, K. S., and Alexander, H. L. (1947). J. Mo. med. Ass., 44,
664.Wright, C. B. (1930). J. Amer. med. Ass., 94, 1218.
206
on July 18, 2020 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.8.3.195 on 1 Septem
ber 1953. Dow
nloaded from

![Fatal asthma in a young patient with severe bronchial ... · Bronchial asthma affects 3-5% of the population [1], and deaths from asthma, although uncommon, have received increasing](https://img.pdfslide.us/doc/110x75/5f1bca2042c0327c71428671/fatal-asthma-in-a-young-patient-with-severe-bronchial-bronchial-asthma-affects.jpg)