-
8/13/2019 Fascia Pathology
1/37
FASCIA PATHOLOGY
-
8/13/2019 Fascia Pathology
2/37
Definition and anatomyThe dense connective tissue that
envelopes muscles grossly, and alsosurrounds every bundle of
musclefibers and each individual muscle cell.
This connective tissue is inextricablylinked with the muscle,
and is
continuous with the tendons andperiosteum
-
8/13/2019 Fascia Pathology
3/37
Fascia is composed of cells includingfibroblasts,macrophages
,mast cellsand extracellular matrix.
The extracellular matrix (ECM) iscomposed of ground
substance,collagen and elastin fibers.
Its richly innervated
-
8/13/2019 Fascia Pathology
4/37
Fibrosis and adhesions
One of the hallmarks of fascia is its mutability andremodeling
in response to mechanical stress.
However, under certain conditions excess
mechanical stress, inflammation or immobilitythis process can
result in excessive anddisorganized collagen and matrix
depositionresulting in fibrosis and adhesions eg in
plantarfascitis
-
8/13/2019 Fascia Pathology
5/37
What is Necrotizing Fasciitis?
life-threatening, progressive, rapidly spreading,inflammatory
infection located in the deep fascia.
infection rapidly destroy the skin and soft tissuebeneath it
Also known as: flesh-eatingbacteria.
Other names: -hemolytic streptococcal gangrene,Meleney ulcer,
acute dermal gangrene, hospitalgangrene, and necrotizing
cellulitis.
3 types of NF. Type I : a polymicrobial flora.
Type IIGroup A -Streptococcus bacteria(most common case)
Type III : marine vibrio gram-negative rods.
-
8/13/2019 Fascia Pathology
6/37
How does one contract NF?
exposed to an individual with anopeningin their skin. direct
contactwith someone carrying the
bacteria the bacterium being carried by the person
itself.
enter through weakened skin, as acontusion, a bruise, a blister,
or even an
abrasion.
-
8/13/2019 Fascia Pathology
7/37
Cofactors that Increase risks
Diabetes
Alcoholism
Immuno-suppression Severe illnesses: heart, lung, or liver
disease
Obesity
-
8/13/2019 Fascia Pathology
8/37
Whats going on inside yourbody?
Bacteria eat away at tissue between skin and muscle
Increase in sensitivity or anaesthetic feel to the skin
itself
Inflammatory response by immune system
Bacterial toxins released
Cytokines impede function of phagocytic cells
Anaerobes thrive speeding up necrotic process Endothelial cells
become damaged;
Increased permeability of the lining of vessels in the body
Poor blood supply inhibit:
Inflammatory response process
Ability for the immune system to properly work
Ability to transfer antibiotics to the affected fascial layer
Vasoconstriction and thrombosis edema hypoxia necrosis of
the fascia, skin, soft tissue, and muscles.
Additional necrosis involving the subcutaneous nerves.
-
8/13/2019 Fascia Pathology
9/37
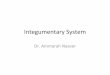
Exams and Laboratory Testing
1. Blood samples2. Testing for elevated or lowered
creatinine,glucose, CPK, bicarbonate, albumin, andcalcium
levels.
3. X-ray4. CT, and MRI scanning5. And most importantly
antibiotic culture andsensitivity tests
-
8/13/2019 Fascia Pathology
10/37
-
8/13/2019 Fascia Pathology
11/37
Symptoms
Bone pain or tenderness
Carpal tunnel syndrome
Muscle weaknessTenderness and swelling of upper and
lower limbs
Thickened skin with puckeredappearance
-
8/13/2019 Fascia Pathology
12/37
Pathology
In early disease there is oedema of thefascia and subcutaneous
tissue with alymphocytic infiltrate containingplasma cells and
eosinophils.
With time the collagen becomesthickened and sclerotic with
extension into the subcutaneousfibrous tissue
-
8/13/2019 Fascia Pathology
13/37
The tissue eosinophils may be focalaround adnexal structures or
diffusewithin the tissue infiltrate
In more extensively involved cases thechanges can extend to the
dermis
The epidermis is typically not involved,
though mild atrophy can be seen in aminority of cases
-
8/13/2019 Fascia Pathology
14/37
Tests done
Gamma globulins
ESR
MRISkin biopsy:Full thickness
-
8/13/2019 Fascia Pathology
15/37
FASCIA TUMOURS
-
8/13/2019 Fascia Pathology
16/37
NODULAR FASCITIS
Common lesion that typically presents as arapidly growing mass
on the flexorforearm, chest, back or elsewhere
Arises from superficial fascia, occasionallyintramuscular or
intravascular
Similar lesions may also develop within the
breasts, bladder,cervix, intra-articular,prostate, vagina and
vulva
-
8/13/2019 Fascia Pathology
17/37
Epidemiology:Peaks at age 40 years; priortrauma in 10% of
cases
Benign behavior, but sometimesmisdiagnosed as sarcoma based
oncellularity, mitotic figures and rapidgrowth
-
8/13/2019 Fascia Pathology
18/37
Gross
Tan-white-gray, myxoid appearance,usually 3 cm or less
(reconsiderdiagnosis if greater than 3 cm)
Nodular with poorly defined margins
May be centered in subcutis, maygrow into skeletal muscle
-
8/13/2019 Fascia Pathology
19/37
Microscopy
Zonation effect with hypocellular central regionand
hypercellular periphery
Composed of uniform, plump, immature,
spindled to stellate fibroblasts ormyofibroblasts without
atypia, with a feathery,"tissue-culture" like growth pattern due
toabundant ground substance
Often with mucoid/myxoid pools (microcysts),a very useful
diagnostic finding
Uniform elongated nuclei with punctate nucleoliand without
significant nuclear atypia
Cellular areas may have storiform or fascicularpatterns (S or C
shaped)
-
8/13/2019 Fascia Pathology
20/37
Often frequent mitotic figures (but no atypicalforms),
lymphocytes and macrophages, redblood cell extravasation, bands of
keloid-type
collagen Vasculature is usually prominent
Walls of small to medium sized vessels areinvolved by reactive
process at periphery of
lesion May infiltrate adjacent fat
May have metaplastic bone, focal cystic areas,ganglion type
cells but no cells with large,
hyperchromatic, atypical nuclei
-
8/13/2019 Fascia Pathology
21/37
Cranial fascitis
Nodular fascitis variant
Infants or children < 2 years old
Rare; usually boys
Soft tissue of scalp and underlying cranial bones
Develops from galea aponeurotica, erodes outertable of cranium
and may infiltrate dura
Some cases show dysregulation of Wnt/-catenin
pathway, suggesting a potential relationship todesmoid
fibromatosis rather than nodularfasciitis
-
8/13/2019 Fascia Pathology
22/37
May be related to birth trauma, craniectomy or bespontaneous
Congenital in a minority of cases
PainlessTypically associated with focal calvarial lytic
change at the lesional site
Grows quickly like nodular fasciitis, but same
benign behavior
-
8/13/2019 Fascia Pathology
23/37
Morphology
Gross:1-3 cm white to pink, mildly mucoid torubbery
mass,unencapsulated but wellcircumscribed
Micro:Loosely arranged broad fascicles of delicatefusiform cells
with edematous to myxoid-appearing interstitium
Nuclear atypia minimal or absent
Mitotic figures ranged from 1-5 per 10 high powerfields
No compact cellularity, no short fascicles, noregional
variations compared to nodular
fasciitis
-
8/13/2019 Fascia Pathology
24/37
Radiography
Lytic defect of skull with sclerotic rim onxray
Treatment: Surgical excision
-
8/13/2019 Fascia Pathology
25/37
Intravascular Fascitis
Variant of nodular fasciitis that involves wall andlumen of
small to medium-sized veins andarteries
Slower growth than classic nodular fasciitis butsame
behavior
Uncommon
Typically seen in 1st through 3rd decades, but can
occur at any ageSlightly more common in men
-
8/13/2019 Fascia Pathology
26/37
Most often found in upper extremity or head andneck region
Less common sites include the lower extremity
and trunkEtiology:Unclear
Conservative excision
-
8/13/2019 Fascia Pathology
27/37
Morphology
Usually 2 cm or less
Nodular or plexiform
Resembles nodular fasciitis (proliferation of plump
spindle cells in a loose "tissue culture"arrangement), but with
a less prominentmucoid matrix and numerous osteoclast-likegiant
cells
May be intra- or extravascular
-
8/13/2019 Fascia Pathology
28/37
Dupuytrens Contracture
Also known as palmar
Nodular proliferative process of palmaraponeurosis, surrounding
adipose and
occasionally dermis, due to fibroblasts,myofibroblasts and
fibrocytes
Most common type of fibromatosis (1-2% ofpopulation), prevalence
increases with age
(24% at age 65+)
-
8/13/2019 Fascia Pathology
29/37
Puckers overlying skin as it agesCauses flexion contracture of
digits 4 and 5due to cord-like expansion of digitalaponeurotic
slipsDoes not involve deep structures such astendons or skeletal
muscleMay be caused by fibrogenic cytokines
-
8/13/2019 Fascia Pathology
30/37
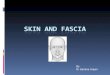
Morphology
Small nodules or nodular masses associated withaponeurosis and
subcutaneous fat, with gray-yellow-white cut surface (color depends
oncollagen content)
Proliferative phase:Uniform, plump, immature spindle
cells(myofibroblasts and fibroblasts) with blandnuclei and
indistinct nucleoliModerate collagen and elongated vessels
-
8/13/2019 Fascia Pathology
31/37
Older lesions:More dense collagen, less cellularityVariable
mitotic figuresOccasional attachment to dermis orcartilaginous
metaplasiaUsually no infiltration of surrounding tissuebeyond
subcutis
-
8/13/2019 Fascia Pathology
32/37
-
8/13/2019 Fascia Pathology
33/37
Morphology
Gross: 2-3 cm nodules associated with
aponeurosis and subcutis, with gray-yellow-white cut surface
(color depends on collagencontent)
Micro
Proliferative phase:Hypercellular collection of uniform,
plump,immature spindle cells with bland nuclei andindistinct
nucleoliModerate collagen and elongated vesselsVariable
multinucleated giant cells
-
8/13/2019 Fascia Pathology
34/37
Older lesions:Denser collagen, less cellularityOften prominent
chronic inflammation,
variable mitotic figures and hemosiderin
-
8/13/2019 Fascia Pathology
35/37
Penile fibromatosis
Also known as Peyronies disease
Fibrous thickening of dermis and Bucks fasciabetween corpora
cavernosa and tunica
albuginea, causing curvature towards side oflesion and
restricting movement of thesestructures during erection
Etiology may be related to Parc protein or Wnt2
-
8/13/2019 Fascia Pathology
36/37
Typically age 40+ years, rarely age 40 or
lessVarious etiologies (microvascular trauma ,
urethritis, sclerosing inflammatory process,idiopathic), appears
to differ from othersuperficial fibromatoses although
associatedwith themPrevalence 3-9%, associated with plaques,
pain, induration, deviation, palmar fibromatosisUsually
dorsolateral penis, 30% have
inflammatory component
-
8/13/2019 Fascia Pathology
37/37
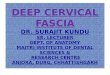
Morphology
Disorganization of collagen of tunica albugineawith formation of
nodules, often hyalinizingfibrosis, perivascular lymphocytic
infiltrate in1/3, linear band of calcification in 1/4