Embed Size (px)
Citation preview
Fascia Iliaca Blocks in acute hip fracture in the older person
TOOLKIT
ACI Pain Management Network
Collaboration. Innovation. Better Healthcare.
ACI Pain Management Network – Fascia Iliaca Blocks in acute hip fracture in the older person
The Agency for Clinical Innovation (ACI) works with clinicians, consumers and managers to design and promote better healthcare for NSW. It does this by:
• service redesign and evaluation – applying redesign methodology to assist healthcare providers and
consumers to review and improve the quality, effectiveness and efficiency of services
• specialist advice on healthcare innovation – advising on the development, evaluation and adoption of
healthcare innovations from optimal use through to disinvestment
• initiatives including Guidelines and Models of Care – developing a range of evidence-based healthcare
improvement initiatives to benefit the NSW health system
• implementation support – working with ACI Networks, consumers and healthcare providers to assist
delivery of healthcare innovations into practice across metropolitan and rural NSW
• knowledge sharing – partnering with healthcare providers to support collaboration, learning capability
and knowledge sharing on healthcare innovation and improvement
• continuous capability building – working with healthcare providers to build capability in redesign, project
management and change management through the Centre for Healthcare Redesign.
ACI Clinical Networks, Taskforces and Institutes provide a unique forum for people to collaborate across clinical
specialties and regional and service boundaries to develop successful healthcare innovations.
A priority for the ACI is identifying unwarranted variation in clinical practice and working in partnership with
healthcare providers to develop mechanisms to improve clinical practice and patient care.
www.aci.health.nsw.gov.au
AGENCY FOR CLINICAL INNOVATION
Level 4, Sage Building
67 Albert Avenue
Chatswood NSW 2067
PO Box 699 Chatswood NSW 2057
T +61 2 9464 4666 | F +61 2 9464 4728
E [email protected] | www.aci.health.nsw.gov.au
SHPN: ACI 150484
ISBN: 978-1-76000-280-0.
Produced by: ACI Pain Management Network
Further copies of this publication can be obtained from the
Agency for Clinical Innovation website at www.aci.health.nsw.gov.au
Disclaimer: Content within this publication was accurate at the time of publication. This work is copyright. It may be reproduced
in whole or part for study or training purposes subject to the inclusion of an acknowledgment of the source. It may not be
reproduced for commercial usage or sale. Reproduction for purposes other than those indicated above, requires written
permission from the Agency for Clinical Innovation.
Version: V1
Date Amended: 01/09/2015
© Agency for Clinical Innovation 2015
ACI Pain Management Network – Fascia Iliaca Blocks in acute hip fracture in the older person
St Vincent’s Hospital Pain in the Elderly Working Party members 2013 and 2014:
Associate Professor Steven Faux, Chair (Director of Rehabilitation & Pain Service)
Dr Andrew Finckh (Staff Specialist, Emergency Department)
Dr Jennifer Stevens (Visiting Anaesthetist)
Dr Elizabeth Harper (Staff Specialist, Geriatric Medicine)
Julie Gawthorne (Clinical Nurse Consultant, Emergency)
Jacqueline Jensen (Registered Nurse, Chronic Pain)
Karon McDonell (Clinical Nurse Consultant, Trauma)
Susan Welch (Pharmacist)
Thomas Jennings (Registered Nurse, Orthopaedics)
Melissa O’Brien (Quality Manager, Clinical Practice Improvement)
Dr Julia Nelson (Orthogeriatric Registrar, 2011).
Fascia Ilaica Blocks (FIB) in Acute Hip Fracture in the Older Person Steering Group committee members:
Dr Phil Corke, Chair of steering group (Anaesthetist, Concord Hospital)
Dr Laura Ahmad (Orthogeriatrician, Royal North Shore Hospital)
Dr Steven Faux (Director Rehabilitation & Pain Service, St Vincents)
Dr Gerald Wong (Anaesthetist, Royal North Shore Hospital)
Dr John Mackenzie (ACI Emergency Care Institute)
Glen Pang (Network Manager, Aged Health)
Jenni Johnson (Network Manager, Pain Management).
ACI Pain Management Network – Fascia Iliaca Blocks in acute hip fracture in the older person
Contents
Section 1 Introduction 1
1.1 Fascia Iliaca Blocks as a method of pain relief in acute hip fractures of older people 1
1.2 Background 1
1.3 Objectives 1
1.4 Training benefits 2
1.5 About the implementation toolkit 2
Section 2 Ascertain facility readiness and capability 3
Section 3 Plan 4
3.1 Allocate an executive sponsor to authorise the work 4
3.2 Identify a project lead 4
3.3 Establish a working group 4
3.4 Define the goal, objectives and scope 5
3.5 Communication plan 5
Section 4 Assess 6
4.1 Conduct an audit of current practice 6
Section 5 Operationalise 7
5.1 FIB training 7
5.2 Evaluation 7
Section 6 Further Information 8
6.1 Feedback 8
6.2 Redesign methodology 8
6.3 Links to other ACI work 8
Section 7 Acronyms 9
Section 8 Bibliography 10
Appendix 1 Pain in the elderly with hip fracture – clinical audit tool 11
Appendix 2 Elderly trauma pain guidelines – hip fracture 13
Appendix 3 Patient / carer brochure 14
Appendix 4 Fascia Iliaca Blocks for preoperative pain management in the older person with hip fracture 16
ACI Pain Management Network – Fascia Iliaca Blocks in acute hip fracture in the older person Page 1
Section 1
Introduction
In Australia, there are 17,000 hip fractures each
year. These predominantly affect older people.
Traditionally, pain relief is in the form of
opiates. Use of opiates alone or in high doses
is known to have adverse effects, such as
delirium. There is therefore a need to improve
outcomes. Reduction in opiates by use of Fascia
Iliaca Blocks (FIB) has been shown to improve
preoperative pain control.
1.1 Fascia Iliaca Blocks (FIB) as a method
of pain relief in acute hip fractures of
older people
This implementation guide has been developed on the
initiative of the St Vincent’s Hospital Acute and Chronic
Pain Services and with the guidance of an ACI Steering
Group. The objective is to provide a guide and training
materials for those centres wishing to pursue FIB as a
means of improving pain management in the care of
older people with hip fractures. The objective is to
minimise the risk of delirium and associated harm
related to unmonitored opioid prescription in the
ambulance, emergency departments and wards prior
to surgery.
1.2 Background
St Vincent’s Hospital Pain Service had begun a process
of using FIBs as the preferred method of pain
management for older people admitted with suspected
or confirmed hip fractures to minimise the incidence of
delirium and harm before and after surgery. Many
supporting tools and resources were developed as part
of this project. St Vincent’s Hospital approached the
ACI as it felt that there was relevance to other hospitals
wishing to pursue this technique, and duplication of
effort would be avoided if the materials were
supported through an ACI process.
A Steering Committee was convened and has overseen
the development of the resources to ensure alignment
with evidence, current practice, variation in service
design and staffing, and applicability across the state.
1.3 Objectives
• To provide tools and resources to enable the use of
FIB as an option in providing effective pain relief in
patients with acute hip fracture.
• To ensure patients with suspected or confirmed
acute hip fracture are provided with safe and
effective best practice preoperative pain relief.
Specifically the documentation refers to ultrasound
guided Fascia Iliaca Block (FIB) utilising an out of
plane approach.
NB: Other options or techniques for administration
of regional analgesia for fractured neck of femur,
including in-plane ultrasound guided and blind
double-pop Fascia Iliaca Block and femoral nerve
blocks, are not addressed in this documentation but
may be considered as local governance, clinical
preference and proficiency allow.
ACI Pain Management Network – Fascia Iliaca Blocks in acute hip fracture in the older person Page 2
1.4 Training benefits
The benefits of implementing FIB training include:
• reduction in adverse events or poor patient
outcomes
• reduced length of stay and less complications
related to delirium
• improved patient experience
• improved skill sets for staff involved in treating
patients with hip fractures
• improved staff satisfaction
• improved efficiencies.
Source: National Institute for Health and Care
Excellence. Hip fracture. Earlier operations and better
care can improve the lives of thousands of hip fracture
patients. Accessed on 2 July 2015 at www.nice.org.uk/
guidance/cg124/resources/earlier-operations-and-
better-care-can-improve-the-lives-of-thousands-of-hip-
fracture-patients
1.5 About the implementation toolkit
This implementation toolkit has been developed to
support the successful implementation of FIB in NSW
health facilities having the appropriate governance.
This includes competency, training, staffing,
equipment, patient volume, infrastructure and
supervision in place. www.anzca.edu.au/resources/
professional-documents
The implementation support materials provided by
the ACI and St Vincent’s Hospital Chronic Pain Service
include:
• implementation guide
• explanatory guide and notes
• video material of how to conduct the procedures
• competency and training materials
• audit tool
• patient and carer information brochure.
The toolkit outlines the following steps to implement
FIB in your facility:
• ascertain facility readiness
• plan
• assess
• operationalise
• evaluate.
ACI Pain Management Network – Fascia Iliaca Blocks in acute hip fracture in the older person Page 3
Section 2
Ascertain facility readiness and capability
A review of local governance and service
structure will be necessary to consider whether
the service has the capacity to provide
adequate clinical competence, supervision and
training to safely carry out the procedure on a
routine basis.
A review of the volume of patients and outcome
presenting with hip fracture attended by the service
may be useful to inform the local governance review.

ACI Pain Management Network – Fascia Iliaca Blocks in acute hip fracture in the older person Page 4
Section 3
Plan
Purpose
The purpose of the project planning phase
is to:
• obtain local sponsorship to support the
implementation of FIB
• define the key members of a project team
and working group
• set a clear goal, objectives and scope.
3.1 Allocate an executive sponsor to authorise
the work
It is essential to identify a member of the local health
district (LHD) executive as the project sponsor. This
should preferably be the director of clinical governance.
A clinical lead also needs to be identified. This could be
the head of the anaesthetic or emergency department,
a nominated anaesthetist, emergency physician or
other critical care specialist or a nurse educator.
The role of project sponsor and clinical lead is not just
to support the project, but to:
• determine and monitor progress and outcomes
• support and promote cultural change
• provide visible and active leadership and
commitment to the project with all levels of staff
• align the goals and objectives of the project at
executive and strategic level to the hospital and
LHD operational plans
• assess, monitor and manage risks associated with
implementation and assist in resolving issues and
barriers escalated by the project manager or
working group.
3.2 Identify a project lead
It is recommended that for the implementation period,
a member of the team is allocated the role of project
lead. The project lead will:
• lead the implementation
• facilitate meetings
• effectively communicate with and engage staff
and clinicians in the project
• evaluate the process, communicate and monitor
outcomes
• escalate ongoing implementation issues to the
executive sponsor.
3.3 Establish a working group
It is recommended that the working group is
multidisciplinary and represents clinical and non-clinical
teams that care for patients undergoing FIB procedures.
Where possible, the working group should include
membership from affected specialty departments.
Representatives should include:
• physicians in emergency medicine
• physicians in geriatric medicine
• pain management specialists
• anaesthesists
• consumers
• nurse educators, clinical nurse consultants
or educators
• pharmacists.
ACI Pain Management Network – Fascia Iliaca Blocks in acute hip fracture in the older person Page 5
In rural areas, representatives can include:
• general practitioners
• nurse managers or nurse educators
• clinical nurse consultant (CNC)
• pharmacists
• consumers
• specialists in fields such as geriatrics, orthopaedics
or anaesthetics as available.
Clinical governance professionals and managers should
also be involved as appropriate and available. Both
nursing and medical staff should be represented.
The role of the working group is to:
• execute the implementation ensuring that agreed
actions and project milestones are delivered
• effectively communicate and engage staff and
clinicians in the project
• develop local solutions as needed
• monitor and evaluate project outcomes.
3.4 Define the goal, objectives and scope
A clear project goal, specific project objectives and a
well-defined scope are important to ensure that
members of the project team are working towards the
same goal. As the project team is likely to include
multiple specialty groups, it is important that the
project goal, objectives and scope are agreed up-front
by all members of the working group.
3.5 Communication plan
Well-planned communications with staff and
stakeholders within the LHD will be essential to the
success of the project. Planning includes:
• developing consistent key messages
• identifying and targeting communications to
specific stakeholders
• scheduling communications to align with key time
points during your project
• ensuring that feedback loops are in place for
all communication.
ACI Pain Management Network – Fascia Iliaca Blocks in acute hip fracture in the older person Page 6
Section 4
Assess
Purpose
The purpose of the assessment phase is to
collect and analyse data about current
processes for the provision of FIB.
4.1 Conduct an audit of current practice
Collecting baseline data allows the service to identify
the key issues or gaps in current practice.
Understanding the current context will allow the
service to identify where improvements can be made.
• Determine the service’s baseline measures and
outcomes pre-implementation; for example,
conduct an audit of roughly 20% of the elderly hip
fracture population (see Appendix 1 for example of
an audit form).
• Identify and prioritise issues raised through the
audit and other measures.
• Review local policy and modify to ensure
consistency with protocol.
ACI Pain Management Network – Fascia Iliaca Blocks in acute hip fracture in the older person Page 7
Section 5
Operationalise
5.1 FIB training
Adopt a ‘train the trainer’ approach, using the
competency documents, resources, training video and
checklists attached as a framework. The working group
may wish to modify or add additional items to meet
local governance arrangements. Identify key champions
such as an emergency department physician,
anaesthetist or nurse educator to oversee the
training process.
Contact St Vincent’s Hospital Pain Service if there is a
need to access training off site.
5.2 Evaluation
The purpose of evaluation is to assess the success of the
implementation of the FIB protocol. It is important to
measure the outcomes of your project to:
• determine if there has been any improvement in
practice
• identify any solutions that are not working and
require reassessment
• satisfy accountability requirements
• enable more informed decisions in regards to
future improvement planning.
Evaluation measures, such as audits, patient satisfaction
and outcome measures should be considered during
the project development and aligned to the project
aims. They are critical to measuring success. Clear
and measurable objectives will help clarify what is
to be evaluated.
Reassess your performance
During the baseline assessment phase, data will have
been collected through a number of methods.
Repeating this assessment after implementation and
for the purposes of ongoing monitoring will allow you
to measure change or improvements in practice.
Sustainable implementation
Remember that the implementation project end date is
not really the end.
The project manager or working group should plan to
review the provision of FIB at regular intervals. This may
be quarterly, half-yearly or yearly depending on the
extent of changes that occurred during the
implementation project.
Communicate your success
By this point in the implementation project, many staff
and other stakeholders will be familiar with the project
and may have contributed to it in some way.
It is important to recognise and celebrate the
contribution of the project manager, working group,
staff and the stakeholders involved in the
implementation at your site. Communicate the
outcomes of the reassessment, particularly if there is
significant improvement.
ACI Pain Management Network – Fascia Iliaca Blocks in acute hip fracture in the older person Page 8
Section 6
Further information
6.1 Feedback
If you have feedback about the resources and materials,
please provide it via Appendix 4 to aci-web@health.
nsw.gov.au
6.2 Redesign methodology
For further information about redesign methodology,
see the ACI Centre for Healthcare Redesign www.aci.
health.nsw.gov.au/centre-for-healthcare-redesign
The e-Learning platform Gem contains valuable
modules on the fundamentals of project management
including redesign methodology and accelerating
implementation methodology (AIM).
Redesign methodology tools are designed to provide
access to flexible learning opportunities. Modules and
assessments can be completed at each individual’s own
pace and at a time that suits them.
The online e-learning modules are available to all NSW
Health employees statewide, who can register
themselves at gem.workstar.com.au
6.3 Links to other ACI work
Minimum standards for the management of hip
fracture in the older person
These guidelines identify best practice for the
management and care of patients with hip fractures for
healthcare providers across NSW. They aim to improve
outcomes for patients with hip fractures requiring
surgery and management in the state. www.aci.health.
nsw.gov.au/networks/aged-health/min-standards-hip-
fractures
Key principles for care of confused hospitalised
older persons
The Care of Confused Hospitalised Older Persons
Program aims to improve the early identification and
management of older people with confusion in
hospital. Patients who experience greater pain are at
higher risk of delirium and depression. Early
identification of confusion, treatment of the underlying
cause and management of symptoms can prevent these
adverse effects and minimise their duration and
severity. www.aci.health.nsw.gov.au/chops
ACI Pain Management Network – Fascia Iliaca Blocks in acute hip fracture in the older person Page 9
Section 7
Acronyms
Abbreviation Description
ACI Agency for Clinical Innovation
AIM accelerating implementation
methodology
ECG electrocardiogram
ED emergency department
GP general practitioner
CIN clinical initiatives nurse
CNC clinical nurse consultant
FIB Fascia Iliaca Block
GP general practitioner
IV intravenous
LHD local health district
MRN medical record number
NSW New South Wales
PRN when necessary (lit. pro re nata)
VMO visiting medical officer
VNRS Verbal Numerical Rating Scale
ACI Pain Management Network – Fascia Iliaca Blocks in acute hip fracture in the older person Page 10
Abou-Setta AM, Beaupre LA, Rashiq S et al. Comparative
effectiveness of pain management interventions for hip
fracture: a systematic review. Annals of Internal Medicine,
2011;155:234–245, accessed on 29 June 2015.
Agency for Clinical Innovation. Care of confused hospitalised
older persons. Accessed on 29 June 2015 at www.aci.health.
nsw.gov.au/chops
Agency for Clinical Innovation. Minimum standards for the
management of hip fractures. Accessed 29 June 2015 at
www.aci.health.nsw.gov.au/networks/aged-health/min-
standards-hip-fractures
Agency for Clinical Innovation. Orthogeriatric model of care
– clinical practice guide, 2010. Accessed on 29 June 2015 at
www.aci.health.nsw.gov.au/__data/assets/pdf_file/0013/153400/
aci_orthogeriatrics_clinical_practice_guide.pdf
Australian and New Zealand College of Anaesthetists.
Guidelines for the management of major regional analgesia,
2014. Accessed on 29 June 2015 at www.anzca.edu.au/
resources/professional-documents/pdfs/ps03-2014-guidelines-
for-the-management-of-major-regional-analgesia.pdf
Australian and New Zealand College of Anaesthetists.
Guidelines on infection control in anaesthesia, 2015. Accessed
on 29 June 2015 at www.anzca.edu.au/resources/
professional-documents/pdfs/ps28-2015-guidelines-on-
infection-control-in-anaesthesia.pdf
Australian and New Zealand Hip Fracture Registry Steering
Group. Australian and New Zealand guideline for hip fracture
care: Improving outcomes in hip fracture management of
adults, September 2014. Accessed on 29 June 2015 at
www.anzhfr.org/images/resources/Guidelines/ANZ%20
Guideline%20for%20Hip%20Fracture%20Care.pdf
Australian Commission on Safety and Quality in Health Care.
National safety and quality health service standards,
September 2012. Accessed on 29 June 2015 at www.
safetyandquality.gov.au/wp-content/uploads/2011/09/
NSQHS-Standards-Sept-2012.pdf
Mak JCS, Cameron ID, March LM. Evidence-based guidelines
for the management of hip fractures in older persons: an
update. Med J Aust. 2010;192(1): 37-41, accessed on 29 June 2015.
Section 8
Bibliography
National Health and Medical Research Council. Emergency
care acute pain management manual, 2011. Accessed on 29
June 2015 at www.nhmrc.gov.au/guidelines-publications/
cp135
National Institute for Health and Care Excellence.
Earlier operations and better care can improve the lives of
thousands of hip fracture patients. Accessed on 29 June 2015
at www.nice.org.uk/guidance/cg124/resources/earlier-
operations-and-better-care-can-improve-the-lives-of-
thousands-of-hip-fracture-patients
National Institute for Health and Clinical Excellence.
Hip fracture: evidence update March 2013: A summary of
selected new evidence relevant to NICE clinical guideline 124
‘The management of hip fracture in adults’, 2011. Accessed
on 29 June 2015 at arms.evidence.nhs.uk/resources/
hub/946207/attachment
Neuraxiom.com. Ultrasound guided regional nerve blocks.
Fascia iliaca compartment block. Accessed on I July 2015 at
www.neuraxiom.com/html/ficb.html
NHS Institute for Innovation and Improvement.
Fractured neck of femur facts. Retrieved on 05/03/2013 from
www.institute.nhs.uk/quality_and_value/high_volume_care/
fractured_neck_of_femur_facts.html
Rat P, Jouve E, Pickering G, Donnarel L, Nguyen L, Michel M,
Capriz-Ribière F, Lefebvre-Chapiro S, Gauquelin F, Bonin-
Guillaume S. Validation of an acute pain-behavior scale for
older persons with inability to communicate verbally:
Algoplus(R). Eur J Pain. 2011 Feb;15(2):198.e1-198.
dx.doi.org/10.1016/j.ejpain.2010.06.012
Scott DM, Chuan AC. Regional anesthesia: Blocks of the head,
upper and lower extremities and para-axial region,
Interactive desktop guide, 2nd ed. Accessed on 29 June 2015
at members.iinet.net.au/~achuan01/
AnaesthesiaDesktopGuide.pdf
ACI Pain Management Network – Fascia Iliaca Blocks in acute hip fracture in the older person Page 11
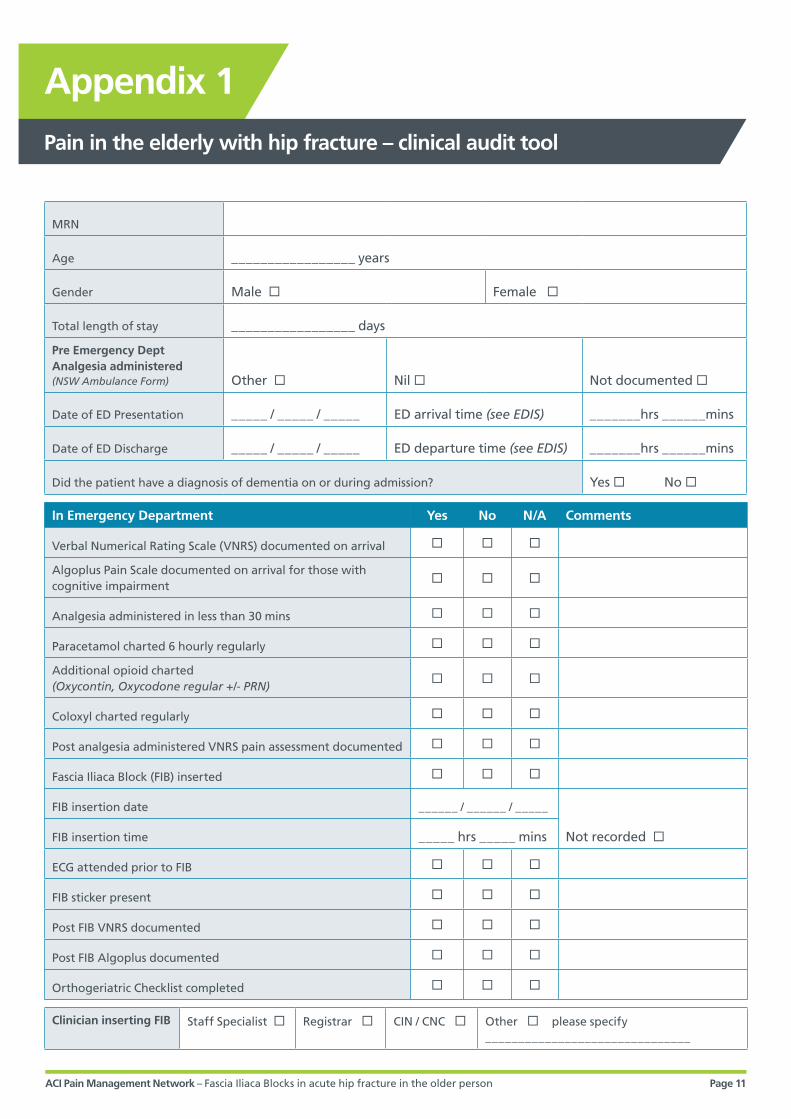
Appendix 1
Pain in the elderly with hip fracture – clinical audit tool
MRN
Age _________________ years
Gender Male Female
Total length of stay _________________ days
Pre Emergency DeptAnalgesia administered(NSW Ambulance Form) Other Nil Not documented
Date of ED Presentation _____ / _____ / _____ ED arrival time (see EDIS) _______hrs ______mins
Date of ED Discharge _____ / _____ / _____ ED departure time (see EDIS) _______hrs ______mins
Did the patient have a diagnosis of dementia on or during admission? Yes No
In Emergency Department Yes No N/A Comments
Verbal Numerical Rating Scale (VNRS) documented on arrival
Algoplus Pain Scale documented on arrival for those with cognitive impairment
Analgesia administered in less than 30 mins
Paracetamol charted 6 hourly regularly
Additional opioid charted (Oxycontin, Oxycodone regular +/- PRN)
Coloxyl charted regularly
Post analgesia administered VNRS pain assessment documented
Fascia Iliaca Block (FIB) inserted
FIB insertion date ______ / ______ / _____
Not recorded FIB insertion time _____ hrs _____ mins
ECG attended prior to FIB
FIB sticker present
Post FIB VNRS documented
Post FIB Algoplus documented
Orthogeriatric Checklist completed
Clinician inserting FIB Staff Specialist Registrar CIN / CNC Other please specify _______________________________
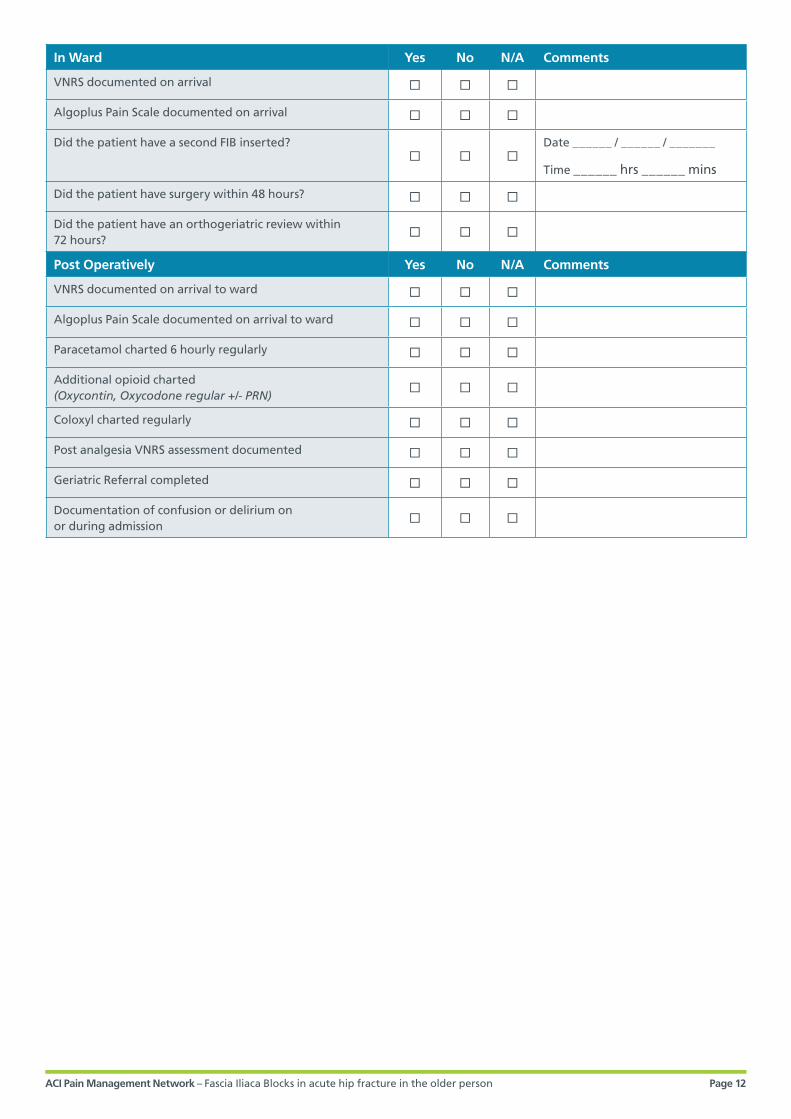
ACI Pain Management Network – Fascia Iliaca Blocks in acute hip fracture in the older person Page 12
In Ward Yes No N/A Comments
VNRS documented on arrival
Algoplus Pain Scale documented on arrival
Did the patient have a second FIB inserted?
Date ______ / ______ / _______
Time ______ hrs ______ mins
Did the patient have surgery within 48 hours?
Did the patient have an orthogeriatric review within 72 hours?
Post Operatively Yes No N/A Comments
VNRS documented on arrival to ward
Algoplus Pain Scale documented on arrival to ward
Paracetamol charted 6 hourly regularly
Additional opioid charted(Oxycontin, Oxycodone regular +/- PRN)
Coloxyl charted regularly
Post analgesia VNRS assessment documented
Geriatric Referral completed
Documentation of confusion or delirium on or during admission
ACI Pain Management Network – Fascia Iliaca Blocks in acute hip fracture in the older person Page 13
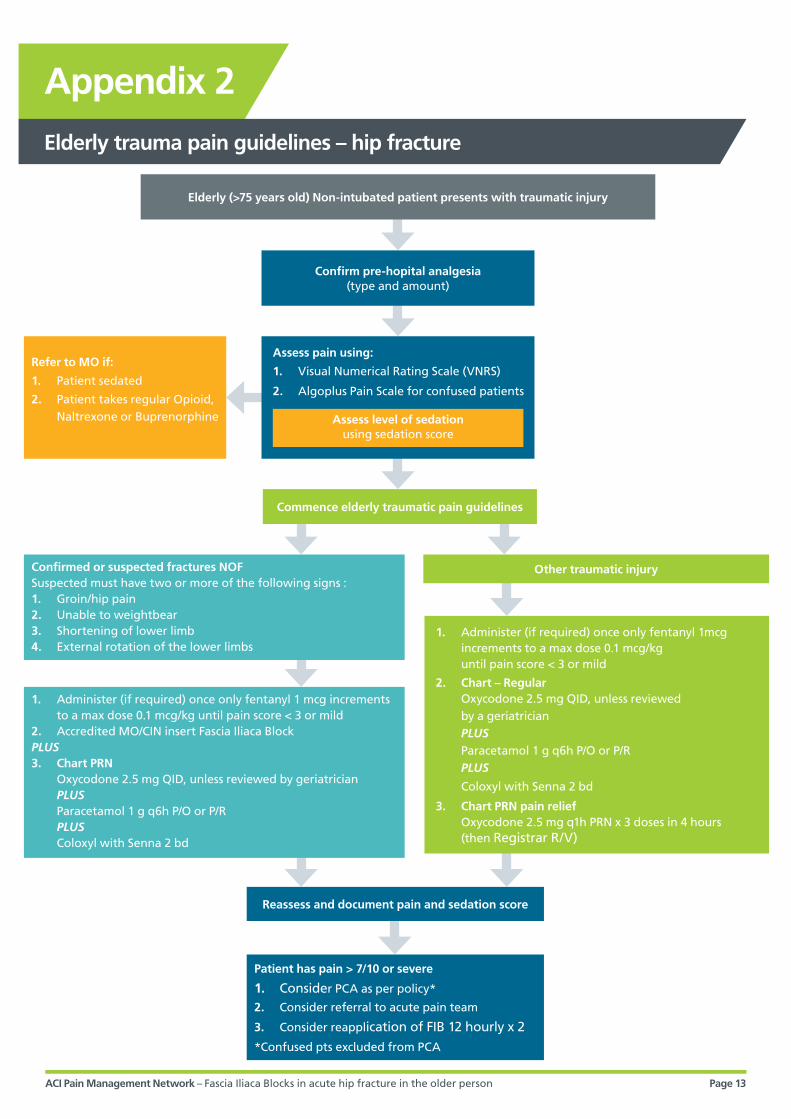
Appendix 2
Elderly trauma pain guidelines – hip fracture
Confirm pre-hopital analgesia (type and amount)
Reassess and document pain and sedation score
Patient has pain > 7/10 or severe
1. Consider PCA as per policy*
2. Consider referral to acute pain team
3. Consider reapplication of FIB 12 hourly x 2
*Confused pts excluded from PCA
Assess pain using:
1. Visual Numerical Rating Scale (VNRS)
2. Algoplus Pain Scale for confused patients
Confirmed or suspected fractures NOFSuspected must have two or more of the following signs :1. Groin/hip pain2. Unable to weightbear3. Shortening of lower limb4. External rotation of the lower limbs
1. Administer (if required) once only fentanyl 1 mcg increments to a max dose 0.1 mcg/kg until pain score < 3 or mild
2. Accredited MO/CIN insert Fascia Iliaca BlockPLUS3. Chart PRN
Oxycodone 2.5 mg QID, unless reviewed by geriatrician PLUS Paracetamol 1 g q6h P/O or P/R PLUS Coloxyl with Senna 2 bd
1. Administer (if required) once only fentanyl 1mcg increments to a max dose 0.1 mcg/kg until pain score < 3 or mild
2. Chart – Regular Oxycodone 2.5 mg QID, unless reviewed by a geriatrician PLUS Paracetamol 1 g q6h P/O or P/R PLUS
Coloxyl with Senna 2 bd
3. Chart PRN pain relief Oxycodone 2.5 mg q1h PRN x 3 doses in 4 hours (then Registrar R/V)
Elderly (>75 years old) Non-intubated patient presents with traumatic injury
Commence elderly traumatic pain guidelines
Other traumatic injury
Refer to MO if:
1. Patient sedated
2. Patient takes regular Opioid, Naltrexone or Buprenorphine Assess level of sedation
using sedation score
ACI Pain Management Network – Fascia Iliaca Blocks in acute hip fracture in the older person Page 14
Appendix 3
Patient / carer brochure
ACI Gastroenterology and Nutrion Network – A Clinician’s Guide: Caring for people with gastrostomy tubes and devices – FAQ Page 1Collaboration. Innovation. Better Healthcare. September 2015
What is a Fascia Iliaca Block?
This is an injection given near your hip that numbs the
nerves in the hip and thigh. If you have a broken hip,
it should give you pain relief for up to 12 hours. This
injection can be given while you are awake.
How is it given?
A doctor or nurse trained in giving the injection will
ask you to lie on your back so that the groin area on
the side of your broken hip can be accessed.
The skin on your groin will be cleaned (this may feel
a bit cold) and you will then have a small injection to
numb the skin.
A deeper second injection will then numb the nerves.
Is it painful?
The first injection to the skin will sting for a few
moments but this will make the area numb so that the
doctor or nurse can put the second needle in with
minimal discomfort.
The whole procedure should not be painful but it can
be uncomfortable. If you feel pain, you should let the
doctor or nurse know.
How long does it take before the injection
starts to work?
It usually takes 30 minutes for the injection to work, but
every patient is different.
What are the benefits of a Fascia Iliaca Block?
The block provides pain relief to the area of the
fracture, reducing the need for other strong drugs
which can have side effects such as sickness, drowsiness
and chest problems.
This leaflet gives patients and their carers information about the benefits and risks of fascia
iliaca block to help them make an informed decision about undergoing this procedure.
FREQUENTLY ASKED QUESTIONS
Fascia Iliaca Block: Treating and managing pain for patients with hip fractures
ACI Pain Management Network
ACI Pain Management Network – Fascia Iliaca Blocks in acute hip fracture in the older person Page 15
ACI Pain Management Network – Fascia Iliaca Block: Treating and managing pain for patients with hip fractures – FAQ Page 2
What if I do not want to have the injection?
If you choose not to have the injection, you will be
given alternative pain relief for your broken hip until
you have surgery.
Are there any side effects with a Fascia
Iliaca Block?
Side effects are very rare but may include:
• not enough pain relief – the injection
may not work
• temporary leg weakness
• infection
• reaction to the drugs
• bleeding
• nerve damage
• absorption of the anaesthetic into the blood
stream, which in turn may cause you to:
| feel unwell
| feel light-headed
| have a tingling or numbness of the lips
| feel drowsy
| have fits.
If you get any of the above symptoms, including pain at
the site of injection, please let the doctors or nurses
know as soon as possible.
Should you have any questions that this leaflet does not
answer, please ask your nurse, doctor or any member of
the healthcare team.
Adapted from NHS Nottingham University Hospital,
Fascia iliaca compartment block: alternative pain relief
for patients with a hip fracture brochure, 2012.
With thanks to Acute and Chronic Pain Services,
Department of Pain Medicine, St Vincent’s Hospital.
Pain Management Network
NSW Agency for Clinical Innovation
Level 4, Sage Building, 67 Albert Ave, Chatswood
Tel 02 9464 4636 | Fax 02 9464 4728
www.aci.health.nsw.gov.au/chronic-pain
If you are taking warfarin or have a
known blood clotting disorder, this
injection is not suitable for you.
If you have forgotten to let doctors
and nurses know, please tell them
as soon as possible.
Important note

ACI Pain Management Network – Fascia Iliaca Blocks in acute hip fracture in the older person Page 16
Appendix 4
Fascia Iliaca Blocks for preoperative pain management in the older person with hip fracture
The Agency for Clinical Innovation has worked with expert clinicians in NSW to develop a toolkit and guideline
to implement Fascia Iliaca Blocks in acute hip fracture in the older person where appropriate. The objective of
the toolkit is to provide guidelines and training materials to implement best practice in the Emergency Department
in relation to pain management in the care of the older person with hip fracture, thus minimising the risk of
delirium and/or harm related to unmonitored opioid prescription in the ambulance, Emergency Department or
ward prior to surgery.
We welcome ongoing feedback on the toolkit using the form below. If you have any questions regarding any of
the information, please contact: Jenni Johnson, Network Manager, Chronic Pain, ACI, Ph: 02 9464 4636
Email: [email protected]
Contact details
Name:
Email:
Phone:
Role/Position:
Organisation:
Specific feedback:
Document/resource Section no./Page no.
Comments
Implementation Toolkit including: • training framework• patient brochure• stickers• competency process and
assessment• log book
Clinical Guideline
Flow chart
Audit tool
General comments:



![Original Article The effect of the fascia iliaca ...636 Int J Clin Exp Med 2020;13(2):634-643 performed by the same anesthesiologist [16]. Under ultrasound guidance, the ultrasound](https://img.pdfslide.us/doc/110x75/60ab9496acee4255e94349e9/original-article-the-effect-of-the-fascia-iliaca-636-int-j-clin-exp-med-2020132634-643.jpg)













![The Role of Fascia Iliaca Compartment Block in Total Hip ...surgery for fractured neck of femur [19]. In this study, pain reduction proved greater with FNB, regardless of factors such](https://img.pdfslide.us/doc/110x75/60e251b9e3002324cf7d7f85/the-role-of-fascia-iliaca-compartment-block-in-total-hip-surgery-for-fractured.jpg)











