Embed Size (px)
Citation preview

CHIEF NURSE EXECUTIVE MEETING
FAR NORTH CALIFORNIA NURSE LEADERS
Thursday, September 24, 2015 11:00 a.m. – 2:00 PM
Enloe Medical Center
Planetree Room, Conference Building 1530 Esplanade | Chico, CA 95926
____________________________________________________
OUR MISSION
The Hospital Council of Northern and Central California’s Mission is to help our members to provide high quality health care and to improve the health status of
the communities they serve.
“Effective, Efficient, Safe, Timely, Patient Centered, Equitable and Affordable.”
OUR VISION
The vision of the Hospital Council is to be the premier healthcare association by providing leadership for change and expertise on issues affecting
the delivery of health care services.
____________________________________________________

Agenda September 24, 2015
Hospital Council Chief Nurse Executive Meeting
ii
AGENDA TIME ITEM SUBJECT ATTACHMENT PAGE 11:00 AM A. WELCOME / INTRODUCTIONS
Connie Rowe, VP Patient Care Services, Enloe Medical Center, Meeting Chair and Host Suzanne Ness, Regional Vice President, Hospital Council of Northern & Central California
A. Far North CA Nurse Leaders 2015 Roster
A
1
11:10 AM B. Sherie Ambrose, Vice President, Patient Care Services,
Mercy Mt. Shasta, Palliative Care (phone-in) Lisa Hubbard, Director , Quality, Risk, Medical Staff and OB | CNO Leadership Development Program Participant
B.1. Palliative Care Updates B.2. Palliative Care for the Seriously Ill B.3. ELNEC Summit Jan. 2016
B.1 B.2 B-3
6 14 24
11:40 AM C. Patricia Blaisdell, CHA, Vice President,
Continuum of Care (Phone-in)
C.1. California Hospital Association Case Management Committee
C.1
40
- What is the role of post-acute care providers (IRF, SNF, LTCH, HHA) in a hospital/health systems’ preparation for Health Care Reform?
- What special expertise/skills do post-acute care providers have that can support a hospital/health systems’ preparation for Health Care Reform?
- How can the Center for Post-Acute Care support and participate in this process?
C.2.A End of Life Options Information and Counseling
(AFL 14-27-AB 2139 Statutes of 2014) C.2.B Unrepresented Patients
C.2.A
C.2.B
44
47 11:55 AM D. Networking Lunch

Agenda September 24, 2015
Hospital Council Chief Nurse Executive Meeting
iii
AGENDA TIME ITEM SUBJECT ATTACHMENT PAGE 12:30 PM E. BJ Bartleson, Vice President, Nursing and Clinical Services,
California Hospital Association E.1. Legislative Update E.2. Nursing Practice - CHA CNO Advisory Group - Health Impact Values in Nursing Workgroup E.3. BRN Challenges E.4. Paramedic Pilot/Alternate Destination E.5. CHA Center for Behavioral Health/Emergency Medical Services (EMS) Workgroup E.6. Emergency Department Inaugural Forum, 12/9 E.7. Sterile Compounding and Medical Safety Tools E.8. Controlled Substance Utilization Review and Evaluation (CURES) E.9. CDPH - Licensing & Certification Program Evaluation - Remediation Work Plan E.10 Health Homes E.10. A. CHA Letter E.10. B. DHCS Concept Paper E.10. C. Health Homes for Patients with Complex Needs
E.1
E.8 A/B
E.9. A/B/C
E. 10.A/B/C
51
59
65
147
1:15 PM F. Jenna Fischer, Quality Improvement and Patient
Safety, Hospital Council F.1. Maternity Care Improvement F.2. HCAHPS Improvement F.3. Safe Table Forums F.4. Patient Safety First Initiative F.5. HQI Annual Meeting F.6. LEAD ACADEMY
F.5/6
188
1:30 PM G. Linda Riggle and Coleen Petersen, Butte-Glenn Career
Pathway Consortium (BGCPC) G.1. High School Health Career Pathway/Workforce Development
Suzanne Ness, Regional Vice President, Hospital Council of Northern and Central California
G.2 California Career Pathways Initiative/Workforce Development G.2. A. Healthcare Workforce Survey
G.2.A
196

Agenda September 24, 2015
Hospital Council Chief Nurse Executive Meeting
iv
AGENDA TIME ITEM SUBJECT ATTACHMENT PAGE 1:45 PM H. Neal Cline, RN, JD, CRFN, Community Paramedicine Project
Manager, Butte County EMS | STEMI and Prehospital Care, Enloe Medical Center, Enloe Medical Center Paramedicine Pilot
H.1. Health Workshop Pilot Projects H.2. Butte County Community Paramedic Team H.3. Community Paramedicine Fact Sheet
H.1 H.2 H.3
206 209 211
I. Adjourn J. Additional Attachments J.1 OADN/ANA Joint Position Statement on Academic
Progression to Meet the Needs of the Registered Nurse, the Health Care Consumer, and the U.S. Health Care System J.2 See Where California Heroin Opioid Problems Are Worst
J.1
J.2
217
226
2015 IMPORTANT DATES – MARK YOUR CALENDARS – Register!
Join us for the 2015 Hospital Quality Institute Conference to achieve ever increasing higher levels of performance, through a culture of respect and professionalism. Learn strategies and tools for achieving reliable care and delivering value to each
patient, each time, and in each community. The content, interactive learning and networking opportunities are not to be missed.
November 11, 2015 - 1:00pm - November 13, 2015 - 12:15pm Lisa Brundage O'Connell Jenna Fischer, CPPS
http://www.hospitalcouncil.net/overview/2015-hospital-quality-institute-conference

ATTACHMENT A
1
1

FAR NORTH CALIFORNIA NURSE LEADERS Banner Lassen Medical Center Kathy Virgil-Belding, Chief Nursing Officer 1800 Spring Ridge Dr. Susanville, CA 96130 Phone: 530-252-2234 Fax: 530-252-2241 [email protected] Assistant: Lori Griffith [email protected] Melanie Glaze, RN Sr. Mgr. Patient Care Services Phone: 530-252-2244 [email protected] Colusa Regional Medical Center Katherine Hughes, Chief Nursing Officer 199 East Webster Street Colusa, CA 95932-2954 Phone: 530-458-5821 ext 346 Fax: 530-458-3210 [email protected] Assistant: Shaun Adams, ext 373 [email protected] Eastern Plumas Health Care District April Fox, RNC, MSN BSN, Chief Nursing Officer 500 First Street Portola, CA 96122 Phone: 530-832-6509 Fax: 530-832-4494 [email protected] Enloe Medical Center Connie Rowe, Vice President, Nursing Services 1531 Esplanade Chico, CA 95926 Phone: 530-332-7815 Fax: 530-899-2067 [email protected] Assistant: Beth Jenkins Phone: 530-332-7156 [email protected]
Fairchild Medical Center Susan Westphal, RN, Chief Nursing Officer 444 Bruce Street Yreka, CA 96097 Phone: 530-841-6286 Fax: 530-841-0913 [email protected] Feather River Hospital Jackie Fullerton, Vice President Patient Care Services 5974 Pentz Road Paradise, CA 95969 Phone: 530-877-9361 X8011 Fax: 530-876-2160 [email protected] Assistant: Alice Aguilar [email protected] Glenn Medical Center Veena Vangari, Chief Nursing Officer 1133 West Sycamore Street Willows, CA 95988 Phone: 530-934-1817 Fax: 530-934-1818 [email protected] Mayers Memorial Hospital Sherry Wilson, Chief Nursing Officer 43563 State Highway 299 East Fall River Mills, CA 96028 Phone: 530-336-5511 ext. 1131 Fax: 530-336-6199 [email protected] Assistant: Jeanette Rodriguez [email protected] Theresa Overton, Acute Nurse Manager Phone: 530-336-5511 x 1242 [email protected]
2
2

Mercy Medical Center - Mt. Shasta Sherie Ambrose, VP, Patient Care Services/CNE 914 Pine Street Mt. Shasta, CA 96067 Phone: 530-926-9348 Fax: 530-926-0517 [email protected] Assistant: Colleen Bring [email protected] Mercy Medical Center - Redding Kimberly Shaw, Vice President, Patient Care Services/CNE 2175 Rosaline Avenue Redding, CA 96049-6009 Phone: 530-225-6164 Fax: 530-242-6125 [email protected] Assistant: Jill Belk 530-225-6119 [email protected] Modoc Medical Center Michele McQuillan, Chief Nursing Officer 228 W. McDowell Avenue Alturas, CA 96101 Phone: 530-233-7031 Fax: 530-233-5022 E-mail: [email protected] Assistant: Christine Nelson 530-233-7031 [email protected] Susan Sauerheber, Nursing Supervisor Phone: (530) 233-7031 [email protected] Orchard Hospital Tracy Atkins, Chief Nursing Officer 240 Spruce Street / Post Office Box 97 Gridley, CA 95948 Phone: 530-846-9045 Fax: 530-846-9027 [email protected]
Oroville Hospital Carol Speer-Smith, Chapter President Vice President, Nursing 2767 Olive Highway Oroville, CA 95966 Phone: 530-532-8404 Fax: 530-532-8433 [email protected] Assistant: Heather Corbaley 530-532-8401 [email protected] Patients Hospital of Redding Diane Rieke, Director, Patient Care Services 2900 Eureka Way Redding, CA 96001 Phone: 530-225-8700 X201 Fax: 530-225-8719 [email protected] Plumas District Hospital Lisette Brown, Chief Clinical Officer 1065 Bucks Lake Road Quincy, CA 95971 Phone: 530-283-7949 Fax: 530-283-7953 [email protected] Seneca Healthcare District Karen Turner, Director of Nursing 130 Brentwood Drive, P.O. Box 737 Chester, CA 96020 Phone: 530-258-2000 Fax: 530-258-3104 [email protected] Assistant: Monteil Ackley 530-258-3887 [email protected] Shasta Regional Medical Center Leslie Woodson, Chief Nursing Officer 1100 Butte Street Redding, CA 96001 Phone: 530-244-2844 Fax: 530-244-5119 [email protected] Assistant: Lisa Drakos 530-244-5454 [email protected]
3
3

St. Elizabeth Community Hospital Joanne Heffner, Vice President – Patient Care Services 2550 Sister Mary Columba Drive Red Bluff, CA 96080 Phone: 530-529-8020 Fax: 530-529-8009 [email protected]. Assistant: Jeri Cairns [email protected] Nancy Shilts, Director Phone: 530-529-8029 [email protected] Penny Costa, Sr. Director of Patient Care Services Phone: 530-529-8305 Pager: 530-528-6563 [email protected] Surprise Valley Health Care District Chris Gibson, Director of Nursing Main & Washington Streets Post Office Box 246 Cedarville, CA 96104 Phone: 530-279-6111 ext. 249 Fax: 530-279-2680 [email protected] Trinity Hospital Judy Nordlund, Director of Nursing 60 Easter Avenue Weaverville, CA 96093 Phone: 530-623-5541x3251 Fax: 530-623-8698 [email protected] Vibra Hospital of Northern California Lisa Stevens, Chief Nursing Officer 2801 Eureka Way Redding, CA 96003 Phone: 530-246-9000 E-mail: [email protected] Assistant: Lisa Mickelsen E-mail: [email protected]
North State Nursing Programs Denise Adams Dean, Career and Technical Education Butte College 3536 Butte Campus Drive Oroville, CA 95965 Phone: 530-895-2329 [email protected] Susan Craig, RN, MSN Nursing Program Director/Chair Phone: 530-879-4338 [email protected] Trudy Old Director NFN Health Workforce Initiative Butte College Skyway Center 2480 Notre Dame Blvd. Chico, CA 95928 Phone: 530-879-9049 [email protected] Sheila Scroggins Director of Nursing Yuba College 2088 N. Beale Road Marysville, CA 95901 Phone: 530-741-6785 Fax: 530-741-6900 [email protected] Janis Laiacona Director, Nursing Program College of the Siskiyous 800 College Ave. Weed, CA 96094 Phone: 530-938-5929 [email protected] Donna Duell Assistant Director / Consultant [email protected] Cora Brownell Assistant Director [email protected]
4
4

Carol Huston Chico State University Director, School of Nursing Chico, CA 95929-0200 Phone: 530-898-5891 [email protected] Judy Mahan Dept. of Allied Health/Nursing Instructor Feather River College 570 Golden Eagle Avenue Quincy, CA 95971 Phone: 530-283-0202 x235 [email protected] Still seeking replacement for Monna Walters Director of Nursing as of 6 26 14 Lassen Community College P.O. Box 3000 478-200 Hwy 139 Susanville, CA 96130 Phone: 530-257-6181 Peggy Rowberg Associate Professor California State University, Chico Holt Hall 336 Chico, CA 95926 Phone: 530-898-3493 Cell: 530-514-7811 [email protected]
Kristie Stephens RN MSN Dean, School of Nursing Simpson University 2211 College View Drive Redding, CA 96003 530-226-226-4529 [email protected] Jean Shackelford Instructor CSU, Chico 14318 St. Mary's Avenue Red Bluff, CA 96080 (530) 527-8984 [email protected] Kathy Royce Dean Health Sciences & University Programs Shasta College P.O. Box 496006 Redding, CA 96049-6066 Phone: 530-339-3610 [email protected] Linda Zorn Statewide Director, Health Workforce Initiative Butte College 2050 Talbert Drive, Suite 300 Chico, CA 95928 Phone: 530-879-9069 Fax: 530-879-0179 [email protected] Suzanne Ness, Regional Vice President Hospital Council of Northern and Central California 1215 K Street, Suite 730 Sacramento, CA 95814 Phone: 916-552-7534 Fax: 916-552-2618 E-mail: [email protected] Pamela Eck, Regional Office Coordinator Phone: 916-552-7653 E-mail: [email protected]
5
5

ATTACHMENT B.1
6
6

Far North CA Nurse Leaders meeting September 24,2015 Hospital Council of Northern and Central California Sherie Ambrose CEN/VP PCS MMCMS Sherie Sherie Ambrose, CNE/VP PCS-MMCMS
PALLIATIVE CARE UPDATES
7
7

Legislative Updates AB-2139 - End of Life Care; Patient Notification-Eggman • Requires the health care provider to notify patient (or person authorized)
the right to comprehensive information and counseling regarding “End of Life” care at the time of terminal diagnosis.
• All Facilities Letter – Effective January 1, 2015
SB 128-End of Life Option Act-Wolk, Monning • Stalled in Assembly Health Committee in July 2015 AB X2-15 Eggman-End of Life Option Act • 9/9/15-The state Assembly(43-34) passed a bill that would allow
physicians to prescribe life-ending drugs to the terminally sick. The End of Life Option Act, awaits final approval by the Senate- (concerns expressed by the Governor)-would require patients to submit two oral requests for a lethal prescription, a minimum of 15 days apart, as well as a written request. The attending physician would receive all three requests.
8
8

SB-19- POLST Registry Act in California- Wolk 12-1-14 California Healthcare Foundation pilot-ignty Health supporting a piolot in the Sacramento area AB 637- authorizing nurse practitioners and physician assistants, under the direction of a physician and within their scope of practice, to sign Physician Orders for Life-Sustaining Treatment (POLST) forms and make them actionable medical orders. The bill, authored by Assembly member Nora Campos (D-San Jose), goes into effect on Jan. 1, 2016.
Legislative Updates 9
9

Legislative Updates SB-19- POLST Registry Act in California- Wolk 12-1-14 California Healthcare Foundation pilot-ignty Health supporting a piolot in the Sacramento area AB 637- authorizing nurse practitioners and physician assistants, under the direction of a physician and within their scope of practice, to sign Physician Orders for Life-Sustaining Treatment (POLST) forms and make them actionable medical orders. The bill, authored by Assembly member Nora Campos (D-San Jose), goes into effect on Jan. 1, 2016.
10
10

• Palliative Care Visioning Day September 22,2015
• Organization charts for Palliative Care
• Staffing Models for 2017 budgets-best model
• Develop Corporate Metric-Board of Directors Goal
• Goal PCQN participation by one facility in each service area-Inside California
Dignity Health projects
11
11

• www.pcqn.org
• Working on Bringing PCQN to Rural Hospitals and clinics
via Partnership Health Plan
Palliative Care Quality Network 12
12

• Number of Palliative Care consults
• Bed type before Palliative Care consult and after PC consult
• Number of Patients transferred to a SNF with a POLST
• Number of PC patients provided the option of Hospice
Suggestions for Palliative Care Metric
13
13

ATTACHMENT B.2
14
14

T h e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med 373;8 nejm.org August 20, 2015 747
Review Article
Palliative care is the interdisciplinary specialty focused on im-proving quality of life for persons with serious illness and their families. Over the past decade,1 the field has undergone substantial growth and
change, including an expanded evidence base, new care-delivery models, innova-tive payment mechanisms, and increasing public and professional awareness.
Cor e Concep t s
In the United States and increasingly in most countries, palliative care and hospice have distinct meanings. Palliative care is interdisciplinary care (medicine, nursing, social work, chaplaincy, and other specialties when appropriate) that focuses on improving quality of life for persons of any age who are living with any serious illness and for their families.2 By treating pain, other symptoms, and psychological and spiritual distress, by using advanced communication skills to establish goals of care and help match treatments to those individualized goals, and by providing sophisticated care coordination, palliative care provides an added layer of support to patients, their loved ones, and treating clinicians. Ideally, palliative care is initi-ated at the time of diagnosis and is provided concordantly with all other disease-directed or curative treatments (Fig. S1 in the Supplementary Appendix, available with the full text of this article at NEJM.org).
Hospice, by contrast, is a formal system of interdisciplinary care that provides palliative care services to the dying in the last months of life. It was first developed in 1967 by Dame Cicely Saunders to provide a setting and model of care for people dying from advanced cancer. Today, the settings for hospice care and payment mechanisms vary across countries. In the United States, unlike most other coun-tries, hospice is a relatively separate system of care for the terminally ill. Eligibil-ity criteria are defined by insurance benefits and federal programs (Medicare, Medicaid, and Veterans Affairs), and Medicare-certified hospices are subject to strict regulatory requirements. Currently, patients qualify for hospice if they have a prognosis of survival of 6 months or less and are willing to forgo curative treat-ments. Under Medicare, this decision includes relinquishing Part A services.
Table 1 outlines the differences between hospice and palliative care in the United States. In this article, we use the term “hospice” to describe the U.S. health care delivery system that provides palliative care under the Medicare hospice benefit, “palliative care” to describe the interdisciplinary specialty, and “palliative medicine” to describe the formal subspecialty of the American Board of Medical Specialties.
Cor e Componen t s of Pa lli ati v e C a r e
The core components of palliative care include the assessment and treatment of physical and psychological symptoms, identification of and support for spiritual
From the Brookdale Department of Geriat-rics and Palliative Medicine, Icahn School of Medicine at Mount Sinai (A.S.K., R.S.M.), and the National Palliative Care Research Center (R.S.M.), New York, and the James J. Peters Veterans Affairs Med-ical Center, Bronx (A.S.K., R.S.M.) — both in New York. Address reprint requests to Dr. Kelley at the Department of Geriatrics and Palliative Medicine, Icahn School of Medicine at Mount Sinai, 1 Gustave L. Levy Pl., Box 1070, New York, NY 10029, or at amy . kelley@ mssm . edu.
N Engl J Med 2015;373:747-55.DOI: 10.1056/NEJMra1404684Copyright © 2015 Massachusetts Medical Society.
Edward W. Campion, M.D., Editor
Palliative Care for the Seriously IllAmy S. Kelley, M.D., M.S.H.S., and R. Sean Morrison, M.D.
The New England Journal of Medicine Downloaded from nejm.org at KAISER PERMANENTE on August 21, 2015. For personal use only. No other uses without permission.
Copyright © 2015 Massachusetts Medical Society. All rights reserved.
15
15

n engl j med 373;8 nejm.org August 20, 2015748
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
distress, expert communication to establish goals of care and assist with complex medical decision making, and coordination of care (Table 2). Ideal-ly, many of these components can and should be provided by primary treating clinicians — much in the way that uncomplicated hypertension or
diabetes is managed by primary care physicians rather than by cardiologists or endocrinologists — with specialist-level palliative care teams pro-viding care in the most complex and difficult clinical cases. However, in reality, most physi-cians and other health care professionals cur-
Characteristic Palliative Care Hospice
Model of care Interdisciplinary team, including physicians, nurses, social workers, chaplains, and staff from other disciplines as needed; primary goal is improved quality of life
Interdisciplinary team, including physicians, nurs-es, social workers, chaplains, and volunteers, as dictated by statute; primary goals are im-proved quality of life and relief of suffering (physical, emotional, and spiritual)
Eligibility Patients of all ages and with any diagnosis or stage of illness; patients may continue all life-prolonging and disease-directed treatments
Patients of all ages who have a prognosis of sur-vival of ≤6 mo, if the disease follows its usual course; patients must forgo Medicare coverage for curative and other treatments related to ter-minal illness
Place Hospitals (most common), hospital clinics, group practices, cancer centers, home care programs, or nursing homes
Home (most common), assisted-living facilities, nursing homes, residential hospice facilities, inpatient hospice units, or hospice-contracted inpatient beds
Payment Physician and nurse practitioner fees covered by Medicare Part B for inpatient or outpa-tient care; hospital teams are included with-in Medicare Part A or commercial insur-ance payments to hospitals for care epi-sodes; flexible bundled payments under Medicare Advantage, Managed Medicaid, ACOs, and other commercial payers
Medicare hospice benefit; standard hospice bene-fit from commercial payers is usually modeled after Medicare; Medicaid, although coverage varies by state; medication costs are included for illnesses related to the terminal illness
* ACO denotes accountable care organization.
Table 1. Palliative Care as Compared with Hospice.*
Domain Key Recommendations
Structure and processes of care Interdisciplinary team, comprehensive interdisciplinary assessment, edu-cation and training; relationship with hospice program
Physical aspects of care Pain and other symptoms are managed with the use of best practices
Psychological and psychiatric aspects of care
Psychological and psychiatric issues are assessed and managed; grief and bereavement program is available to patients and families
Social aspects of care Interdisciplinary social assessment with appropriate care plan; referral to appropriate services
Spiritual, religious, and existential aspects of care
Spiritual concerns are assessed and addressed; linkages to community and spiritual or religious resources are provided as appropriate
Cultural aspects of care Culture-specific needs of patients and families are assessed and addressed; recruitment and hiring practices reflect the cultural diversity of the com-munity
Care of the imminently dying patient Signs and symptoms of impending death are recognized and communicated; hospice referral is recommended when patient is eligible
Ethical and legal aspects of care Patient’s goals, preferences, and choices form basis for plan of care; the team is knowledgeable about relevant federal and state statutes and regulations
* Adapted from the National Consensus Project for Quality Palliative Care.2
Table 2. Palliative Care Domains and Recommendations from the National Consensus Panel Guidelines.*
The New England Journal of Medicine Downloaded from nejm.org at KAISER PERMANENTE on August 21, 2015. For personal use only. No other uses without permission.
Copyright © 2015 Massachusetts Medical Society. All rights reserved.
16
16

n engl j med 373;8 nejm.org August 20, 2015 749
Palliative Care for the Seriously Ill
rently in practice have had limited or no formal training in these areas.3
The following sections highlight key concepts and recent developments in palliative care prac-tice. Evidence is drawn largely from observa-tional studies, with an increasing number of recent randomized, controlled trials. Interested readers may find additional details regarding specific domains of palliative care research in other recently published reviews.4-7
Physical and Psychological Symptoms
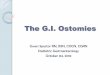
Whereas pain is the most studied and publicized symptom experienced by persons with common serious illnesses, observational prevalence stud-ies suggest that pain is only one of many dis-tressing symptoms (Fig. 1).8-18 Routine compre-hensive symptom assessment with the use of validated instruments is indicated in the context of advanced disease. As compared with routine care, which includes standard clinical histories
and review of systems, formal symptom assess-ment with the use of validated instruments can improve the identification of distressing symp-toms and lead to enhanced comfort and better outcomes.19 Table S1 in the Supplementary Ap-pendix summarizes standard approaches to man-aging the common symptoms, such as anorexia, anxiety, constipation, depression, delirium, dys-pnea, nausea, and fatigue, that occur in patients with serious illness.
Spirituality
Data suggest that spiritual concerns are com-mon in persons with serious illness and that the majority want to discuss their spirituality with their physicians.20 Nevertheless, less than 50% of physicians believe that it is their role to address such concerns, and only a minority of patients report having their spiritual needs addressed.20,21 Widespread consensus holds that health care chaplains should provide spiritual care,2 yet there
Figure 1. Symptom Prevalence in Advanced Illness.
Data are from representative studies of symptom prevalence among patients with cancer,8-12 congestive heart fail-ure,13,14 chronic obstructive pulmonary disease (COPD),15 chronic kidney disease (CKD),13,14 or dementia16,17 and among patients who received highly active antiretroviral therapy for the acquired immunodeficiency syndrome (AIDS).18 Self-reported data regarding some symptoms were unavailable for patients with dementia.
Sym
ptom
Pre
vale
nce
(% o
f pat
ient
s)100
80
60
40
20
0
90
70
50
30
10
Cancer CongestiveHeart Failure
COPD CKD Dementia AIDS
Pain
Breathlessness
Fatigue or lack of energy
Anorexia
Nausea or vomiting
Constipation
Anxiety or nervousness
Depression or sadness
Dry mouth
Sleep disturbance
The New England Journal of Medicine Downloaded from nejm.org at KAISER PERMANENTE on August 21, 2015. For personal use only. No other uses without permission.
Copyright © 2015 Massachusetts Medical Society. All rights reserved.
17
17

n engl j med 373;8 nejm.org August 20, 2015750
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
are insufficient numbers of health care chap-lains and very few are certified in palliative care. Thus, most seriously ill patients depend on other members of the health care team to address spiritual concerns.
Various studies highlight the importance of spirituality and religious practice with respect to outcomes in seriously ill patients. An observa-tional study by Winkelman et al. showed that patients with cancer who had unmet spiritual concerns were more likely to have significantly worse psychological quality of life than those whose spiritual concerns were addressed.22 In addition, a multisite cohort study involving 343 patients with advanced cancer showed that the patients whose spiritual needs were supported received more hospice care and were less likely to have burdensome nonbeneficial interventions near the end of life than those whose needs were not met and, furthermore, that spiritual support from the medical team or chaplain was associ-ated with higher quality-of-life scores.23,24 In the same cohort, patients who relied highly on reli-gious faith to cope with cancer were more likely than those with a low level of religious coping to receive mechanical intubation and intensive care unit (ICU) care near the end of life.25 Where-as consensus supports referral to a chaplain when spiritual concerns are identified, the efficacy of spiritual interventions has not been studied. Similarly, the mechanisms by which spiritual distress affects outcomes and whether these mechanisms are modifiable remain unknown.
Communication Skills
Empirical research that is focused on communi-cation in the context of serious illness has grown rapidly in the past decade. Building on consensus-based approaches to conducting difficult conver-sations (e.g., “breaking bad news”), a series of randomized trials and skills assessments before and after training have rigorously studied these approaches, refined frameworks for these dis-cussions, identified core communication skills, and begun to examine the clinical outcomes associated with effective communication train-ing.26-28 Common communication scenarios may involve communicating serious news, discussing prognostic uncertainty, establishing goals of care, and selecting treatment options.29
Various efforts have honed cognitive road maps for these specific clinical scenarios, such
as SPIKES (setting up the interview, assessing the patient’s perception, obtaining the patient’s invitation, giving knowledge and information, responding to emotion, and summarizing the discussion), and have identified core skills for effective communication, such as expressing em-pathy with the use of NURSE (naming, under-standing, respecting, supporting, and exploring) statements.29 Communication skills training programs that are based on empirical research now exist — both online (www.capc.org/topics/communication-and-palliative-care) and in work-shop settings (www.vitaltalk.org).
In a large, prospective cohort study involving patients with advanced cancer, those who had a goals-of-care discussion with their physician were less likely than patients who did not have such a discussion to die in an ICU or to receive me-chanical ventilation and cardiopulmonary resus-citation and were more likely to be enrolled in hospice for longer than 1 week.30 Another pro-spective cohort study involving patients in the ICU and their families showed that structured discus-sions about patients’ wishes for end-of-life care were associated with significantly increased over-all family satisfaction with ICU care and improved family satisfaction with decision making.31 Con-siderable strides have also been made in the sci-ence of advance care planning and decision sup-port tools.32,33 Particularly relevant to clinicians who are building primary palliative care skills and are aiming to engage patients in advance care plan-ning are public-use websites that have materials from these studies (e.g., www.prepareforyourcare .org, www.agingwithdignity.org/five-wishes.php, and www.acpdecisions.org).
Model s of Pa lli ati v e C a r e Deli v er y
Hospitals
The most common setting for nonhospice pal-liative care services in the United States, and in much of the world, is the acute care hospital. Initially established within academic medical cen-ters in North America, palliative care programs have spread to other hospital types. Indeed, over the past decade, palliative care programs have grown by more than 150%, such that almost 90% of hospitals with 300 beds or more and two thirds of hospitals with 50 beds or more now have palliative care programs.34 Beginning in
The New England Journal of Medicine Downloaded from nejm.org at KAISER PERMANENTE on August 21, 2015. For personal use only. No other uses without permission.
Copyright © 2015 Massachusetts Medical Society. All rights reserved.
18
18

n engl j med 373;8 nejm.org August 20, 2015 751
Palliative Care for the Seriously Ill
2011, the Joint Commission established the Ad-vanced Certification for Palliative Care Pro-grams.35 To date, 82 programs have received this certification.35
Within hospitals, the primary model of care delivery is the interdisciplinary consultation team. Large hospitals and mature programs may also include dedicated inpatient units. In addition to these traditional models, new service-delivery models and innovations include dedicated ICU teams, comanagement models, in which a pal-liative care specialist joins an existing specialty team (e.g., oncology), and triggers for automatic palliative care referrals. Multiple randomized, controlled trials and a few observational studies that have compared the outcomes in seriously ill patients who were referred to hospital-based pal-liative care teams with the outcomes in patients who received usual care have shown reduced symptom distress,36-38 enhanced quality of life,37,38 and decreased spiritual distress23 among the pa-tients referred to palliative care. Although several quasi-experimental studies have also shown re-duced costs and resource utilization,5,7 no formal cost-effectiveness studies (i.e., measuring both costs and a range of patient and family out-comes) have been completed to date.7
Community
Historically in the United States, community-based palliative care was available only through hospice programs and, therefore, available only to patients with a prognosis of survival of 6 months or less who had decided to forgo further curative treatments. Hospice continues to provide the largest proportion of palliative care in home-based settings, but this care is provided for lim-ited time spans and only during the final stages of disease. The overall quality of and satisfaction with hospice care has been consistently high.39
In the past decade, community-based models of palliative care have been developed to serve seriously ill people who are not eligible for hos-pice. These programs are evolving rapidly as a result of the Affordable Care Act (ACA), which expanded cost-sharing programs (e.g., account-able care organizations), created bundled-payment programs, and encouraged the formation of com-mercially managed Medicare and Medicaid pro-grams. Because of the incentives provided in these new programs, private payers and Medicare Ad-vantage plans have been early innovators in de-
veloping palliative care programs because of the potential of these programs to reduce costs and improve quality. These programs use interdisci-plinary palliative care teams to establish clear goals of care, enhance symptom management and caregiver support in the home setting, coor-dinate care, and provide an extra layer of support to treating physicians.40,41
Unlike traditional programs for managing chronic disease, these new programs serve a highly complex population and are designed to include the core domains of palliative care (Table 2). Although robust data on their cost-effectiveness are still needed, preliminary obser-vational data from community-based programs and evidence from randomized trials of other programs of outpatient palliative care have shown enhanced symptom management, improved pa-tient and family satisfaction scores, and signifi-cant reductions in hospitalization rates, emer-gency department visits, days in the ICU, and physician office visits.4,40,41 Furthermore, in two randomized trials involving certain subpopula-tions, persons receiving palliative care in com-munity settings have had longer survival than community-dwelling persons with the same diag-nosis who are not receiving palliative care.37,42 Further study is needed to replicate this observed survival benefit and elucidate the mechanisms, because survival was not the primary outcome in either of the studies cited. Community-based palliative care services are more well developed in Canada, Western Europe, and Australia than they are in the United States.6,42-44
Long-Term Care
Approximately 1.8 million U.S. residents live in nursing homes, and this number is expected to more than double by 2030.45,46 The palliative care needs of this population are vast. More than 25% of elderly persons die in nursing homes, 67% of persons with advanced dementia live their final days in this setting,16 and more than half of nursing home residents require extensive or com-plete assistance with activities of daily living.45
Currently, there are three models for deliver-ing palliative care in nursing homes. The most established model is hospice. Many nursing homes contract with a hospice agency for services, and the percentage of persons in nursing homes who received hospice services before they died in-creased from 14% in 1999 to 33% in 2006.47 As
The New England Journal of Medicine Downloaded from nejm.org at KAISER PERMANENTE on August 21, 2015. For personal use only. No other uses without permission.
Copyright © 2015 Massachusetts Medical Society. All rights reserved.
19
19

n engl j med 373;8 nejm.org August 20, 2015752
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
compared with nursing home care that does not include hospice, hospice use in nursing homes is associated with lower rates of invasive therapies and hospitalizations, improved management of pain and symptoms, and higher family satisfac-tion with care.47 The 6-month prognostic re-quirement for hospice eligibility greatly limits access, however, given the duration of need and the unpredictable prognoses of most nursing home residents.
Another model is palliative care consultation, in which an external palliative care physician or nurse practitioner provides recommendations to the nursing home clinicians and bills services under Medicare Part B. Difficulties related to this model include a lack of reimbursement mechanisms for nonphysician members of the palliative care team and a reliance on the nurs-ing home staff — who may not have palliative care training — to implement and follow through on recommendations. Finally, some nursing homes have developed internal palliative care teams or specialized units, which are focused primarily on residents with advanced dementia.
E x pa nding Access t o Pa lli ati v e C a r e a nd B a r r ier s t o Deli v er y
Although palliative care was focused initially on patients dying from cancer, the patient popula-tion that may benefit from palliative care has expanded considerably. Many randomized, con-trolled trials and case–control studies of pallia-tive care interventions to date have shown reduc-tions in patients’ symptoms and health care utilization and improvements in quality of life and family satisfaction across a wide spectrum of populations, including patients with advanced cancer,37 neurologic disease,48 or lung disease42 and older adults with multiple coexisting condi-tions and frailty.6,49 The patient population that benefits most from referral to specialist-level palliative care and the appropriate timing of such referral are still being defined by empirical research, yet consensus recommendations sup-port referral at the time of diagnosis for patients with advanced cancer, neurologic disease, or organ damage; those with multiple coexisting conditions, frailty, or advanced cognitive impair-ment; those with a high symptom or iatrogenic-treatment burden (e.g., those who have received a bone marrow transplant for acute leukemia);
and those who have onerous family or caregiver needs regardless of prognosis.2,36
Considerable barriers may prevent many per-sons from accessing or using palliative care ser-vices. First, the number of palliative care special-ists falls far short of what is necessary to serve the population in need. A 2010 study estimated that 6000 to 18,000 additional physicians are needed to meet the current demand in the inpa-tient setting alone.50 Similar shortages are also anticipated across other disciplines. The demand for the expansion of palliative care services in new care settings that was created by incentives under the ACA and the Joint Commission Ad-vanced Certification for Palliative Care, as de-scribed above, is further straining the limited specialist-level palliative care workforce.
Finally, regional, socioeconomic, and racial and ethnic-group determinants influence access to palliative care.51,52 The factors associated with increased availability of hospital-based palliative care include not-for-profit status, geographic lo-cations outside the southern United States, teach-ing hospitals, and faith-based hospitals.52 In addition, persons of minority races and ethnic groups access palliative care and hospice ser-vices far less frequently than do whites.51 This situation is particularly worrisome given evidence that, as compared with whites, these groups have higher rates of inadequately treated pain, prefer-ence-discordant medical treatments, and low sat-isfaction with care and provider communication.51
E v idence G a ps a nd Fu t ur e Dir ec tions
Key research needs to be funded and performed if palliative care is going to achieve its potential to enhance value throughout the health care system. First, as noted above, important gaps in clinical evidence need to be addressed so that persons with serious illness can receive the best available care. For example, the biologic bases of nonpain symptoms are poorly understood, and treatments for symptoms such as breathlessness, fatigue, pruritus, delirium, and even pain are suboptimal, and randomized, controlled trials of interventions are needed to identify ways to improve care for patients with those symptoms.
Second, the needs of older adults with serious illness and their caregivers and the longitudinal nature of those needs have yet to be well de-
The New England Journal of Medicine Downloaded from nejm.org at KAISER PERMANENTE on August 21, 2015. For personal use only. No other uses without permission.
Copyright © 2015 Massachusetts Medical Society. All rights reserved.
20
20

n engl j med 373;8 nejm.org August 20, 2015 753
Palliative Care for the Seriously Ill
scribed.53 In particular, the complex care needs of patients with multiple coexisting conditions must be investigated. The population at risk must be defined beyond traditional disease-specific or prognosis-based definitions, and a better under-standing of the multiyear needs of these persons and their caregivers is required in order to de-velop targeted care models and, given an inade-quate workforce, to deploy the workforce effi-ciently.53 Third, data to guide care for seriously ill children and for adults with end-stage demen-tia are needed. Finally, the development and evaluation of palliative care–delivery models out-side hospitals is essential. If this research is to be undertaken, research funding for palliative care will need to be increased beyond the 0.01% of the National Institutes of Health budget that currently supports research on palliative care.54
Knowledge of palliative care and the skills of non–palliative medicine physicians also need to be improved to meet patients’ needs. Expanding the primary palliative care skills of all clinicians will be a key step toward resolving the shortage in the palliative care workforce. The core pallia-tive care competencies of communication, pain and symptom management, and psychosocial assessment remain, at best, a small part of most medical school and residency training programs. The vast majority of practicing physicians and trainees has rudimentary skills in these areas, which negatively affects patient and family out-comes.3 Conversely, an increasing body of evi-dence suggests that these skills (particularly communication skills) can be effectively learned and developed and are associated with improved outcomes.26-28 Strategies to expand specialist-level palliative care training and generalist train-ing in core palliative care knowledge and skills are needed.
Major issues impeding the access to palliative care are the perceptions among doctors that pal-liative care is appropriate only at the end of life, that palliative care is synonymous with hospice, and that patients will react negatively and lose all hope if palliative care referral is discussed.55,56 In contrast to the perceptions of physicians, a re-cent survey showed that almost 90% of adults in the United States had either no knowledge or limited knowledge of palliative care. When read a definition, more than 90% of the respon-dents stated that they would want palliative care for themselves or their family member and that it should be universally available.57 Targeted social marketing and educational efforts must be directed both to the public and to medical professionals.
Palliative care is now a rapidly growing medical specialty in the United States, and a mounting body of evidence shows that palliative care teams enhance the quality of health care for persons living with serious illness and for their families, while reducing medical expenditures. Palliative care teams are well established in most U.S. hospitals, although penetration is varied, and most of the patients and families who could benefit from palliative care services still do not receive them. New models of community-based palliative care are emerging, although data on their cost-effectiveness are not yet available. Gaps in research, workforce deficits, and defi-ciencies in public and professional knowledge need to be addressed if care for persons with serious illness and their families is to be further improved.
No potential conflict of interest relevant to this article was reported.
Disclosure forms provided by the authors are available with the full text of this article at NEJM.org.
References1. Morrison RS, Meier DE. Palliative care. N Engl J Med 2004; 350: 2582-90.2. Clinical practice guidelines for qual-ity palliative care. 3rd ed. Pittsburgh: National Consensus Project for Quality Palliative Care, 2013 (http://www .nationalconsensusproject .org/ NCP_ Clinical_Practice_Guidelines_3rd_Edition .pdf).3. Block SD. Medical education in end-of-life care: the status of reform. J Palliat Med 2002; 5: 243-8.4. Rabow M, Kvale E, Barbour L, et al. Moving upstream: a review of the evi-
dence of the impact of outpatient pallia-tive care. J Palliat Med 2013; 16: 1540-9.5. Smith S, Brick A, O’Hara S, Normand C. Evidence on the cost and cost-effective-ness of palliative care: a literature review. Palliat Med 2014; 28: 130-50.6. Gomes B, Calanzani N, Curiale V, Mc-Crone P, Higginson IJ. Effectiveness and cost-effectiveness of home palliative care services for adults with advanced illness and their caregivers. Cochrane Database Syst Rev 2013; 6: CD007760.7. May P, Normand C, Morrison RS. Eco-nomic impact of hospital inpatient pallia-
tive care consultation: review of current evidence and directions for future re-search. J Palliat Med 2014; 17: 1054-63.8. Oi-Ling K, Man-Wah DT, Kam-Hung DN. Symptom distress as rated by ad-vanced cancer patients, caregivers and physicians in the last week of life. Palliat Med 2005; 19: 228-33.9. Modonesi C, Scarpi E, Maltoni M, et al. Impact of palliative care unit admission on symptom control evaluated by the edmonton symptom assessment system. J Pain Symptom Manage 2005; 30: 367-73.10. Potter J, Hami F, Bryan T, Quigley C.
The New England Journal of Medicine Downloaded from nejm.org at KAISER PERMANENTE on August 21, 2015. For personal use only. No other uses without permission.
Copyright © 2015 Massachusetts Medical Society. All rights reserved.
21
21

n engl j med 373;8 nejm.org August 20, 2015754
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
Symptoms in 400 patients referred to pal-liative care services: prevalence and pat-terns. Palliat Med 2003; 17: 310-4.11. Walsh D, Donnelly S, Rybicki L. The symptoms of advanced cancer: relation-ship to age, gender, and performance sta-tus in 1,000 patients. Support Care Can-cer 2000; 8: 175-9.12. Moens K, Higginson IJ, Harding R. Are there differences in the prevalence of palliative care-related problems in people living with advanced cancer and eight non-cancer conditions? A systematic re-view. J Pain Symptom Manage 2014; 48: 660-77.13. Nordgren L, Sorensen S. Symptoms experienced in the last six months of life in patients with end-stage heart failure. Eur J Cardiovasc Nurs 2003; 2: 213-7.14. Anderson H, Ward C, Eardley A, et al. The concerns of patients under palliative care and a heart failure clinic are not be-ing met. Palliat Med 2001; 15: 279-86.15. Bausewein C, Booth S, Gysels M, Kühnbach R, Haberland B, Higginson IJ. Understanding breathlessness: cross-sec-tional comparison of symptom burden and palliative care needs in chronic ob-structive pulmonary disease and cancer. J Palliat Med 2010; 13: 1109-18.16. Mitchell SL, Teno JM, Kiely DK, et al. The clinical course of advanced dementia. N Engl J Med 2009; 361: 1529-38.17. Pautex S, Herrmann FR, Le Lous P, et al. Symptom relief in the last week of life: is dementia always a limiting factor? J Am Geriatr Soc 2007; 55: 1316-7.18. Karus D, Raveis VH, Alexander C, et al. Patient reports of symptoms and their treatment at three palliative care projects servicing individuals with HIV/AIDS. J Pain Symptom Manage 2005; 30: 408-17.19. Bausewein C, Daveson B, Benalia H, Simon ST, Higginson IJ. Outcome mea-surement in palliative care: the essentials. London: PRISMA, 2011 (http://www .kcl .ac .uk/ lsm/ research/ divisions/ cicelysaun-ders/ attachments/ keyreport-Guidance-on-Outcome-Measurement-in-Palliative-Care .pdf).20. El Nawawi NM, Balboni MJ, Balboni TA. Palliative care and spiritual care: the crucial role of spiritual care in the care of patients with advanced illness. Curr Opin Support Palliat Care 2012; 6: 269-74.21. Rodin D, Balboni M, Mitchell C, Smith PT, VanderWeele TJ, Balboni TA. Whose role? Oncology practitioners’ per-ceptions of their role in providing spiri-tual care to advanced cancer patients. Support Care Cancer 2015 January 28 (Epub ahead of print).22. Winkelman WD, Lauderdale K, Bal-boni MJ, et al. The relationship of spiri-tual concerns to the quality of life of ad-vanced cancer patients: preliminary findings. J Palliat Med 2011; 14: 1022-8.23. Balboni TA, Vanderwerker LC, Block SD, et al. Religiousness and spiritual sup-
port among advanced cancer patients and associations with end-of-life treatment preferences and quality of life. J Clin On-col 2007; 25: 555-60.24. Balboni TA, Paulk ME, Balboni MJ, et al. Provision of spiritual care to patients with advanced cancer: associations with medical care and quality of life near death. J Clin Oncol 2010; 28: 445-52.25. Phelps AC, Maciejewski PK, Nilsson M, et al. Religious coping and use of in-tensive life-prolonging care near death in patients with advanced cancer. JAMA 2009; 301: 1140-7.26. Back AL, Arnold RM, Tulsky JA, Baile WF, Fryer-Edwards KA. Teaching commu-nication skills to medical oncology fel-lows. J Clin Oncol 2003; 21: 2433-6.27. Au DH, Udris EM, Engelberg RA, et al. A randomized trial to improve com-munication about end-of-life care among patients with COPD. Chest 2012; 141: 726-35.28. Tulsky JA, Arnold RM, Alexander SC, et al. Enhancing communication between oncologists and patients with a computer-based training program: a randomized trial. Ann Intern Med 2011; 155: 593-601.29. Back A, Arnold R, Tulsky J. Mastering communication with seriously ill pa-tients: balancing honesty with empathy and hope. Cambridge, United Kingdom: Cambridge University Press, 2009.30. Wright AA, Zhang B, Ray A, et al. As-sociations between end-of-life discus-sions, patient mental health, medical care near death, and caregiver bereavement adjustment. JAMA 2008; 300: 1665-73.31. Johnson JR, Engelberg RA, Nielsen EL, et al. The association of spiritual care providers’ activities with family members’ satisfaction with care after a death in the ICU. Crit Care Med 2014; 42: 1991-2000.32. Butler M, Ratner E, McCreedy E, Ship-pee N, Kane RL. Decision aids for advance care planning: an overview of the state of the science. Ann Intern Med 2014; 161: 408-18.33. Sudore RL, Fried TR. Redefining the “planning” in advance care planning: pre-paring for end-of-life decision making. Ann Intern Med 2010; 153: 256-61.34. National Palliative Care Registry. An-nual survey summary: results of the 2012 National Palliative Care Registry Survey, as of July 2014 (https:/ / registry .capc .org/ cms/ portals/ 1/ Reports/ Registry_Summa-ry%20Report_2014 .pdf).35. The Joint Commission. Advanced cer-tification for palliative care programs. 2011 (http://www .jointcommission .org/ certification/ palliative_care .aspx and http://www .qualitycheck .org/ Certifica-tionList .aspx).36. Higginson IJ, Finlay I, Goodwin DM, et al. Do hospital-based palliative teams improve care for patients or families at the end of life? J Pain Symptom Manage 2002; 23: 96-106.
37. Temel JS, Greer JA, Muzikansky A, et al. Early palliative care for patients with metastatic non-small-cell lung cancer. N Engl J Med 2010; 363: 733-42.38. Bakitas M, Lyons KD, Hegel MT, et al. Effects of a palliative care intervention on clinical outcomes in patients with ad-vanced cancer: the Project ENABLE II ran-domized controlled trial. JAMA 2009; 302: 741-9.39. Teno JM, Clarridge BR, Casey V, et al. Family perspectives on end-of-life care at the last place of care. JAMA 2004; 291: 88-93.40. Ciemins EL, Stuart B, Gerber R, New-man J, Bauman M. An evaluation of the Advanced Illness Management (AIM) pro-gram: increasing hospice utilization in the San Francisco Bay area. J Palliat Med 2006; 9: 1401-11.41. Spettell CM, Rawlins WS, Krakauer R, et al. A comprehensive case management program to improve palliative care. J Pal-liat Med 2009; 12: 827-32.42. Higginson IJ, Bausewein C, Reilly CC, et al. An integrated palliative and respira-tory care service for patients with ad-vanced disease and refractory breathless-ness: a randomised controlled trial. Lancet Respir Med 2014; 2: 979-87.43. Fainsinger RL, Brenneis C, Fassbend-er K. Edmonton, Canada: a regional mod-el of palliative care development. J Pain Symptom Manage 2007; 33: 634-9.44. Eagar K, Watters P, Currow DC, Aoun SM, Yates P. The Australian Palliative Care Outcomes Collaboration (PCOC) — mea-suring the quality and outcomes of pallia-tive care on a routine basis.Aust Health Rev 2010; 34: 186-92.45. Hoyert DL, Xu J. Deaths: preliminary data for 2011. Natl Vital Stat Rep 2012; 61(6): 1-51 (http://www .cdc .gov/ nchs/ data/ nvsr/ nvsr61/ nvsr61_06 .pdf).46. Centers for Disease Control and Pre-vention, National Center for Health Sta-tistics. National Nursing Home Survey: 2004 current resident tables – estimates, 2012 (http://www .cdc .gov/ nchs/ nnhs/ resi-dent_tables_estimates .htm).47. Miller SC, Lima J, Gozalo PL, Mor V. The growth of hospice care in U.S. nurs-ing homes. J Am Geriatr Soc 2010; 58: 1481-8.48. Edmonds P, Hart S, Gao W, et al. Pal-liative care for people severely affected by multiple sclerosis: evaluation of a novel palliative care service. Mult Scler 2010; 16: 627-36.49. Gómez-Batiste X, Caja C, Espinosa J, et al. The Catalonia World Health Organi-zation demonstration project for pallia-tive care implementation: quantitative and qualitative results at 20 years. J Pain Symptom Manage 2012; 43: 783-94.50. Lupu D; American Academy of Hos-pice and Palliative Medicine Workforce Task Force. Estimate of current hospice and palliative medicine physician work-
The New England Journal of Medicine Downloaded from nejm.org at KAISER PERMANENTE on August 21, 2015. For personal use only. No other uses without permission.
Copyright © 2015 Massachusetts Medical Society. All rights reserved.
22
22

n engl j med 373;8 nejm.org August 20, 2015 755
Palliative Care for the Seriously Ill
force shortage. J Pain Symptom Manage 2010; 40: 899-911.51. Johnson KS. Racial and ethnic dis-parities in palliative care. J Palliat Med 2013; 16: 1329-34.52. Center to Advance Palliative Care. A state-by-state report card on access to palliative care in our nation’s hospitals. 2008 (http://www .capc .org/ reportcard).53. Kelley AS. Epidemiology of care for
patients with serious illness. J Palliat Med 2013; 16: 730-3.54. Gelfman LP, Du Q, Morrison RS. An update: NIH research funding for pallia-tive medicine 2006 to 2010. J Palliat Med 2013; 16: 125-9.55. Schenker Y, Crowley-Matoka M, Dohan D, et al. Oncologist factors that influence referrals to subspecialty palliative care clinics. J Oncol Pract 2014; 10(2): e37-e44.
56. Hanratty B, Hibbert D, Mair F, et al. Doctors’ understanding of palliative care. Palliat Med 2006; 20: 493-7.57. Center to Advance Palliative Care. Public opinion research on palliative care. 2011 (https:/ / www .capc .org/ media/ filer_public/ 18/ ab/ 18ab708c-f835-4380-921d -fbf729702e36/ 2011-public-opinion -research-on-palliative-care .pdf).Copyright © 2015 Massachusetts Medical Society.
The New England Journal of Medicine Downloaded from nejm.org at KAISER PERMANENTE on August 21, 2015. For personal use only. No other uses without permission.
Copyright © 2015 Massachusetts Medical Society. All rights reserved.
23
23

ATTACHMENT B.3
24
24

Hilton Los Angeles North/Glendale &
Executive Meeting Center Glendale, CA
ELNEC Summit January 21-22, 2016
25
25

CONNECT TO ELNEC ANYTIME
Contents
About ELNEC ................................................................................................................................................. 2
ELNEC Team .................................................................................................................................................. 3
ELNEC Faculty ................................................................................................................................................ 4
ELNEC Summit Overview .............................................................................................................................. 6
ELNEC Summit Agenda .................................................................................................................................. 8
Accommodations .......................................................................................................................................... 9
General Questions ...................................................................................................................................... 11
Summit Registration Form .......................................................................................................................... 13
26
26

2
About ELNEC The End-of-Life Nursing Education Consortium (ELNEC) project is an international education initiative to improve palliative care. The project provides training in palliative care with essential information to nursing students and practicing nurses, including undergraduate and graduate nursing faculty, continuing education providers, staff development educators, specialty nurses in pediatrics, oncology, critical care, geriatrics and advanced practice nurses. ELNEC also welcomes other health care professionals. The project, which began in February 2000, was initially funded by a major grant from The Robert Wood Johnson Foundation. Additional funding has been received from Aetna Foundation, Archstone Foundation, California HealthCare Foundation, Cambia Health Foundation, Milbank Foundation, National Cancer Institute, Oncology Nursing Foundation, Open Society Foundation and the U.S. Department of Veterans Affairs. The ELNEC project is administered by the American Association of Colleges of Nursing (AACN) in Washington, D.C., and City of Hope, in Duarte, CA. The esteemed faculty includes a national cadre of nursing leaders in palliative care. ELNEC trainers then go on to host professional development seminars for practicing nurses within their institution, incorporating ELNEC content into nursing curriculum, hosting regional training sessions to expand ELNEC’s reach into rural and underserved communities, presenting ELNEC at national and international conferences, coordinating community partnerships and improving the quality of nursing care in other innovative ways. Want to learn more about ELNEC? Visit http://www.aacn.nche.edu/elnec
27
27

CONNECT TO ELNEC ANYTIME
ELNEC Team
Betty Ferrell, RN, PhD, MA, FAAN, FPCN, CHPN Director of Nursing Research & Education and Professor; Principal Investigator of ELNEC City of Hope Duarte, CA [email protected]
Rose Virani, RNC, MHA, OCN, FPCN Senior Research Specialist, ELNEC Project Director City of Hope Duarte, CA [email protected]
Pam Malloy, MN, RN, OCN, FPCN ELNEC Project Director, Co-Investigator American Association of Colleges of Nursing Duarte, CA [email protected]
Lauren Wilson, BA Research Coordinator ELNEC Coordinator City of Hope Duarte, CA [email protected]
Andrea Garcia-Ortiz, MBA Senior Research Coordinator ELNEC Coordinator City of Hope Duarte, CA [email protected]
Linda Garcia, BA Research Coordinator ELNEC Coordinator City of Hope Duarte, CA [email protected]
Kelly Greer, BS Research Coordinator ELNEC Coordinator City of Hope Duarte, CA [email protected]
Jose Llanas ELNEC Project Assistant City of Hope Duarte, CA [email protected]
28
28

4
ELNEC Faculty
Pat Berry, PhD, RN, ACHPN, FPCN, FAAN Professor, Director Hartford Center of Gerontological Nursing Excellence Oregon Health and Science University Portland, OR
Patrick J. Coyne, MSN, ACHPN, ACNS-BC, FAAN, FPCN Clinical Nurse Specialist, Assistant Professor and Director for Palliative Care at the Medical University of South Carolina Charleston, SC
Connie Dahlin, APRN-BC, ACHPN®, FPCN, FAAN Director of Professional Practice; Palliative Care Consultant Hospice and Palliative Nurses Association Boston, MA
Betty Ferrell, RN, PhD, MA, FAAN, FPCN, CHPN Director of Nursing Research & Education and Professor; Principal Investigator of ELNEC City of Hope Duarte, CA
Susan Gibson, RN, FNP-BC, ACHPN Program Coordinator Community Palliative Care program at Visiting Nurse and Hospice Care (VNHC) Santa Barbara, CA
Barbara Head, PhD, RN, CHPN, ACSW, FPCN Assistant Professor of Medicine and Director of the Interdisciplinary Program for Palliative Care and Chronic Illness University of Louisville Louisville, KY
Carol O. Long, PhD, RN, FPCN, FAAN Geriatric Palliative and Community-Based Health Care Consultant C.O. Long Consulting Phoenix, AZ
Pam Malloy, MN, RN, FPCN Director and Co-Investigator of End-of-Life Nursing Education Consortium (ELNEC) American Association of Colleges of Nursing (AACN) Washington, DC
Patricia Maani-Fogelman, DNP Doctor of Nursing Practice and Nurse Practitioner Geisinger Medical Center Danville, PA
Polly Mazanec, PhD, AOCN®, ACNP-BC, FPCN Nurse Practitioner Cleveland Veterans Administration Medical Center Cleveland, OH
Judith Paice, RN, PhD, FAAN Director of the Cancer Pain Program- Division of Hematology-Oncology; Research Professor of Medicine Northwestern University; Feinberg School of Medicine Chicago, IL
Kathy Perko, RN, MS, PNP, CPON, CHPPN, CPLC Pediatric Nurse Practitioner Program Director of Bridges Palliative Care Department, Doernbecher Children’s Hospital at OHSU Portland, OR
29
29

CONNECT TO ELNEC ANYTIME
Rebekah “Beka” Riemer, RN, CCRN Inpatient Palliative Care Team, Little Company of Mary Torrance, CA
Gay Walker RN, CHPPN Director TrinityKids Care (a division of) Providence TrinityCare Hospice Torrance, CA
30
30

6
ELNEC Summit Overview
January 21-22, 2016
Glendale Grand Ballrooms Hilton Glendale Glendale, CA
Tracks Offered – Choose Only One ELNEC APRN (Adult track only) ELNEC Core ELNEC Critical Care ELNEC Geriatric ELNEC Pediatric
Resources
o Review the 2014 Institute of Medicine (IOM) report on palliative care and implications for practice, education, and research.
o Leadership-building in palliative nursing. View documentary showcasing an ELNEC trainer who started a hospice/palliative care service.
o Each participant will receive 10 communication vignettes/videos via flash drive to use in their future ELNEC courses.
o Up-dated resources for self-care. o Up-dated curricula. o Each participant will receive the 2015 edition of the Oxford Textbook of Palliative Nursing. o More specific information about community and rural palliative care services.
Intended Audience for Core, Critical Care, Geriatric, or Pediatric Track While ELNEC is developed by nurses for nurses, we welcome all nurses, social workers, physicians, chaplains, volunteers etc., who have an interest in palliative care.
Specific to Core, Critical Care, Geriatric, and Pediatric Course
o New role play (for ELNEC-Core only). o ELNEC modules reviewed: Introduction to Palliative Nursing, Pain Management, Symptom
Management, Ethics, Culture, Communication, Loss/Grief/Bereavement, and Final Hours. o Review new slides that can be used by ELNEC trainers when speaking about palliative care in the
community (non-healthcare professionals). o Note: These four tracks are Train-the-Trainer courses.
Intended Audience for APRN The target audience will be masters, PhD, or DNP prepared APRNs (certified registered nurse anesthetists, certified nurse‐midwives, clinical nurse specialists and certified nurse practitioners) who are clinically focused. Students in any of these graduate programs are also welcome to attend. A heavy emphasis will be on pharmacology and symptom assessment and management. Physicians and physician assistants who are interested in learning more about palliative care are welcome to attend. APRNs from a wide‐variety of clinical settings are invited to participate (e.g. acute care settings, homecare, hospices, palliative care, clinics, long‐term care/skilled nursing facilities, etc).
31
31

CONNECT TO ELNEC ANYTIME
Specific to APRN
o Nine ELNEC modules will be reviewed: Introduction to Palliative Nursing, Pain Management, Symptom Management, Communication, Final Hours with Ethical Considerations and Cultural/Spiritual Implications embedded, Finances, Quality, Education and Leadership.
o Note: APRN course is not a Train-the-Trainer course. The primary purpose of this course will be to assist YOU in increasing your knowledge about palliative care, providing you with tools to provide evidence‐based practice, and exhibiting ways to promote the work you are doing as an APRN. We do recognize that many APRNs are involved in staff development. You will certainly have the materials and resources to teach others, but the purpose and emphasis of this course is on practice issues, rather than a train‐the‐trainer model, as is with other ELNEC curricula.
Costs $575 early bird, $625 after December 18th deadline: ELNEC Core ELNEC Critical Care ELNEC Geriatric ELNEC Pediatric
$675 early bird, $725 after December 18th deadline: ELNEC APRN (Adult track only offered at this course).
*$50 discount per person when 3 or more colleagues apply from the same institution!
Registration Click Here to register! The ELNEC Summit offers the 5 ELNEC courses simultaneously. Please choose one. Early bird rate deadline is December 18th so apply now! You will register online then send in your payment form separately. Should you have any questions or issues, please contact [email protected].
Note: It is very important that you stay for the entire training. In order to receive your CE’s, you must attend the course in its entirety. No early departures. Keep this in mind when making your return flight reservations. If you are unable to attend the training in its entirety, you will not receive CE’s nor an ELNEC Trainer certificate.
CE Information Provider approved by the California Board of Registered Nursing, BRN Provider #: CEP 13380 for 13 contact hours (CE Provider: City of Hope National Medical Center/Beckman Research Institute).
Post Course After the course, we hope that the trainers go back to their institutions and educate their colleagues.
1. We ask that trainers updated their curricula every three years. If you need to update, simply Click Here for a purchase form.
2. We like to know what our trainers are doing post course. If you do hold an ELNEC training, please contact Pam Malloy at [email protected] and she will be able to give you further direction.
32
32

8
ELNEC Summit Agenda
33
33

CONNECT TO ELNEC ANYTIME
Accommodations Conference HILTON LOS ANGELES NORTH/GLENDALE & EXECUTIVE MEETING CTR 100 West Glenoaks Blvd. Glendale, CA, 91202 The Summit will be held in the Glendale Grand Ballrooms
Host Hotel Hilton Los Angles North/Glendale & Executive Meeting Ctr. 100 West Glenoaks Blvd. Glendale, CA, 91202 818.956.5466 Check In: 3:00 PM Check Out: 12:00 PM
Reservations Hotel and travel expenses are the responsibility of the participant. A block of rooms has been reserved at the hotel: Reserve Online Here If you do call in, please state that you are with the “ELNEC- City of Hope” to receive rate. Rates for rooms are: $144/night (exclusive or taxes and fees)—traditional singles/doubles. To receive these hotel rates, you must make reservations by: January 8th, 2016
(First come, first serve basis, so book early!)
Hotel Amenities Three Restaurants/Lounges, Outdoor Pools, Fitness Room, Business Center and more. Please refer to the hotel site for more amenities here.
Airport Burbank (BUR) 15 min./8 mi. Los Angeles International Airport (LAX) 40 min./25 mi.
Transportation to get from Airport to Hotel Option One: Super Shuttle
o Fee: $15 USD approx (one way shared van from BUR) o Fee: $30 USD approx (one way shared van from LAX)
For shuttle arrangements, please call or visit http://www.supershuttle.com Option Two: Taxi
o Fee: about $25 USD (BUR Airport)
Parking: Self Parking: $19.00 (Garage Parking) Valet: $24.00 (Valet Parking)
34
34

10
Local Area o ABC Studios/5.0 MI o Burke Williams Spa/7.0 MI o City Center/7.0 MI o Disneyland/40.0 MI o Dodger Stadium/6.0 MI o Downtown LA/10.0 MI o Getty Center Museum/18.0 MI o Griffith Observatory/2.0 MI o Hollywood/10.0 MI o LA Convention Center/10.0 MI o Los Angeles Zoo/3.0 MI o NBC Studios/5.0 MI o Rose Bowl/Pasadena Old Towne/4.0 MI o Universal Studios Hollywood/7.0 MI o Warner Brothers Studios/5.0 MI
More Information: Click Here
35
35

CONNECT TO ELNEC ANYTIME
General Questions
How many CEs are provided? Provider approved by the California Board of Registered Nursing, BRN Provider #: CEP 13380 for 13 contact hours (CE Provider: City of Hope National Medical Center/Beckman Research Institute).
What should I wear during the training sessions? Business casual, no jeans please. At times it can be chilly in the conference rooms so please bring a sweater just in case.
What if I need to leave 2 hours before the training is completed on the last day? It is very important that you stay for the entire training. In order to receive your CE’s, you must attend the course in its entirety. No early departures. Keep this in mind when making your return flight reservations. If you are unable to attend the training in its entirety, you will not receive CE’s nor an ELNEC Trainer certificate.
Shipping materials home that were received at the conference?
You will be given a syllabus, other books and resources. It is recommended that you do one of the following: Bring an extra, empty suitcase to take these materials home in or you may ship your materials home through the hotel. Prices will vary, depending on final destination. Expect 5-7 business days for delivery. A shipping box, tape and label will be given to you free of charge.
I have a Bachelor of Science degree in nursing and I am the sole member of the palliative care consult service at my community hospital. Can I attend the APRN course, since I am actively involved in this work?
The emphasis on the APRN course is on master and doctoral prepared advanced practice. You are encouraged to attend an ELNEC‐Core train‐the‐trainer course.
I am a PA who practices in a busy cardiology office. Could I attend ELNEC‐APRN?
Yes, you are invited to register for ELNEC‐APRN. Please note that the curriculum is written by nurses and for nurses. However, in the past 15 years of providing ELNEC education, many other members of the interdisciplinary team have attended a national and/or regional ELNEC course. Palliative Care is focused on interdisciplinary care.
I teach in a graduate program in a School of Nursing. Would the information I obtain in ELNEC- APRN provide me with materials to share with my graduate students?
Yes, you will have PowerPoint slides, case studies, and supplemental teaching materials on subjects such as pain management, symptom management, communication, leadership, etc., that you can share with your graduate students. Note: APRN courses are not Train-the-Trainer courses.
36
36

12
I attended a national ELNEC‐Core course a few years ago. Can I just order the CD from ELNEC- APRN, as I have ordered other ELNEC CDs in the past?
Because the APRN courses are so different from the other ELNEC courses, you will need to attend the APRN course in person as CDs will only be made available to those who attend the APRN course.
Will ELNEC certify me in hospice/palliative care?
ELNEC is a train-the-trainer course—not a certification course. If you are interested in obtaining certification in hospice and palliative nursing, go to the National Board for Certification of Hospice and Palliative Nurses (NBCHPN) www.nbchpn.org.
In order to renew my APRN license, I need continuing education (CE) credits related to pharmacology. Will I receive CE’s specifically related to pharmacology content?
Yes, you will receive CE’s related to pharmacology content found in the Pain, Symptom Management, and Final Hours modules.
If I have further questions, who should I contact?
Questions about registration? Please contact Andrea Garcia-Ortiz at [email protected] General questions? Please contact Pam Malloy at [email protected]
Please visit the ELNEC Website: www.aacn.nche.edu/ELNEC
Follow ELNEC!
37
37

CONNECT TO ELNEC ANYTIME
Summit Registration Form
Personal Information
First Name: Last Name: Credentials:
Home Phone #: Street Home Address:
City: State: Zip:
Preferred Email (*you will receive confirmation at this email):
Institution Information
Place of Employment: Job Title:
Phone Number: Street Address:
City: State: Zip:
License #: State of Issue:
Dietary Needs? (Vegetarian, Gluten Free, etc)
How did you hear about this conference?
*NOTE: CEs cannot be administered without the above information*
Provider approved by the California Board of Registered Nursing, BRN Provider #: CEP 13380 for 13 contact hours (CE Provider: City of Hope National Medical Center/Beckman Research Institute).
Pictures are generally taken at various ELNEC courses for purposes of promoting ELNEC to potential funders, presenting at conferences, printing in newsletters, social media, etc. Please mark “yes” or “no”, if you would like or prefer not to have your picture taken. Yes No
Name of Card Holder:
Type of Card (Visa, AMEX, etc)
Card Number: Exp. Date: Signature of Cardholder:
NOTE: Credit cards are processed through City of Hope and your statement will read, “City of Hope”
Send registration form with payment to: Make checks payable to “City of Hope/ELNEC”
ELNEC APRN-Adult Early bird fee $675 prior to December 18, 2015. After, fee is $725
$
ELNEC Core, Critical Care, Geriatrics, or Pediatrics Early bird fee $575 prior to December 18, 2015. After, fee is $625
$
*Cancellation Policy: Registrations that are cancelled up to one week before the conference will be refunded, minus a $100 administrative fee. Cancellations received with less than one week’s notice will be refunded, minus a $250 administrative fee. *There will be no refunds for no-shows.
Questions? Andrea Garcia-Ortiz at: [email protected] 626-256-4673 x 63810
Or you can send via: Fax: 626-301-8941 Email: [email protected]
Please refer to the ELNEC website for hotel information, FAQ, and more information on course:
*Special rate for ELNEC participants are available at Glendale Hilton for $144/night (exclusive of taxes and fees). Cut off for special rate is January 8, 2016, but reserve early as it’s on a first come, first serve basis!
Room Reservation Here: http://www.hilton.com/en/hi/groups/personalized/B/BURHGHF-ELNEC-20160120/index.jhtml
ATTN: Andrea Garcia-Ortiz City of Hope/NR&E 1500 E Duarte Rd, #173 Duarte, CA 91010-3000
January 21-22, 2016 38
38

Next Stop…
Tulsa, OK
ELNEC Summit September 22-23, 2016
39
39

ATTACHMENT C.1
40
40

2015 Case Management Committee
Roster
Members Marcy Adelman, RN, CCM, MSN Clinical Resource Management Palomar Health 456 E. Grand Ave. Escondido, CA 92025 O: 442-281-5551
Lynne Ashbeck VP Population Health Community Medical Centers 789 N. Medical Center Drive East Clovis, CA 93611 O: 559-324-4799
Regina Berman, RN, MA, VP, Population Health Management Memorial Care Health System 17360 Brookhurst Street Fountain Valley, CA 92708 O: 714-377-3016
Diane Brown, PhD, RN, CPHQ, FNAHQ, FAAN Executive Director, Care Coordination Kaiser Permanente, Northern California 1950 Franklin Street, 19th Floor Oakland, CA 94612 O: 510-987-3769
Therese Carrabine, RN, MS Case Management & Patient Placement Director Cedars Sinai Medical Center 8700 Beverly Blvd. Suite 2802 Los Angeles, CA 90048 O: 310-423-6966
Todd Cook Chief Care Management Officer Providence Health & Services 501 South Buena Vista Street Burbank, CA 915005 O: 818-847-3307
Karen Dunning Director of Operations, Care Coordination Sutter Health System Offices 2890 Gateway Oaks Drive, Suite250 Sacramento, CA 95833 O: 916-649-4077
Heather Esget, RN, BSN, ACM Director of Case Management Shasta Regional 1100 Butte St. Redding, CA 96001 O: 530-229-2841
41
41

2015 Case Management Committee
Tammy Hoeffel, RN, BSN Director of Case Management, Social Services and Palliative Care John Muir Medical Center-Cross Campus 1601 Ygnacio Valley Blvd Walnut Creek, CA 94596 O: 925-941-5097
Theresa Kurtinaitis, MSN, RN Vice President, Case Management SHARP Healthcare 8695 Spectrum Center Blvd. San Diego, CA 92123 O: 858-499-3106
Toby Marsh, RN, MSA, MSN, FACHE, NEA-BC Director, Patient Care Services UC Davis 2315 Stockton Boulevard, Suite 4305 Sacramento, CA 95817 O: 916-734-0436
Elizabeth Miller, RN, MSN Executive Director, Care Management Adventist Health 1509 Wilson Terrace Glendale, CA 91206 O: 818-409-8264
Terri Scott, RN, BSN Regional Senior Director, Care Coordination Dignity Health/Greater Sacramento Service Area 4001 J. St. Sacramento, CA 95819 O: 916-851-2980
Ricki Stajer, RN, MA, CPHQ Vice President, Care Coordination PIH Health 12401 Washington Blvd Whittier, CA 90602 O: 562-698-0811x12780
Lisa Stroud, RN, MS, PhD (c) Director of Care Management Santa Clara Valley Medical Center 751 South Bascom Avenue San Jose, CA 95128 O: 408-885-4489
Tessie Sulit Wagoner, RN-BC, MHA, BSN, CCM, IQCI Regional Senior Director, Case Management Kindred Healthcare/West Region 200 Hospital Circle Westminster, CA 92783 O: 714-899-5020
42
42

2015 Case Management Committee
Regional Association Representatives Ivonne Der Torosian, MPA, BSM Regional Vice President-Central Valley and Central Coast Hospital Council of Northern and Central California 1625 E. Shaw, Suite 139 Fresno, CA 93710 O: 559-650-5694
Julia Slininger, RN, BS, CPHQ Vice President, Quality & Patient Safety Hospital Association of Southern California 515 Figueroa Street, Suite 1300 Los Angeles, CA 90071 O: 213-538-0766
Judith Yates Senior Vice President Hospital Association of San Diego and Imperial Counties 5575 Ruffin Road, Suite 225 San Diego, CA 92123 O: 858-614-1559
STAFF Patricia L. Blaisdell, FACHE Vice President, Continuum of Care California Hospital Association 1215 K. Street, Suite 800 Sacramento, CA 95814 O: 916-552-7553
Boris Kalanj Director, Cultural Care & Patient Experience Hospital Quality Institute 1215 K Street, Suite 900 Sacramento, CA 95814 O: 916-552-7694
Debby Rogers, RN, MS, FAEN Vice President, Clinical Performance and Transformation California Hospital Association 1215 K. Street, Suite 800 Sacramento, CA 95814 O: 916-552-7575
Marisa Ward Administrative Assistant California Hospital Association 1215 K. Street, Suite 800 Sacramento, CA 95814 O: 916-552-7656
43
43

ATTACHMENT C.2.A
44
44

State of California—Health and Human Services Agency
California Department of Public Health
RON CHAPMAN, MD, MPH EDMUND G. BROWN, JR. Director & State Health Officer Governor
November 12, 2014 AFL 14-27 TO: All Healthcare Facilities SUBJECT: AB 2139: Provision of End-of-Life Options Information and Counseling AUTHORITY: Health and Safety Code (HSC) sections 442.5 and 442.7 This All Facilities Letter (AFL) provides notice of the enactment of Assembly Bill 2139 (Chapter 568, Statutes 2014). Effective January 1, 2015, when a health care provider (an attending physician, surgeon, physician assistant, or nurse practitioner) makes a diagnosis that a patient has a terminal illness, the health care provider is required to notify the patient or, when applicable, another person authorized to make health care decisions for the patient, of the right to receive comprehensive information and counseling regarding legal end-of-life options. The notification may be provided at the time of diagnosis or at a subsequent visit in which the provider discusses treatment options with the patient or the other authorized person. The information and counseling sessions may include a discussion of treatment options in a culturally sensitive manner that the patient and his/her family or, when applicable, another person authorized to make health care decisions for the patient, can easily understand. If the health care provider does not wish to comply with the request for that information and counselling, the health care provider shall do both of the following:
refer or transfer the patient to another health care provider for provision of that information and
provide the patient, or the person authorized to make health care decisions for the patient, with information on procedures to transfer to another health care provider that shall provide the requested information.
Center for Health Care Quality, MS 0512 P.O. Box 997377 Sacramento, CA 95899-7377 (916) 324-6630 ● (916) 324-4820 FAX
Internet Address: www.cdph.ca.gov
45
45

AFL 14-27 November 12, 2014 Page 2
Please note that facilities are responsible for following all applicable laws. Any failure of the California Department of Public Health to expressly notify facilities of statutory or regulatory requirements does not relieve facilities of their responsibility for following all laws and regulations. Facilities should refer to the full text of all applicable sections of the HSC and Title 22 of the California Code of Regulations to ensure compliance. If you have questions regarding any of the matters discussed in this AFL, please contact your local District Office. Sincerely, Original signed by Jean Iacino Jean Iacino Interim Deputy Director
46
46

ATTACHMENT C.2.B
47
47

CHAPTER 568 FILED WITH SECRETARY OF STATE SEPTEMBER 25, 2014 APPROVED BY GOVERNOR SEPTEMBER 25, 2014 PASSED THE SENATE AUGUST 21, 2014 PASSED THE ASSEMBLY AUGUST 25, 2014 AMENDED IN SENATE AUGUST 18, 2014 AMENDED IN ASSEMBLY MAY 13, 2014 AMENDED IN ASSEMBLY APRIL 2, 2014 INTRODUCED BY Assembly Member Eggman (Principal coauthor: Senator Leno) (Coauthors: Assembly Members Ammiano, Olsen, and Wieckowski) (Coauthors: Senators Monning and Wolk) FEBRUARY 20, 2014 An act to amend Sections 442.5 and 442.7 of the Health and Safety Code, relating to terminal illness. LEGISLATIVE COUNSEL'S DIGEST AB 2139, Eggman. End-of-life care: patient notification. Under existing law, the State Department of Public Health licenses and regulates health facilities, including hospice facilities, and the provision of hospice services. Existing law establishes the Medical Practice Act, which provides for the regulation and licensure of physicians and surgeons by the Medical Board of California. When a health care provider, as defined, makes a diagnosis that a patient has a terminal illness, existing law requires the health care provider to provide the patient, upon the patient's request, with comprehensive information and counseling regarding legal end-of-life options, as specified, and provide for the referral or transfer of a patient, as provided, if the patient's health care provider does not wish to comply with the patient's request for information on end-of-life options. This bill would apply these provisions to another person authorized to make health care decisions, as defined, for a patient with a terminal illness diagnosis. The bill would additionally require the health care provider to notify, except as specified, the patient or, when applicable, the other person authorized to make health care decisions, when the health care provider makes a diagnosis that a patient has a terminal illness, of the patient's and the other authorized person's right to comprehensive information and counseling regarding legal end-of-life care options. THE PEOPLE OF THE STATE OF CALIFORNIA DO ENACT AS FOLLOWS: SECTION 1. Section 442.5 of the Health and Safety Code is amended to read: 442.5. (a) When a health care provider makes a diagnosis that a patient has a terminal illness, the health care provider shall do both of the following: (1) Notify the patient of his or her right, or when applicable, the right of another person authorized to make health care decisions
48
48

for the patient, to comprehensive information and counseling regarding legal end-of-life options. This notification may be provided at the time of diagnosis or at a subsequent visit in which the provider discusses treatment options with the patient or the other authorized person. (2) Upon the request of the patient or another person authorized to make health care decisions for the patient, provide the patient or other authorized person with comprehensive information and counseling regarding legal end-of-life care options pursuant to this section. When a terminally ill patient is in a health facility, as defined in Section 1250, the health care provider, or medical director of the health facility if the patient's health care provider is not available, may refer the patient or other authorized person to a hospice provider or private or public agencies and community-based organizations that specialize in end-of-life care case management and consultation to receive comprehensive information and counseling regarding legal end-of-life care options. (b) If a patient or another person authorized to make health care decisions for the patient, requests information and counseling pursuant to paragraph (2) of subdivision (a), the comprehensive information shall include, but not be limited to, the following: (1) Hospice care at home or in a health care setting. (2) A prognosis with and without the continuation of disease-targeted treatment. (3) The patient's right to refusal of or withdrawal from life-sustaining treatment. (4) The patient's right to continue to pursue disease-targeted treatment, with or without concurrent palliative care. (5) The patient's right to comprehensive pain and symptom management at the end of life, including, but not limited to, adequate pain medication, treatment of nausea, palliative chemotherapy, relief of shortness of breath and fatigue, and other clinical treatments useful when a patient is actively dying. (6) The patient's right to give individual health care instruction pursuant to Section 4670 of the Probate Code, which provides the means by which a patient may provide written health care instruction, such as an advance health care directive, and the patient's right to appoint a legally recognized health care decisionmaker. (c) The information described in subdivision (b) may, but is not required to, be in writing. Health care providers may utilize information from organizations specializing in end-of-life care that provide information on factsheets and Internet Web sites to convey the information described in subdivision (b). (d) Counseling may include, but is not limited to, discussions about the outcomes for the patient and his or her family, based on the interest of the patient. Information and counseling, as described in subdivision (b), may occur over a series of meetings with the health care provider or others who may be providing the information and counseling based on the patient's needs. (e) The information and counseling sessions may include a discussion of treatment options in a culturally sensitive manner that the patient and his or her family, or, when applicable, another person authorized to make health care decisions for the patient, can easily understand. If the patient or other authorized person requests information on the costs of treatment options, including the availability of insurance and eligibility of the patient for coverage, the patient or other authorized person shall be referred to
49
49

the appropriate entity for that information. (f) The notification made pursuant to paragraph (1) of subdivision (a) shall not be required if the patient or other person authorized to make health care decisions, as defined in Section 4617 of the Probate Code, for the patient has already received the notification. (g) For purposes of this section, "health care decisions" has the meaning set fourth in Section 4617 of the Probate Code. (h) This section shall not be construed to interfere with the clinical judgment of a health care provider in recommending the course of treatment. SEC. 2. Section 442.7 of the Health and Safety Code is amended to read: 442.7. If a health care provider does not wish to comply with his or her patient's request or, when applicable, the request of another person authorized to make health care decisions, as defined in Section 4617 of the Probate Code, for the patient for information on end-of-life options, the health care provider shall do both of the following: (a) Refer or transfer a patient to another health care provider that shall provide the requested information. (b) Provide the patient or other person authorized to make health care decisions for the patient with information on procedures to transfer to another health care provider that shall provide the requested information.
50
50

ATTACHMENT E.1
51
51

Bill No. Author Location/Action CHA Position Staff Contact
Care Coordination
SB 675 Liu(D-La Cañada Flintridge)
Would require hospitals to record the name of a family caregiver, if any; notify the caregiver upon patient discharge; and provide information and instructions on post-hospital care needs, as appropriate.
Awaiting action on the Governor’s desk.
Neutral, As Amended
Pat Blaisdell/Barbara Glaser
Community Benefits
AB 1046 Dababneh(D-Encino)
Would align California’s community benefit requirements with the federal Affordable Care Act; would streamline reporting mandates and provide greater transparency and consistency in the reporting and disclosure of investments made by nonprofit hospitals to strengthen the health and well-being of their communities.
Two-year bill. Sponsor Amber Kemp/ Kathryn Scott
SB 346 Wieckowski(D-Fremont)
Would rewrite California’s existing community benefit law to expand community benefit requirements to nonprofit multispecialty clinics; would limit charity care to a multiplier of Medicare reimbursement and exclude the unreimbursed cost to hospitals for providing services to Medi-Cal patients.
Failed passage in Senate Health Committee April 29. Reconsideration granted.
Oppose Amber Kemp/ Kathryn Scott
Emergency Services
AB 172 Rodriguez(D-Pomona)
Would make an assault committed against a physician, nurse or other health care worker of a hospital or county jail, who is engaged in providing services within the emergency department, punishable by imprisonment in a county jail not exceeding one year, a fine not exceeding $2,000, or both.
Awaiting action on the Governor’s desk.
Support Gail Blanchard-Saiger/BJ Bartleson/Connie Delgado
AB 503 Rodriguez(D-Pomona)
Would permit hospitals to release patient-identifiable medical information to pre-hospital emergency medical services providers, to the California Emergency Medical Services Authority and to local emergency medical services agencies for quality assessment and improvement purposes.
Awaiting action on the Governor’s desk.
Sponsor BJ Bartleson/Connie Delgado
AB 579 Obernolte(R-Big Bear Lake)
Would create an exception to permit a general acute care hospital to operate an emergency department if all applicable licensure and building code requirements are satisfied.
Two-year bill. Sponsor BJ Bartleson/Connie Delgado
The Legislature has concluded the first year of the 2015-16 legislative session. The focus of attention will now move to the actions of the Governor, who has until midnight on October 11 to sign, veto or allow bills to become law without his signature. Details on high-priority health care-related bills CHA is tracking this legislative session are provided below. For an online version of this report that can be filtered by topic and is updated daily, visit www.calhospital.org/key-state-issues.
September 18, 2015
52
52

California Hospital Association Key State Issues Bill No. Author Location/Action CHA Position Staff Contact
Emergency Services (continued)
AB 658 Wilk(R-Santa Clarita)
Existing law establishes a default payment rate to be paid by local law enforcement to hospitals for noncontracted emergency health care services. Under AB 658, hospitals would have the option to use either the OSHPD cost-to-charge ratio or a current approved cost-to-charge ratio from the Medicare program for noncontracted emergency services, to calculate the rate to be paid by law enforcement agencies.
Signed by the Governor July 16 (Chapter 119).
Sponsor Amber Ott/Barbara Glaser
End-of-Life/Palliative Care
ABX2 15 Eggman(D-Stockton)
Introduced August 17, this special session bill enacts the End of Life Option Actauthorizing an adult who meets certain qualifications, and who has been determined by their attending physician to be suffering from a terminal disease, to make a request for medication for the purpose of ending their own life. ABX2 15 is sustantially the same as SB 128 (Wolk, D-Davis).
Awaiting action on the Governor's desk.
Oppose Jackie Garman/Barbara Glaser
SB 128 Wolk(D-Davis)
Would enact the End of Life Option Act authorizing adults who meet certain qualifications, and who have been determined by their attending physician to be suffering from a terminal illness, to make a request for medication for the purpose of ending their own life. Would provide that such a death would have no effect on a will, health care service plan or health insurance contract, and would provide civil and criminal immunity.
To be heard in Assembly Health Committee.
Oppose Jackie Garman/Barbara Glaser
AB 533 Bonta (D-Alameda)
Attempts to address “surprise billing” by out-of-network providers. The introduced version of the bill contained ambiguities that could have been interpreted to impose obligations on network hospitals to provide information they do not have and/or cannot obtain for noncontracted physicians. Amended April 15 for clarification, the bill would apply only to noncontracting individual health professionals, not to hospitals.
Two-year bill. Neutral, As Amended
Dietmar Grellmann/Tanya Robinson-Taylor
AB 1027 Gatto (D-Glendale)
Would require a health plan, at the consumer’s request, to provide information on the contracted rate between the plan and a provider or supplier for a procedure or course of treatment.
Two-year bill. Oppose Dietmar Grellmann/Tanya Robinson-Taylor
AB 1086 Dababneh (D-Encino)
Would require health plans to honor a patient’s assignment of benefits from a health plan to a physician if the patient is provided with a disclosure that the patient may be responsible for additional out-of-network costs.
Failed passage in Assembly Health Committee April 28. Reconsideration granted.
Follow, Hot Dietmar Grellmann/Tanya Robinson-Taylor
SB 137 Hernandez(D-Azusa)
Would require health plans to maintain accurate online and paper provider directories. Plans are required to notify contracted providers annually about information that will be included in the directory, and the provider must confirm its accuracy or provide updated information. If the provider does not respond and specified efforts to contact the provider have failed, a one month claim payment delay may be imposed. The delayed payment must be made within three days of a provider response.
Awaiting action on the Governor’s desk.
Neutral Dietmar Grellmann/Tanya Robinson-Taylor
SB 546 Leno (D-San Francisco)
Would require health plans and insurers in the large group market to submit rate filings to regulators. Would also require public disclosure of rate increases and supporting cost data.
Awaiting action on the Governor’s desk.
Follow Dietmar Grellmann/Tanya Robinson-Taylor
Health Coverage
Page 2
53
53

California Hospital Association Key State Issues Bill No. Author Location/Action CHA Position Staff Contact
AB 81 Wood (D-Healdsburg)
Would extend the seismic safety deadline for a new hospital in Willits to Sept. 15, 2015, which would provide time to complete construction that is already 90 percent complete. Would allow the hospital to remain fully operational while meeting the new deadline, keeping health care accessible to rural communities within the county.
Signed by the Governor July 13 (Chapter 63).
Support Cheri Hummel/Kathryn Scott
AB 232 Obernolte(R-Big Bear Lake)
Existing law authorizes the Office of Statewide Health Planning and Development (OSHPD) to grant an additional two-year extension to the seismic mandate in specified circumstances. AB 232 would authorize a critical access hospital located in the City of Tehachapi to resubmit to OSHPD its application for an extension to January 1, 2020.
Awaiting action on the Governor's desk.
Support Cheri Hummel/ Barbara Glaser
SB 483 Beall(D-San Jose)
Would require a general acute care hospital to obtain approval to provide supplemental services in an observation unit. Would require hospitals to submit financial reports to OSHPD, designate observation beds, limit observation stays to 24 hours and establish staffing ratios for observation.
Held on Suspensein Senate Appropriations Committee May 28.
Oppose Debby Rogers/Connie Delgado
Labor
AB 304 Gonzalez (D-San Diego)
Would amend the paid sick leave law that went into effect July 1, 2015. Would alter the requirements for the rate at which paid sick leave is paid, as well as the accrual requirements when an employer relies on an existing paid time off policy.
Signed by the Governor July 13 (Chapter 67).
Follow, Hot Gail Blanchard-Saiger/ Kathryn Scott
AB 850 Ridley-Thomas(D-Los Angeles)
Would require general acute care hospitals to provide health care workers who enter the room of a specified patient with specified personal protection equipment and a powered air purifying respirator. Would exceed the protection requirements established by the CDC, CDPH and the Cal/OSHA Aerosol Transmissible Disease Standard.
Two-year bill. Oppose Gail Blanchard-Saiger/ Kathryn Scott
SB 327 Hernandez(D-Azusa)
Would reject the adverse meal period decision in Gerard v. Orange Coast Memorial Medical Center, wherein the court invalidated the Industrial Welfare Commission (IWC) regulation allowing employees in the health care industry to waive one of their two meal periods, even when their shift exceeds 12 hours — a regulation in place since 1993. This bill would clarify that the IWC’s regulation has been valid since October 2000, and that hospitals, other health care employers and employees may rely on the validity of their voluntary meal period waivers.
Awaiting action on the Governor's desk.
Sponsor Gail Blanchard-Saiger/ Kathryn Scott
Medi-Cal
AB 366 Bonta(D-Alameda)
Substantially amended in Assembly Appropriations Committee. The bill would now require the Department of Health Care Services to annually submit to the Legislature a monitoring report providing an assessment of access to care in Medi-Cal and identifying a basis to evaluate the adequacy of Medi-Cal reimbursement rates and the existence of other barriers.
Held on Suspense in Senate Appropriations Committee August 27.
Support Anne McLeod/ Barbara Glaser
Health Facilities
Page 3
54
54

California Hospital Association Key State Issues Bill No. Author Location/Action CHA Position Staff Contact
Medi-Cal (continued)
SB 36 Hernandez(D-Azusa)
Proposed amendments to SB 36 would permit the director of DHCS to request one or more temporary waiver extensions to continue the operation of the current waiver, the “California Bridge to Reform Demonstration,” until the approved effective date of the subsequent waiver.
Awaiting action on the Governor's desk.
Support Amber Kemp/ Barbara Glaser
SB 243 Hernandez(D-Azusa)
Would repeal implementation of prior year Medi-Cal rate reductions, which include the 10 percent reduction to Medi-Cal providers and the retroactive amount owed to the state by hospital-based SNFs; increase payment rates for outpatient health care providers to that of Medicare payment levels; increase hospital Medi-Cal DRG rates on a one-time basis and require annual increases thereafter; and require the state to reimburse Medi-Cal managed care plans at the upper end of their rate range.
Held on Suspense in Senate Appropriations Committee May 28.
Support Anne McLeod/ Barbara Glaser
SB 586 Hernandez(D-Azusa)
Would eliminate the sunset of the “carve out" of the California Children's Services program from Medi-Cal managed care. Would require DHCS to contract with one or more Kids Integrated Delivery Systems to provide integrated care that includes existing CCS benefits and all other health care services provided under Medi-Cal.
Two-year bill. Follow, Hot Anne McLeod/ Barbara Glaser
Medical Waste
SB 225 Wieckowski(D-Fremont)
Would clarify the type of bio-hazardous bag that can be used in hospitals and the type of shipping documents required for medical waste transport, and make other clarifying amendments to the Medical Waste Management Act.
Awaiting action on the Governor’s desk.
Sponsor Cheri Hummel/Kathryn Scott
Mental Health
AB 1193 Eggman(D-Stockton)
Would require each county to implement Laura’s Law provisions unless it elects not to participate by enacting a resolution passed by the county board of supervisors that states the reasons for opting out and any facts or circumstances considered in the decision.
Held on Suspense in Assembly Appropriations Committee May 28.
Support Sheree Kruckenberg/Tanya Robinson-Taylor
AB 1194 Eggman(D-Stockton)
Would clarify involuntary commitment laws and help county mental health departments, law enforcement jurisdictions, local county counsel and officers of superior courts to more consistently evaluate and determine an individual’s level of dangerousness, including consideration of the historical course of a person’s mental health disorder.
Awaiting action on the Governor’s desk.
Support Sheree Kruckenberg/Tanya Robinson-Taylor
AB 1300 Ridley-Thomas(D-Los Angeles)
Would modernize sections 5150, 5151 and 5152 of the Welfare and Institutions Code under the Lanterman-Petris-Short Act. Would clarify and better define the 5150 detention process to establish consistent application statewide and ensure patients receive the most appropriate care in the least restrictive environment.
Two-year bill. Sponsor Sheree Kruckenberg/Tanya Robinson-Taylor
Page 4
55
55

California Hospital Association Key State Issues Bill No. Author Location/Action CHA Position Staff Contact
Nursing Services
AB 1306 Burke (D-Inglewood)
Would remove the physician supervision requirement for certified nurse midwives (CNMs) by allowing them to manage a full range of primary health services, perform peripartum care, provide emergency care when a physician is not present, and perform and repair episiotomies in all practice settings. As amended May 28, the bill subjects CNMs to a ban on corporate practice. Such a ban would be an unwarranted and precedent-setting expansion of the corporate practice ban and would create an artificial and unnecessary barrier to employment options for CNMs.
Two-year bill. Oppose Jackie Garman/David Perrott/Connie Delgado
SB 323 Hernandez(D-Azusa)
Would allow nurse practitioners to practice to the full extent of their education and training to ensure access to health care delivery systems for millions of Californians who now have access to coverage under the ACA.
Two-year bill. Support BJ Bartleson/Connie Delgado
Pharmacies
AB 258 Levine(D-San Rafael)
Would prohibit a hospital, physician or other participant in the organ transplant process from denying patients’ eligibility as organ recipients based solely on their use of medical marijuana, unless the use is clinically significant to that decision.
Signed by the Governor July 7 (Chapter 51).
Follow, Hot David Perrott/Tanya Robinson-Taylor
Public Health
AB 508 Garcia(D-Bell Gardens)
Would establish the California Maternal Quality Care Collaborative (CMQCC) within CDPH. Would require CMQCC to establish a statewide system for collecting and maintaining data related to, among other things, pregnancy-related maternal deaths. Would require hospitals that provide obstetrical services to submit information on maternal mortality to CMQCC each month.
Two-year bill. Follow, Hot David Perrott/Tanya Robinson-Taylor
AB 521 Nazarian(D-Sherman Oaks)
Would require hospitals to offer an HIV test to every patient who has blood drawn after being admitted to a hospital from the emergency department. If the patient consents, the hospital would be required to conduct the test and provide results before the patient leaves the hospital or, if that is not possible, by mail or telephone. In addition, the provider or person administering the test would need to ensure that the patient receives timely information and counseling, as appropriate, to explain the results and implications for the patient’s health.
Awaiting action on the Governor’s desk.
Oppose David Perrott/Tanya Robinson-Taylor
SB 277 Pan(D-Sacramento)
Would eliminate the exemption from immunization based on personal beliefs, but would allow exemption from future immunization requirements deemed appropriate by CDPH for either medical reasons or personal beliefs. Would exempt students in home-based private schools and students enrolled in independent study programs from the prohibition.
Signed by the Governor June 30 (Chapter 35).
Support David Perrott/Tanya Robinson-Taylor
Page 5
56
56

California Hospital Association Key State Issues Bill No. Author Location/Action CHA Position Staff Contact
Public Health (continued)
SB 792 Mendoza(D-Artesia)
Would protect children in day care centers and family day care homes from the threat of infectious diseases by requiring employees to be immunized in accordance with the CDC schedule for routine adult immunizations. Under the current mandate for immunizations for specific infectious diseases, the Legislature's intent was to provide a means to eventually achieve total immunization of appropriate age groups against several infectious diseases, including hepatitis B, measles, pertussis and others.
Awaiting action on the Governor’s desk.
Support David Perrott/Tanya Robinson-Taylor
Skilled-Nursing Facilities
AB 927 McCarty(D-Sacramento)
Would expand disclosure requirements for applicants for a license to operate a skilled-nursing facility. Would require an application be denied if a person named in the application was a director, officer, general partner or owner of even limited interest in a licensee or parent organization of a licensee of a facility, during the seven-year period prior to the application, during which that facility had a violation that resulted in specified actions or outcomes.
Two-year bill. Follow, Hot Pat Blaisdell/Jackie Garman/Barbara Glaser
AB 1518 (Committee on Aging and Long-Term Care)
Would increase access to the home and community-based Medi-Cal Nursing Facility/Acute Hospital Waiver by increasing the number of authorized waiver slots and requiring an expedited authorization process for patients in acute care hospitals who are awaiting discharge to a skilled-nursing facility.
Two-year bill. Support Pat Blaisdell/Jackie Garman/Barbara Glaser
SB 779 Hall(D-Los Angeles)
Would require CDPH to develop staff-to-patient ratio regulations for certified nursing assistants in freestanding skilled-nursing facilities that would increase required nurse staffing to 4.1 hours per patient day.
Held on Suspensein Senate Appropriations Committee May 28.
Neutral, As Amended
Pat Blaisdell/Jackie Garman/Barbara Glaser
Tobacco Tax Issues
ABX2 16 Bonta (D-Alameda)
Would raise the cost of a pack of cigarettes by $2 and would impose a tax on e-cigarettes. The tax increase is projected to raise about $1.5 billion in the first year, with the money benefitting anti-smoking programs, health services for low-income families and tobacco-related medical research. This bill is one of several tobacco-related bills in the special session on health care.
To be heard in Assembly Public Health and Developmental Services Committee.
Follow, Hot Anne McLeod/ Barbara Glaser
ABX2 19 Bonta (D-Alameda)
Would establish a new managed care organization provider tax, to be administered by the Department of Health Care Services in consultation with the Department of Managed Health Care. The provider tax will be assessed by the department on licensed health care service plans and managed care plans contracted with the department to provide Medi-Cal services. Would require health plans to report to the department specified enrollment information on a quarterly basis.
To be heard in Assembly Public Health and Developmental Services Committee.
Follow, Hot Anne McLeod/ Barbara Glaser
SBX2 13 Pan(D-Sacramento)
SBX2 13 is identical to ABX2 16. To be heard in Senate Rules Committee.
Follow, Hot Anne McLeod/ Barbara Glaser
Page 6
57
57

California Hospital Association Key State Issues Bill No. Author Location/Action CHA Position Staff Contact
Tobacco Tax Issues (continued)
ABX2 14 Hernandez(D-Azusa)
Would implement a $2 per pack increase in the tobacco tax, estimated to generate more than a billion dollars annually, as well as an equivalent tax increase on e-cigarette products. A portion of the revenue would go toward increasing Medi-Cal reimbursement rates. The remainder would go toward existing tobacco-funded programs. Would also extend the tax on Managed Care Organizations to provide additional money for the health care system and an increase of $230 million annually for regional centers and providers of services to the developmentally disabled. The MCO tax proposal generates $1.3 billion annually.
On the Senate Floor (Special Session).
Follow, Hot Anne McLeod/ Barbara Glaser
Page 7
58
58

ATTACHMENT E.8 A/B
59
59

Controlled Substance Utilization Review and Evaluation System (CURES) Original mandate: By January 1, 2016, prescribers and dispensers of controlled substances Schedule II-IV must be registered with California’s Controlled Substance Utilization Review and Evaluation System (CURES), version 2.0. The CURES database provides information on Schedule II-IV controlled substances prescribed in California. This means all pharmacists. Current update: CURES 2.0 is still in flux. The DOJ has changed plans a lot in the last few months. At this time, DOJ has user testing underway via what they are terming a “soft launch” – beta testing in real time situations with larger users, ie. UC Davis doctors, MBC and law enforcement. We don’t have feedback as to the way it is working right now. The CHA and Kaiser are working with the DOJ regarding systems compatibility and compliance dates. The goal, which has not yet been introduced, is to streamline registration which will eliminate the notary requirement. If approved, this should allow overnight registration vs. the 6 weeks it currently takes. With at least 100,000 who still need to register – a more efficient method will need to be employed to meet the current registration deadlines. The DOJ is also looking at designating non-prescribing delegates who can request reports from the database BUT it looks like the registered provider will still have to go into the system to retrieve the info. Website and official overview: http://oag.ca.gov/cures-pdmp
60
60

PRESCRIPTION DRUG MONITORING PROGRAM
Controlled Substance Utilization Review and Evaluation System (CURES)
CURES 2.0 Soft Launch and Phased Rollout
June 30, 2015
The Department of Justice (DOJ) and the Department of Consumer Affairs (DCA) are pleased to
announce that the state’s new Controlled Substance Utilization Review and Evaluation System –
commonly referred to as “CURES 2.0” – will go live on July 1, 2015. This upgraded
prescription drug monitoring program features a variety of performance improvements and
added functionality.
In order to ensure a smooth transition from the current system, CURES 2.0 will be rolled out to
users in phases over the next several months, beginning with early adoption by a select group of
users who currently use CURES and meet the CURES 2.0 security standards, including
minimum browser specifications.** DOJ is currently identifying prescribers and dispensers who
meet these criteria and will contact and coordinate their enrollment into CURES 2.0. For all
other current users, access to CURES 1.0 will not change and no action is needed at this time.
For users and entities not currently enrolled in CURES, further notification will be provided in
August as to the enrollment/registration process.
Practitioners and health systems should begin to prepare for universal adoption of the system by
January 2016, at which point all users will be required to meet CURES 2.0’s security standards.
If you have any questions please contact [email protected].
Thank you for your continued support of the CURES program.
61
61

**CURES 2.0 users will be required to use Microsoft Internet Explorer Version 11.0 or greater,
Mozilla FireFox, Google Chrome, or Safari when accessing the system.
CURES Contact Information: [email protected] or (916) 227-3843
The Controlled Substance Utilization Review and Evaluation System (CURES) is a database
containing information on Schedule II through IV controlled substances dispensed in California.
It is a valuable investigative, preventive, and educational tool for the healthcare community,
regulatory boards, and law enforcement.
The California Prescription Drug Monitoring Program (PDMP) maintains the CURES database.
The PDMP allows authorized users, including licensed healthcare prescribers eligible to
prescribe controlled substances, pharmacists authorized to dispense controlled substances, law
enforcement, and regulatory boards, to access patient controlled substance history information
maintained in CURES. The PDMP is committed to assisting in the reduction of pharmaceutical
drug diversion without affecting legitimate medical practice or patient care.
Through online access to CURES, authorized prescribers and pharmacists can quickly review
information via Patient Activity Reports (PAR) in an effort to identify and deter drug abuse and
diversion through accurate and rapid tracking of Schedule II through IV controlled substances.
In 2014, over 3.5 million PAR requests were processed.
To obtain access to CURES, prescribers and pharmacists must: (1) submit an application form
electronically; and (2) mail a notarized copy of their printed and signed Application
Confirmation, along with copies of the following supporting documents: Drug Enforcement
Administration registration certificate (prescribers only), medical or pharmacist license, and a
government-issued photo identification. Applicants can email their complete CURES
application packet to [email protected] or mail by standard U.S. mail to:
California Department of Justice
PDMP/CURES
P.O. Box 160447
Sacramento, CA 95816
62
62

The Department of Justice (DOJ) limits access to and dissemination of CURES information to
licensed prescribers, licensed pharmacists, law enforcement personnel, and regulatory board
personnel strictly for patient care or official investigatory/regulatory purposes. The DOJ pursues
regulatory and/or criminal sanctions for misuse of CURES information.
The Health Insurance Portability and Accountability Act of 1966 (HIPAA) and all confidentiality
and disclosure provisions of California law cover the information contained in CURES. All users
must comply with HIPAA Privacy Rule Requirements when using CURES.
Submission of Controlled Substance Data
California Health & Safety Code Section 11165(d) requires dispensing pharmacies, clinics, or
other dispensers of Schedule II through IV controlled substances to provide specified dispensing
information to the DOJ on a weekly basis in a format approved and accepted by the DOJ.
Currently, the ASAP 2009 Version 4.1 format is accepted.
Direct Dispense Reporting Application
The DOJ, in coordination with Atlantic Associates, Inc. (AAI), allows direct dispense prescribers
and entities, including pharmacies filling less than 25 prescriptions per month, to electronically
report dispensing data to the DOJ. The direct dispense application can be accessed on the Direct
Dispense website located at www.aaicures.com. Also available at this website are instructions on
how to apply for an account and submit dispense data. Please note that the DOJ no longer
accepts paper direct dispense reports.
To access the secured direct dispense site, dispensers must first complete the application at
http://aaicures.com/register.for.access.php. Once an application has been submitted, an email
confirmation from AAI will provide approved users with a username and temporary password.
If an email confirmation is not received within 48 hours of submitting the application, please
contact AAI at [email protected] or (800) 539-3370.
For additional information concerning controlled substance prescription data reporting, please
contact AAI at [email protected] or (800) 539-3370.
Prescription Forms (For Prescribers)
Obtain Security Prescription Forms
63
63

California law requires prescribers of any Schedule II through V controlled substance to obtain
and use tamper-resistant prescription forms ordered only from state-approved security printers.
To order tamper-resistant prescription forms, please refer to the Approved List of Security
Prescription Printers for vendors authorized by the DOJ and their contact information.
Report Lost or Stolen Prescription Forms
Reports of lost or stolen prescription forms or pads must be reported to local law enforcement
and the PDMP. Users registered with CURES can electronically report their lost or stolen
prescription forms or pads online when logged into their CURES account. A law enforcement
agency report number is required when submitting a report of lost or stolen prescription forms
to the PDMP.
For questions concerning how to report lost or stolen prescription pads or forms, please contact
the Security Prescription Printer Program at [email protected].
64
64

ATTACHMENT E.9.A/B/C
65
65

Recommendation Targeted Goal (Considered Complete When…) As defined by Hubbert Systems Consulting's August 2014 Remediation
Recommendations Report
CDPH Priority Tier
Anticipated Timeline for Initiation
Anticipated Timeline for Completion Progress Report as of February 15, 2015
1. Build a Visionary Executive Leadership Team
All vacant senior management positions are filled permanently with individuals who meet defined leadership qualifications; leadership development training has been completed; leadership qualities, competencies, and skills have been defined and communicated; and a process for ongoing evaluation of executives’ performance is in place.
High Spring 2015 Ongoing • Current CHCQ executives participating in CDPH leadership development and executive coaching program. • Deputy director, assistant deputy director, and policy and planning chief have been appointed. • Process for conducting annual management reviews is in place.
2. Create a Change Management and Governance Structure
An Executive Governance Council has been established, trained in change management, and assignment of an executive sponsor for each improvement team has been made. In addition, a written change management plan that defines the structure, governance, and processes for implementation of all recommendations will be in place.
Urgent November 2014
May 2015
• Executive Governance Council members identified, comprising CHHS, CDPH, and CHCQ representation. • Contract for project management to oversee multi-year Remediation Recommendations Work Plan is completed; hiring is proceeding for staff.
3. Expand External Stakeholder Engagement
A designated external stakeholder unit and long-term care and non-long term care advisory committees are meeting regularly. In addition, a meaningful number of items tracked in the stakeholder issues log will be satisfactorily resolved.
Urgent November 2014
November 2015
• Third Semi-Annual Stakeholder Forum to take place Sept. 4, 2015. • CHCQ meeting quarterly with all stakeholder advisory groups, with intermediate follow-up. • Developing action log to track stakeholder meeting deliverables and follow-up.
4. Develop and Implement a Strategic Plan
An L&C strategic plan including strategic objectives, measures, targets, and specific initiatives has been developed and communicated throughout the organization. In addition, there must be a plan and a clearly defined process for annual strategic planning.
High Winter 2014 Spring 2015 • Contractor hired and strategic planning offsite held for CHCQ executives and managers in early November; agenda included development of 2014- 2017 strategic map. • Draft Strategic Map developed and can be found on the CDPH web site (http://www.cdph.ca.gov/programs/Documents/CHCQStrategicMap.pdf) • Developing goals and objectives.
5. Restructure L&C for Increased Efficiency and Accountability
Restructuring efforts have been fully implemented and an ongoing plan for evaluating organizational design and structure has been incorporated into the annual strategic planning process.
High Winter 2014 Ongoing • Central Applications Unit (CAU) restructuring contract completed. Hiring staff to begin phase-in of full centralization of CAU. • Professional Certification Branch restructuring contract completed.
66
66

6. Overhaul Approach for LA County Workload Management and Oversight
All work performed by LA County on behalf of the L&C Program is overseen by a defined organizational entity that leads, plans, schedules, coordinates, communicates, tracks, evaluates, reports, and corrects, as necessary. Interim milestones include identifying a contract officer/managerand key support staff, completion of a contract administration plan, development of key performance measures and related reports, and the scheduling of regular meetings.
Urgent November 2014
November 2015 • CHCQ Branch Chief and Health Program Specialist I (retired Health Facilities Evaluator Manager II) assigned to oversight and supervision of Los Angeles County contract performance. • Completed hiring of the LA County Monitoring Unit, staffed by two nurse surveyors and a nurse supervisor. Six State Observation Survey Analysis (SOSA) surveys have been conducted. • Bi-weekly conference calls with LA Health Facilities Inspection Division (HFID) senior management regarding ongoing enforcement, provider, and operational issues. • Ongoing quality assurance audit studies for LA offices. • Bi-weekly conference calls with program managers re: workload and provider issues. • Three-year contract with LA County signed July 8, 2015, incorporating specific yearly performance metrics. • CHCQ conducted critical training in investigation and survey practices. Additional training needs will be identified and trainings conducted as needed.
7. Establish and Monitor Key Performance Indicators
The Program posts its initial Dashboard to the CDPH internet site. Urgent November 2014
November 2015
• IT staff has been dedicated to the development of an online dashboard presentation for the performance metrics now being posted in PDF format online. Developed additional metrics for dashboard reporting that follow strategic planning process. • Quarterly updates being made to CHCQ Performance Metrics and posted to the CDPH web site. SB 75 established timelines for complaint investigations and citations
8. Build Capacity for Ongoing Organizational Improvement
The Performance Management and Improvement Section has been formed, trained, and demonstrates the capability to lead and support QI/PI initiatives for the L&C Program.
Urgent November 2014
April 2016
• Preliminary discussions underway for Recommendation #5 include consideration of this recommendation. • Continued Data Integrity Group dialogue, with members from all levels of program with responsibility for data input or data use, identifying areas needing improvement (e.g. triaging, prioritizing and timeframes). • Open Complaint Data tool developed to improve performance management of district office workloads.
9. Improve Hiring and Promotion Processes
The time to hire and promote L&C staff is decreased to an average of less than two months.
High Spring 2015 Winter 2015 • Executive Governance Council members have met with CDPH Human Resources Branch executives to bring focus to this area. • A workgroup was established for HRB & L&C to collaborate on Remediation Plan items 9 and 11. • Mass HFEN hiring process implemented July 1, 2015. Standard application review and interview questions were established for all district offices.
10. Develop a Staffing Model and Workforce Plan
The Program has adopted and implemented a new methodology for projecting staffing needs and has a well- developed, comprehensive, written policies and procedures for workforce planning.
High Winter 2014 Spring 2017 • Evaluation of adjustments to workload projection process and necessary changes to related procedures. • Created a staffing model to allocate field staff based on the district office’s workload needs.
67
67

• CHCQ will continue to evaluate the accuracy and effectiveness of the DO- specific staffing model. • CHCQ has made adjustments to the inputs of the estimate’s key variables to more accurately reflect the staffing needed to accomplish mandated workload. • CHCQ will continue to evaluate the estimate model, and the methodology for estimating the key inputs.
11. Design and Implement a HFEN Recruitment Strategy and Campaign
When the vacancy rate for HFENs is less than 5% state- wide and a comprehensive long-term recruitment strategy and plan have been adopted.
Urgent November 2014
November 2015 • CDPH Web page updated to reflect current vacancies and salaries • Statewide recruitment underway with coordinated HFEN interviews at all 14 district offices. • Established a recruiter workgroup. • Completed development of recruiter contract scope of work.
12. Design and Implement an Employee Retention Plan for District Offices
The turnover rate for HFENs, District Office Supervisors, and District Office Managers is less than 10% state-wide.
High Spring 2015 Spring 2016 • Preliminary discussions related to Recommendation # 11 also considering opportunities to address this recommendation concurrently. • Developing a scope of work to focus on employee retention and onboarding techniques.
13. Improve HFEN On-Boarding and Initial Training
Improvements to HFEN on-boarding and initial training have been implemented including a HFEN mentoring program. In addition, measureable improvements to new-hire satisfaction will be accomplished, which may be evaluated using a periodic employee survey.
Medium Fall 2015 Fall 2016 • Established Onboarding and training workgroup.
14. Improve On-Boarding and Initial Training for Non-HFEN Staff
Improvements to on-boarding and initial training for all staff have been implemented. In addition, measureable improvement in new-hire satisfaction will be accomplished, which may be evaluated using a periodic employee survey.
Medium Fall 2015 Fall 2016 • Onboarding and training workgroup reviewing common elements of onboarding and orientation for non-HFEN headquarters staff.
15. Implement a Comprehensive Program for Ongoing Training and Staff Development
Improvements to ongoing training and staff development for all staff have been implemented and measureable improvement in employee satisfaction with training has been accomplished (i.e., via a periodic employee survey).
Medium Fall 2015 Fall 2016 • Executive Governance Council members have met with CDPH’s Office of Leadership and Workforce Development executives to investigate and plan for inclusion of CHCQ employees in CDPH training and staff development programming. • Monthly facilitated calls and quarterly in-person meetings in place for field staff training supervisors. • Monthly training session for field operations and HQ support staff in ASPEN software applications, data integrity, and updates in processes.
68
68

16. Develop and Implement a Leadership and Management Skills Development Program
A comprehensive leadership and management skills development program has been implemented and measureable improvement in supervisor and manager satisfaction has been accomplished.
Medium Fall 2015 Fall 2016 • Executive Governance Council members have met with CDPH’s Office of Leadership and Workforce Development executives to investigate and plan for inclusion of CHCQ managers and supervisors in CDPH leadership and management skills programming. • An academy for district office managers and administrators took place in August 2015. • Supervisor academy is scheduled for January, March, and June 2016.
17. Improve Communication, Collaboration, and Sharing of Best Practices
A comprehensive communication plan has been implemented for the L&C Program as a whole and for each of the recommendations in this report. In addition, the Program should demonstrate measureable improvement in employee satisfaction (i.e., via survey) with internal communication, collaboration, and sharing of best practices (e.g., those described in the Assessment and Gap Analysis report).
Urgent November 2014
November 2015
• CHCQ hired a stakeholder liaison/communications specialist in July 2015. • Internal CHCQ quarterly newsletter to begin publication August in 2015. • Created district office Topics and Issues Council.
18. Implement Lean Thinking for Key Work Processes
At least three key work processes, e.g., facility complaint investigations, state licensing surveys, and citation/penalty issuance, have been measurably improved (i.e., fewer hours expended, improved outcomes, or both) using the Lean Thinking approach.
High Spring 2015 Fall 2016 • Central Applications Unit restructuring contract completed. • Professional Certification Branch contract completed. • Two CHCQ Quality Improvement Teams are working with Fresno State consultants on the Complaints Investigations Process and the Citations Issuance Process.
19. Deploy IT Hardware and Software Upgrades
The business process and technology maps have been completed; policies and procedures have been updated; and requirements for IT upgrades have been approved.
Medium Fall 2015 Spring 2017 • Purchasing tablets to replace laptop computers for HFEN field staff.
20. Update Policies & Procedures Updated L&C policies and procedures are current and easily accessible to all staff. In addition, the infrastructure and necessary resources will be in place to ensure the Program’s policies and procedures remain current.
High Spring 2015 Fall 2016 • CHCQ has restructured the Policy Section to establish a “Policy Unit” consisting of a manager, three analysts, and two retired annuitants dedicated to updating policies and procedures. The manager is onboard. All analysts are expected to be onboard in August.
21. Update Regulations [Not defined in Remediation Recommendations Report.] High Spring 2015 Ongoing • Four CHCQ regulation packages have been drafted and submitted for executive level reviews during FY 15-16. • Additional staff has been hired to draft regulations, including two attorneys.
69
69

Center for Health Care Quality Semiannual Stakeholder Forum
September 4, 2015
70
70

Agenda
• Welcome and Overview • Program Updates • Healthcare Associated Infections Program
• Skilled Nursing Facilities Nursing Hours Per Patient Day
• Open Dialogue • Next Steps
71
71

Welcome and Overview
72
72

Process Overview and Ground Rules
73
73

Center for Health Care Quality Program Updates
74
74

CDPH Leadership Karen Smith, MD, MPH Director and State Health Officer Claudia Crist, RN Chief Deputy Director of Policy and Programs Brandon Nunez Chief Deputy Director of Operations Susan Fanelli Assistant Director Jean Iacino Deputy Director, CHCQ Scott Vivona Assistant Deputy Director CHCQ C.J. Howard Chief, Policy & Planning CHCQ Recruiting for 2 Field Operations Chiefs - LTC/NLTC
75
75

Long-Term Care Complaints Investigation Timeliness by District Office
July 1, 2014 – June 30, 2015
Source: http://www.cdph.ca.gov/programs/Documents/LTC_Complaints_14-15_Q1Q2_Final.pdf, (Published 2/3/15)
76
76

Long-Term Care Complaints Average Days from Receipt to Completion
Source: http://www.cdph.ca.gov/programs/Documents/LTC_Complaints_14-15_Q1Q2_Final.pdf, (Published 2/3/15)
77
77

Long-Term Care Complaints Completion Time by Intervals
78
78

Long-Term Care Entity-Reported Incidents Investigation Timeliness by District Office July 1, 2014 – June 30, 2015
Source: http://www.cdph.ca.gov/programs/Documents/LTC_ERI_14-15_Q1Q2-Final.pdf, (Published 2/3/15)
79
79

Long-Term Care Entity Reported Incidents Average Days from Receipt to Completion
80
80

Long-Term Care Entity Reported Incidents Completion Time by Intervals
Source: http://www.cdph.ca.gov/programs/Documents/LTC_ERI_14-15_Q1Q2-Final.pdf, (Published 2/3/15)
81
81

FY 15/16 Budget
• $30.4 million and 237 additional positions to conduct licensing and certification activities
• $14.8 million additional funding for Los Angeles County contract
• $2.5 million to implement quality improvement projects • dashboards • recruiting and retention strategies
• $378,000 and 3 positions to provide on-site oversight and perform workload management, training, and quality improvement activities in Los Angeles County
82
82

Health Facility Evaluator Nurse (HFEN) Mass Hiring
• Mailed 594 recruitment letters to HFEN candidates throughout the state.
• Received and screened approximately 175 applications for minimum qualifications – Approximately 150 met the minimum qualifications
• District Offices began interviewing the week of July 20th.
• As of 8/27/15, 64 pending hires
83
83

LTC Complaint Investigation Timelines
SB 75 established LTC complaint investigation timelines: • Beginning July 1, 2016, complete IJ-level
complaints within 90 days of receipt. • Beginning July 1, 2017, complete ALL LTC
complaints within 90 days of receipt. • Beginning July 1, 2018 complete all LTC
complaint within 60 days of receipt. • Beginning July 1, 2016 issue state citations
within 30 days of completing investigation.
84
84

Quality Improvement Projects • Complaint Investigations – Improve completion
timeliness of complaints • Citations – Improve timeliness of issuing state
citations • Workgroups map processes and identify delays
and barriers • Identify best practices • Implement test phase using Plan, Do, Check, Act
85
85

Questions and Comments 86
86

CHCQ Healthcare-Associated Infections (HAI) Program
Lynn Janssen, MS, CIC, CPHQ Branch Chief
87
87

Objectives
1. Describe our Program activities for preventing HAI (defined as infections that occur as a result of healthcare)
2. Discuss new defined roles for public health in - HAI surveillance and prevention - Regional approaches for the control of antimicrobial
resistant infections and C difficile diarrheal infections
88
88

HAI in California Hospitals Annual Report
• Data reported by 400 acute care hospitals (no exclusions for size) to the National Healthcare Safety Network (NHSN)
• Published via a web page that includes • Summary report of key findings and public health action • 90 data tables • Interactive map • Technical reports for each infection type
89
89

90
90

Annual Report of HAI in California Hospitals, 2013
91
91

Influenza Vaccination Among Health Care Personnel (HCP) in California
Hospitals - Annual Report • Data reported by 400 acute care hospitals to
NHSN • Published via a web page that includes report of
key findings and public health actions, 5 data tables, technical report
• 2013-2014 flu season data continued to show incremental improvement in HCP vaccination rates
• Employees – 81% • Non-employee HCP – 63%
92
92

Liaison Infection Preventionist (IP) Program • Regionally-based Liaison IPs, highly experienced,
certified in infection control and epidemiology (CIC) • Assigned approximately 45 hospitals each to perform
assessments/consult if high HAI rates • Conduct monthly regional calls to connect with their
area hospitals and relay updates from CDPH HAI Program
• Expanding to non-hospital settings through Mar 2018 Example: Oct – Mar 2016 − 60 high HAI incidence hospitals (based on 2014 published data) − 80 LTC facilities identified by CDPH L&C district offices − 68 Outpatient hemodialysis clinics − 30 Outpatient facilities at risk for unsafe injection practices
93
93

California Campaign to Prevent Bloodstream Infections in
Hemodialysis Patients
• 514 outpatient hemodialysis centers in California • HAI Program staff include a full-time Dialysis
Liaison IP and part-time nurse consultant • Five-year plan to provide onsite assessments and
strategies to prevent bloodstream infections • One-day assessments of adherence to CDC prevention
strategies with same day feedback • Webinars, website, and a one-day infection prevention
class
94
94

• CDPH & CDC onsite assessments of Ebola Treatment Hospitals Nov-Dec 2014 • 5 University of California Medical Centers: UC Davis, UC San Francisco, UCLA, UC Irvine, UC San Diego • 3 Kaiser-Permanente Hospitals: South Sacramento, Oakland, Los Angeles
• In coordination with local public health and EMS
Coordination of Ebola Hospital Preparedness
95
95

Core Actions to Address Antimicrobial Resistance (AR)
• Improve antimicrobial prescribing through antimicrobial stewardship
• Preventing infections and transmission of antimicrobial resistant pathogens
• Tracking antimicrobial resistance patterns
96
96

California is a Leader in Antimicrobial Stewardship Legislation • Senate Bill 739 – By January 1, 2008
• Hospitals required to develop process for monitoring judicious use of antibiotics, sharing results with quality improvement committee(s)
• Senate Bill 1311 – By July 1, 2015 Hospitals required to have • Antimicrobial stewardship policy in accordance with
federal/professional guidelines • Physician-supervised multidisciplinary committee • Physician or pharmacist with AS knowledge/training • Report to quality improvement committees
97
97

150 California Hospitals Participating in 2015
ASP Collaborative
Hospital Type No. (%)
Community 122 (81) Major Teaching 5 (3) Pediatrics 8 (5) Long Term Acute Care 9 (6) Critical Access 7 (5)
98
98

Regional Approach to Antimicrobial Resistance and CDI Prevention
1. Monitor adherence to infection prevention practices in hospitals and long-term care facilities • Contact precautions • Hand hygiene • Communication when transferring patients with
CDI/AR
2. Start or enhance an antimicrobial stewardship program with particular attention to CDI 30 30
3. Evaluate and enhance environmental cleaning
99
99

Orange County CDI Prevention Collaborative
100
100

Documented Patient Sharing Among Orange County CDI Collaborative
Participant Facilities
101
101

102
102

2015 Top Ten HAI Page Views Pages Avg Time
Viewed (Seconds)
1 Healthcare-Associated Infections - Main Page 73 2 California Antimicrobial Stewardship Program Initiative 180 3 HAI Information and Current Reports 124 4 Cleaning, Disinfection and Sterilization (Basics of IP course) 190 5 Who is at Risk of Getting a MRSA Infection? 84 6 What is a CLABSI? 97 7 Vancomycin-resistant Enterococci (VRE) 89 8 Carbapenem-Resistant Enterobacteriaceae (CRE) 137 9 MRSA: Methicillin-Resistant Staphylococcus aureus 97 10 Clostridium Difficile Infection (CDI) 79
103
103

Total Views – By Program January - July 2015
395,834
138,256
0
50,000
100,000
150,000
200,000
250,000
300,000
350,000
400,000
450,000
HAI Program Tobacco Program
104
104

California Injection Safety Program 105
105

CDPH HAI Program Role in Outbreak Investigations
• Subject matter experts in infection prevention and control
• Provide consultation and support to local public health agencies
• Provide guidance and recommendations to CDPH L&C and other regulatory agencies
• Coordinate with CDC content experts for up-to-date guidance and recommendations
• Coordinate outbreak investigations that cross local health jurisdiction boundaries
106
106

Notable HAI Investigations in the Past Year
1. 09/2014: Evaluation of bloodstream infections in dialysis clinics in collaboration with CDC - throughout California
2. 11/2014: Transmission of HCV in Regenerative Medicine Clinic – Santa Barbara County
3. 01/2015: Transmission of CRE via endoscopy procedures – Los Angeles County
4. 05/2015: Transmission of CRE in 13 patients at SNF – Alameda County
107
107

Summary • The HAI Program is committed to reducing HAI in California
• Using Data for Action to prioritize and focus on hospitals with high HAI incidence
• Modeling a regional approach for AR; CDI prevention is a high priority
• Ensuring preparedness for Ebola and other emerging infectious diseases
• Seeking input from the HAI Advisory Committee, providers, regulators, and local public health to enhance our efforts
108
108

Skilled Nursing Facilities Nursing Hours Per Patient Day
109
109

Staffing Audit Process
• Unannounced visits.
• 24 randomly selected dates.
• Facility must: – Document and delineate nursing service hours. – Provide average census for each audited day. – Provide exact patient day start time.
• Only direct caregivers counted toward NHPPD.
110
110

Staffing Audit Process 111
111

Quality Assurance Review and Appeal Hearings
• Quality Assurance Review Team: – Conducts final review. – Issues Statement of Deficiency outlining final audit
results. – Issues Administrative Penalty for Non-compliance of
more than 5% of audited days. • Facility May Appeal Administrative Appeal
112
112

Performance Metrics (as of July 31, 2015) Facility Audit Status (% Audited) 824 74.98%
Compliant 754 91.50%1-Day Non-Compliant 48 5.83%2-11 Days Non-Compliant ($15,000 penalty) 19 2.31%12-24 Days Non-Compliant ($30,000 penalty) 3 0.36%Not audited (Facility closed, sold, not a Skilled Nursing Facility, etc.) 0 0.00%
Penalties Issued 6$15,000 penalty 5$30,000 penalty 1
Status on Penalties Issued 6Penalty not issued (Facility closed, sold, etc.) 0Appeal hearing denied by Office of Administrative Hearings and Appeals 0Facility did not appeal 3Appeal overturned (Administrative Penalty stands) 0Appeal upheld (Administrative Penalty withdrawn) 0Appeal hearing pending 3
Penalty amount assessed 90,000$ Penalty amount rescinded (Appeal upheld) -$ Penalty amount due 45,000$ Total penalty amount collected 45,000$
http://www.cdph.ca.gov/programs/LnC/Documents/PP1-PP4-FOR-WEBSITE.PDF
113
113

Skilled Nursing Facility Nurse Staffing Survey
114
114

Skilled Nursing Facility Nurse Hours per Patient Day
• Do you think the 3.2 nursing hours per patient day standard is sufficient?
• Please share your reasoning for your response, including any supporting data.
115
115

LTC Nurse Staffing Standards
• If you think the 3.2 nursing hours per patient day standard is not sufficient for long-term care, what standard would you recommend?
• Please include any supporting data.
116
116

Long-term Care Nurse Staffing Composition
• Do you think long-term care nurse
staffing standards should have requirements specific to CNAs, LVNs, and RNs?
117
117

Long-term Care Nurse Staffing Composition
• If you think that long-term care nurse staffing standards should have requirements specific to CNAs, LVNs and RNs, what do you think would be an appropriate staffing mix?
118
118

Questions and Comments 119
119

Open Dialogue
120
120

Meeting Record and Follow-Up
Questions may be sent to: [email protected]
Meeting report and updates will be posted at:
http://cdphinternet/programs/Pages/CHCQStakeholderForum.aspx
121
121

Save the Date!
Next Semi-Annual Stakeholders’ Forum will be:
Thursday, February 25, 2016
2 p.m. to 4 p.m.
122
122

Center for Health Care Quality Licensing & Certification
Program Evaluation
August 2014 rev.
123
123

Presentation Overview • Background • Evaluation Approach • Findings • Recommendations • Next steps
124
124

Background The Center for Health Care Quality (CHCQ) • Licensing and Certification Program
‒ Approximately 1,200 staff in 14 district offices throughout state and a contract with Los Angeles County
‒ $184.158 million budget (Fiscal Year 2013-14) ‒ Responsible for enforcing state and federal statutory and
regulatory standards related to the quality of care provided by approximately 30 types of health care facilities
‒ Responsible for the certification of nurse assistants, home health aides, hemodialysis technicians and the licensure of nursing home administrators.
• Healthcare-Associated Infections Program ‒ Responsible for public reporting of infection rates and
prevention measures with California’s hospitals (located in Richmond)
125
125

Background • April 2012 CMS requirements for L&C Program
– Corrective action plan – Performance benchmarks established – Comprehensive program assessment requested
• Goal of Program Assessment:
determine the key challenges, issues and barriers impacting performance of state licensing and federal
survey and certification operations.
126
126

Background
• CDPH engaged Hubbert Systems Consulting to conduct this assessment. – Phase I: Initial Assessment – Phase II: Gap Analysis – Phase III: Recommendations – Data collected through interviews (more than
200 around the state, within and outside of CDPH), surveys, site visits, and document review
127
127

Evaluation Approach • Program evaluation focused on 7 categories of organizational
performance: – Leadership, strategic planning, customers, measurement &
analysis, workforce, operations, results • Gap analysis
– Compared current capabilities to desired / required capabilities
– Identified program strengths and opportunities for improvement
128
128

Findings STRENGTHS
• Talented staff with strong technical expertise, extensive knowledge, dedication to program mission, and a desire to serve
• Significant improvements made since 2012
• Additional improvement initiatives already underway
129
129

Findings OPPORTUNITIES FOR IMPROVEMENT:
Work Performance
• Meeting the CMS survey and certification workload expectations timely and to quality standards
• Timely re-licensing surveys • Timely closure of facility investigations • Timely closure of investigations involving certified nurse assistants,
home health aids, and certified hemodialysis technicians • Oversight of contract with Los Angeles County • Timely issuance of citations
130
130

Findings OPPORTUNITIES FOR IMPROVEMENT:
Workforce Management • Recording and analyzing staffing hours • Recruitment and retention of Health Facility Evaluator Nurses
(HFENs) • Hiring and on-boarding processes • Employee morale • Succession planning • Program-wide approach for assessing training needs
131
131

Findings OPPORTUNITIES FOR IMPROVEMENT:
Work Systems and Processes • Standardization and automation of survey and investigation
processes • Greater access to Internet while in the field • Flow of information both internally and externally • Data collection, analysis, and reporting
132
132

Findings OPPORTUNITIES FOR IMPROVEMENT:
Leadership, Management and Oversight • Strategic planning • Performance measurement and management • Organizational structure • Communication, coordination, and collaboration
133
133

Recommendations OVERVIEW – A “Remediation Roadmap” • 21 interdependent recommendations in 4 categories:
1.Leadership, strategic planning, and customer needs
2.Measurement, analysis and performance improvement
3.Workforce 4.Operations
• 100+ detailed actions and milestones • Multi-year implementation timeline
134
134

Recommendations Leadership, strategic planning and customer needs
1. Build a Visionary Executive Leadership Team
2. Create a Change Management and Governance Structure
3. Expand External Stakeholder Engagement
135
135

Recommendations Leadership, strategic planning and customer needs, continued 4. Develop and Implement a Strategic Plan
5. Restructure L&C for Increased Efficiency and Accountability
6. Overhaul Approach for LA County Workload Management and Oversight
136
136

Recommendations Measurement, analysis and performance improvement
7. Establish and Monitor Key Performance Indicators
8. Build Capacity for Ongoing Organizational Improvement
137
137

Recommendations Workforce 9. Improve Hiring and Promotion Practices
10. Develop a Staffing Model and Workforce Plan
11. Design and Implement a HFEN Recruitment Strategy and Campaign
138
138

Recommendations Workforce, continued
12. Design and Implement an Employee Retention Plan
for District Offices
13. Improve HFEN On-Boarding and Initial Training
14. Improve On-Boarding and Initial Training for Non-HFEN Staff
139
139

Recommendations Workforce, continued
15. Implement a Comprehensive Program for Ongoing
Training and Staff Development
16. Develop and Implement a Leadership and Management Skills Development Program
140
140

Recommendations Operations
17. Improve Communication, Collaboration and
Sharing of Best Practices
18.Implement Lean Thinking for Key Work Processes
19.Deploy IT Hardware and Software Upgrades
Operations
141
141

Recommendations Operations, continued 20. Update Policies & Procedures
21. Update Regulations
142
142

Implementation
The man who moves a mountain begins by carrying away small stones. • Developing performance metrics to be posted online
quarterly beginning in October 2014 • Enhancing oversight of LA County with site visits, quality
assurance projects, and training
• Modifying our estimate methodology and timekeeping system to more accurately capture workload ~Confucius
CDPH has already begun several activities related to implementing report recommendations, including:
143
143

Implementation • Holding semiannual all stakeholder meetings, the first to
occur on September 4, 2014
• Initiating senior L&C leadership in-person meetings with every District Office
• Developing a Health Facilities Evaluator specification revision package to address salary compaction, retention and promotion issues
144
144

Implementation • Contracting for business process redesign efforts in the
Centralized Applications Unit and Professional Certification Branch
• Securing approval for two new Career Executive Assignment positions to improve efficiency and accountability
145
145

Questions?
Consultants’ Reports available online at: http://www.cdph.ca.gov/programs/Pages/CenterHealthcareQuality.aspx
146
146

ATTACHMENT E.10.A/B/C
147
147

December 3, 2014 Toby Douglas Director California Department of Health Care Services 1501 Capitol Avenue Sacramento, CA 95814 SUBJECT: Health Homes for Patients with Chronic Needs Via e-mail: [email protected] Dear Director Douglas: On behalf of our more than 400 member hospitals and health systems, the California Hospital Association (CHA) is pleased to submit the attached comments on the California Department of Health Care Services’ (DHCS) draft concept paper titled, Health Homes for Patients with Complex Needs (HHPCN). We be-lieve there is a great need to create Medicaid health homes to coordinate the full range of physical health, behavioral health, and community-based long-term services and supports (LTSS) to treat the whole-person across the lifespan. CHA appreciates the Department’s emphasis in this initiative to implement and spread care models which includes coordinated, team-based care for individuals with chronic conditions, with an emphasis on per-sons with high-costs, high-risks, and high utilization who can benefit most from increased care coordina-tion , resulting in reduced hospitalizations and emergency department visits, improved patient engage-ment and decreased costs. With DHCS programs now serving nearly 11.3 million Medi-Cal members, and as the number of enrollees in Medi-Cal continues to increase, this continued emphasis on coordinated care will help the Department to achieve its mission of providing Californians with access to affordable, high-quality health care, including medical, dental, mental health, substance use disorder services, and long-term services and supports. Hospitals are the first place in which many individuals with chronic conditions seek care. As such, the partnership of hospitals is integral to this initiative’s success given their place within the medical neigh-borhood. While DHCS’ concept paper indicates that hospitals may be included as a community-based care management entity, we strongly encourage DHCS to require the inclusion of hospitals in the health home infrastructure. Hospitals are leaders in providing the core health home services outlined in DHCS’ concept paper - comprehensive care management, care coordination and health promotion, comprehen-sive transitional care, individual and family support, referral to community and social support services and use of health information exchange and technology (HIE/HIT) to link services – and their partnership should be viewed as critical to the success of this care model. Hospitals’ participation in the health home network infrastructure should be viewed as necessary given that the health home network will serve as the central point for directing patient-centered care and will be accountable for:
148
148

Director Toby Douglas Page 2 December 3, 2014
Reducing avoidable health care costs, specifically preventable hospital admissions/readmissions
and avoidable emergency room visits; Providing timely post discharge follow-up; and Improving patient outcomes by coordinating physical health, behavioral health and community-
based LTSS. Additionally, given hospitals’ leadership in their communities, hospitals have ample opportunities to en-gage patients, providers and their local communities in a variety of ways to promote the success of this initiative, including:
Convening affiliated physicians and building relationships between providers; Leveraging staff resources to assist in care coordination; Offering information technology and capital resources to primary care providers; Providing leadership and administrative expertise; and Taking on communication roles that have the potential to increase patient participation.
Given these critical roles, CHA encourages DHCS to more clearly delineate within in the final draft the important role that hospitals have played – and will continue to play – in partnering with local communi-ties to provide coordinated, whole-person care to this medically complex population. CHA appreciates the opportunity to provide feedback to DHCS on this initiative. We commend DHCS for its commitment to improve the health of all Californians; enhance quality, including the patient care experience, in all of its programs; and reduce its per capita health care program costs. We appreciate your consideration of our attached recommendations and look forward to collaborating with DHCS to provide provider education regarding this initiative. If you have any questions, please contact me at (916) 552-7536 or [email protected]. Sincerely,
Anne McLeod Senior Vice President, Health Policy & Innovation
149
149

Health Homes for Patients with Complex Needs (HHPCN) California Concept Paper
DRAFT 11/17/14
The purpose of this paper is to share DHCS’s proposed concept for the Affordable Care Act (ACA) Section 2703 health homes with the California stakeholder community in order to seek questions and comments that will inform further development of the model.
Key Components of HHPCN Medi-Cal intends to submit a Section 2703 state plan amendment (SPA) application in summer/fall of 2015, which would provide federal regulatory authority for implementing the HHPCN model for Medicaid beneficiaries. HHPCN has several key components, which are outlined below.
Target Population Per federal requirements, states can choose to define one or more of the following groups of eligible individuals for Section 2703 health home enrollment:
1. Individuals with two or more chronic conditions;2. Individuals with one chronic condition and at risk for another;3. Individuals with serious and persistent mental illness.
HHPCN will target all three categories for health home eligibility with an emphasis on persons with high-costs, high-risks, and high utilization who can benefit from increased care coordination of physical health, behavioral health, community-based LTSS and social supports, resulting in reduced hospitalizations and emergency department (ED) visits, improved patient engagement and decreased costs. Specific eligible conditions have not yet been finalized; however, the following list of eligible chronic conditions (see Table 1) is being used to develop estimates of the eligible population and their current health care costs.
Background The Medicaid Health Home State Plan Option, authorized under ACA Section 2703, allows states to create Medicaid health homes to coordinate the full range of physical health, behavioral health, and community-based long term services and supports (LTSS) needed by beneficiaries with chronic conditions. Federal matching funds are available for two years at 90%, and, if implemented in California, The California Endowment (TCE) has offered to fund the remaining 10% of funds (up to $25 million per year) required for these additional services for that same two year period. Assembly Bill 361 (AB361), enacted in 2013, authorized California to submit a Section 2703 application, subject to several conditions, including cost neutrality and an evaluation after the first two years.
Through a complementary planning process, the California State Innovation Model (CalSIM) initiative, developed a recommendation to create “Health Homes for Patients with Complex Needs” (HHPCN). This HHPCN is one of four initiatives in the CalSIM Testing application that California made to the Center for Medicare and Medicaid Innovation (CMMI). These initiatives are multi-payer. Highlights of the testing grant application are included in the attached webinar slides. Approval of the testing grant application is expected to be announced in the fall of 2014.
In collaboration with the CalSIM initiative and with respect to the requirements of Section 2703 and California’s AB 361, the state has developed a set of policy goals (see Addendum A) that will guide the planning and implementation of the HHPCN.
150
150

Table 1: Eligible Chronic Conditions
Chronic Conditions
Physical Health Behavioral Health
Asthma /COPD Diabetes Traumatic Brain Injury Hypertension Congestive Heart Failure Coronary Artery Disease Chronic Liver Disease Chronic Renal Disease Chronic Musculoskeletal HIV/AIDS Seizure Disorders Cancer
Substance Use Disorder Major Depression Bipolar Disorder Anxiety Disorder Psychotic Disorders (including Schizophrenia) Personality Disorders Cognitive Disorders Post-Traumatic Stress
The state will develop the overall eligibility criteria; either the state or the health plans will use these criteria to determine individual eligibility. Providers may have an ability to refer individuals into the eligibility determination process that is run by the state or the plans. DHCS also anticipates health home enrollment will follow an opt-out approach, with eligible individuals being assigned to a health home provider and given the opportunity to choose not to participate in this voluntary program. Health home services must be made available to all categorically-needy Medi-Cal enrollees who meet the eligibility criteria. DHCS plans to include all full scope Medi-Cal enrollees, including the Medicaid expansion aid category for patients who meet the eligibility criteria of HHPCN. For the individuals eligible via the Medicaid expansion, the state will receive 100% federal match (gradually decreasing to 90% in 2020) rather than the enhanced federal match of 90% during the first eight quarters. Acuity DHCS anticipates that eligibility criteria will be based on: a) targeted conditions, and b) specified acuity level as determined by risk analysis software and/or administrative utilization data. Patient acuity and intensity of service needs will inform tiering of services and payment. In addition, anyone who has the qualifying chronic conditions and is also chronically homeless will have specific provider requirements for care management that would otherwise be unnecessary for those who are already stably housed. Geographic Phasing Considerations The state will likely roll out health homes in a phased approach, starting with the Coordinated Care Initiative (CCI) counties (see Table 2). CCI counties are being targeted for the HHPCN initiative given that dually eligible individuals are already enrolled in managed care plans and providers in those counties already have experience with higher care coordination standards, enhanced coordination with behavioral health and community-based LTSS, and an established Medicare shared savings arrangement. Table 2: Potential HHPCN Geography Roll-Out
Date County
January 2016 CCI counties as readiness allows
July 2016 Remaining CA counties as readiness allows
151
151

Health Home Network Infrastructure Health homes as envisioned by California will be structured as a health home network with members functioning as a team to provider whole-person care coordination. This network would include a lead entity, one or more community based care management entities, and community and social support services. The care management entity must include a dedicated care manager assigned to each enrollee. DHCS will leverage California’s existing managed care, behavioral health, and community-based LTSS system infrastructure in the implementation of health homes. A visual model of the Health Homes for Patients with Complex Needs (HHPCN) Network follows:
LEAD ENTITY: QUALIFYING MEDI-CAL MANAGED CARE PLANS
Maintains overall responsibility for the health home network, including administration, network
management, health information technology and exchange (HIT/HIE)
Receives health home payment from the state and flows to partners
COMMUNITY-BASED CARE MANAGEMENT ENTITIES: Sample orgs could include: FQHCs, hospitals, clinics, IPAs, behavioral health entities
Responsible for providing the core health home services:
Dedicated care manager is located within this entity
Entity receives payment for health home services via a contract
with the plan
Makes referrals to community partners for non-Medicaid funded
services
COMMUNITY AND SOCIAL SUPPORT SERVICES: Sample organizations could include supportive housing providers, food banks, employment assistance, social services, etc
Provides services that meet the enrollees’ broader needs (e.g. supportive housing services, social
services and supports)
May not necessarily receive health home funding
Comprehensive care management
Care coordination and health promotion
Comprehensive transitional care
Individual and family support
Referral to community and social support
services
Use of (HIT/HIE) to link services
152
152

The health home network will serve as the central point for directing patient-centered care and will be accountable for:
Reducing avoidable health care costs, specifically preventable hospital admissions/readmissions and avoidable emergency room visits;
Providing timely post discharge follow-up, and
Improving patient outcomes by coordinating physical health, behavioral health and community-based LTSS.
This will be accomplished by the lead entity and the community based care management entity either through direct provision of health home services, or through contractual arrangements with appropriate providers who will be providing integration through care coordination and planning of heath care services.
Qualifying Medi-Cal Managed Care Plans can serve as health home lead entities and must partner with one or more community based care management entities for the provision of health home services. The lead entity remains responsible for all health home program requirements, including services performed by the contracted health home providers. Payment for health home services will be paid by the state to the lead entity, which will then flow payment to appropriate network partners.
Community based care management entities will provide care coordination and planning of the core health care services to all health home enrollees and will assign each enrollee a dedicated care manager.
Care management entities will utilize community and social support services to facilitate referrals, provide resource information, and provide services that meet the enrollees’ broader needs.
The enrollee’s health action plan will be under the direction of a dedicated care manager who is accountable for facilitating access to physical health care, behavioral health care, and community-based LTSS. In addition the dedicated care manager will provide linkages to community social supports, and coordinate with entities that authorize these services as necessary to support the achievement of individualized health action goals.
The intensity of services provided will correspond to the need of the enrollee, and this may be formalized through program requirements in “service tiers.”
Hospitals that are part of a health home network must have procedures in place for referring beneficiaries who seek or need treatment in a hospital emergency department or inpatient department to the enrollee’s qualified health home.
DHCS will continue to explore the models for Medi-Cal beneficiaries who are receiving services for behavioral health conditions and children who are receiving services through the California Children’s Services (CCS). Behavioral health service providers and the CCS delivery system must be substantially integrated into the health home model for beneficiaries who meet health home eligibility requirements and access services through behavioral health and CCS providers.
General Health Home Network Qualifications
Lead entity requirements - Qualifying managed care plans will serve as the lead entities of the health home
network, and will be accountable for the administration of the health home. Some administrative functions
may be able to be performed by a designee. Administrative functions could include:
153
153

Collecting encounter data from health homes and submitting service encounters to DHCS, payment disbursement, quality monitoring, contracting, reporting;
Collecting, analyzing and reporting financial, health status and performance and outcome measures to objectively determine progress towards meeting health home goals;
Establishing procedures for referring any health home enrollee who seeks or needs treatment/services to a Medicaid designated provider.
Connecting enrollees to a care management entity and dedicated care manager who can address the full breadth of clinical and social service needs for enrollees who require assistance due to complex chronic conditions, mental health and substance use disorder issues and community-based LTSS needs.
Assembling the health home network to also include partners that provide local community and social services such as facilitating referrals, sharing resource information, and providing services that meet the enrollees’ broader needs.
Community based care management entity requirements – Care management entities will include organizations such as FQHCs, hospitals, clinics, IPAs, and behavioral health entities. To qualify, organizations must demonstrate the ability to:
Actively engage the enrollee in developing a Health Action Plan; this shall be done in person whenever possible;
Reinforce and support the enrollee’s Health Action Plan;
Coordinate with authorizing and prescribing entities as necessary to reinforce and support the enrollee’s health action goals;
Advocate, educate and support the enrollee to attain and improve self-management skills
Ensure the receipt of evidence-based care;
Support enrollees and families during discharge from hospital and institutional settings, including providing evidence-based transition planning; and,
Accompany the enrollee to critical appointments. Certification Process The health home lead entity will certify care management entities through a process similar to managed care plan provider certification. DHCS will provide general guidelines and requirements and the plans will certify qualified providers to serve as partner care management entities. Provider Education and Technical Assistance (TA) The state will leverage a TA program designed through the CalSIM HHPCN program, with additional TA provided as needed. Programs will likely be available through multiple modalities with webinars and a learning collaborative for all health home network partners, and selective individual practice coaching for providers who serve a high volume of the target population. Service Definitions DHCS is assessing gaps between what Medi-Cal managed care plans and Medi-Cal behavioral health service providers currently provide and the services required under the health home provision. In the coming months, DHCS will finalize the definitions for the following core health home services (see Addendum B for draft service definitions):
• Comprehensive care management; • Care coordination and health promotion;
154
154

• Comprehensive transitional care from inpatient to other settings, including appropriate follow up; • Individual and family support, which includes authorized representatives; • Referral to community and social support services, if relevant; and, • The use of health information technology to link services, as feasible and appropriate.
Some of the population targeted for the health homes program could benefit from palliative care, and DHCS intends to include coordination and referrals for palliative care in the health home model. CalSIM will support DHCS in developing ways to enhance delivery of palliative care as a specific initiative linked to health homes. As part of the health home notification and enrollment process, DHCS will inform beneficiaries of the optional health home benefits and explain options if a member would need to choose between care management programs (e.g. TCM or health homes). From a monitoring perspective, DHCS will identify and track services via unique coding to ensure non duplication of services, which may include eligibility, plan enrollment, and payment systems. Health Information Exchange and Technology (HIE/HIT) Development of the HHPCN requires the secure exchange of information among various organizations providing services to a given enrollee. The CalSIM initiative will strive to leverage existing HIE/HIT capacity, and provide technical assistance to organizations to meet this requirement. Quality Measures and Evaluation Plan CMS has established a recommended core set of health care quality measures (see Addendum C, Table 1 for draft quality measures) that it intends to promulgate in the rulemaking process. This core set of eight measures was selected based on priority areas of behavioral health and preventive care and aligns with existing core sets for adults and children. Additional details can be found in the CMS technical specifications and resource manual. Three utilization measures (see Addendum C, Table 2) were also identified by CMS to assist with the overall federal health home evaluation, and will become a reporting requirement as well. In addition to the required core measures, the state will also track state-specific quality measures which will draw from both existing Medicaid measures and multi-payer measurement that will be driven by the CalSIM process. Initial state-specific indicators for consideration are included in the HHPCN policy goals document (see Addendum A). To the extent possible, DHCS will leverage existing managed care evaluation tools, such as a standardized patient satisfaction survey, in the health home for maximum consistency. DHCS will contract with an external evaluator prior to the start of health home program services to ensure the program is designed to allow for federal and state measurement and evaluation activities. Payment Methodology and Rates DHCS is considering a payment approach that would include a per member per month (PMPM) payment carved in to the managed care plan capitation payment. DHCS intends for the payment methodology to include tiering based on patient acuity. Further research regarding the eligible population will be needed to identify appropriate funding levels. As described in the provider section, health home payments would flow through the lead entities which will then be responsible for negotiating contracts and setting rates with qualified care management entities.
155
155

DHCS will further develop the health home payment methodology and funding once the target population, geographic area, provider standards and service definitions have been finalized. State Match CMS provides an enhanced federal financial participation (FFP) for the first eight quarters of health home operation, starting on the effective date of the SPA. This enhanced match is 90% federal funds (10% state match). The California Endowment has offered to fund the first eight quarters of (10%) state match up to a maximum of $25 million per year. Timeline DHCS intends to develop the health home model over the coming months, in collaboration with stakeholders, (see the current timeline below, Table 3). A draft model will be shared in spring 2015 with the Substance Abuse and Mental Health Services Administration (SAMHSA), as required by 2703 legislation. The timeline also includes time for optional sharing with CMS for informal feedback in early summer 2015. The current timeline plans for CMS approval by January 2016 with a program start date of January 2016. This timeframe would allow for provider education activities to occur in late 2015 and throughout 2016 to prepare additional providers for health home implementation. Table 3: Health Home Development and Implementation Timeline
9/14-1/16 DESIGN AND DECISION-MAKING
9/14 - 3/15 Meetings and stakeholder engagement process focusing on aligning model development with a multi-payer strategy
1/15 SIM test grant starts (anticipated)
3/15 Finalize SPA and remaining details of payment methodology
4/15 Required consult with Substance Abuse and Mental Health Services Administration (SAMHSA)
4/15-7/15 CMS consultation on coverage issues and reimbursement model
8/15-1/16 Ongoing stakeholder communication and early preparations
8/15 Formal submission to CMS
1/1/16 CMS approval of 2703 SPA
7/15 – 7/18 IMPLEMENTATION AND PROVIDER TECHNICAL ASSISTANCE (TA)
7/15 – 12/15 Begin to provide TA, build health home networks, and prepare for program implementation
1/16 Begin operating health homes (SPA effective date for enhanced match purposes)
12/17 End of enhanced match for first 2703 health home SPA
1/18 Completion of initial AB 361 evaluation timeframe
Stakeholder Input DHCS, in coordination with CalSIM, will initiate a stakeholder engagement process beginning in November 2014. If you have comments or questions about this concept paper, or if you wish to be included in future notices of stakeholder engagement opportunities, please send your request to the DHCS health home mailbox: [email protected]. For ongoing CalSIM updates, please send your information to [email protected].
156
156

ADDENDUM A
MULTI-PAYER DRAFT POLICY GOALS AND MEDI-CAL OBJECTIVES The California State Innovation Model (SIM) initiative Workgroup #2 focused on the Let’s Get Healthy California (LGHC) goal area of Living Well: Preventing and Managing Chronic Disease. The Workgroup’s main recommendation “to create health homes for persons with multiple chronic conditions” was included in its SIM Testing application to the Center for Medicare and Medicaid Innovation (CMMI). Specifically, this initiative focuses on the promotion and sustainability of health homes designed to manage medically complex patients with patterns of high utilization and multiple chronic conditions, who live at home, and could benefit from intensive primary care services. The initiative will not fund individual services; rather, it will be used to spread and scale the provision of these services across California. Additionally, the initiative will align incentives to move away from volume-based payments toward a value-based payment model. The initiative is similar to other health home efforts across the country – especially those that focus on high-utilizers – and in particular is similar in design to a CMMI-funded California demonstration focused on Medicare beneficiaries (the Intensive Outpatient Care Program).
OVERARCHING GOAL: TRIPLE AIM – BETTER HEALTH, BETTER CARE, LOWER COSTS
The overarching goal of the Triple Aim will continue to shape the health home effort. Multi-payer policy goals will be used to guide the development of the HHPCN and other design decisions will flow from these goals. In the near future, process and outcome measures will be identified to track progress toward these goals. In addition, there are particular program requirements for Medi-Cal to implement this initiative. Both the multi-payer policy goals and the Medi-Cal specific objectives are described below.
Multi-Payer Draft Policy Goals
Aim HHPCN Policy Goal Draft Key Indicators
Cost Reportable net cost avoidance within two years, which will require reporting period to be 18 months.
Projected: actual net costs
Projected: actual ED visits, inpatient admits, and inpatient days
Care Experience
Improve care coordination
Patient experience measure; CAHPS already used in MediCal, consider patient activation measure (PAM)
Percent of patients whose doctor’s office helps coordinate their care with other providers
Integrate palliative care into primary care delivery Terminal hospital stays that include intensive care unit days
Strengthen community linkages within heath homes
Demonstrated linkages with housing or other social services; demonstrated e-referral to CA Smokers’ Helpline
Strengthen team-based care, including use of community health workers/ promotores/ other frontline workers
Demonstrated inclusion of frontline workers
Population Health
Improve the health outcomes of people with high risk chronic diseases
Preventable hospitalizations, per 100,000 population
Overall health status reported to be good, very good, or excellent
157
157

Medi-Cal Objectives
In addition to the preceding multi-payer policy goals, Medi-Cal objectives include:
1. Ensure sufficient provider infrastructure and capacity to implement HHPCN as an entitlement
program. Because ACA Section 2703 Health Homes is an optional Medicaid entitlement benefit, DHCS
must ensure adequate provider infrastructure and access within the geographic areas that the State
selects for operation. Access must be available for all members who 1) meet the health home eligibility
requirements and 2) choose to access health home services. DHCS must also provide the services
according to the Medicaid “freedom of choice of providers” requirements.
2. Ensure that health home providers appropriately serve members experiencing homelessness.
Homelessness is a major complicating factor in the health outcomes of many chronically ill patients.
California recognized this through the enactment of Assembly Bill 361, which authorizes the state
Department of Health Care Services to create a health home program for enrollees with chronic
conditions. AB 361 requires that providers who serve homeless members to have the specific
capabilities to engage and serve these members, including making linkages (referrals) to supportive
housing and other social services.
3. Increase integration of physical and behavioral health services. Beneficiaries with physical and
behavioral health issues tend to have a significantly worse prognosis for their illness and incur high
health care costs. Improving coordination or integration of physical and behavioral health services will
improve outcomes across the Triple Aim.
4. Create synergies with the Coordinated Care Initiative (CCI) in the eight participating counties.
Through Cal Medi-Connect, up to 456,000 Medi-Cal beneficiaries in eight selected counties who are
seniors or people with disabilities and also receive Medicare benefits (dual-eligibles) will receive
coordinated medical, behavioral health, long-term institutional, and home-and community-based
services through an organized delivery system. The Center for Medicare and Medicaid Services (CMS)
requires that dually eligible beneficiaries are included in health home initiatives in order to receive
enhanced federal matching funds. Because California has a waiver to provide comprehensive services
to this population it will be important to ensure that any services under the health home initiative are
additive to the Medi-Connect program.
5. Maximize federal funding while also achieving fiscal sustainability after eight quarters of federal
funding. After eight quarters, the federal match for health home services will be reduced from 90% to
50%. For the health homes initiative to continue it will be imperative to demonstrate a net return on
investment within two years after implementation, per the following AB361 requirements:
a. DHCS must complete a Health Home program evaluation within two years after
implementation.
b. DHCS may only implement a Health Home program if DHCS makes prior, and ongoing,
projections that no additional General Fund monies will be used to fund the program
administration, evaluation, and services. DHCS may use General Fund monies to operate the
program but the program can not result in a net increase in ongoing General Fund costs for the
Medi-Cal program.
158
158

ADDENDUM B
Service Definitions
Comprehensive Care Management
Comprehensive care management primarily involves the activities related to developing the enrollees’
comprehensive, individualized care plan, called a health action plan (HAP). HAPs should incorporate the
patient’s physical health needs, behavioral health needs and any community-based LTSS. Care
management services include screenings and assessments with standardized tools, and issues identified will
be included in the HAP. HAPs will be reassessed based on the enrollees’ progress or changes in their needs.
Dedicated care managers assess enrollees’ readiness for self-management and promote self-management
skills so the enrollee is better able to engage with health and service providers and support the
achievement of self-directed, individualized health goals to attain recovery, improve functional or health
status, or prevent or slow declines in functioning. As appropriate, the enrollee’s family should be
incorporated in the initial health assessments and subsequent reassessments. Referrals and HAP goals
should also be tracked via the HAP. The dedicated care manager will deliver this service, primarily in-
person.
Care Coordination and Health Promotion
Care coordination includes the implementation of the enrollees’ comprehensive, individualized care plan,
or HAP. At a minimum, the care coordination function includes: developing a person-centered plan based
on needs and desires of the enrollee; sharing options with the enrollee for accessing care; providing
information to the enrollee regarding care planning; monitor medications and treatment adherence by
enrollees; managing referrals, coordination and follow-up to needed services and supports. Care
coordination may include case conferences in order to ensure that the enrollees’ care is continuous and
integrated among all service providers. The dedicated care manager will deliver this service with the work
occurring in a variety of settings.
Comprehensive Transitional Care
Comprehensive transitional care addresses the activities related to preventing patient admissions and
readmissions. It requires the health home to have a process in place for prompt notification of an
enrollees’ admission or discharge to/from an emergency department, hospital inpatient facility,
residential/treatment facility, or other. At a minimum, the care transition function includes: receipt of a
summary care record or discharge summary; medication reconciliation; planning related to the timely
scheduling of follow-up appointments with recommended outpatient providers and/or community
partners. Both the managed care plan and care management entity, led by the dedicated care manager,
will be involved in the delivery of this service.
Individual and Family Support Services
Individual and family support services include activities that ensure that enrollees and their families are
knowledgeable about the enrollees’ conditions with the overall goal of improving the enrollees’ adherence
to treatment. Communication and information shared with the enrollees and their families and care givers
should meet health literacy standards and be culturally appropriate. At a minimum, individual and family
support services could include: use of peer supports and/or support groups to work with enrollees and their
159
159

families; use of self-care programs to help increase enrollees’ understanding of their conditions and care
plan. In addition, this service may include advocacy for the enrollees and their families to identify and
obtain needed resources (e.g. transportation) that supports their ability to meet goals. The dedicated care
manager and peer support staff would be key to the delivery of these services.
Referral to Community and Social Supports
Referral to community and social supports addresses the identification of community-based resources to
meet the whole-person needs of the enrollee and active referral and follow-up to these resources.
Communication and information shared with the enrollees should meet health literacy standards and be
culturally appropriate. Community and social supports include but are not limited to: housing, food,
employment, child care, community-based LTSS, school and faith based services, and disability services.
The dedicated care manager and peer support staff would be key to the delivery of these services.
Use of Health Information Technology and Exchange to Link Services
To be determined.
160
160

ADDENDUM C
Quality Measures Table 1: CMS Health Home Core Measures
Measure Steward
Adult Body Mass Index (BMI) Assessment
HEDIS*
Screening for Clinical Depression and Follow-up Plan
CMS*
Plan All-Cause Readmission Rate HEDIS*
Follow-up After Hospitalization for Mental Illness HEDIS*#
Controlling High Blood Pressure HEDIS*
Care Transition – Timely Transmission of Transition Record AMA-PCPI*
Initiation and Engagement of Alcohol and Other Drug Dependence Treatment
HEDIS*
Prevention Quality Indicator (PQI) 92: Chronic Conditions Composite AHRQ * Included in Adult Core Set # Included in Child Core Set
Table 2: Utilization Measures for CMS Evaluation
Measure Steward
Ambulatory Care – Emergency Department Visits HEDIS
Inpatient Utilization CMS
Nursing Facility Utilization CMS
161
161

Health Homes for Patients with Complex Needs California Concept Paper Version 2.0
Draft 4/10/2015
A. INTRODUCTION 3
1. BACKGROUND 3 2. STATUTORY AUTHORITY 3 3. GUIDING PRINCIPLES 4
Overarching Goal: Triple Aim – Better Care, Better Health, Lower Costs 4
B. CALIFORNIA HEALTH HOME SERVICE MODEL 6
1. ELIGIBILITY CRITERIA 6 Target Population 6 Acuity 7 Eligibility Criteria Selection Data Analysis 7
2. HEALTH HOME SERVICES 8 Comprehensive Care Management 8 Care Coordination and Health Promotion 9 Comprehensive Transitional Care 9 Individual and Family Support Services 9 Referral to Community and Social Supports 9 Use of Health Information Technology and Exchange to Link Services 9
3. HHP NETWORK INFRASTRUCTURE 10 4. MEDI-CAL MANAGED CARE PLAN RESPONSIBILITIES 12
Qualifications 12 Certification 13 Duties 13
5. COMMUNITY BASED CARE MANAGEMENT ENTITY 13 Qualifications 14 Certification 15 Duties 15 Multi-Disciplinary Health Home Team 16
6. BENEFICIARY ASSIGNMENT 18 Assignment/Enrollment 18 Referral 19 Consent 19 Discharge 19
7. PAYMENT METHODOLOGIES 19 8. REPORTING 20
C. ADDITIONAL PROGRAM ELEMENTS AND TIMELINE 21
1. HHP INTERACTION WITH EXISTING MEDI-CAL PROGRAMS 21 Mental Health and Substance Use Disorder 21 Targeted Case Management / 1915 C Waiver 22
162
162

1115 Waiver Renewal 22 2. CURRENT STATUS OF IMPLEMENTATION 23
Timeline 23 Geographic Phasing 24 County Readiness 24
3. TECHNICAL ASSISTANCE 24 4. PROGRAM EVALUATION 25 5. STAKEHOLDER ENGAGEMENT PRIOR TO SPA SUBMISSION 26
163
163

A. Introduction This Health Homes for Patients with Complex Needs (herein referred to as Health Home Program or HHP) California Concept Paper Version 2.0 is the culmination of policy development activities to date on this important project. HHP Concept Paper Version 2.0 is an enhancement to the HHPCN California Concept Paper released on 11/17/2014. DHCS has matured various policy areas and considered stakeholder input to prepare this paper. HHP Concept Paper Version 2.0 Section A. provides a recap of the enabling legislation and guiding principles, and is followed in Section B. by a review of the policy parameters of the Health Home Program. Section C. provides information about the interaction of the Health Home Program with existing Medi-Cal programs, project status and a discussion of ongoing stakeholder engagement.
1. Background
The Medicaid Health Home State Plan Option is afforded to states under the Patient Protection and Affordable Care Act (Pub. L. 111-148), enacted on March 23, 2010, as revised by the Health Care and Education Reconciliation Act of 2010 (Pub. L. 111-152), enacted on March 30, 2010, together known as the Affordable Care Act (ACA) Section 2703 allows states to create Medicaid health homes to coordinate the full range of physical health, behavioral health, and community-based long term services and supports (LTSS) needed by beneficiaries with chronic conditions. Federal matching funds are available for two years, and, if implemented in California, The California Endowment (TCE) has offered to fund the remaining 10 percent of funds (up to $25 million per year) required for these additional services for that same two year period. Assembly Bill 361 (AB 361), enacted in 2013, authorized California to submit a Section 2703 application, subject to several conditions, including cost neutrality and an evaluation after the first two years. With respect to the requirements of Section 2703 and AB 361, the State has developed a set of policy goals (see Section A.3, Guiding Principles) that will guide the planning and implementation of the HHP. 2. Statutory Authority
Although The Center for Medicare and Medicaid Services (CMS) is obligated to develop federal regulations for ACA 2703 Health Homes there is no information currently available regarding this rulemaking process.
In California, AB 361 authorizes DHCS, subject to federal approval, to create an ACA Section 2703 HHP for beneficiaries with chronic conditions. AB 361 provides that those provisions shall not be implemented unless federal financial participation is available and that the program is cost neutral regarding State General Funds. AB 361 also requires that if DHCS implements the program, DHCS ensures that an evaluation of the program is completed and that DHCS submits a report to the appropriate policy and fiscal committees of the Legislature 2 years after implementation of the program.
164
164

3. Guiding Principles
Overarching Goal: Triple Aim – Better Care, Better Health, Lower Costs The overarching goal of the Triple Aim will continue to shape the health home effort. The Let’s Get Healthy California (LGHC) and subsequent State Health Care Innovation Plan reports supported the creation of health homes for persons with chronic conditions. A number of policy goals were established to provide a framework for policy development of health homes, as follows:
• Improve care coordination. A primary function of Health Homes is to provide increased care coordination for individuals with chronic conditions. This increased care coordination is provided through the six Health Home Services, described in Section B.2, each oriented to a specific component of whole person care coordination with the goal of improving the overall health care provided to the individual.
• Integrate palliative care into primary care delivery.
• Strengthen community linkages within health homes. Linkages to housing and social services are critical to providing whole person care in Health Homes. Requirements for strong linkages, assistance and follow-up to community resources will ensure that these resources are available to this population. In addition to linking and coordinating available social services, the multi-disciplinary care team will also encourage the HHP beneficiary to participate in evidence-based prevention programs such as diabetes management, smoking cessation, and other available programs that are documented to use best practices and have positive outcomes. Information about the availability of these programs will be provided to the beneficiary.
• Strengthen team-based care, including use of community health workers/promotores/other frontline workers. Health homes will be required to have team-based care, including community health workers. Because of the linkages to housing and other social services, and potential outreach activities, community health workers can have a role in providing Health Home services. See Section B.5 for information on multi-disciplinary care team and community health workers.
• Improve the health outcomes of people with high risk chronic diseases. • Reportable net cost avoidance within two years, which will require reporting
period to be 18 months.
In addition to the Innovation Plan goals, DHCS established objectives for the implementation of the HHP.
1. Ensure sufficient provider infrastructure and capacity to implement HHP as an
entitlement program. Because ACA Section 2703 Health Homes is an optional Medicaid entitlement benefit, DHCS must ensure adequate provider infrastructure and access within the geographic areas that the State selects for operation. Access must be available for all beneficiaries who 1) meet the health home eligibility
165
165

requirements and 2) choose to access health home services. DHCS must also provide the services according to the Medicaid “freedom of choice of providers” requirements, which means beneficiaries are allowed to choose among available providers.
2. Ensure that health home providers appropriately serve members experiencing homelessness. Homelessness is a major complicating factor in the health outcomes of many chronically ill patients. California recognized this through the enactment of AB 361, which authorizes DHCS to create a health home program for enrollees with chronic conditions. AB 361 requires that providers who serve homeless members have the specific capabilities to engage and serve these members, including making linkages (referrals) to supportive housing and other social services. There is additional information about services for homeless members throughout this document.
3. Increase integration of physical and behavioral health services. Beneficiaries with both physical and behavioral health issues tend to have a significantly worse prognosis for their conditions and incur higher health care costs. Improving coordination or integration of physical and behavioral health services will improve outcomes across the Triple Aim.
4. Create synergies with the Coordinated Care Initiative (CCI) in the seven participating counties. Through Cal Medi-Connect, Medi-Cal beneficiaries in seven selected counties who are dually-eligible for Medicare and Medi-Cal receive coordinated medical, behavioral health, long-term institutional, and home-and community-based services through an organized delivery system. CMS requires that dually-eligible beneficiaries are included in health home initiatives. It will be important to ensure that any services under the health home initiative are complementary to the Medi-Connect program.
5. Maximize federal funding while also achieving fiscal sustainability after eight quarters of federal funding. After eight quarters, the federal match for health home services will be reduced from 90 percent to 50 percent. The eligibility criteria and other program parameters being defined for the Health Home Program are intended to allow the program to be fiscally sustainable from the outset. To ensure this goal, AB 361 has the following two requirements:
a. DHCS must complete a health home program evaluation within two years after implementation.
b. DHCS may only implement a health home program if no additional General Fund monies will be used to fund the program administration, evaluation, and services. DHCS may use General Fund monies to operate the program but the program can not result in a net increase in ongoing General Fund costs for the Medi-Cal program.
The DHCS HHP has added goals to provide additional framework for the policy development process:
166
166

• Focused Program on High-Cost Beneficiaries with Chronic Conditions. The DHCS HHP will focus on a Medi-Cal population that has chronic conditions and increased utilization and cost of health care. The focused attention on this segment of the population allows for increased care coordination across the Medi-Cal system for beneficiaries meeting the program criteria.
• Wrap Increased Care Coordination Around Existing Care. Another goal of HHP is to provide the increased care coordination as close to the point of care delivery as possible in the community. In most cases it is expected to be at an appropriate site where a beneficiary chooses to receive most of their care or at an alternative site chosen by the beneficiary. Increased care coordination will be wrapped around the current care delivery for each beneficiary.
B. California Health Home Service Model
1. Eligibility Criteria
Target Population Per federal requirements, states can choose to define one or more of the following groups of eligible individuals for Section 2703 health home enrollment:
1. Individuals with two or more chronic conditions; 2. Individuals with one chronic condition and at risk for another; 3. Individuals with serious and persistent mental illness.
HHP will target all three categories for health home eligibility with an emphasis on beneficiaries with high-costs, high-risks, and high utilization who can benefit from increased care coordination of physical health, behavioral health, community-based LTSS, palliative care, and social supports, resulting in reduced hospitalizations and emergency department (ED) visits, improved HHP beneficiary engagement and decreased costs. Specific eligible conditions have not yet been finalized; however, the following list of eligible chronic conditions (see Table 1) is being used to develop estimates of the eligible population and their current health care costs.
167
167

Table 1: Eligible Chronic Conditions
Chronic Conditions Physical Health Behavioral Health
Asthma /COPD Diabetes Traumatic Brain Injury Hypertension Congestive Heart Failure Coronary Artery Disease Chronic Liver Disease Chronic Renal Disease Chronic Musculoskeletal HIV/AIDS Seizure Disorders Cancer Cognitive Disorders
Substance Related and Addictive Disorders Major Depression Disorders Bipolar Disorders Psychotic Disorders (including Schizophrenia) Personality Disorders Trauma- and Stressor- Related Disorders
Health Home services must be made available to all categorically-needy Medi-Cal beneficiaries who meet the eligibility criteria. All full scope Medi-Cal beneficiaries who meet the eligibility criteria of HHP will be included. For the beneficiaries eligible via the new Medicaid ACA optional expansion eligibility category, the State will receive 100 percent federal match (gradually decreasing to 90 percent in 2020) rather than the enhanced federal match of 90 percent during the first eight quarters.
Acuity DHCS anticipates that eligibility criteria will be based on: a) targeted conditions, and b) specified acuity level as determined by risk analysis software and/or administrative utilization data. HHP beneficiary acuity and intensity of service needs will inform tiering of services and payment. For example, program criteria may include three, or more, risk groupings of the HHP eligible beneficiaries. The higher risk groupings (tiers) would receive more intensive HHP services.
In addition, for HHP beneficiaries who are experiencing homelessness, the HHP will include requirements to address the unique needs of this specific population.
Eligibility Criteria Selection Data Analysis DHCS will review historical Medi-Cal data to identify the administrative data elements and criteria that can be used to determine HHP eligibility. The goal of the data analysis is to identify all beneficiaries who have both:
• High levels of negative health outcomes/utilization; and • Specific chronic conditions and social determinants of health that present the best
opportunity for better care management (with Health Home services) that will improve health outcomes and reduce avoidable, frequent, high-cost utilization.
168
168

After this population is identified, DHCS will determine the administrative data characteristics that 1) are unique to this group, and 2) can be used to identify eligible beneficiaries through an administrative data, or referral, eligibility process.
In general, DHCS expects that this process will identify an eligible group that represents approximately 3-5 percent of the highest risk Medi-Cal population who can benefit from additional intensive care management. DHCS will make available to stakeholders the data and process that was used to develop the eligibility criteria, as well as data on the proposed eligible population (utilization and cost, demographics, conditions), service cost assumptions, case-manager ratio assumptions, and savings assumptions. DHCS will describe the following elements for the proposed eligible population:
1. Description of the Data Set used for the analysis and what is included and excluded from
the data set. 2. Specific Eligibility Criteria - used to identify the proposed Health Home population,
including the acuity criteria and target chronic conditions. 3. Descriptive statistics regarding Health Costs and utilization for total per-member-per-
month (PMPM) costs and by major cost categories. 4. Descriptive statistics for Avoidable Utilization, such as inpatient days at various levels,
ED visits, and short-stay Skilled Nursing Facility days. 5. Demographics, including the total number eligible, percentage of Medi-Cal population,
and percentages for geographic location, race, and gender, and Medi-Cal eligibility category.
6. Descriptive statistics for chronic conditions and other social determinants of health, including percentages for specific chronic conditions, homelessness, foster care, and those who have conditions that are appropriate for specialty mental health treatment, Substance Use Disorder (SUD), and California Children’s Services (CCS) services.
The topics addressed within this Eligibility Criteria Section will be part of the technical workgroup meetings identified in the Stakeholder Engagement Prior to SPA Submission Section of this paper.
2. Health Home Services
Comprehensive Care Management Comprehensive care management primarily involves the activities related to developing the HHP beneficiary’s comprehensive, individualized care plan, called a Health Action Plan (HAP). HAPs should incorporate the HHP beneficiary’s physical health, mental health and substance use disorder, community-based LTSS, palliative care, and social support needs. Care management services include screenings and assessments with standardized tools, and issues identified will be included in the HAP. The HAP is a person-centered plan based on the needs and desires of the beneficiary. HAPs will be reassessed based on the HHP beneficiary’s progress or changes in their needs. Comprehensive care management includes assessing the HHP beneficiary’s readiness for self-management and promoting self-management skills so that the HHP beneficiary is better able to engage with health and service providers and support the achievement of self-directed, individualized health goals to attain recovery, improve functional or health status, or prevent or slow declines in
169
169

functioning. As appropriate, the HHP beneficiary’s family should be incorporated in the initial health assessments and subsequent reassessments. Referrals and HAP goals should also be tracked via the HAP.
Care Coordination and Health Promotion Care coordination includes the implementation of the HHP beneficiary’s comprehensive, individualized care plan, or HAP. At a minimum, the care coordination function includes: working with HHP beneficiary to implement a person-centered HAP; sharing options with the HHP beneficiary for accessing care; providing information to the HHP beneficiary regarding care planning; monitoring medications and treatment adherence by HHP beneficiaries; and managing referrals, coordination and follow-up to needed services and supports. Care coordination may include case conferences in order to ensure that the HHP beneficiary’s care is continuous and integrated among all service providers.
Comprehensive Transitional Care Comprehensive transitional care addresses the activities related to preventing HHP beneficiary admissions and readmissions. It requires the health home to have a process in place for prompt notification of the HHP beneficiary’s admission or discharge to/from an emergency department, hospital inpatient facility, residential/treatment facility, or other. At a minimum, the care transition function includes: receipt of a summary care record or discharge summary; medication reconciliation; planning related to the timely scheduling of follow-up appointments with recommended outpatient providers and/or community partners; and appropriate care/place to stay post-discharge.
Individual and Family Support Services Individual and family support services include activities that ensure that the HHP beneficiary and their family are knowledgeable about the HHP beneficiary’s conditions with the overall goal of improving the HHP beneficiary’s adherence to treatment. Communication and information shared with the HHP beneficiary and their family and care givers should meet health literacy standards and be culturally appropriate. At a minimum, individual and family support services could include: use of peer supports and/or support groups to work with the HHP beneficiary and their family; and use of self-care programs to help increase the HHP beneficiary’s understanding of their conditions and care plan. In addition, this service may include advocacy for the HHP beneficiary and their family to identify and obtain needed resources (e.g. transportation) that support their ability to meet goals.
Referral to Community and Social Supports Referral to community and social supports addresses the identification of community-based resources to meet the whole-person needs of the HHP beneficiary and active referral and follow-up to these resources. Communication and information shared with the HHP beneficiary should meet health literacy standards and be culturally appropriate. Community and social supports include, but are not limited to: housing, food and nutrition, employment, child care, community-based LTSS, school and faith-based services, and disability services.
Use of Health Information Technology and Exchange to Link Services Health information Technology (HIT)/Health Information Exchange (HIE) are important components of the HHP. Health Home services such as Care Coordination, Health Promotion, and Comprehensive Care Transition will be enhanced by the use of Electronic
170
170

Medical Record (EMR) systems, and HIE. DHCS has established goals for EMR/HIT/HIE use in the HHP as follows:
• Provide a HHP Beneficiary Portal • Utilize EMR/HIT/HIE to register HHP beneficiaries • Utilize EMR/HIT/HIE to perform Point of Care Charting • Utilize EMR/HIT/HIE to prepare/send/receive/consume a summary of care record for
care transitions DHCS expects organizations that are covered by the Meaningful Use requirements to utilize EMR/HIT/HIE to meet these goals. Organizations that are not covered by Meaningful Use may need a Medi-Cal Managed Care Plan (MCP) or Cal MediConnect Plan (included by reference with MCP for the remainder of this paper) to support the achievement of these goals.
3. HHP Network Infrastructure
DHCS’s Health Home implementation will utilize California’s managed care infrastructure as a critical building block. DHCS will provide Health Home services through our managed care delivery system to beneficiaries enrolled in managed care. The small percentage of Fee-For-Service (FFS) beneficiaries who meet HHP eligibility criteria will have the choice to enroll in Managed Care to receive their HHP services. Managed Care serves approximately 85 percent of full scope Medi-Cal beneficiaries and is an available choice for all full-scope Medi-Cal beneficiaries statewide.
HHP is supported by the existing services provided in the managed care environment. The MCPs’ connectivity with their provider networks facilitates the care planning, care coordination, and care transition coordination requirements of HHP, including assignment of each HHP beneficiary to a Primary Care Provider. HHP will be able to utilize the MCPs’ existing communication and reporting capabilities to perform health promotion, encounter reporting, and quality of care reporting. The care management and coordination services provided through the HHP will enhance the whole person care for beneficiaries with chronic conditions. MCPs also have existing relationships with the Medi-Cal county specialty mental health plans (MHP) in each county to facilitate care coordination. To the extent possible and reasonable DHCS will align care management methods and tools with those currently used by MCPs for care coordination, for example DHCS will look to align with Cal MediConnect where possible. This topic is included in the issues for further discussion with a technical workgroup as described in Section C.5. The HHP will be structured as a health home network with members functioning as a team to provide whole-person care coordination. This network includes MCP, one or more Community Based Care Management Entity (CB-CME), and community and social support services (taken together as the health home). The HHP will serve as the central point for directing patient-centered care and will be accountable for:
171
171

• Improving beneficiary outcomes by coordinating physical health, mental health and substance use disorder, community-based LTSS, palliative care and social support needs; and
• Reducing avoidable health care costs, specifically preventable hospital admissions/readmissions, avoidable emergency department visits, and avoidable nursing facility stays.
This will be accomplished through the partnership between MCP and the community-based care management entity (CB-CME) either through direct provision of health home services, or through contractual arrangements with appropriate providers who will be providing components of the health home services and planning and coordination of other services The MCP and CB-CME must demonstrate ability to perform each of the following functional requirements as outlined in the State Medicaid Director letter on HHPs, dated 11/16/2010. This includes documentation of the processes used to perform these functions and the methods used to assure service delivery takes place in the described manner:
1. Provide quality-driven, cost-effective, culturally appropriate, and person- and family-centered health home services;
2. Coordinate and provide access to high-quality health care services informed by evidence-based clinical practice guidelines;
3. Coordinate and provide access to preventive and health promotion services, including prevention of mental illness and substance use disorders;
4. Coordinate and provide access to mental health and substance use disorder services; 5. Coordinate and provide access to comprehensive care management, care
coordination, and transitional care across settings. Transitional care includes appropriate follow-up from inpatient to other settings, such as participation in discharge planning and facilitating transfer from a pediatric to an adult system of health care;
6. Coordinate and provide access to chronic disease management, including self-management support to HHP beneficiaries and their families;
7. Coordinate and provide access to individual and family supports, including referral to community, social support, and recovery services;
8. Coordinate and provide access to long-term care supports and services; 9. Develop a person-centered care plan for each HHP beneficiary that coordinates and
integrates all of his or her clinical and non-clinical health-care related needs and services;
10. Demonstrate a capacity to use health information technology to link services, facilitate communication among team members and between the health team and individual and family caregivers, and provide feedback to practices, as feasible and appropriate; and
11. Establish a continuous quality improvement program, and collect and report on data that permits an evaluation of increased coordination of care and chronic disease management on individual-level clinical outcomes, experience of care outcomes, and quality of care outcomes at the population level.
172
172

4. Medi-Cal Managed Care Plan Responsibilities Health Home MCPs will be responsible for the overall administration of the health home. They will have a health home addendum to an existing contract with DHCS. It is anticipated that payment will flow from DHCS to the MCP to the CB-CMEs for the provision of health home services. The MCP may also pay providers who are not included formally on the CB-CME’s multi-disciplinary health home team, but who are responsible for coordinating with the CB-CME care manager to conduct case conferences and to provide input to the HAP. These providers are separate and distinct from the roles outlined for the multi-disciplinary health home team (see Section 6 for multi-disciplinary team description). In counties that implement HHP, participation in HHP and serving as a Health Home MCP is mandatory for the following organizations. DHCS will work with these organizations to prepare for the implementation of HHP and to determine network adequacy and readiness:
• Medi-Cal managed care plans (Medicaid only benefit plans); and • Cal MediConnect plans (combined Medicaid and Medicare benefit plans)
Participation as the health home MCP is optional for the following organizations in the health home implementation counties. Based on the entities’ ability to meet the health home MCP qualifications, readiness, and ability to carry out all responsibilities and duties of the MCP, optional MCPs include:
• MHPs and Drug Medi-Cal - Organized Delivery System demonstration participants
(DMC-ODS) where the entity is an integrated Mental Health/Substance Use Disorder plan; and
• CCS Organized Delivery System entities
Additional information regarding these organizations is presented in Section C.1.
Qualifications Health home MCP shall meet the following qualifications:
1. Have authority to access Medi-Cal claims data for the population served; 2. Have an adequate network of CB-CMEs in geographic target areas for HHP to serve
eligible beneficiaries, as defined by DHCS; 3. Have the capacity to qualify and support organizations who meet the standards for
CB-CMEs, including: • Identifying organizations who meet the CB-CME standards; • Providing the infrastructure and tools necessary to support CB-CME in care
coordination; • Gathering and sharing HHP beneficiary-level information regarding health care
utilization, gaps in care and medications; • Providing outcome tools and measurement protocols to assess CB-CME
effectiveness; and
173
173

• Developing and offering learning activities that will support CB-CME in effective delivery of health home services.
Certification DHCS will ensure that MCP are qualified, both through review of certification criteria and through a readiness review process that will take place before implementation of HHP. MCP responsibilities will be incorporated into the MCP contract as an amendment and clear operational policies will be established by the MCP.
Duties MCPs will be expected to perform the following broad duties/responsibilities:
1. Attribute assigned HHP beneficiaries to CB-CMEs; 2. Sub-contract with CB-CMEs for the provision of HHP services and ensure that CB-
CMEs fulfill all required CB-CME duties and achieve HHP goals; 3. Notify the CB-CME of inpatient admissions and emergency department visits, to the
extent possible; 4. Track and share data with CB-CMEs regarding each participant’s health history; 5. Track quality measures; 6. Collect, analyze and report financial measures, health status and other measures and
outcome date to be reported during the State’s evaluation process; 7. Provide beneficiary resources (e.g. customer service, beneficiary grievances) relating
to HHP; 8. Receive payment from DHCS and disperse funds to CB-CMEs through collection and
submission of claims/encounters by the CB-CME and per the contractual agreement made between the MCP and the CB-CME;
9. Establish and maintain a data-sharing agreement that is compliant with all federal and state laws and regulations, when necessary, with other providers;
10. Ensure access to timely services for HHP beneficiaries, including seeing HHP beneficiaries within established length of time from discharge from an acute care stay;
11. Ensure participation by HHP beneficiaries’ MCP contracted providers who are not included formally on the CB-CME’s multi-disciplinary HHP team but who are responsible for coordinating with the CB-CME care manager to conduct case conferences and to provide input to the HAP. These providers are separate and distinct from the roles outlined for the multi-disciplinary HHP team (see Section 6 for multi-disciplinary team description).
5. Community Based Care Management Entity
CB-CMEs will serve as the frontline provider of health home services and will be rooted in the community. MCPs will certify and select organizations to serve as CB-CMEs through a process similar to current managed care plan provider certification and will contract with selected entities. DHCS will provide general guidelines and requirements, with assistance/input from a MCP technical workgroup in order to help MCPs select, qualify and contract with CB-CMEs.
174
174

The MCP’s development of a network of CB-CMEs should seek to promote HHP goals, with particular attention to the following goals:
• Ensuring that care management delivery and sufficient health home funding are provided at the point of care in the community.
• Ensuring that providers with experience serving frequent utilizers of health services, and those experiencing homelessness, are available as needed.
• Leveraging existing county and community provider care management infrastructure and experience where possible and appropriate.
• Utilizing community health workers in appropriate roles.
It is the intent of the HHP that CB-CMEs serve as the single entity with overall responsibility for ensuring that an assigned HHP beneficiary receives access to the full range of HHP services. It is also the intent of the HHP to provide flexibility in how the CB-CMEs are organized. CB-CMEs may subcontract with other entities or individuals to perform some CB-CME duties. Regardless of subcontracting arrangements, CB-CMEs retain overall responsibility for all CB-CME duties. DHCS encourages MCPs and CB-CMEs to utilize this flexibility, where needed, to achieve HHP goals, and in particular the four goals noted above. In situations where the MCP can demonstrate that there are insufficient entities rooted in the community that are capable or willing to provide for the full range of CB-CME duties, the MCP can perform duties of the CB-CME, or subcontract with other entities to perform these duties, with advance approval from DHCS. In addition, the MCP may provide, or subcontract with another community-based entity to provide, specific CB-CME duties to assist a CB-CME to provide the full range of CB-CME duties when this MCP assistance is the best organizational arrangement to promote HHP goals, and in particular the four goals noted above. As part of future program development work, DHCS will develop specific program requirements, with input from a stakeholder technical workgroup(s), to operationalize the four HHP goals noted above. See Section C.5 for description of technical workgroups.
Qualifications Health home CB-CMEs shall meet the following qualifications:
1. Experience serving Medi-Cal beneficiaries; 2. Comply with all program requirements; 3. Have strong, engaged organizational leadership who agree to participate in learning
activities, including in-person sessions and regularly scheduled calls; 4. Provide appropriate and timely in-person care coordination activities, as needed. If in
person communication is not possible, alternative communication methods in addition to in-person such as telemedicine or telephonic contacts may also be utilized if culturally appropriate and accessible for the HHP beneficiary to enhance access to services for HHP beneficiaries and families where geographic or other barriers exist and according to beneficiary choice;
5. Have the capacity to accompany HHP beneficiaries to critical appointments, when necessary, to assist in achieving HAP goals;
175
175

6. Agree to accept any eligible HHP beneficiaries assigned by the MCP, according to their contract with the MCP;
7. Demonstrate engagement and cooperation of area hospitals, primary care practices and behavioral health providers to collaborate with the CB-CME on whole-person care coordination;
8. As feasible, use HIT/HIE to link health home services and share relevant information with other providers involved in the HHP beneficiary’s care, in accordance with the HIT/HIE goals noted in Section 3.
Certification Organizations must be one of the following types of organizations to authorize them to serve as a CB-CME and be able to meet the qualifications and duties below:
• Community mental health center • Community health center • Hospital or hospital-based physician group or clinic • Local health department • Primary care or specialist physician or physician group • Substance use disorder treatment provider • Providers serving those that experience homelessness • Providers serving individuals/persons diagnosed with HIV/AIDS • Other entities who meet certification and qualifications of a CB-CME may serve in
this capacity if selected and certified by the MCP
Duties CB-CMEs will be expected to perform the following duties/responsibilities:
1. Responsible for care team staffing, according to HHP required staffing ratios to be determined by DHCS, and oversight of direct delivery of the core health home services;
2. Implement systematic processes and protocols to ensure beneficiary access to the multi-disciplinary health home team and overall care coordination;
3. Ensure person-centered and integrated health action planning that coordinates and integrates all of the health home beneficiary’s clinical and non-clinical health care related needs and services and social services needs and services;
4. Engage HHP beneficiaries in developing a HAP and reinforcing/maintaining the care plan in order to accomplish stated goals;
5. Coordinate with authorizing and prescribing entities as necessary to reinforce and support the HHP beneficiary’s health action goals, conducting case conferences as needed in order to ensure HHP beneficiary care is integrated among providers;
6. Support the HHP beneficiary in obtaining and improving self-management skills to prevent negative health outcomes and improve health;
7. Assure the receipt of evidence-based care; 8. Manage referrals, coordination and follow-up to needed services and supports;
actively maintain a directory of community partners for referrals; 9. Support HHP beneficiaries and families during discharge from hospital and
institutional settings, including providing evidence-based transition planning; 10. Accompany the HHP beneficiary to critical appointments when necessary;
176
176

11. Provide service in the community in which the HHP beneficiary lives so services can be provided in-person, if needed;
12. Provide 24-hour, seven days a week availability of information and emergency consultation services to HHP beneficiaries in coordination with the HHP beneficiary’s MCP nurse advice line;
13. Provide quality-driven, cost-effective health home services in a culturally competent manner that addresses health disparities and improves health literacy.
As part of future program development work, DHCS will develop specific program requirements, with input from a stakeholder technical workgroup, to address requirements for the HAP and to guide HHP staffing ratios for case managers and other staff as needed. As previously noted, beneficiary acuity and intensity of service needs will inform tiering of services and payment. Program staffing ratios will be intended to describe the human resources that are required to be solely dedicated to the HHP services. The ratios will be specific to the various service tiers.
Multi-Disciplinary Health Home Team DHCS will require the following team members on a multi-disciplinary health home team. The multi-disciplinary health home team consists of staff employed by the CB-CME that provide HHP funded services. The team will primarily be located at the CB-CME organization, except as noted above regarding organization flexibility. A HHP goal is to provide health home services where beneficiaries seek care and, thus, it is expected that staffing and the day-to-day care coordination should occur at the CB-CME level rather than at the MCP.
In addition to required CB-CME team members, the MCP may choose to also make HHP-funded payments to providers that are not explicitly part of the CB-CME team, but who serves as the HHP beneficiary’s service providers for participation in case conferences and information sharing in order to support the development and maintenance of the HHP beneficiary’s HAP. The MCP may make such payments directly to the providers or through their CB-CME requirements and funding.
Multi-Disciplinary Health Home Team Qualifications and Roles
Required Team Members
Qualifications Role
Dedicated Care Manager (CB-CME or by contract)
• Strong background in managing multi-disciplinary teams
• Paraprofessional (with appropriate training) or licensed case manager, social worker, or nurse
• Oversees provision of health home services and implementation of HAP
• Offer services where the HHP beneficiary lives and seeks care
• Connect HHP beneficiary to other social services he/she may need
• Advocate on behalf of beneficiaries with health care professionals
• Use tools like motivational
177
177

interviewing and trauma informed care practices
• Work with hospital staff to plan for discharge
• Engage eligible HHP beneficiaries
• Accompany HHP beneficiary to office visits, as needed
• Health promotion and self-management training
• Arrange transportation • Assist with linkage to social
supports • Calling HHP beneficiary to
facilitate health home visit with care manager
HHP Director (CB-CME)
• Strong background in managing multi-disciplinary teams
•
• Overall responsibility for management and operations of the team.
• Responsible for quality measures and reporting for the team
Clinical Consultant (CB-CME or MCP)
• Clinician consultant(s), who may be primary care physician, specialist physician, psychiatrist, psychologist, pharmacist, registered nurse, advanced practice nurse, nutritionist, licensed clinical social worker, or other behavioral health care professional
• Review and inform HAP • Clinical resource for care
manager, as needed • Facilitate access to primary care
and behavioral health providers, as needed to assist care manager
Community Health Workers (CB-CME or by contract)
• Paraprofessional or peer advocate
• Administrative support to care manager
• Engage eligible HHP beneficiaries
• Accompany HHP beneficiary to office visits, as needed
• Health promotion and self-management training
• Arrange transportation • Assist with linkage to social
supports • Mailing health promotion
materials • Calling HHP beneficiary to
facilitate health home visit with
178
178

care manager
For HHP Beneficiaries Experiencing Chronic Homelessness: Housing Navigator (CB-CME or by contract)
• Paraprofessional or other
qualification based on experience and knowledge of the population and processes
• Form and foster relationships with and communication between team members, housing providers, and beneficiary advocates
• Connect and assist the HHP beneficiary to get recuperative care or bridge housing
• Connect and assist the HHP beneficiary to get available permanent housing
Additional team members, such as a pharmacist or nutritionist, may be included on the multi-disciplinary team in order to meet the HHP beneficiary’s individual care coordination needs. HAP planning and coordination will require participation of other providers who may not be part of the CB-CME multi-disciplinary health home team, such as the involvement of a pharmacist for medication reconciliation for care transitions. It is the responsibility of the MCP to ensure their cooperation.
6. Beneficiary Assignment
Assignment/Enrollment DHCS will develop the overall eligibility criteria and either DHCS or the MCP will use these criteria and administrative data to determine beneficiaries who are eligible for health home services.
MCPs will be responsible for enrolling eligible beneficiaries, using state-determined, CMS-approved criteria. MCPs will link enrolled HHP beneficiaries to one of their contracted CB-CMEs and notify the HHP beneficiary via a letter. If the HHP beneficiary’s assigned primary care physician is affiliated with a CB-CME, the HHP beneficiary will be assigned to that CB-CME, unless the beneficiary chooses another CB-CME. The letter will inform the HHP beneficiary that they are eligible for heath home services, and identify their MCP and CB-CME. The letter will explain that health home participation is voluntary, beneficiaries have the opportunity to choose a different CB-CME, and that HHP beneficiaries can opt out at any time. The letter will also explain the process for opting out and include a form to return if a HHP beneficiary decides not to participate. A telephone and/or in-person engagement process may be developed to supplement or replace the letter enrollment process in certain situations. In counties where there are multiple MCPs available, the HHP beneficiary may change their MCP once per month in accordance with current MCP choice policies. Engagement of eligible HHP beneficiaries will be critical for the program success.
179
179

Referral Providers may refer eligible beneficiaries to the beneficiary’s assigned MCP to confirm if they are eligible for health home services. Referrals are more likely necessary in the situation of a new Medicaid beneficiary who may not have the Medi-Cal claims history that identifies them as health home eligible. Provider referrals will indicate that the provider has verified that the beneficiary meets the eligibility criteria stated on the referral form. The provider will submit the referral form to the MCP for confirmation. CB-CMEs cannot add beneficiaries to the health home rolls without prior approval from the MCP.
Consent Consent to participate in HHP and consent to release of information forms will be secured by the CB-CME care manager during initial visit with the HHP beneficiary. These consent forms/records will be maintained by the MCP and the CB-CME.
Discharge If an eligible beneficiary cannot be engaged within a specified period of time, opts out, or refuses or fails to participate actively in health home planning and coordination, the HHP beneficiary will be discharged from the HHP and the MCP will discontinue CB-CME health home funding for that beneficiary. If, at a later date, the eligible beneficiary decides to participate in a Health Home, the beneficiary may choose to opt-in to the HHP. DHCS will define required activities to attempt to engage beneficiary prior to discharge.
7. Payment Methodologies
As described in the provider section, health home payments will flow through the lead entities which will then be responsible for negotiating contracts and setting rates with qualified community-based care management entities or other providers to ensure the delivery of Health Home services. DHCS intends to instruct health plans to implement a three-tier payment process for health homes, based on the acuity of the patients enrolled in the program. Rates to health plans are anticipated to be developed according to this methodology. For the first three months, health homes will receive an enhanced “member engagement tier” reimbursement rate. This payment acknowledges the extensive up front work required from the health homes to assist with enrollees during comprehensive care management (e.g. engaging the enrollee, conducting initial assessments, developing the HAP). This rate will be provided for up to three months with an additional incentive payment to the health home upon completion of the HAP. The HAP must be completed before the health home can receive future payments based on patient acuity. At least one core health home service must be provided each quarter in order for a payment to be made to the health home. The health home will report every quarter that they have provided a core service to each member for whom they are receiving a health home payment.
180
180

The MCP may contract with its community-based provider network to provide Health Home Services, and/or make arrangements (via a memorandum of understanding or similar agreements) for Health Home service components. (For example, the payment methodology assumes that counties will still have responsibility for coordination of specialty mental health services; however, the MCPs will bear some HHP costs that would be associated with coordinating with the counties, on a paid or unpaid basis, dependent upon DHCS direction or MCP choice. See also the Mental Health and Substance Use Disorder Section in this document for a description of a separate county-organized Health Home MCP for beneficiaries with conditions that are appropriate for specialty mental health treatment and Substance Use Disorder needs). When the MCP has demonstrated that community-based providers are not available, not willing, or do not have the capacity, to provide Health Home services, the MCP may directly provide one or more components of the HHP services.
8. Reporting CMS has established a recommended core set of health care quality measures (see Table 1 below for draft quality measures). This core set of eight measures was selected based on priority areas of behavioral health and preventive care and aligns with existing core sets for adults and children. Additional details can be found in the CMS technical specifications and resource manual. Three utilization measures (see Table 2 below) were also identified by CMS to assist with the overall federal health home evaluation, and will become a reporting requirement as well.
In addition to the required core measures, the State will also track state-specific quality measures related to Health Home service delivery. To the extent possible, DHCS will leverage existing managed care evaluation tools, such as a standardized beneficiary satisfaction survey, in the health home for maximum consistency. DHCS will contract with an external evaluator prior to the start of HHP services to ensure the program is designed to allow for federal and state measurement and evaluation activities
181
181

Table 1: CMS Health Home Recommended Core Measures
Measure Steward
Adult Body Mass Index (BMI) Assessment
HEDIS*
Screening for Clinical Depression and Follow-up Plan
CMS*
Plan All-Cause Readmission Rate HEDIS*
Follow-up After Hospitalization for Mental Illness HEDIS*#
Controlling High Blood Pressure HEDIS*
Care Transition – Timely Transmission of Transition Record AMA-PCPI*
Initiation and Engagement of Alcohol and Other Drug Dependence Treatment
HEDIS*
Prevention Quality Indicator (PQI) 92: Chronic Conditions Composite
AHRQ
* Included in Adult Core Set # Included in Child Core Set
Table 2: Utilization Measures for CMS Evaluation
Measure Steward
Ambulatory Care – Emergency Department Visits HEDIS
Inpatient Utilization CMS
Nursing Facility Utilization CMS
C. Additional Program Elements and Timeline
1. HHP Interaction with Existing Medi-Cal Programs
Mental Health and Substance Use Disorder DHCS recognizes that coordination of mental health services will be a major component of HHP. HHP services are required to be provided for the whole person, including mental
182
182

health care. In the California HHP structure of MCPs and CB-CMEs, it is expected that direct HHP services for HHP beneficiaries will primarily occur at the CB-CMEs, even though MCPs may play a role. Therefore, it is important that CB-CMEs that have HHP beneficiaries who receive mental health services have the capability to support the various needs of their beneficiaries.
For HHP beneficiaries without conditions that are appropriate for specialty mental health treatment, it is anticipated that their physical health oriented CB-CME is an appropriate setting for their health home services. These CB-CMEs would typically be affiliated with an MCPs.
DHCS and stakeholders have noted that HHP beneficiaries with conditions that are appropriate for specialty mental health treatment may prefer to receive their primary health home services from their MHPs contracted provider acting as a designated CB-CME. To facilitate care coordination for HHP beneficiaries through a MHP designated CB-CME, DHCS is considering how to enable MHPs to perform MCP responsibilities in HHP. The current working premise is as follows (also reflected in Section B.5 Medi-Cal Managed Care Plans):
MHPs can perform MCP HHP responsibilities through a delegation contract with the MCPs in the county. Drug Medi-Cal - Organized Delivery System demonstration participants (DMC-ODS) can perform MCP HHP responsibilities where the entity is an integrated MH/SUD plan. This type of entity would perform the MCP HHP responsibilities for a health home eligible managed care beneficiary who 1) qualifies to receive services provided under the Medi-Cal scope of service for this type of entity (MHP or Drug Medi-Cal services); and 2) chooses a county MHP, or county MH/SUD plan, affiliated CB-CME instead of a CB-CME affiliated with the MCP. In cases where the MHP serves as both an administrator and a provider of direct services, the MHP could assume the responsibilities of both the MCP and a CB-CME.
Targeted Case Management / 1915 C Waiver Targeted Case Management and 1915c Home and Community Based Services Waiver programs provide services to many Medi-Cal beneficiaries who will likely also meet the eligibility criteria for HHP. Because there are comprehensive case management components within these programs and there is a federal prohibition against providing duplicative federally funded services, more investigation is required to determine the best course of actions for each program and the beneficiaries currently served by them. However, for beneficiaries who qualify for more than one of these programs, it is likely that beneficiaries will be allowed to participate in only one program and that they will have the choice regarding program participation selection. DHCS plans to continue this investigation and work with stakeholders for these important programs.
1115 Waiver Renewal DHCS recently submitted a proposal to CMS for the 1115 Waiver renewal. It contains numerous objectives for improving DHCS’s health care delivery system through improved coordination and care delivery across physical and behavioral health. There are a number of concepts in the 1115 Waiver renewal that complement a HHP such as the use of multi-
183
183

disciplinary care teams and implementation of a coordinated “no wrong door” approach for patients with chronic conditions who need care across physical and behavioral health. The effort to renew the 1115 Waiver is an iterative process with CMS. The initial concepts included in the application are subject to change and evolution and will happen concurrently with policy development of the HHP. As the 1115 Waiver development continues, DHCS will ensure that the services that are provided in counties that are also implementing Health Homes are complementary.
2. Current Status of Implementation
Timeline
Health Home Program Timeline
8/14 – 7/15 Ongoing program design. Solicit, evaluate, and incorporate stakeholder as needed.
4/15 – 7/15 One time required consult with Substance Abuse and Mental Health Services Administration (SAMHSA)
4/15 – 7/15 CMS consultation on coverage issues and reimbursement model
8/14 – 1/16 Ongoing stakeholder engagement
8/15 Formal State Plan Amendment (SPA) submission to CMS
10/15 – 12/15 CMS approval of 2703 SPA
7/15 – 7/18 Implementation & Provider Technical Assistance
7/15 – 12/15 Begin to provide TA, build health home networks, and prepare for program implementation
1/16 Begin operating HHP (SPA effective date for enhanced match purposes)
12/17 End of enhanced match for first 2703 health home SPA
1/18 Completion of initial AB 361 evaluation timeframe
184
184

Geographic Phasing ACA 2703 allows geographic phasing of Health Home services. As noted above in the ‘Managed Care’ section, DHCS believes that HHP will be successful and sustainable because of the infrastructure in the manage care environment. In CCI counties there are additional requirements that are aligned with HHP that will allow the MCPs, MHPs, and providers to better implement and operate HHP for the benefit of eligible beneficiaries.
DHCS is planning to phase the HHP implementation on a county by county basis, based upon readiness. Currently, two phases are planned, the first on January 1, 2016, for CCI counties and potential other counties that are ready. The second phase for remaining counties that demonstrate readiness is scheduled for July 1, 2016.
County Readiness DHCS recognizes that readiness in a county includes the readiness of the MCPs, MHPs, and other entities that might assume MCP HHP responsibilities; the CB-CMEs; all associated social services and supports; and the existing provider community.
All MCPs and other entities noted above, will be required to commit to and demonstrate their ability to meet the duties identified in Section B.5, and that they have the ability to assemble CB-CME networks to serve all eligible beneficiaries in the county regarding all CB-CME requirements and duties and all other specified program goals and requirements.
DHCS plans to review the readiness evaluation tool with stakeholders in the next few months.
3. Technical Assistance
The HHP will provide technical assistance (TA) for Health Home network providers (CB-CME and MCPs) through multiple modalities, including webinars and a learning collaborative for all health home network partners, and to the extent funding is available, selective individual practice coaching for providers who serve a high volume of the target population. Per federal rules, TA may not be funded with ACA Section 2703 Health Home funding, though TA may be funded through regular Medicaid funding with a 50 percent federal match. California plans to use part of it’s the Center for Medicare and Medicaid State Innovation Model design grant for Health Home TA as well as other external resources. DHCS is drafting a TA plan to prepare CB-CMEs to improve participants’ care.
Lessons learned from the Intensive Outpatient Care Program (IOCP) and from the Frequent Users of Health Services Initiative (FUHSI), a safety net program that was funded by The California Endowment and the California Health Care Foundation from 2002-2008, will be included in the TA plan.
The TA plan will include the following: • The design of a tool to conduct organizational assessments of provider organizations
identified by health plans and the State as potential CB-CMEs. The assessment tool addresses content areas, such as staff composition and data infrastructure, which are predictors of successful implementation. The assessments will be conducted telephonically with follow-up site visits where more review is warranted.
185
185

Assessments will be conducted to 1) Identify existing care coordination programs already providing CB-CME services and 2) Identify organizations with the infrastructure to build new health home programs for complex patients and qualify as a CB-CME.
• Provide two levels of TA: a. TA for existing programs qualified as CB-CMEs which includes access to
care coordinator training and a learning network to share best practices; b. TA to build new Health Homes for complex patients which includes intensive
training of organizational leaders to set up programs within their organizations and the care coordinators with responsibility for direct patient care.
4. Program Evaluation
An evaluation of the HHP within two years after implementation is required by the California authorizing legislation (AB 361). As required by CMS, the HHP must report on a core set of health care quality measures, utilization measures, and quality data. DHCS may only implement an HHP if DHCS determines that no additional General Fund monies will be used to fund the program administration, evaluation, and services. DHCS may use General Fund monies to operate the program but the program can not result in a net increase in ongoing General Fund costs for the Medi-Cal program. An external evaluator will be contracted to monitor, evaluate, and complete the final evaluation report in addition to production of various reports to inform and assess the progress of the program. The evaluation will be designed to verify the fiscal sustainability of the program design after the eight quarters of enhanced federal match and measure enrollment, utilization, expenditure, encounter, quality indicators, and other data required for reporting purposes including but not limited to avoidable hospital readmissions.
• The primary goals of the evaluation will be to assess the sustainability and impact on the
overarching Triple Aim goals of better health, better health care, and lower per capita costs while reporting on a core set of health care quality measures, utilization measures, and quality data.
• The evaluator will work with DHCS to design the evaluation and seek feedback from stakeholders on the design.
• Administrative data on active health home participants will be used to measure costs and determine methodology to measure the effect of these costs on the HHP.
• The evaluator will measure the total cost of the program. Additionally, the calculation of cost will report cost-effectiveness that result from improved coordination of care and chronic disease management achieved through the HHP.
• The receipt of timely data from all health home partners will be critical for the evaluation. Feedback to DHCS and other stakeholders throughout the program implementation period may provide strategic information to support future planning.
• The timing of the evaluation activities and products will be dependent on the speed of program implementation in each of the programs, and may be changed in order to maximize utility of evaluation findings.
186
186

DHCS anticipates contracting with an external evaluator prior to the start of HHP implementation to ensure the program is designed to allow for federal and state measurement and evaluation activities and inform the MCPs and health home providers of reporting requirements. Additional State standardized measures may be identified to track progress toward the Triple Aim goals.
5. Stakeholder Engagement Prior to SPA Submission DHCS initiated a stakeholder engagement process beginning in November 2014.
Time Period: April 2015 to August 2015 (Anticipated SPA submission)
Stakeholder engagement has been and will continue to be critical to the development of the HHP. DHCS will facilitate several engagement events between the April release of this second iteration of the DHCS Concept Paper and the anticipated August SPA submission to CMS. DHCS will convene a series of technical workgroup meetings (likely 2-4 meetings) with a small group of key stakeholders to gain advice on detailed aspects of policy development on the following topics:
• MCP and CB-CME qualifications, duties, and organizational structures; • Methods to promote program goals through program requirements for MCP HHP
network development, including: o Ensuring care management delivery and funding at the point of care in the
community; o HHP provider experience requirements for those experiencing homelessness; o Leveraging existing county and community provider care management
infrastructure and experience where appropriate. • Assessment, HAP, reporting requirements, metrics, referrals; • Eligibility Criteria, Tiers, Case Manager Ratios, and Cost and Savings Assumptions.
To facilitate the workgroup process, DHCS will develop policy proposals and/or questions and provide these to the group in advance with sufficient time for review. DHCS will convene the workgroup, either by telephone or in-person, to review comments on the agenda material. DHCS will also solicit written comments from the group within a reasonable period of time after the workgroup meeting.
DHCS will convene a separate technical workgroup for one meeting to gain advice on engaging and providing HHP services to those experiencing homelessness. DHCS will work with the sponsors of AB 361, Corporation for Supportive Housing, and the Western Center on Law and Poverty to design the membership and agenda for this workgroup. The format and process will be the same as the other technical workgroup meetings.
DHCS will release a DRAFT-FINAL concept paper for stakeholder review prior to the anticipated SPA submission to CMS in August 2015.
If you have comments or questions about this concept paper, or if you wish to be included in future notices of stakeholder engagement opportunities, please send your request to the DHCS health home mailbox: [email protected].
187
187

ATTACHMENT F.5/6
188
188

respect reliability resilience
November 11–13, 2015 Sheraton Grand Sacramento Hotel
and Sacramento Convention Center
2015 Hospital Quality Institute Conference California’s Preeminent Quality and Patient Safety Conference
189
189

respect reliability resilience
2015 Hospital Quality Institute Conference California’s Preeminent Quality and Patient Safety Conference
November 11–13, 2015
Sacramento Convention Center and the
Sheraton Grand Sacramento
Join us for the 2015 Hospital Quality Institute Conference to achieve
ever increasing levels of performance through a culture of respect and
professionalism. Learn strategies and take home tools for achieving
reliable care and delivering value to each patient, each time, and in
each community. The content, interactive learning and networking
opportunities are not to be missed.
Who should attend?
Everyone who cares about quality health care and who
is committed to the respect, dignity and experience of
patients and families that need and depend on us.
What will you gain by participating?
• Join the call to action to achieve reliability and make California the national quality leader.
• Leverage the experience of others to solve shared problems and create a culture of excellence.
• Engage in innovative thinking and actionable strategies while freed from the demands of your workday schedule.
• Hear from nationally recognized experts about best practices and meaningful solutions.
• Demonstrate your leadership to create a culture of respect, reliability and resilience.
• Become inspired and engaged by connecting and learning with like-minded colleagues.
190
190

Wednesday, November 11
1:00 – 4:30 p.m. Pre-Conference Workshops (choose one): Seating is limited
Creating the Culture of Safety: Respect, Reliability and Resilience
Michael Leonard, MD, Managing Partner (far left) and Allan Frankel, MD,
Chief Medical Officer (left), Safe and Reliable Healthcare, Paveljit Bindra, MD, Chief Medical Officer/Chief Information Officer, Citrus Valley Health Partners
Creating a safety culture will be explored in-depth by a team of experts. What is it, how do you seek it, how do you measure it and how do you improve it? This will be a highly interactive session with tools, methods and consultations tailored to the interests of the participants and their organizations.
Managing Behavior that Undermines a Safety Culture
William Cooper, MD, MPH, Professor of Pediatrics and Health Policy, Vanderbilt University School of Medicine
What does an organization do when individual or group behaviors undermine the best attempts to create a safe and reliable environment? This session will help you understand the relationship between behavior and outcomes, recognize behaviors that undermine a safety culture, identify organizational elements to address these behaviors, and pinpoint interventions to create change.
4:45 – 6:00 p.m. VIP Tour of the Capitol Join your colleagues for a private, behind-the-scenes tour of the State Capitol hosted by William J. Emmerson, DDS, former state senator and currently senior vice president, state relations and advocacy for the California Hospital Association.
Thursday, November 12
7:30 – 8:30 a.m. Sponsor Show, Best Practices Showcase and Continental Breakfast
8:30 – 9:00 a.m. Welcome, Overview and Remarks
Julie Morath, RN, MS, President/CEO, Hospital Quality Institute (left)
Joe Kiani, Founder, Patient Safety Movement Foundation
9:00 a.m. – 12:15 p.m. Opening Keynotes
The Changing Landscape of Patient Safety
Tejal Gandhi, MD, MPH, President and CEO, National Patient Safety Foundation and the Lucian Leape Institute
Dr. Gandhi describes trends and lessons learned to create safer care in hospitals, health care
systems and ambulatory care settings. Her insights will inspire you to commit to creating an engaged and harm free experience for patients and the health care workforce.
Reliability, Respect and Resilience — Building and Sustaining a Learning Organization
Gary Kaplan, MD, Chairman and CEO, Virginia Mason Health System
Hear about Virginia Mason’s journey to transform health care through the Virginia Mason Production System. Dr. Kaplan will highlight the foundational
elements of a safety culture and explain how to continuously improve care and eliminate defects through a commitment to respect for people and a fully engaged workforce.
Meet the Press Plenary Session
Tejal Gandhi, MD, MPH, President and CEO, National Patient Safety Foundation and the Lucian Leape Institute; Gary Kaplan, MD, Chairman and CEO, Virginia Mason Health System; Thornton Kirby, FACHE, President and CEO, South Carolina Hospital Association; C. Duane Dauner, President/CEO, California Hospital Association; Julie Morath, RN, MS, President/CEO, Hospital Quality Institute;
and Kevin Riggs, Senior Vice President, Randle Communications
Mr. Riggs, an Emmy award-winning reporter and broadcast news anchor, will conduct a hard hitting, “Meet-the-Press” style interview with health care
quality and safety leaders, 15 years post the IOM’s To Err is Human. Bring your questions and participate in this interactive session.
conference agenda
191
191

12:15 – 1:30 p.m. Hosted Luncheon
1:30 – 3:00 p.m. Concurrent Breakout Sessions (choose one):
Optimizing Sepsis Care: New Evidence and Measures
Sean Townsend, MD, Vice President of Quality and Safety, California Pacific Medical Center
Learn about the new evidence changing how we resuscitate patients. Get ahead of the curve and prepare for new CMS reporting requirements.
Improving Perinatal Care in California
Elliott Main, MD, Julie Vasher, DNP, RNC-OB, CNS-BC, C-EFM, and Valerie Cape, Leadership Team, California Maternal Quality Care Collaborative
California’s success in reducing morbidity and mortality is shaping the national dialogue. Hear about the lessons learned, challenges and solutions.
Data Sanity and the Business Case for Improvement
Helen Macfie, PharmD, Chief Transformation Officer, MemorialCare Health System and Gayle Sandhu, MS, FACHE, Corporate Senior Director, Quality Assurance, Scripps Health
Experts will explain how to navigate the health care landscape of increased transparency, proliferation of measures, revenues at risk, and demand for accountability for outcomes. This session will provide practical experience-based models for developing the business case for initiatives to receive the “green light” for implementation.
World Café: Advancing Patient and Family Engagement in California (Session continues into the next breakout period. Seating is limited.)
Facilitated by Jane Taylor, EdD, Improvement Advisor and Learning Designer, Institute for Healthcare Improvement and Boris Kalanj, MSW, Director of Cultural Care and Experience, Hospital Quality Institute
Participate in a facilitated, interactive session designed to tap the collective wisdom of the group through a series of conversations. World Café will offer you an open space to discuss the current state of patient and family engagement, and inspire commitment to transformative change.
3:30 – 5:00 p.m. Concurrent Breakout Sessions (choose one):
HAIs Have Met Their Match: Coordinated Prevention Strategies and Practices
Rekha Murthy, MD, FIDSA, FSHEA, Chair, HQI’s HAI Workgroup and Medical Director of Hospital Epidemiology, Cedars-Sinai Medical Center; Lynn Janssen, MS, CIC, CPHQ, Chief, HAI Program, California Department of Public Health; and Christine Martini-Bailey, RN, BSN, QI Project Lead, Health Services Advisory Group
Learn how you can engage with the improvement strategies and activities of leading organizations to prevent infections using the Centers for Disease Control’s Targeted Assessment for Prevention tool.
Simple Changes to Improve Event Response, Causal Analysis and Risk Mitigation
Rory Jaffe, MD, MBA, Executive Director, California Hospital Patient Safety Organization of HQI
Benefit from the findings of over 700,000 CHPSO safety reports to identify and mitigate risk in your organization. Learn how to identify important signals in high-volume low-severity events, avoid blaming individuals while maintaining accountability, and much more.
Creating Surgical Teams of High Reliability
Molly Clopp, RN, MS, MBATM, Strategic Leader; Claire Spanbock, RN, MBA, CNOR, Regional Director Perioperative Services; William Greif, MD, APIC for OR; and Paul Preston, MD, Anesthesiology; Kaiser Permanente Medical Group
Surgical safety champions will present the elements of their multi-year journey to assure that all surgeries are performed by highly reliable teams. Successful strategies and tools to continuously improve surgical team performance will be shared.
World Café: Advancing Patient and Family Engagement in California (continued)
5:00 – 6:00 p.m. Networking Reception
192
192

Friday, November 13
7:30 – 8:30 a.m. Sponsor Show, Best Practices Showcase and Continental Breakfast
8:30 – 8:45 a.m. Welcome and Overview
C. Duane Dauner President/CEO California Hospital Association
8:45 a.m. – 12:15 p.m. Closing Keynotes
Harnessing the Power of Zero
Thornton Kirby, FACHE, President and CEO, South Carolina Hospital Association
Become inspired by the journey of leaders who have discovered that the numerical expression of a highly reliable system is zero:
zero defects, zero harm, zero lapses in quality, zero health disparities. Mr. Kirby will challenge participants to harness the power of zero and strive for high reliability.
The Digital Doctor: Hope, Hype and Harm at the Dawn of Medicine’s Computer Age
Robert M. Wachter, MD, Professor and Associate Chairman of the Department of Medicine, University of California, San Francisco
Drawing from his new book, Dr. Wachter will reflect on this remarkable era in which health
care – driven by $30 billion in federal incentive payments – has finally become a digital industry. He explores the peril and promise of health IT and what it means to be a clinician and a patient in the modern era.
Upstream of Respect and Reliability in Care
Rishi Manchanda, MD, MPH, President and Founder, Health Begins
Physician, public health innovator and author of The Upstream Doctors will challenge us to reignite the Hippocratic Oath by addressing the
social and environmental conditions that often underlie sickness. Dr. Manchanda will offer practical examples of how health care can collaborate across boundaries to provide equitable and human-centered care.
respect reliability resilience
“This is one of the best programs
that I have ever attended — and
I have been in the hospital
performance improvement field
since 1978.”
“Exceptional content; amazing
line-up of top presenters; great
opportunities for attendee
participation; focus of meeting
was spot-on.”
“Absolutely inspiring. It was
great to see the successes from
various hospital members and
also be part of the discussion
about being the change agent.”
“Great statewide conference —
feels like a national conference.”
What attendees had to say about last year’s event:
193
193

1215 K Street, Suite 800, Sacramento, CA 95814 www.hqinstitute.org
Hospital Quality Institute is a collaboration of:
California Hospital Association Hospital Council of Northern and Central California Hospital Association of Southern California Hospital Association of San Diego and Imperial Counties
HQI thanks our current corporate sponsors for their support of the conference.
Diamond sponsors:
Sapphire sponsors:
Ruby sponsor: Topaz sponsors:
Continuing EducationFull attendance at each day’s educational sessions is a prerequisite for receiving continuing education (CE) credit. Attendees must sign in each day and include professional license number, if required.
CE applications have made for NHAP, NAHQ and ASHRM.
Health Care Executives — The Hospital Association of Southern California is authorized to award 3 pre-conference hours and 9 conference hours of ACHE Qualified Education credit (non-ACHE) for this program toward advancement or recertification in the American College of Healthcare Executives. Participants in this program wishing to have the continuing education hours applied toward ACHE Qualified Education credit should indicate their attendance when submitting an application to the American College of Healthcare Executives for advancement or recertification.
Nursing — Provider approved by the California Board of Registered Nursing, CEP #970 for 3.6 pre-conference contact hours and 10.8 conference contact hours. (Nursing CEs sponsored by Hospital Association of Southern California.)
TuitionRegister by September 30 and save
Full conference plus pre-conference workshop (Wednesday, Thursday AND Friday) $530
Full conference (Thursday AND Friday) $450
Pre-conference only (Wednesday) $125
Registrations received after September 30 add $100.
50% discount pricing for students, medical residents and patient family advisors. Limited number of discounts available. For application contact HQI at (916) 552-7600.
Cancellation Policy/Late PaymentA $75 non-refundable processing fee will be retained for each cancellation received in writing by October 9, 2015. No refunds will be made after this date. Substitutions are encouraged. Cancellation and substitution notification may be emailed to [email protected]. Payments not received by the conference date may be subject to a 10% late fee. In the unlikely event the program is cancelled, HQI will fully refund paid registrants within 30 days.
Americans with Disabilities ActIf you require special accommodations pursuant to the Americans with Disabilities Act, contact HQI at (916) 552-7600.
QuestionsGo to www.hqinstitute.org/hqi2015 or call (916) 552-7600.
Locations
Sacramento Convention Center 1400 J Street Sacramento, CA 95814
Sheraton Grand Sacramento Hotel 1230 J Street Sacramento, CA 95814
The Sacramento Convention Center is approximately 25 minutes from the Sacramento International Airport.
Accommodations Room reservation deadline is October 16
The Sheraton Grand Sacramento is the host hotel for the conference. Located in the heart of downtown Sacramento and across the street from the Sacramento Convention Center, the Sheraton is close to the State Capitol, numerous dining options, shopping and parks. Area attractions, such as Sutter’s Fort, Old Sacramento and the historic Railroad Museum, are close by.
Single and double rooms are available at a special, discounted rate of $169 per night. For reservations, call (800) 325-3535 and mention the “2015 Hospital Quality Institute Conference.” The discounted sleeping room deadline is October 16, but don’t delay — discounted rooms could sell out prior to the deadline.
194
194

SESSION 1 - From Peer, to Manager, to Leader- Leading People Differently
SESSION 2 - Leadership Communication Best Practices- Coaching Employees to Higher Performance
SESSION 3 - Leading Others Through Change- Managing Performance
SESSION 4 - Building and Leading Effective Teams- Planning and Running Effective Team Meetings
SESSION 5 - Resolving Interpersonal Conflict- Organizing your Time, Work and Priorities
SESSION 6 - Why and How of Organizational Policies- Business and Finance for Today’s Health Care Leader
LEADERSHIP • ENGAGEMENT • ACCOUNTABILITY • DEVELOPMENT
LEAD Academy Trains Managers To Be Successful Leaders
Do Your Mid-Level Managers Have The SkillsTo Be Successful Leaders?
LEAD Academy empowers recently hired, newly appointed or previously untrained health care managers to better understand and use their strengths to lead. LEAD Academy is built on the underlying principle that effective leadership requires productive relationships to support excellence in patient care and a sustainable workforce capable of managing change.
This is an excellent journey to rejuvenate and reinforce leadership skills. One must take advantage of this wonderful opportunity and the LEAD Academy is a must for any novice to intermediate level manager.
— Jonathan DavidPatient Care Manager
Stanford Healthcare
“
“
LEAD Academy is an education program provided by:
LEAD Academy sessions provide an engaging and safe environment to practice newly learned skills and align work goals and actions to support the broader vision of your organization.
LEAD Academy cohorts work together for six monthly meetings, a full day each month, focusing on:
• Self-development• Supporting the development of
others• Managing and developing a
successful organization
When your staff finishes their LEAD Academy cohort, they will:
1. Improve the performance of the people that report to them
2. Enhance their contribution to the achievement of your hospital’s strategic goals
3. Increase their own self-management skills during every day and stressful situations
LEAD Academy Curriculum
For more information contact Jenna Fischer, CPPS, Vice President of Education, Quality and Patient Safety925-746-5106, [email protected] , www.hospitalcouncil.net/lead-academy
Over 270 health care managers completed LEAD Academy
in 2015 representing 45 hospital and health system
members of theHospital Council of
Northern and Central California
195
195

ATTACHMENT G.2.A
196
196

1. Hospital Name:
2. Name of person completing this survey
Please estimate the total annual number of hires (headcount) you estimate will need to take place foreach year (2016-2020) based on expected vacancies, turnover, anticipated retirements, and otherfactors. You are welcome to add other key positions at the bottom of the survey.
Indicate the number of hires by calendar year:
NURSING
3. New Nursing Graduates - AA2016
2017
2018
2019
2020
4. New Nursing Graduates - BSN2016
2017
2018
2019
2020
5. Case Managers2016
2017
2018
2019
2020
197
197

6. Registered Nurses (2+ years of experience)2016
2017
2018
2019
2020
7. Critical Care Nurses (ED/ICU/OR/PACU)2016
2017
2018
2019
2020
8. Critical Care Nurses - Pedi2016
2017
2018
2019
2020
9. Specialty Nurses (OB/Wound/Diabetes/Other)2016
2017
2018
2019
2020
10. Home Health Nurses2016
2017
2018
2019
2020
198
198

11. Hospice Nurses2016
2017
2018
2019
2020
12. Nurse Leaders/Supervisors2016
2017
2018
2019
2020
13. Nurse Practitioners2016
2017
2018
2019
2020
14. Nurse Anesthetists2016
2017
2018
2019
2020
Please estimate the total annual number of hires (headcount) you estimate will need to take place foreach year (2016-2020) based on expected vacancies, turnover, anticipated retirements, and otherfactors. You are welcome to add other key positions at the bottom of the survey.
Indicate the number of hires by calendar year:
OTHER
199
199

15. Physician Assistants2016
2017
2018
2019
2020
16. Perfusionists2016
2017
2018
2019
2020
17. Surgical Techs2016
2017
2018
2019
2020
Please estimate the total annual number of hires (headcount) you estimate will need to take place foreach year (2016-2020) based on expected vacancies, turnover, anticipated retirements, and otherfactors. You are welcome to add other key positions at the bottom of the survey.
Indicate the number of hires by calendar year:
ALLIED HEALTH
18. Pharmacists2016
2017
2018
2019
2020
200
200

19. Pharmacy Techs2016
2017
2018
2019
2020
20. Clinical Laboratory Scientists2016
2017
2018
2019
2020
21. Occupational Therapists2016
2017
2018
2019
2020
22. Physical Therapists2016
2017
2018
2019
2020
23. Speech Therapists2016
2017
2018
2019
2020
201
201

24. Respiratory Therapists2016
2017
2018
2019
2020
25. Radiological Technologists2016
2017
2018
2019
2020
26. Sub-Modality Imaging (CT, PET, MRI, Sonography)2016
2017
2018
2019
2020
27. Medical Billing/Coding (certificate)2016
2017
2018
2019
2020
Please estimate the total annual number of hires (headcount) you estimate will need to take place foreach year (2016-2020) based on expected vacancies, turnover, anticipated retirements, and otherfactors. You are welcome to add other key positions at the bottom of the survey.
Indicate the number of hires by calendar year:
BEHAVIORAL HEALTH
202
202

28. Psychiatrists2016
2017
2018
2019
2020
29. Psychiatric Techs2016
2017
2018
2019
2020
30. Counselor/Therapist (LCSW, LMFT, Psychologist)2016
2017
2018
2019
2020
Please estimate the total annual number of hires (headcount) you estimate will need to take place foreach year (2016-2020) based on expected vacancies, turnover, anticipated retirements, and otherfactors. You are welcome to add other key positions at the bottom of the survey.
Indicate the number of hires by calendar year:
OTHER HOSPITAL-IDENTIFIED JOBS
31. Other hospital-identified jobs:
Hiring Priorities
32. Please indicate from the list below your top 3 hiring priorities in the next five years:
203
203

Not a Priority First Priority Second Priority Third Priority
New Nursing Graduates -AA
New Nursing Graduates -BSN
Case Managers
Registered Nurses (2+years of experience)
Critical Care Nurses(ED/ICU/OR/PACU)
Specialty Nurses(OB/Wound/Diabetes/Other)
Home Health Nurses
Hospice Nurses
Nurse Leaders/Supervisors
Nurse Practitioners
Nurse Anesthetists
Physician Assistants
Perfusionists
Surgical Techs
Pharmacists
Pharmacy Techs
Clinical LaboratoryScientists
Occupational Therapists
Physical Therapists
Speech Therapists
Respiratory Therapists
Radiological Technologists
Sub-Modality Imaging (CT,PET, MRI, Sonography)
Medical Billing/Coding(certificate)
Psychiatrists
Psychiatric Techs
204
204

Counselor/Therapist(LCSW, LMFT,Psychologist)
Not a Priority First Priority Second Priority Third Priority
For each of the following, please indicate how concerned you are regarding its impact on yourhospital's workforce adequacy. Indicate the impact for each position.
Workforce Adequacy Concerns
33. Impact Score
No Concern Some Concern Concerned Very ConcernedExtremelyConcerned
Aging healthcareworkforce within hospital
Population growth inregion
Cultural diversity
Linguistic capabilities
Impact of health reform
Impact of California statebudget cuts onhealthcare professionaleducation
Leaves of absence
Disabilityaccommodations and/orphysical limitations
205
205

ATTACHMENT H.1
206
206

Health Workforce Pilot Projects Program Application #173: Community Paramedicine
Updated November 17, 2014 APPLICANT/SPONSOR: PROJECT DIRECTOR: Emergency Medical Services Authority (EMSA) Howard Backer, MD, MPH, FACEP 10901 Gold Center Drive, Suite 400 EMSA Director Rancho Cordova, CA 95670 SPONSOR TYPE: Government agency engaged in health or education activities PURPOSE: Determine whether paramedics working in an expanded role in their community can help improve health system integration, efficiency, and/or fill identified health care needs. APPLICATION CHRONOLOGY: Application Submitted: December 28, 2013 Application Approved for Completeness: February 7, 2014 45-Day Public Review Process: February 14-March 30, 2014 Public Hearing: July 30, 2014 Staff Recommendation Released: October 13, 2014 Project Approved: November 14, 2014-November 13, 2015 ESTIMATED COST AND FUNDING SOURCES: Estimated Cost: $1,120,000 Funding Sources Committed: California Health Care Foundation Grant $750,000 Emergency Medical Services Authority $370,000 Total Committed $1,120,000 PROJECT DESCRIPTION: The applicant proposes to generate, collect and analyze data that will examine the practice of Community Paramedicine (CP) and serve as a basis to recommend changes to existing statutes and regulations in the following general project areas:
a) Transport patients with specified conditions to alternate locations that can be managed in health care settings other than an acute care emergency department, such as an urgent care or general medical clinic.
b) Address the needs of frequent 9-1-1 callers or frequent visitors to emergency departments by helping them access primary care and other social or psychological services.
c) Provide short-term home follow-up care for persons recently discharged from the hospital and at increased risk of a return visit to the emergency department or readmission to the hospital with referral from the hospital, clinic, or medical provider.
d) Provide short-term home support for persons with diabetes, asthma, congestive heart failure, or multiple chronic conditions with referral and under protocol from the medical home clinic or provider.
e) Partner with public health, community health workers and primary care providers in underserved areas to provide preventive care.
207
207

PROJECT OBJECTIVES: • Provide additional training to exiting EMT-Paramedics to prepare them to practice as
Community Paramedics under auspices of HWPP. • Demonstrate cost-effectiveness of care provided by Community Paramedics compared
to care as it is currently provided. • Demonstrate that Community Paramedics can safely and effectively provide care that
improves health care efficacy, patient-centered care, and integration of health system resources with reductions in both unnecessary ambulance transports to emergency departments and hospital readmissions.
Proposed Number of Trainees 100 Proposed Number of Supervisors 26 Proposed Number of Sites 13
BACKGROUND OF THE PROJECT: Selected passages have been taken from the HWPP #173 application.
“Community Paramedicine (CP) is a new and evolving model of community-based health care in which paramedics function outside of their customary emergency response and transport roles in ways that facilitate more appropriate use of emergency care resources and/or enhance access to primary care for medically underserved populations. CP programs typically are designed to address specific local problems and to take advantage of locally developed linkages and collaborations between and among emergency medical services and other health care and social service providers and, thus, are varied in nature. Interest in CP has substantially grown in recent years based on the belief that it may improve access to and quality of care while also reducing costs. In recent years, Community Paramedicine programs have been implemented in a number of states, including Colorado, Minnesota, Texas, Maine, Pennsylvania and Nevada, as well as other countries including Canada, England, New Zealand, and Australia. The implementation and operational costs of these programs in the U.S. and their outcomes are still being assessed. Few published reports of data are available at this time. There is a longer history and more literature on the outcomes of CP programs in other countries, but differences in methods of financing and delivering care in these countries makes it difficult to generalize the findings to the U.S. Interest in developing CP programs has been especially high in rural and other medically underserved areas.” The sponsor states that “this project will not displace other healthcare providers, but will fill unmet local needs utilizing paramedic skills and availability. Utilizing paramedics in expanded roles is attractive because they are already trained to perform patient assessments and recognize and manage life-threatening conditions in out-of-hospital settings. They are accustomed to providing care in home and community settings under relatively austere medical care conditions; are available 24 hours a day, seven days a week, 365 days a year; and are widely trusted and respected by the public. Further, paramedics are accustomed to collaborating with other health care providers in a variety of settings.” LAWS AND REGULATIONS PERTINENT TO THE PROPOSED PROJECT:
• California Code of Regulations, Title 22, Division 9, Chapter 4 • Health and Safety Code, Division 2.5, Chapter 2, 1797.52 • Health and Safety Code, Division 2.5, Chapter 4, 1797.218 • Health and Safety Code, Division 107, Part 3, Chapter 3, Article 1, commencing with
Section 128125, the Health Workforce Pilot Projects Program • California Code of Regulations: Title 22, Division 7, Chapter 6
208
208

ATTACHMENT H.2
209
209

Neal Cline, RN, JD, CRFN
Community Paramedicine Project Manager Butte County EMS
Community Paramedic Team
Program Description
Pilot concept: Post hospital discharge follow-up
Readmission reduction (post hospital or emergency department follow up, care for chronic conditions) -
Patients with a discharge diagnosis of Acute Myocardial Infarction (AMI) and Congestive Heart Failure
(CHF).
Patient follow up (post hospital or emergency department follow ups). Community paramedics will work
with the community's medical facilities and their Patient-Centered Medical Home (PCMH) initiatives to
provide follow-up monitoring for patients recently released from the hospital to reduce post-discharge
complications and costly readmissions.
Operating Areas
Butte County
Providers and Partners
Enloe Medical Center and Butte County EMS
Source: http://www.emsa.ca.gov/butte_county_CP
210
210

ATTACHMENT H.3
211
211

June 2015
Community Paramedicine Fact Sheet
What is Community Paramedicine? Community Paramedicine (CP) is a model of community-based health care in which paramedics function outside their customary emergency response and transport roles in ways that facilitate more appropriate use of emergency care resources and enhance access to primary care for medically underserved populations. CP programs typically are designed to address specific local problems. Interest in community paramedicine has substantially grown in recent years based on the belief that it may improve access to and quality of care while also reducing costs.
Community Paramedicine fills healthcare service gaps, without replacing healthcare workers. CP focuses on providing services, where access to care is limited, or a short term intervention is needed. By targeting locally identified health care needs, and offering a creative solution to fill local health care gaps, CP helps to increase access to care, and often reduces health care costs by providing the right level of care based on the individuals medical needs.
Community Paramedics are not independent practitioners; they work under clear medical control of a physician, receiving direction and supervision to ensure patient safety. The Community Paramedic training program builds upon the training and skill sets of experienced paramedics. Additional training in patient assessment, clinical skills and familiarity with the other healthcare providers and social services available in a local community will all be a part of the required training, and will lead to a more integrated approach to health care delivery.
Where are there Community Paramedic programs? North Carolina, Colorado, Minnesota, Maine, and Texas have implemented variations of community paramedicine. These programs have demonstrated that paramedics can be trained to safely and effectively perform an expanded role, with cost savings. An example of this is the CP program in Fort Worth, Texas, which is funded by healthcare systems and provider groups on either a fixed amount per visit or a percent of demonstrated cost savings from preventable emergency department visits or hospitalizations. In Colorado a single county program saved $1,250 per visit in health care costs for each of its 29 patients in the first year.
California CP Pilot Program: The California Emergency Medical Services Authority (EMSA) is working in partnership with the California HealthCare Foundation in implementing community paramedicine, utilizing the Health Workforce Pilot Program option through the Office of Statewide Health Planning and Development to test the concept in California. Visit OSHPD’s website to learn more about HWPP and to review an abstract of this
212
212

June 2015
project at: http://www.oshpd.ca.gov/hwdd/HWPP.html
Project # Pilot Test Concept
EMS Providers Pilot Project Manager
CP001 Alt Trans Destinations
Santa Monica, Glendale
Baxter Larmon, PhD, MICP UCLA Center for Prehospital Care David Geffen School of Medicine 10990 Wilshire Blvd., Suite 1450 Los Angeles, CA 90024 Office 310 903 0631 [email protected]
CP002 Post Discharge (CHF)
Glendale Fire Departments
Steven J. Rottman, MD Professor of Emergency Medicine David Geffen School of Medicine Medical Director, UCLA Center for Prehospital Care 10990 Wilshire Blvd., Suite 1450 Los Angeles, CA 90024 Tel: 310.794-0595 [email protected]
CP003 Alt Trans Destinations
Fountain Valley, Huntington Beach & Newport Beach Fire Departments
Vicki Sweet MSN, RN, CEN, FAEN County of Orange Health Care Agency 405 W. Fifth Street Suite 301A Santa Ana, CA 92701 714-834-5034 [email protected]
CP004 Post Discharge Follow Up
Butte County EMS
Neal Cline, RN, JD, CFRN Butte County EMS 5959 Pacific Street Rocklin, CA 95677 Office 530-332-7933 Cell 530-680-2428 [email protected]
CP005 Directly Observed TB Treatment
AMR Ventura Michael Taigman, General Manager American Medical Response Ventura 616 Fitch Avenue Moorpark, CA 93021 Office 510-593-5730 [email protected]
CP006 Hospice Support
AMR Ventura Michael Taigman, General Manager American Medical Response Ventura 616 Fitch Avenue Moorpark, CA 93021 Office 510-593-5730 [email protected]
CP007 Post Discharge Follow Up
Alameda City Fire Department
Elsie Kusel Alameda County EMS Agency
213
213

June 2015
Frequent 911 Callers
1000 San Leandro Blvd, Suite 200 San Leandro, CA 94557 Office 510-618-2003 [email protected]
CP008 Post Discharge Follow up
San Bernardino County Fire Department
Leslie Parham, San Bernardino County Fire Department 157 W. 5th Street, Second Floor San Bernardino, CA 92415-0451 [email protected]
CP009 Alt Destinations
Carlsbad Fire Department
Linda Allington, RN, MPH, MPA City of Carlsbad Fire Department 2560 Orion Way Carlsbad, CA 92010 Office:(760) 931-2175 [email protected]
CP010 Frequent 911 Callers
City of San Diego & Rural Metro Corp
Anne Marie Jenson, PM Rural/Metro Ambulance Company 1010 Second Avenue, Suite 300 San Diego, CA 92101 Office 619-533-4338 [email protected]
CP012 Alt Destinations (Mental Health)
AMR Stanislaus Linda Diaz, BSN, RN, PHN Mountain Valley - EMS 1101 Standiford Ave. Ste D-1 Modesto, Calif. 95350 209-566-7207 (direct line) 209-529-5085 (office) 209-769-2063 (cell) [email protected]
CP013 Post Discharge Follow Up
Medic Ambulance
James Pierson, Vice President Medic Ambulance Service 506 Couch Street Vallejo, CA 94590 Office 707-644-1761 [email protected]
214
214

June 2015
Visit OSHPD's website to learn more about HWPP and to review an Abstract of this project at: http://www.oshpd.ca.gov/hwdd/HWPP.html
California CP Pilot Timeline: Activity Time Frame
Emergency Medical Services Authority submits Community Paramedicine Pilot Project application to OSHPD.
December 20, 2013
Health Workforce Pilot Project HWPP #173 Community Paramedicine application deemed complete by OSHPD.
February 18, 2014
OSHPD Directors Approval of HWPP #173
November 14, 2014
Core Community Paramedicine Training provided by the UCLA Center for Prehospital Care, under the direction of Dr. Baxter Larmon, Director, UCLA Center for Prehospital Care & Professor at the David Geffen School of Medicine. 77 of the 79 enrolled Students graduated from this program.
January 7, 2015 thru February 19, 2015
Local Site Specific Training conducted within each Pilot Project Site
February 20, 2015 – June 1, 2015
Baseline Data Report submitted to OSHPD by UCSF’s Independent Evaluation Team in accordance with regulation.
May 29, 2015
OSHPD Approves CP 004 Butte, Post Discharge, CP 005 Ventura Directly Observed TB Medication, & CP 007 Alameda, Post Discharge for June 1, 2015 Implementation.
May 28, 2015
OSHPD Approves CP 006 Ventura Hospice, CP 007 Alameda Frequent 911 User & CP 008 San Bernardino Post Discharge for July 1, 2015 Implementation.
June 29, 2015
215
215

June 2015
How can I learn more about Community Paramedicine? Contact the Emergency Medical Services Authority (EMSA) for more information about California’s Community Paramedicine pilot project, the goals and benefits of integrating Paramedics into the health delivery system and the long term outcomes of exploring Community Paramedicine.
Lou Meyer Priscilla Rivera Project Manager Personnel Standards Manager Community Paramedicine Emergency Medical Services Authority Mobile: (209) 507-2386 (916) 431-3707 Office: (916) 431-3709 [email protected] [email protected]
216
216

ATTACHMENT J.1
217
217

Organization for Associate Degree Nursing and American Nurses Association Joint Position Statement on Academic Progression to Meet the
Needs of the Registered Nurse, the Health Care Consumer, and the U.S. Health Care System
Page 1
Organization for Associate Degree Nursing and American Nurses Association Joint Position Statement on Academic Progression to
Meet the Needs of the Registered Nurse, the Health Care Consumer, and the U.S. Health Care System
Position Statement All nurses must have access to seamless academic progression through high-quality, accredited nursing education programs that will meet the anticipated demand for qualified nurses over the next several decades. The Organization for Associate Degree Nursing (OADN) and American Nurses Association (ANA) commit to partnering with nursing and health care leaders, state legislature and regulatory agencies, universities, colleges, and other stakeholders in supporting and adopting innovative and emerging strategies to achieve that goal. Background This document identifies current evidence-based strategies that promote seamless academic progression with an emphasis on reaching the Institute of Medicine’s (IOM’s) Future of Nursing report-recommended goal that 80% of nurses be educated to the Bachelor of Science in Nursing (BSN) degree level by 2020. Community colleges, in collaboration with universities and practice partners, have developed several innovative academic models to achieve that goal, including (a) creating community college–university dual enrollment partnerships and (b) conferring of the baccalaureate degree by community colleges. In the early 1950s, Dr. Mildred Montag sought to alleviate a critical shortage of nurses by decreasing the length of time for entry into practice. She advocated reducing nursing education to 2 years by providing a strong educational base for nursing instruction and education in community and junior colleges. Dr. Montag proposed educating a technical nurse for 2 years to assist the professional nurse, whom she envisioned as having a baccalaureate degree. At the time, many practitioners wanted to continue the 3-year, hospital-based diploma programs that were already educating the vast majority of nurses in the United States. Others argued the BSN degree should be required for entering the nursing profession. A few were interested in having nursing education take place in an academic setting but did not think that 4 years of college were crucial for nurses to provide excellent patient care. As a result, an Associate degree (AD) in nursing education expanded quickly across the United States as a means to educate
218
218

Organization for Associate Degree Nursing and American Nurses Association Joint Position Statement on Academic Progression to Meet the
Needs of the Registered Nurse, the Health Care Consumer, and the U.S. Health Care System
Page 2
the nursing workforce. As the number of AD programs was increasing, diploma programs began closing for numerous reasons. (Appalachian State University, 2015). In 1964, the ANA House of Delegates adopted a motion that ANA “continue to work toward baccalaureate education as the educational foundation for professional nursing practice.” In 2000, the ANA Board of Directors reaffirmed that baccalaureate education should be the standard for entry into professional nursing practice (ANA, 2000). The Tri-Council for Nursing—whose members are the ANA, American Association of Colleges of Nursing (AACN), the American Organization of Nurse Executives (AONE), and the National League for Nursing (NLN)—issued a policy statement that supported a highly educated nursing workforce and that advocated educational advancement of registered nurses as a critical component of safe and effective patient care (Tri-Council of Nursing, 2010). The prestigious IOM issued The Future of Nursing: Leading Change, Advancing Health (2011), which is a blueprint for the future that offers a series of recommendations for how nurses’ roles, responsibilities, and education should change to respond to a complex, evolving health care system and to changing patient needs. Recommendations from the report focus on the intersection between health needs across the life span and the requisite skills and knowledge that nurses require to address those needs. One major recommendation identified that nurses should achieve higher levels of education and training through an education system that promotes seamless academic progression. Specifically, the report recommends increasing the percentage of registered nurses (RNs) with a BSN degree to 80% by the year 2020. Currently, 51% of nurses in the United States have a BSN degree, and 57% percent of nurses begin their nursing education at a community college, graduating with an associate degree (U.S. Department of Health and Human Services, 2013). In response to the IOM report, the leaders of the AACN, the American Association of Community Colleges (AACC), the Association of Community College Trustees (AACT), the NLN, and the National Organization for Associate Degree Nursing (N-OADN, but now OADN) endorsed a shared goal of academic progression for all nursing students and graduates (N-OADN, 2012). The American Nurses Association endorsed the statement in January 2013. In addition, the Robert Wood Johnson Foundation (RWJF) developed an initiative to advance Academic Progression in Nursing (APIN), thereby working with state-level Future of Nursing action coalitions to identify best practices for achieving seamless academic progression and to broadly disseminate those practices (RWJF, 2012). In 2013, RWJF convened a community college presidents’ meeting that included community college leaders from across the nation, Tri-Council for Nursing members, leaders from APIN, and other stakeholders to improve communication and collaboration about academic progression through discussion of possible options and next steps. All attendees affirmed the valuable contribution of community colleges in providing opportunities for entry into the nursing workforce by individuals with diverse racial and ethnic backgrounds and socioeconomic statuses. Participants also agreed that best
219
219

Organization for Associate Degree Nursing and American Nurses Association Joint Position Statement on Academic Progression to Meet the
Needs of the Registered Nurse, the Health Care Consumer, and the U.S. Health Care System
Page 3
practices must be in place to support and promote academic progression across all levels from associate to doctoral degree. John Lumpkin, MD, MPH, RWJF’s senior vice president, concurred: “Community colleges have a role to play in preserving nursing as a profession.… In partnership with community colleges, we can influence social change” (RWJF, 2014a). A potential complicating factor in meeting the IOM recommendation is the registered nurse workforce projections. The Bureau of Labor Statistics has projected that 555,100 RNs and advanced practice registered nurses (APRNs) will retire between 2012 and 2022, and the demand for nurses will create 574,400 additional jobs for RNs and APRNs. The combination of those two forces will generate 1.13 million vacancies for RNs and APRNs between 2012 and 2022 (ANA, 2014). The vacancies, in turn, will create the need for additional faculty and classroom space to meet the demand. Issues and Scope of the Problem Several major issues confront the nursing profession with respect to academic progression: � Between 2010 and 2014, the number of baccalaureate-prepared nurses has increased from 49% to 51%. An opportunity exists to reach the recommended IOM benchmark of 80% by 2020. (RWJF, 2014b) � Approximately 44% of hospitals and other health care settings are requiring new employees to have a bachelor’s degree in nursing—a 4.6% increase since 2012, while 78.6% of employers are expressing a strong preference for BSN-prepared nurses (AACN, 2013). � Magnet-designated hospitals and health care systems must demonstrate evidence of a plan to increase BSN-prepared nurses to 80% by 2020. All nurse managers must hold a BSN or higher nursing degree as of January 2013. (American Nurses Credentialing Center, 2013). � In 2012, 28% of qualified applicants were not accepted into nursing education programs (NLN, 2012) � Capacity issues are greatly affected by academic infrastructure issues, including shortages of qualified faculty, of classroom space, and of clinical practicum sites. In the absence of strong academic progression pathways, the faculty shortage cannot be resolved.
Recommended Strategies for Transforming U.S. Nursing Education Through APIN and the Center to Champion Nursing in America, RWJF has supported the development of innovative, sustainable models that provide seamless academic progression. Several promising models are in place, and each is based on strong partnerships and close collaboration between community colleges and universities. Brief
220
220

Organization for Associate Degree Nursing and American Nurses Association Joint Position Statement on Academic Progression to Meet the
Needs of the Registered Nurse, the Health Care Consumer, and the U.S. Health Care System
Page 4
descriptions of each of the models that facilitate seamless academic progression follow (RWJ, 2015). BSN Degree Awarded from a Community College Currently, the RN to BSN degree model offers nurses the opportunity for registered nurses to continue their postlicensure education in a community college setting and to receive a BSN degree. AD nurses with an RN license can advance directly to obtaining a BSN, and the community college awards the BSN degree. That model is especially beneficial for nurses who are place-bound with limited access to other options in their area, and it frequently is more affordable. The RN to BSN programs at community colleges are nationally accredited, transferable degrees that prepare the graduates to further their education. In a 2005 position statement, the AACN said it supports awarding BSN degrees at community colleges provided the Essentials of Baccalaureate Education for Professional Nursing Practice are used and the program is nationally accredited (AACN, 2005). Discussions are beginning regarding whether and how community colleges may confer 4-year BSN degrees. Dual Enrollment Community College–University Partnership Model The dual enrollment strategy builds on aspects of other models, including models for state or regional shared curricula, the competency- or outcome-based curriculum, and the RN to BSN degree program at community colleges. The student is enrolled at both the community college and the university. Prerequisites and nursing curricula are aligned between the community college and university partners. Students enter at the community college and may take university courses concurrently or interspersed with community college classes. At the conclusion of the 4 years, the student graduates with an AD conferred by the community college and a BSN conferred by the university, respectively, and then the graduate takes the National Council Licensure Examination for Registered Nurses (NCLEX-RN). RN to Master of Science in Nursing (MSN) Accelerated Option Model The RN to MSN model offers a shorter timeline for completion than traditional BSN or MSN programs, and it provides an additional pathway to streamlined educational progression. The RN to MSN popularity is driven by the fact that an increasing number of AD graduates, many whom already hold a bachelor’s degree in another field of study, are returning to school with the intention of obtaining an MSN. It is an accelerated model that values the practice experience of AD nurses and meets BSN criteria. The model is a seamless, university-based program and emphasizes practice components. State or Regionally Shared Competency-Based Curriculum Model The state or regionally shared competency-based models include partners that generally represent different educational approaches and backgrounds but that develop a shared understanding and a common goal and framework. The scope of the curriculum reaches beyond core competencies and across the entire profession as it focuses on knowledge, attitudes, and skills. The curriculum is not standardized, but successful models are based on strong partnerships between community colleges and
221
221

Organization for Associate Degree Nursing and American Nurses Association Joint Position Statement on Academic Progression to Meet the
Needs of the Registered Nurse, the Health Care Consumer, and the U.S. Health Care System
Page 5
4-year schools of nursing that are using agreed-upon outcomes or competencies to provide seamless, streamlined programs that culminate in conferral of a BSN degree. Statewide or Regional Curriculum Model The statewide or regional educational collaboratives between universities and community colleges enable students to transition automatically and seamlessly from an AD to a BSN degree program, with all schools sharing curriculum, simulation facilities, and faculty. The model requires a strong partnership between community colleges and universities with schools of nursing sharing as many components as possible, such as prerequisites, courses, enrollment, and admission standards. Implementation of the model requires (a) formal articulation agreements between community colleges and universities, (b) adjustment of prerequisite and nursing curricula, and (c) acceptance from regulatory bodies and institutions. Successful implementation of that model provides students with streamlined academic progression. Consistent with the IOM recommendations, transforming nursing education remains a priority to facilitate meeting the evolving and increasingly complex demands of the health care system in the United States. Community colleges are contributing to building the nursing workforce and must continue to play a role in preparing the nursing workforce. The strategies should include encouraging community college–university partnerships and granting community colleges the ability to offer the baccalaureate degree to meet the goal of having 80% of nurses educated to the BSN level by 2020. Definitions Academic Progression involves educational articulation models that promote lifelong learning through the attainment of academic credentials. Accreditation is the process of certification of competency, authority, or credibility. American Nurses Credentialing Programs Magnet Recognition Instituted in 1994, the American Nurses Credentialing Center Magnet Recognition Program recognizes hospitals and health care systems that meet criteria and standards for nursing excellence. Resource: http://www.nursecredentialing.org/magnet.aspx Pathway to Excellence ANCC’s Pathway to Excellence program recognizes health care and long-term care organizations that meet the criteria for a positive work environment and that foster and support excellent nursing practice. Resource: http://www.nursecredentialing.org/pathway Community College Baccalaureate is a bachelor’s degree conferred by a community college that is authorized to do so.
222
222

Organization for Associate Degree Nursing and American Nurses Association Joint Position Statement on Academic Progression to Meet the
Needs of the Registered Nurse, the Health Care Consumer, and the U.S. Health Care System
Page 6
Competency-Based Curriculum is defined by the Learning Collaborative on Advancing Education Transformation, which is part of the Center to Champion Nursing in America, as the process in which education partners, who generally represent different educational approaches and backgrounds, develop a shared understanding and a common goal and framework. The scope of the curriculum reaches beyond core competencies and focuses on knowledge, attitudes, and skills that encompass professional nursing practice. The curriculum is not standardized, but the model aims to reach standardized outcomes. Dual Enrollment is the concept of a student enrolling concurrently in two separate academic institutions at the same time, often studying in two related programs. Nursing Accreditation is a voluntary specialized peer-reviewed process that is based on identified standards and a system of assessment, evaluation, and continuous improvement. It serves as an assurance of quality educational standards and outcomes. Seamless Academic Progression encompasses the concept of advancement from one educational facility to another in an orderly and clearly charted plan so that one can acquire sequential degrees without the repetition of coursework or cumbersome prerequisite coursework. Statewide Curriculum Programs are educational collaboratives between universities and community colleges that enable students to transition automatically and seamlessly from an ADN to a BSN program, with all schools sharing curriculum, simulation facilities, and faculty. Faculty workload is reduced, and the schools make more efficient and greater use of resources. Implementation of such programs requires formal articulation agreements between community colleges and universities, adjustment of prerequisite and nursing curricula, and buy-in from legislative bodies and institutions. Approved by OADN: June 2, 2015
223
223

Organization for Associate Degree Nursing and American Nurses Association Joint Position Statement on Academic Progression to Meet the
Needs of the Registered Nurse, the Health Care Consumer, and the U.S. Health Care System
Page 7
References American Association of Colleges of Nursing. (2005). Baccalaureate nursing programs offered by community colleges. Retrieved from http://www.aacn.nche.edu/publications/position/ccbsn American Association of Colleges of Nursing. (2013). Employment of new nurse graduates and employer preferences for baccalaureate-prepared nurses. Retrieved from http://www.aacn.nche.edu/leading_initiatives_news/news/2013/employment13 American Nurses Association. (2000). ANA reaffirms commitment to BSN for entry into practice (2/25). [News release.] Retrieved from http://www.nursingworld.org/FunctionalMenuCategories/MediaResources/PressReleases/2000/CommitmenttoBSN.aspx American Nurses Association. (2014). Fast facts: The nursing workforce 2014. Retrieved from http://www.nursingworld.org/MainMenuCategories/ThePracticeofProfessionalNursing/workforce/Fast-Facts-2014-Nursing-Workforce.pdf American Nurses Credentialing Center. (2013). 2014 Magnet application manual. Silver Spring, MD: ANCC. Appalachian State University. (2014). The beginnings of associate degree nursing education in North Carolina. Retrieved from http://nursinghistory.appstate.edu/beginnings-associate-degree-nursing-education-nc Institute of Medicine. (2011). The future of nursing: Leading change, advancing health.
Retrieved from http://www.iom.edu/Reports/2010/The-Future-of-Nursing-Leading-
Change-Advancing-Health.aspx
National Organization for Associate Degree Nursing. (2012). Joint statement on
academic progression for nursing students and graduates. Retrieved from
http://www.oadn.org/files/resources-
initiatives/140212_joint_statement_academic_progression_ana_endorsed.pdf
National League for Nursing. (2012). Admissions to nursing programs: Disposition of applications to basic RN programs, fall 2012. Retrieved from http://www.nln.org/newsroom/nursing-education-statistics/admissions-to-nursing-programs Robert Wood Johnson Foundation. (2012). Future of nursing: Campaign for action academic progression in nursing. [Web page.] Retrieved from http://campaignforaction.org/apin
224
224

Organization for Associate Degree Nursing and American Nurses Association Joint Position Statement on Academic Progression to Meet the
Needs of the Registered Nurse, the Health Care Consumer, and the U.S. Health Care System
Page 8
Robert Wood Johnson Foundation. (2014a). Summary of the 2013 community presidents’ meeting and progress in the year since it was convened. Retrieved from http://campaignforaction.org/sites/default/files/Community%20Colleges%20Presidents%20Meeting%20Proceedings.pdf Robert Wood Johnson Foundation. (2014b). Future of nursing: Campaign for action dashboard indicators. [Web page.] Retrieved from http://campaignforaction.org/dashboard Robert Wood Johnson Foundation (2015). Future of nursing: Campaign for action:
Advancing nursing education/academic progression-promising education progression
models. [Web page.] Retrieved from http://campaignforaction.org/directory-of-
resources/advancing-nursing-education-academic-progression
Tri-Council of Nursing. (2010). Consensus policy statement on the educational
advancement of registered nurses. Retrieved from
http://tricouncilfornursing.org/documents/TricouncilEdStatement.pdf
U.S. Department of Health and Human Services. (2013). The U.S. nursing workforce: Trends in supply and education. Retrieved from http://bhpr.hrsa.gov/healthworkforce/supplydemand/nursing/nursingworkforce/nursingworkforcefullreport.pdf
225
225

ATTACHMENT J.2
226
226

See Where California's Heroin, Opioid Problems Are Worst
BY PHILLIP REESE - PREESE @SACBEE.COM
California hospitals treated more than 11,500 patients suffering an opioid or heroin overdose in 2013, new state figures show.
That's roughly one overdose every 45 minutes. It's also up more than 50 percent from 2006.
Charles Krupa Associated Press A tube of a drug known by its old brand name, Narcan, is displayed. It counteracts the effects of heroin and strong painkillers.
The trend explains a rise in the number of California infants born suffering withdrawal from heroin or painkillers.
Hospitals in rural superior California see the highest rate of opioid overdoses. Between 2006 and 2013, Shasta County hospitals saw more than 1,100 overdose, or eight overdoses per 10,000 residents, more than triple the statewide average.
To read the entire article and view interactive maps go to link below. Read more here: http://www.sacbee.com/site-services/databases/article31324532.html#storylink=cpy
227
227