Embed Size (px)
Citation preview

FAQ (FREQUENTLY ASKED QUESTIONS) ON MEDICAL INSURANCE SCHEME FOR RETIRED
EMPLOYEES OF PUNJAB & SIND BANK
1. What is the definition of family under the scheme?
The family of a retired employee includes Self + Dependent Spouse only
2. What is Sum Insured?
Hospitalisation Treatment Coverage
Officers: Rs.4.00 Lac
Award Staff (Clerks and Sub-Staff) : Rs.3.00 Lac
3. What is the date of joining the Scheme:
All Retired Employees to be covered from the date of their joining the scheme. Only one
time option is being given to Ex-employees / Retirees to join the scheme now. Those
who do not opt now, would not be allowed to join later. Once they have joined and
subsequently opted out, they cannot rejoin.
4. The Last Date for option letter to reach H.O. PF Department:
Although the date of inception of the scheme was 01.11.2015, but still, there is an open
window kept for accommodating Retirees to join up to three months from the inception of
policy i.e. 1st Nov 2015.
5. What is the Age limit for Joining this Scheme:
There is no upper age limit for joining the scheme. Retirees of any age may join the scheme.
6. Who is the insurance Company and TPA (Third party Administrator) in the policy:
Insurance Company: M/s United India Insurance Co. Ltd.
Name & Address of T.P.A MDIndia Healthcare Services (TPA) Pvt. Ltd.
18/13 WEA, Ground Floor, Ganga Plaza, Pusa Lane, Karol Bagh, Near Hanuman Murti, New Delhi-110005 Toll Free Customer Care No.: 1800 233 11 66 Toll Free Cashless No.: 1800 233 45 05
Contact Person: Abhinandan Dubey (Relationship Manager ): 08587856684

Retired Employees may contact Mr. Abhinandan Dubey of M/s MDIndia Healthcare Services
(TPA) Pvt. Ltd. for any of their query related to policy/cards.
7. Room Eligibility : Room Rent Including Room and boarding charges Rs.5000/- per day. ICU Charges Rs.7500/- per day
8. Pre- Post Hospitalization : Expense incurred during the Pre-hospitalization and Post-hospitalization period will be covered for 30 days prior to hospitalization and 90 days after discharge respectively. NOTE : The above information is indicative only and are subject to modification/amendments as per clarifications that may be received from IBA. *******

a) Name of TPA / Insurance Company: MDIndia Healthcare Services (TPA) Pvt Ltd
b) Toll free phone number: 18002334505
c) Toll free Fax: 18602334447 & 18602334449
f) Contact number of attending relative
g) Insured card ID number:
h) Policy number / Name of corporate:
Yes No
Yes No
f) Provisional diagnosis:
Yes No Yes No
Yes No Yes No
G P L A
:
`
`
`
`
`
`
`
`
We confirm having read, understood and agreed to the Declaration on the reverse of this form
(PLEASE READ VERY CAREFULLY)
DECLARATION
a) Name of the treating doctor:
b) Qualification: c) Registration No. with state code:
l) All inclusive package charges, if any applicable:
k) Medicines + Consumables + Cost of implants (if applicable, please
Any other Ailment, give details:
specify), other hospital expenses, if any:
g) Expected cost of investigation + diagnostics:
h) ICU Charges:
i) OT Charges:
m) Sum Total, expected cost of hospitalization:
Details of the patient admitted Mandatory : Past history of any chronic illness If Yes, since (month / year)
a) Date of admission: b) Time:
c) Is this an emergency / a planned hospitalization event? Planned
j) Professional fees Surgeon + Anesthetist Fees + consultation charges:
details
l) In case of accident: i. Is it RTA? ii. Date of injury: iii. Reported to Police: iv. FIR No.:
i. Route of drug administration:
k) How did the injury occur?
m) Contact number, if any: (PLEASE COMPLETE DECLARATION ON THE REVERSE SIDE OF THIS FORM)
TO BE FILLED BY THE TREATING DOCTOR / HOSPITAL
i. ICD 10 Code
Medical Management Surgical Management Intensive Care Investigation Non allopathis Treatment
i) Employee ID:
j) Currently do you have any other Mediclaim / Helath Insurance: Company Name:
Give details:
k) Do you have a family physician? l) Name of the family physician:
b) Gender :
e) Contact number:
TO BE FILLED BY THE INSURED / PATIENT
months d) Date of Birth: Male Female
(If yes attach reports)
m) In case of maternity: Date of Delivery:
a) Name of the treating doctor:
PLEASE FAX / SCAN PAGE 1 ONLY
REQUEST FOR CASHLESS HOSPITALISATION FOR MEDICLAIM INSURANCE POLICY
(To be filled in block letters)
DETAILS OF THE THIRD PARTY ADMINISTRATOR
c) Age: years
a) Name of the patient:
Emergency
d) Expected no. of days in hospital: Days e) Room Type:
b) Contact number:
c) Nature of illness/ disease d) Relevant clinical findins:
with presenting complaints
if any
f) Per Day Room Rent + Nursing & Service Charges + Patient's Diet:
present ailment,
ii. Past history of
g) Proposed line of treatment:
e) Duration of the present ailment: Days i. Date of first consultation:
v. Injury / Disease caused due to substance abuse / alcohol consumption: vi. Test conducted to extablish this?
h) If investigation & / or Medical
j) If other treatments, provide
Any HIV or STD / Related ailments
Diabetes
Heart Disease
Hypertension
Hyperlipidemia
Osteoarthritis
Asthma / COPD / Bronchitis
Cancer
Alcohol or drug abuse
Management, provide details
i) If Surgical, name of surgery: i. ICD 10 PCS Code
(IMPORTANT: PLEASE TURN OVER)
Hospital Seal (must contain hospital ID) Patient / Insured Name & Signature

DOCUMENTS TO BE PROVIDED BY THE HOSPITAL IN SUPPORT OF THE CLAIM
1. Detailed Discharge Summary and all Bills from the hospital
2. Cash Memos from the Hospitals / Chemists supported by proper prescription.
b) Contact number: d) Patient’s / Insured’s Signature:
HOSPITAL DECLARATION
1. We have no objection to any authorized TPA / Insurance Company official verifying documents pertaining to hospitalization.
2. All valid original documents duly countersigned by the insured / patient as per the checklist below will be sent to TPA / Insurance Company within 7 days of the patient's discharge.
5. Certificates from attending Medical Practitioner / Surgeon that the patient is fully cured.
6. We agree to provide clarifications for the queries raised regarding this hospitalization and we take the sole responsibility for any delay in offering clarifications.
7. We will abide by the terms and conditions agreed in the MOU.
Hospital Seal
4. Surgeon's Certificate stating nature of operation performed and Surgeon's Bill and Receipt.
PAGE 2: NOT TO BE FAXED/SCANNED
DECLARATION BY THE PATIENT / REPRESENTATIVE
1. I agree to allow the hospital to submit all original documents pertaining to hospitalization to the Insurer/T.P.A after the discharge. I agree to sign on the Final Bill & the Discharge Summary, before my discharge.
2. Payment to hospital is governed by the terms and conditions of the policy. In case the Insurer / TPA is not liable to settle the hospital bill, I undertake to settle the bill as per the terms and conditions of the policy.
3. All non-medical expenses and expenses not relevant to current hospitalization and the amounts over & above the limit authorized by the Insurer/T.P.A not governed by the terms and conditions of
the policy will be paid by me. In case any clarification is needed on admissibility of a particular item I shall contact T.P.A at the Toll Free Number on the reverse of this form.
4. I hereby declare to abide by the terms and conditions of the policy and if at any time the facts disclosed by me are found to be false or incorrect I forfeit my claim and agree to indemnify the Insurer / T.P.A
3. All non medical expenses , OR expenses not relevant to hospitalization or illness, OR expenses disallowed in the Authorization Letter of the TPA / Insurance Co, OR arising out of incorrect
information in the pre-authorisation form will be collected from the patient.
4. WE AGREE THAT TPA / INSURANCE COMPANY WILL NOT BE LIABLE TO MAKE THE PAYMENT IN THE EVENT OF ANY DISCREPANCY BETWEEN THE FACTS IN THIS FORM AND
DISCHARGE SUMMARY or other documents.
5. The patient declaration has been signed by the patient or by his representative in our presence.
3. Receipts and Pathological Test Reports from Pathologists, supported by note from the attending Medical Practitioner / Surgeon recommending such pathological Tests.
5. I agree and understand that T.P.A is in no way warranting the service of the hospital & that the Insurer / TPA is in no way guaranteeing that the services provided by the hospital will be of a particular quality or standard.
6. I hereby warrant the truth of the forgoing particulars in every respect and I agree that if I have made or shall make any false or untrue statement, suppression or concealment, my right to claim
7. I agree to indemnify the hospital against all expenses incurred on my behalf, which are not reimbursed by the Insurer / TPA.
a) Patient’s / Insured’s Name:
Doctor's Signature

b) BOM Employee ID No
SECTION A
City:
Yes No
Yes No
Diagnosis: e) Previously covered by any other Mediclaim/ Health Insurance : Yes No
f) If yes, Company Name :
City:
: :
Yes No
Yes No Yes No
Claim Documents Submitted- Check List:
` `
` `
` `
` Implants - Invoices / BarCode Stickers
Yes No
` `
` `
` `
`
SECTION A
SECTION B
SECTION C
Pharmacy Bills:
SECTION D
SECTION E
SECTION F
SECTION H
Others: MLC/FIR:
9
10
7
8
Total
Date: Place: Signature of the insured:
DECLARATION BY THE INSURED
I hereby declare that the information furnished in this claim form is true & correct to the best of my knowledge and belief. If I have made any false or untrue statement, suppression or concealment of any material fact with respect to questions asked in relation to this
claim, my right to claim reimbursement shall be forfeited. I also consent & authorize TPA / insurance company, to seek necessary medical information / documents from any hospital / Medical Practitioner who has attended on the person against whom this claim is
made. I hereby declare that I have included all the bills / receipts for the purpose of this claim & that I will not be making any supplementary claim except the pre/post-hospitalization claim, if any.
Amount (`)Issued By Towards
1
2
v. Pre/Post hosp. Lump sum benefit: vi. Others: Investigation Reports (including CT /
DETAILS OF BILLS ENCLOSED
Sl. No. Bill No. Date
MRI / Report CD's / HPE)
CLAIM FORM - PART A
TO BE FILLED IN BY THE INSURED
The issue of theis form is not to be taken as admission of liability
(To be filled in block letters)
a) Currently covered by any other Mediclaim/ Health Insurance:
Sum Insured (`):
DETAILS OF PRIMARY INSURED : PUNJAB AND SIND ZONAL OFFICE / REGIONAL OFFICE:
f) BOM Emp Branch Location
d) Have you been hospitalized in the last four years since inception of the contract?
Pin Code:
3
4
5
6
Hospital Main Bill
Pre hospitalisation Bills: ___ Nos
Post hospitalisation Bills: ___ Nos
iv. Convalescence: Doctor's request for investigation
(if yes, provide details in annexure) Pharmacy Bill & Cash Memo
c) Details of Lump sum / cash benefit claimed:
b) Claim for Domiciliary Hospitalization:
Operation Theatre Notes
Hospital Break-up bill
i. Pre Hospitalization Expenses
iii. Post Hospitalization Expenses
v. Ambulance Charges vi. Others (code):
Doctor's Prescription of Medicines
i. Hospital Daily Cash: ii. Surgical Cash: ECG, USG, X Ray Etc
iii. Critical Illness Benefit:
Hospital Discharge Summarydaysvi. Pre hospitalization period: vii. Pre hospitalization period: days
ii. Hospitalization Expenses
iv. Health Check up Cost
Total
Claim FormDuly signed
Hospital Orginal Bill & Paid Receipts
DETAILS OF CLAIM
a) Details of treatment expenses claimed
h) Time:
i) If injury, give cause: Self inflicted Road Traffic Accident Substance abuse / Alcohol Consumption i. If Medico Legal:
f) Time: g) Date of Discharge:
3 or more beds per room
ii. Reported to police: iii. MLC Report & Police FIR attached: j) System of medicine:
c) Hospitalization due to: Illness Maternity d) Date of injury/ Date Disease first detected/ Date of Delivery:
e) Date of Admission:
Father Mother
Injury
b) Room category occupied: Day Care Single occupancy Twin sharing
(Please specify)
Service f) Occupation: Self Employed Homemaker
e) Relatuionship to Primary Insured: Self Spouse Child
d) Date of Birth:
(Please specify)
Other
DETAILS OF HOSPITALIZATION
a) Name of Hospital where Admitted:
State:
Pin Code: Phone No: Email ID:
g) Address (if different from above):
Student Retired Other
a) Name :
b) Gender : Male Female c) Age: years months
DETAILS OF INSURED PERSON HOSPITALIZED
a) Policy no:
c) MDIndia ID No:
Emp Name:
e) Address:
State:
b) Date of commencement of first insurance without break:
Phone No: Email ID:
DETAILS OF INSURANCE HISTORY
Date:
c) If yes, company name: Policy No:

d) Name of the treating doctor:
e) Qualification:
e) Date of Birth:
: :
a) b)
Yes No
Yes No
Yes No Yes No Yes No
Hospital Registration No:
Yes No Yes No
g) Yes No
DETAILS IN CASE OF NON NETWORK HOSPITAL (ONLY FILL IN CASE OF NON NETWORK HOSPITAL)
a) Address of the hospital:
Phone No:
Place:
SECTION A
SECTION B
SECTION C
SECTION D
SECTION E
Facilities available in the hospitai
Does Hospital Maintains Daily Records of Patients & Makes them Accesible to Insurance Company's Authorized Personanel
DECLARATION BY THE HOSPITAL
State:City:
Reg Authority:
Local or State Government Licensed Pin Code:
i. If yes, give cause Self inflicted Road Traffic Accident Substance abuse / alcohol consumption
ii. If injurydue to Substance abuse / alcohol consumption, Test Conducted to establish this: iv. Reported to Police: iii. If Medico Legal: (if yes, attach reports)
v. FIR No. vi. If not reported to police, give reason:
ii. Additional Diagnosis :
f) Hospitalization due to injury:
e) If authorization by network hospital not obtained, give reason:
i. Procedure 1 :
ii. Procedure 2 :
iii. Procedure 3 :
iv. Details of Procedure :
iii. Co-morbidities :
c) Pre authorization obtained: d) Pre-authorization number:
ICD 10 PCS Description
iv. Co-morbidities :
ii. Gravida Status:
l) Status at time of discharge: Discharged to home Discharged to another hospital Deceased m) Total claimed amount
j) Type of Admission: Emergency Planned Day Care Maternity
DETAILS OF AILMENT DIAGNOSED (PRIMARY)
i. Primary Diagnosis :
ICD 10 Codes Description
i) Time:
DETAILS OF PATIENT ADMITTED
a) Name of Patient:
b) IP Registration No.: c) Gender : Female months Male
c) Hospital ID:
d) Age: years
f) Date of Admission: g) Time: h) Date of Discharge:
Non Network
Date:
We hereby declare that the information furnished in this Claim Form is true & correct to the best of our knowledge and belief. If we have made any false or untrue statement, suppress or concealment of anu material fact, our right to claim under this claim shall be
forfeited.
d) Hospital PAN e) Number of inpatient beds ii. ICU:
Seal & Signature of the Hospital Authority Name & Signature of the Insured
(Please read very carefully)
i. OT:
a) Name of the Hospital:
Network c) Type of Hospital: (if non network, fill Section E)
k) If Maternity: i. Date of Delivery:
g) Phone No. f) Registration No. with state code:
CLAIM FORM - PART B
TO BE FILLED IN BY THE HOSPITAL
The issue of theis form is not to be taken as admission of liability
(To be filled in block letters)
DETAILS OF HOSPITAL
Please include the original preauthorization request form in lieu of PART A

b) BOM Employee ID No
City:
(DD/MM/YYYY) (DD/MM/YYYY)
Total Number of Claim Documents Submitted:
Select the Number as below in lieu of the documents submitted
Illness Certificate by Treating Doctor with Duration
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30+
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30+
Investigation Prescriptions by Treating Doctor 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30+
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30+
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30+
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30+
DOMICILIARY TREATMENT - CLAIM FORM TO BE FILLED IN BY THE INSURED (The issue of this form is not to be taken as admission of liability)
(To be filled in block letters)
DETAILS OF PRIMARY INSURED : PUNJAB & SIND BANK ZONAL OFFICE / REGIONAL OFFICE:
a) Policy no:
In case more than 10 Bills are to be submitted then attach separate annexure using the same above format:
Pin Code: Phone No: Email ID:
c) MDIndia ID No: f) BOM Emp Branch Location
Emp Name:
e) Address:
State:
DETAILS OF INSURED PERSON HOSPITALIZED
a) Name :
b) Gender : Male Female c) Age: years months d) Date of Birth:
e) Relatuionship to Primary Insured: Self Spouse Child Father Mother
f) Occupation: Service Self Employed Homemaker Student Retired Other (Please specify)
Other (Please specify)
Claim FormDuly signed
DETAILS OF CLAIMS
a) Name of Treating Doctor:
b) Commencement of Treatment: Date
c) Domiciliary Treatment For:
c) Treatment End Date:
Claim Documents Submitted- Check List:
DETAILS OF BILLS ENCLOSED:
Investigation Bills Cash Memo
Investigation Reports
Pharmacy Prescriptions by Treating Doctor
Pharmacy Bills Cash Memo
Treating Doctor Consultancy Charges Cash Receipts
Sl. No. Bill No. Date Issued By Towards - Pharmacy, Investigations or Consultancy Charges Amount (̀ )
1
2
3
4
5
6
7
8
DECLARATION BY THE INSURED
I hereby declare that the information furnished in this claim form is true & correct to the best of my knowledge and belief. If I have made any false or untrue statement, suppression or concealment of any material fact with respect to questions asked in relation to
this claim, my right to claim reimbursement shall be forfeited. I also consent & authorize TPA / insurance company, to seek necessary medical information / documents from any hospital / Medical Practitioner who has attended on the person against whom this
claim is made. I hereby declare that I have included all the bills / receipts for the purpose of this claim & that I will not be making any supplementary claim except the pre/post-hospitalization claim, if any.
Date: Place: Signature of the insured:
9
10
Members are requested to submit the Illness Certificate by Treating Doctor with detailed duration of the illness for which the treatment would be done.
Sheet1
Page 1
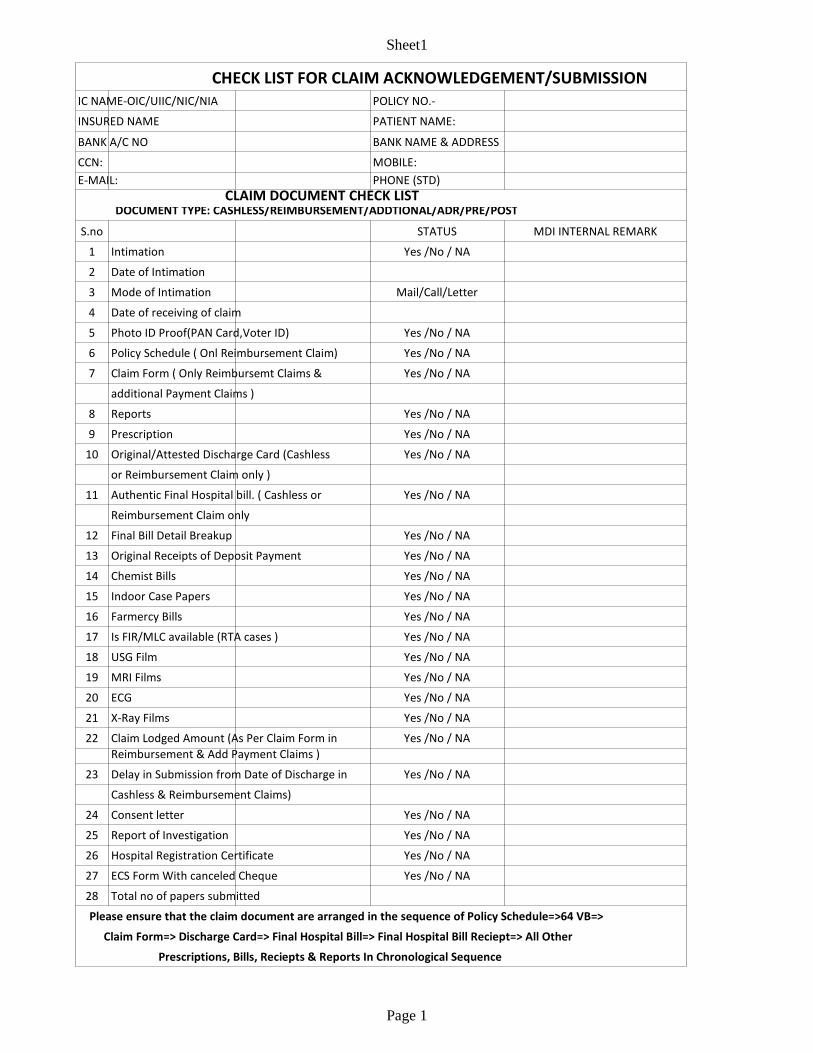
IC NAME-OIC/UIIC/NIC/NIA POLICY NO.-
INSURED NAME PATIENT NAME:
BANK A/C NO BANK NAME & ADDRESS
CCN: MOBILE:
E-MAIL: PHONE (STD)
STATUS MDI INTERNAL REMARK
1 Intimation Yes /No / NA
2 Date of Intimation
3 Mode of Intimation Mail/Call/Letter
4 Date of receiving of claim
5 Photo ID Proof(PAN Card,Voter ID) Yes /No / NA
6 Yes /No / NA
7 Yes /No / NA
additional Payment Claims )
8 Reports Yes /No / NA
9 Prescription Yes /No / NA
10 Original/Attested Discharge Card (Cashless Yes /No / NA
or Reimbursement Claim only )
11 Authentic Final Hospital bill. ( Cashless or Yes /No / NA
Reimbursement Claim only
12 Final Bill Detail Breakup Yes /No / NA
13 Original Receipts of Deposit Payment Yes /No / NA
14 Chemist Bills Yes /No / NA
15 Indoor Case Papers Yes /No / NA
16 Yes /No / NA
17 Is FIR/MLC available (RTA cases ) Yes /No / NA
18 USG Film Yes /No / NA
19 MRI Films Yes /No / NA
20 ECG Yes /No / NA
21 X-Ray Films Yes /No / NA
22 Claim Lodged Amount (As Per Claim Form in Yes /No / NA
Reimbursement & Add Payment Claims )
23 Delay in Submission from Date of Discharge in Yes /No / NA
Cashless & Reimbursement Claims)
24 Consent letter Yes /No / NA
25 Report of Investigation Yes /No / NA
26 Hospital Registration Certificate Yes /No / NA
27 Yes /No / NA
28 Total no of papers submitted
CHECK LIST FOR CLAIM ACKNOWLEDGEMENT/SUBMISSION
CLAIM DOCUMENT CHECK LIST DOCUMENT TYPE: CASHLESS/REIMBURSEMENT/ADDTIONAL/ADR/PRE/POST
S.no
Policy Schedule ( Onl Reimbursement Claim)
Claim Form ( Only Reimbursemt Claims &
Farmercy Bills
ECS Form With canceled Cheque
Please ensure that the claim document are arranged in the sequence of Policy Schedule=>64 VB=>
Claim Form=> Discharge Card=> Final Hospital Bill=> Final Hospital Bill Reciept=> All Other
Prescriptions, Bills, Reciepts & Reports In Chronological Sequence

������������� �������������������������
�
�������������
������� ���������
����������������������������������
�
�����������������
�
��������������� ���������
������� �����������
�������!��"�
!����������
!����� ������
�
�
������� �����#�
�
������������ � � � � � � � � ��������������$����������%���������
�
���&����� ����������
�
�
�������������
'( �������������������������������������������������� �������������)����������������������"�*���+��)�������(��������,��
�������������������������������-�����������������������������������������-�����+��������������������������������
�������(�
.( ���+������������������������� ��������������������������������������/��������������������������������*�����,��
������������������������������������������������� ���������������,�(�
0( ����������,�����&!��+���������-�������������$�����������,����/�������������������������(�
����#�
�����#� ��+�����������������������
�
////////////////////////////////////////////////////////////////� ��1 ��� 23 ��4&� ��///////////////////////////////////////////////////////////////�
�
���#��������������������������������������������������������������������$�����������������������������������
���$�����������"���������������5�������"��������������������������� ���&�6����������(�
�
�

HOW TO DOWNLOAD SOFT COPY OF HEALTH CARDS
Login to our website www.mdindiaonline.com
Click on My Account
Click on IBA login

HOW TO DOWNLOAD SOFT COPY OF HEALTH CARDS
Select your Bank from the dropdown menu and enter your PF No. in User ID as well as Password:
You may change your password and proceed for E Card.





























