Embed Size (px)
Citation preview

Fanconi AnemiaFanconi Anemia
Priya GopalanPriya Gopalan
April 7, 2006April 7, 2006

CaseCase Clinical FeaturesClinical Features DiagnosisDiagnosis FA pathwayFA pathway ManagementManagement ConclusionsConclusions

CaseCase
A 21 year old Mexican woman with a A 21 year old Mexican woman with a history of anemia, presented to a local history of anemia, presented to a local clinic with a positive home pregnancy test. clinic with a positive home pregnancy test. After confirming her pregnancy (she was After confirming her pregnancy (she was approximately 13 weeks pregnant), she approximately 13 weeks pregnant), she had several labs drawn, including a CBC. had several labs drawn, including a CBC. She was found to be pancytopenic, and She was found to be pancytopenic, and was told to come to BJC for admission.was told to come to BJC for admission.

CaseCase
She complained of fatigue and easy She complained of fatigue and easy bruising for many months, but no bruising for many months, but no epistaxis, hematochezia, melena or epistaxis, hematochezia, melena or hematuria. Furthermore, her menstrual hematuria. Furthermore, her menstrual cycles had been regular and moderate cycles had been regular and moderate until 3 months ago.until 3 months ago.

CaseCase
Past Medical History: She was first told that she Past Medical History: She was first told that she was anemic 5 years ago, in Mexico. At that was anemic 5 years ago, in Mexico. At that time, she had a bone marrow biopsy performed. time, she had a bone marrow biopsy performed. She is not sure what it showed, but she was told She is not sure what it showed, but she was told to take Proverone (medroxyprogesterone) once to take Proverone (medroxyprogesterone) once a day, which she was unable to afford.a day, which she was unable to afford.
Medications: NoneMedications: None
Allergies: NoneAllergies: None

CaseCase
Social History: She moved to the U.S. 2 Social History: She moved to the U.S. 2 years ago, from Mexico. She is single and years ago, from Mexico. She is single and works as a housekeeper. She denies any works as a housekeeper. She denies any tobacco, alcohol or drug use.tobacco, alcohol or drug use.

CaseCase
Family History:Family History: She has 3 siblings in the U.S., and 10 siblings She has 3 siblings in the U.S., and 10 siblings
in Mexico. One sister in Mexico, who is now in Mexico. One sister in Mexico, who is now 15 years old, was just diagnosed with anemia, 15 years old, was just diagnosed with anemia, and had a bone marrow biopsy. She is not and had a bone marrow biopsy. She is not sure what it showed.sure what it showed.
No family history of hematological disorders, No family history of hematological disorders, cancers or early deaths. Her grandparents cancers or early deaths. Her grandparents and parents are alive and healthy.and parents are alive and healthy.

CaseCase
Physical examination:Physical examination: Height: 5’0”Height: 5’0” Significant only for bilaterally short thumbsSignificant only for bilaterally short thumbs No dermatologic abnormalitiesNo dermatologic abnormalities
Labs:Labs: WBC: 2.1 (41%N, 53%L; ANC 900)WBC: 2.1 (41%N, 53%L; ANC 900) Hemoglobin / Hematocrit: 4.9/14.2 (MCV 111)Hemoglobin / Hematocrit: 4.9/14.2 (MCV 111) Platelets: 17,000Platelets: 17,000

CaseCase
Other labs:Other labs: CMP WNL (Cr 0.4)CMP WNL (Cr 0.4) Vitamin B12 and folic acid WNLVitamin B12 and folic acid WNL Reticulocyte 2.4%Reticulocyte 2.4% Hepatitis panel/HIV negative, ANA negativeHepatitis panel/HIV negative, ANA negative Peripheral smear: normal-appearing WBC, Peripheral smear: normal-appearing WBC,
RBC and platelets, but greatly reduced in RBC and platelets, but greatly reduced in numbernumber

CaseCase
Bone Marrow Biopsy:Bone Marrow Biopsy: Markedly hypocellular marrow, with markedly Markedly hypocellular marrow, with markedly
decreased trilineage hematopoiesis, decreased trilineage hematopoiesis, consistent with aplastic anemia (cellularity consistent with aplastic anemia (cellularity <5%)<5%)
No overt dysplastic featuresNo overt dysplastic features Cytogenetics were pendingCytogenetics were pending

CaseCase
A diagnosis of Fanconi Anemia was A diagnosis of Fanconi Anemia was suspected based on:suspected based on: History of “anemia” at age 16History of “anemia” at age 16 History of “anemia” in a sister, at age 15History of “anemia” in a sister, at age 15 Short statureShort stature Shortened thumbs bilaterallyShortened thumbs bilaterally PancytopeniaPancytopenia Bone marrow hypocellularityBone marrow hypocellularity

Fanconi AnemiaFanconi Anemia
Inherited recessive diseaseInherited recessive disease Usually autosomal recessiveUsually autosomal recessive Recently, an X-linked form has been Recently, an X-linked form has been
described (Meetei et al 2004)described (Meetei et al 2004) 12 different complementation groups12 different complementation groups
Determined by somatic cell hybridization Determined by somatic cell hybridization analysisanalysis
11 genes cloned11 genes cloned

FA complementation groups and FA genesFA complementation groups and FA genesFA FA
complementation complementation groupgroup
FA geneFA gene Approx. frequency Approx. frequency in FA patients (%)in FA patients (%)
Chromosomal Chromosomal LocationLocation
AA FANCAFANCA 6060 16q24.316q24.3
BB FANCBFANCB RareRare Xp22.31Xp22.31
CC FANCCFANCC 1515 9q22.39q22.3
D1D1 BRCA2BRCA2 55 13q12.313q12.3
D2D2 FANCD2FANCD2 55 3p25.33p25.3
EE FANCEFANCE RareRare 6p21.36p21.3
FF FANCFFANCF RareRare 11p1511p15
GG FANCGFANCG 1010 9p139p13
II UnknownUnknown RareRare UnknownUnknown
JJ BRIP1BRIP1 RareRare 17q23.217q23.2
LL FANCLFANCL RareRare 2p162p16
MM FANCMFANCM RareRare 14q21.214q21.2
from Kennedy and D’Andrea, Genes & Development, 2005

Clinical featuresClinical features
Incidence is 3/1,000,000Incidence is 3/1,000,000 Heterozygote frequency ~1/300 in U.S. and EuropeHeterozygote frequency ~1/300 in U.S. and Europe Ashkenzai Jewish population carrier frequency 1/89Ashkenzai Jewish population carrier frequency 1/89 Afrikaners carrier frequency 1/83Afrikaners carrier frequency 1/83
Median age at diagnosis is 5-7 Median age at diagnosis is 5-7 (Alter et al., Blood 2003)(Alter et al., Blood 2003)
Median survival is 20-30 yrs. Median survival is 20-30 yrs. (Alter et al., Blood 2003)(Alter et al., Blood 2003)
Phenotypic variability occurs even within families Phenotypic variability occurs even within families (Koc et al., Br J Haem 1999)(Koc et al., Br J Haem 1999)

Clinical FeaturesClinical Features
Characterized by Characterized by Congenital abnormalitiesCongenital abnormalities Progressive bone marrow failure Progressive bone marrow failure Increased risk of malignanciesIncreased risk of malignancies

Frequency of abnormalities in FA
Abnormality Frequency (%)
Skeletal (radial ray, hip, vertebral scoliosis, rib) 71
Skin pigmentation (café au lait, hyper- and hypopigmentation) 64
Short stature (median height 5th %ile) 63
Eyes (microphthalmia) 38
Renal and urinary tract 34
Male genitalia 20
Mental retardation 16
Gastrointestinal (eg, anorectal, duodenal atresia) 14
Cardiac abnormalities 13
Hearing 11
Central nervous system (eg, hydrocephalus, septum pellucidum) 8
No abnormalities 30
Tischkowitz, M D et al. J Med Genet 2003;40:1-10 (taken from Dokal, 2000)

Copyright ©2003 BMJ Publishing Group Ltd.
Tischkowitz, M D et al. J Med Genet 2003;40:1-10
(A) Typical radial ray abnormalities and (B) cafe au lait patches and hypopigmentation

Progressive bone marrow failure Progressive bone marrow failure Most common etiology of inherited bone Most common etiology of inherited bone
marrow failuremarrow failure• Others include dykeratosis congenita, Others include dykeratosis congenita,
amegakaryocytic thrombocytopenia, Schwachman-amegakaryocytic thrombocytopenia, Schwachman-Diamond syndromeDiamond syndrome
Increased risk of MDS and AML (15,000x)Increased risk of MDS and AML (15,000x) Many have monosomy 7, or duplication of 1q Many have monosomy 7, or duplication of 1q
(Auerbach et al., Cancer Genet Cytogenet 1991)(Auerbach et al., Cancer Genet Cytogenet 1991)
Clinical FeaturesClinical Features

Clinical FeaturesClinical Features
Increased risk of solid tumor formation Increased risk of solid tumor formation (hepatic, esophageal, oropharyngeal, (hepatic, esophageal, oropharyngeal, vulvar)vulvar) Average age at diagnosis is 23*Average age at diagnosis is 23* Cumulative incidence ~30% by age 45**Cumulative incidence ~30% by age 45**
*Shimamura et al., Gene Reviews 2002 (genetests.org)**Alter et al. Blood 2003

DiagnosisDiagnosis
Pts. with congenital abnormalities are Pts. with congenital abnormalities are often diagnosed as neonates/infantsoften diagnosed as neonates/infants
Others may be diagnosed when Others may be diagnosed when hematological problems occurhematological problems occur Median age of onset of pancytopenia is 7 Median age of onset of pancytopenia is 7
(Butturini et al., Blood 1994)(Butturini et al., Blood 1994)
Usually normal CBC at birthUsually normal CBC at birth First develop macrocytosis, then First develop macrocytosis, then
thrombocytopenia, and eventually thrombocytopenia, and eventually neutropenianeutropenia

DiagnosisDiagnosis
Based on chromosomal hypersensitivity to Based on chromosomal hypersensitivity to cross-linking agentscross-linking agents Chromosome fragility test: Mitomycin C (MMC) or Chromosome fragility test: Mitomycin C (MMC) or
diepoxybutane (DEB) added to lymphoctyes – diepoxybutane (DEB) added to lymphoctyes – increases the number of chromosome breaks and increases the number of chromosome breaks and radial structuresradial structures
• Very specific for FA, regardless of severity of diseaseVery specific for FA, regardless of severity of disease• Can do chromosome breakage analysis on amniotic cells, Can do chromosome breakage analysis on amniotic cells,
chorionic villus cells or fetal bloodchorionic villus cells or fetal blood

DiagnosisDiagnosis Difficult to screen using molecular testing due to multiple Difficult to screen using molecular testing due to multiple
complementation groups and heterogeneity of mutationscomplementation groups and heterogeneity of mutations Afrikaners: 60% of 46 pts. had deletion of exons 12-31 in Afrikaners: 60% of 46 pts. had deletion of exons 12-31 in
FANCA (Tipping et al., PNAS 2001)FANCA (Tipping et al., PNAS 2001) Ashkenazi’s: Many have mutation IVS4+4A Ashkenazi’s: Many have mutation IVS4+4A T (altered splice T (altered splice
site and deletion of exon 4) in FANCC (Gillio et al., Blood 1997)site and deletion of exon 4) in FANCC (Gillio et al., Blood 1997) Also used for carrier testing and prenatal diagnosisAlso used for carrier testing and prenatal diagnosis

Niedernhofer et al., Science 2005

FA cells were treated with mitomycin C and harvested in metaphase. Typical abnormalities include radial formation (green circle) and chromosome breaks (red arrows).

FA pathwayFA pathway
During S-phase, DNA replication is During S-phase, DNA replication is mediated by DNA polymerases acting at mediated by DNA polymerases acting at multiple replication forksmultiple replication forks
Alkylating agents such as MMC and DEB Alkylating agents such as MMC and DEB induce cross-links, halting replication at induce cross-links, halting replication at the forks the forks
When replication is halted due to cross-When replication is halted due to cross-linking, the FA pathway is activatedlinking, the FA pathway is activated

Activation of the FA pathwayActivation of the FA pathway
Activated during the S phase in response to Activated during the S phase in response to DNA replication fork arrestDNA replication fork arrest Leads to local single-stranded DNALeads to local single-stranded DNA Single-stranded DNA binds to, among other proteins, Single-stranded DNA binds to, among other proteins,
ATR (ataxia telangiectasia and RAD3-related protein, ATR (ataxia telangiectasia and RAD3-related protein, an S-phase checkpoint kinase)an S-phase checkpoint kinase)
ATR phosphorylates many DNA repair and ATR phosphorylates many DNA repair and checkpoint proteins, including CHK1 (Checkpoint checkpoint proteins, including CHK1 (Checkpoint Kinase 1)Kinase 1)
ATR and CHK1 are somehow involved in activating ATR and CHK1 are somehow involved in activating the FA pathway (Seckel syndrome)the FA pathway (Seckel syndrome)
Andreassen et al., Genes and Dev 2004Andreassen et al., Genes and Dev 2004

FA gene productsFA gene products Complex 1 may detect stalled replication forksComplex 1 may detect stalled replication forks
It appears to monoubiquitinate FANCD2 (at Lys 561)It appears to monoubiquitinate FANCD2 (at Lys 561)• FANCL may be the catalytic subunitFANCL may be the catalytic subunit
Complex 2 may be involved in DNA repairComplex 2 may be involved in DNA repair FANCD2-Ub relocalizes to chromatin (dependent on FANCD2-Ub relocalizes to chromatin (dependent on
BRCA1)BRCA1) It associates with/may promote binding of other DNA It associates with/may promote binding of other DNA
damage repair proteins, including FANCD1 (BRCA2), damage repair proteins, including FANCD1 (BRCA2), BRCA1, RAD51, PCNA, NBS1, and possibly FANCJ BRCA1, RAD51, PCNA, NBS1, and possibly FANCJ ((BRCA1-Interacting Protein [BRIP1]BRCA1-Interacting Protein [BRIP1]))
• DNA repair pathways may be involved in the pathogenesis of DNA repair pathways may be involved in the pathogenesis of inherited forms of breast cancerinherited forms of breast cancer
Kennedy and D’Andrea, Genes and Dev 2005,Kennedy and D’Andrea, Genes and Dev 2005,Fei et al., Cell Cycle 2005Fei et al., Cell Cycle 2005

Richard D. Kennedy et al. Genes Dev. 2005; 19: 2925-2940
Schematic interaction of the FA pathway
L=catalytic element?
=BRIP1
and BRCA1, RAD51, PCNA, NBS1

Richard D. Kennedy et al. Genes Dev. 2005; 19: 2925-2940
A schematic diagram depicting how the FA pathway may function to coordinate the cellular response to replication fork arrest following DNA damage

Richard D. Kennedy et al. Genes Dev. 2005; 19: 2925-2940,adapted from Niedzwiedz et al. Mol. Cell 2004; 15: 607-620.
A simplified model of FA-mediated cross-link repair that involves nucleotide excision repair (NER), translesion synthesis (TLS), and homologous recombination (HR)

Initial managementInitial management
Refer for genetic counselingRefer for genetic counseling Testing of siblingsTesting of siblings
Renal ultrasound, hearing test, eye examRenal ultrasound, hearing test, eye exam Endocrine evaluation if evidence of growth Endocrine evaluation if evidence of growth
failure (check growth hormone levels, failure (check growth hormone levels, TSH)TSH)
Referral to hand surgeon for radial ray Referral to hand surgeon for radial ray defects defects
Bone marrow biopsyBone marrow biopsy

ManagementManagement
Bone marrow failureBone marrow failure TransfusionsTransfusions Androgens (e.g. oral oxymethalone) – can improve Androgens (e.g. oral oxymethalone) – can improve
blood counts in 50% of pts.blood counts in 50% of pts.• Side effects: Masculinization, acne, hyperactivity, premature Side effects: Masculinization, acne, hyperactivity, premature
closure of epiphyses, liver toxicity, hepatic adenomasclosure of epiphyses, liver toxicity, hepatic adenomas Growth factors (G-CSF, CM-CSF) – should not be Growth factors (G-CSF, CM-CSF) – should not be
used in patients with clonal cytogenetic abnormalitiesused in patients with clonal cytogenetic abnormalities Bone marrow transplantationBone marrow transplantation
• FA cells are very sensitive to radiation and alkylating agents FA cells are very sensitive to radiation and alkylating agents – can use greatly reduced doses – can use greatly reduced doses
• 2-yr. survival 70% for allo;* 20-40% for MUD**2-yr. survival 70% for allo;* 20-40% for MUD**
*Guardiola et al. Bone Marrow Transplant 1998;**MacMillan et al., Br J Haematol 2000

ManagementManagement
Surveillance for solid tumorsSurveillance for solid tumors 42% risk of malignancy 20 yrs. after 42% risk of malignancy 20 yrs. after
transplant (Deeg et al. Blood 1996)transplant (Deeg et al. Blood 1996) Annual gyn examsAnnual gyn exams If malignancy is diagnosed, treatment is If malignancy is diagnosed, treatment is
limited by the increased sensitivity to DNA-limited by the increased sensitivity to DNA-damaging chemotherapeutic agentsdamaging chemotherapeutic agents

Management - Gene therapyManagement - Gene therapy
Goal is to permanently correct hematological Goal is to permanently correct hematological manifestations by transducing hematopoietic manifestations by transducing hematopoietic progenitor cells with a vector containing the progenitor cells with a vector containing the deficient genedeficient gene
Knockout mice with FANCC using retroviral Knockout mice with FANCC using retroviral vectors - phenotypic correction vectors - phenotypic correction (Gush et al., Blood (Gush et al., Blood 2000)2000) Clinical trial disappointing (Liu et al., Human Gene Clinical trial disappointing (Liu et al., Human Gene
Therapy 1999)Therapy 1999) Knockout mice with FANCA and FANCC using Knockout mice with FANCA and FANCC using
lentiviral vectors – more promising (integrates lentiviral vectors – more promising (integrates into the genome) into the genome) (Galimi et al. Blood 2002)(Galimi et al. Blood 2002)

ConclusionsConclusions FA is characterized by congenital abnormalities, FA is characterized by congenital abnormalities,
bone marrow failure and predisposition to bone marrow failure and predisposition to malignancies (leukemias and solid tumors)malignancies (leukemias and solid tumors)
Diagnosis is based on hypersensitivity to cross-Diagnosis is based on hypersensitivity to cross-linking agents such as DEB and MMClinking agents such as DEB and MMC
FA pathway is involved in repair of DNA cross-FA pathway is involved in repair of DNA cross-linkslinks FANCD1 is BRCA2, FANCJ is BRIP1 and FANCD2 FANCD1 is BRCA2, FANCJ is BRIP1 and FANCD2
associates with BRCA1 and BRIP1, suggesting a role associates with BRCA1 and BRIP1, suggesting a role for DNA repair pathways in the pathogenesis of for DNA repair pathways in the pathogenesis of inherited breast cancersinherited breast cancers
Treatment includes bone marrow transplantationTreatment includes bone marrow transplantation

CaseCase
The patient’s FA test was negative. She The patient’s FA test was negative. She does, however, have aplastic anemia, and does, however, have aplastic anemia, and does want to keep her baby. She met with does want to keep her baby. She met with Dr. DiPersio this week to discuss Dr. DiPersio this week to discuss transplantation.transplantation.

Richard D. Kennedy et al. Genes Dev. 2005; 19: 2925-2940
The FA pathway may function to specifically coordinate more than one pathway following cross-linking damage, whereas IR and UV damage can be repaired through
other pathways

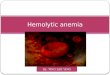
Figure 1. Some Features of Fanconi's Anemia.
The physical and cytogenetic findings in some patients with Fanconi's anemia are shown. Panel A shows the characteristically short thumb; Panel B shows a cafe au lait spot; and Panel C shows chromosomal breaks as revealed by cytogenetic analysis (A indicates chromatid breaks, B chromatid fragments, and C a dicentric chromosome). Other common clinical manifestations include short stature, skin hyperpigmentation, pancytopenia, and renal anomalies.




![Marinov - Anemia and haemorrhagic diatheses 2016 [Eng].ppt - Anemia and... · ANEMIA Time Anemias due to impaired ... Pathway Common Pathway. 4/13/2016 21 ... Marinov - Anemia and](https://img.pdfslide.us/doc/110x75/5d15387088c993e8108c4415/marinov-anemia-and-haemorrhagic-diatheses-2016-eng-anemia-and-anemia.jpg)