Embed Size (px)
Citation preview
Family Supports for Children with Disabilities Research Symposium
Family-Centred Care in Childhood Disability Services: Understanding the Steps in the Dance
Barry Trute, PhDARC Professor of Family-Centred Care
Social Work, Nursing, PaediatricsUniversity of Calgary
Edmonton (2005)
Presentation Objectives
Link the research findings of the Manitoba Studies (of families with young children with developmental and cognitive disabilities), with the conclusions of the Sobsey & Calder review of family support research:
• Family research design issues• Family support knowledge
Provide research findings from the Manitoba Studies that:– build on theoretical contributions and research of
• Dunst, Trivette et al. and
• Rosenbaum, King, King et al.– Offer practical advice for the selection of process and
outcome measures in the study of family-centred services
Shift in Service Orientation
Change in basics of relational and participatory components of practice (Dunst, 2002)
Move from professional “paternalism to enablement”, “judgemental to supportive” stances (Epps & Jackson, 2000)
Shift in Service Assumptions
Assume “normal families with special children” unless proven otherwise
Assume family is the most vital ecological context for early child development
Assume parents are the “experts” on their children (and should be “senior” service planning partners)
Assume professionals will go in and out of life of child while parents are the constants
Program Context Shapes Applied Research & Evaluation Design in Family-Centred Services
Child Service Setting:HealthAcute Care versus Chronic CareSpecialty Areas: Developmental, Oncology, Psychiatry
Child WelfareNeglect-Home Builders, Child Abuse-Family Preservation
Family Life StageYoung child with autism spectrum diagnosisElementary school child with FASDAdolescent with chronic bowel disorderMiddle-aged child with mother with dementia
Family Beliefs and CultureSocial Network SupportTrust versus Mistrust of Service Providers
The Manitoba Studies: Families with Young Children with Cognitive and Developmental Disabilities
Survey of “Strong” Families (1986)– Paediatrician and social work independent (blind) nomination– 36 families interviewed at home in rural and urban settings – separate interviews and data collection with mothers and fathers– Children with average age of 3 years
Longitudinal Family Tracking (1987, 1990, 1994)– 87 families when children were on average 5, 8 & 12 years of age– In home interviews (2-3 hours in duration)– Separate interviews with mothers and fathers in Winnipeg
Re-implementation of family-centred care in Manitoba (2003, 2004) (SSHRC: 828-1999-1037)– 111 families at 6 months after entry to childhood disability services (Time 1) and
12 months later (Time 2)– In home interviews with mothers and fathers in urban and rural communities– Children on average 4 yrs of age (with developmental & cognitive disabilities)
Components Of Information Gathering: Tracking FCS Re-implementation Study
(website: www.familystrengths.ca)
(1) Pilot Study of Families (2) Reliability Family Cohort (Quantitative Design) (3) Longitudinal Family Survey (Quantitative Design) (4) Longitudinal Family Survey (Qualitative Design) (5) Family File Reviews in child disability services (6) Service Coordinator Quantitative and Qualitative Surveys (7) Supervisor Focus Groups (8) Key Informant Qualitative Interviews
Quantitative Service Measures“Parent Perspective”
Measure of the Processes of Care (MPOC-20) (King, Rosenbaum et al.: CanChild)
Family Centered Behavior Scale (Petr & Allen: Beach Center)
Professional And Parent Alliance Scale (PAPAS) (Trute & Hiebert-Murphy)
Consumer Satisfaction Questionnaire (CSQ-8) (Attkisson)
Family Needs Survey (Bailey et al.)
Quantitative Service Measures“Professional Perspective”
MPOC-SP (King et al.)
– Self assessment for degree of “family-centred” practice
FOCUS (Bailey et al.)
– Team or program area’s degree of “family-centered” practice
Consumer Satisfaction in FCS
CS for ongoing service monitoring– Tailored to local hospital or program setting– Focus on family-centered service elements
CS as major dependent variable in FCS outcome studies– CSQ-8 (psychometric standard) – Replication with other FCS studies
• (e.g., CanChild: McMaster University)
Family-Centered Practice and “Working Alliance”
(PAPAS: parent feels understood & respected, while having trust & hope in service provider)
Dunst et al.: “Relational elements”Rosenbaum et al.: “Respectful and supportive care”
Items in the Professional and Parent Alliance Scale (PAPAS: Trute & Hiebert-Murphy, 2005)
Scale Question: “When you think of the relationship you have with your (family worker, etc.)”:
Items are scored on the following five-point Likert scale: (1) Never, (2) Rarely, (3) Some of the time, (4) Most of the time, (5) All of the time
Example Items:
1. I feel the worker respects me as a person2. I feel annoyed with the worker*3. I feel the worker understands my needs and
priorities
*Item 2 is scored in reverse
Research Issue:Clarify Key Components of FCP
Is Family-Centred Practice essentially having a “positive working alliance” between professional and parent – (i.e., professionals having good relations
with parents)? Dunst, Trivette et al. hypothesis:
– FCP contains both “relational” and “participatory” practices
Mothers as Primary Evaluators of Family-Centred Services in Manitoba Studies
Statistical analysis issue– Independence of mother/fathers scores when served by
same service provider and in same family (fundamental assumption)
Sample size issue– More statistical power with larger sample (which is usually
mothers, as fathers often defer to mothers’ greater contact with professionals and service knowledge)
Separate gender analyses highly informative– when have adequate samples of mothers and fathers
Predicting Mothers’ Consumer Satisfaction with FCS - MPOC (N=86)
Hierarchical regression (dep=CSQ-8)
Step 1: PAPAS– F(p<.001) t-papas(p<.001) r2=.49
Step 2: PAPAS & MPOC-20– F(p<.001) t-papas & t-mpoc (p<.001)– R square change=.07 with MPOC (p<.001)
Predicting Mothers’ Consumer Satisfaction with FCS - FCBS (N=86) Hierarchical regression (dep=CSQ-8)
Step 1: PAPAS– F(p<.001) t-papas(p<.001) r2=.49
Step 2: PAPAS & FCBS– F(p<.001) t-papas & t-mpoc (p<.001)– R square change=.11 with FCBS (p=.008)
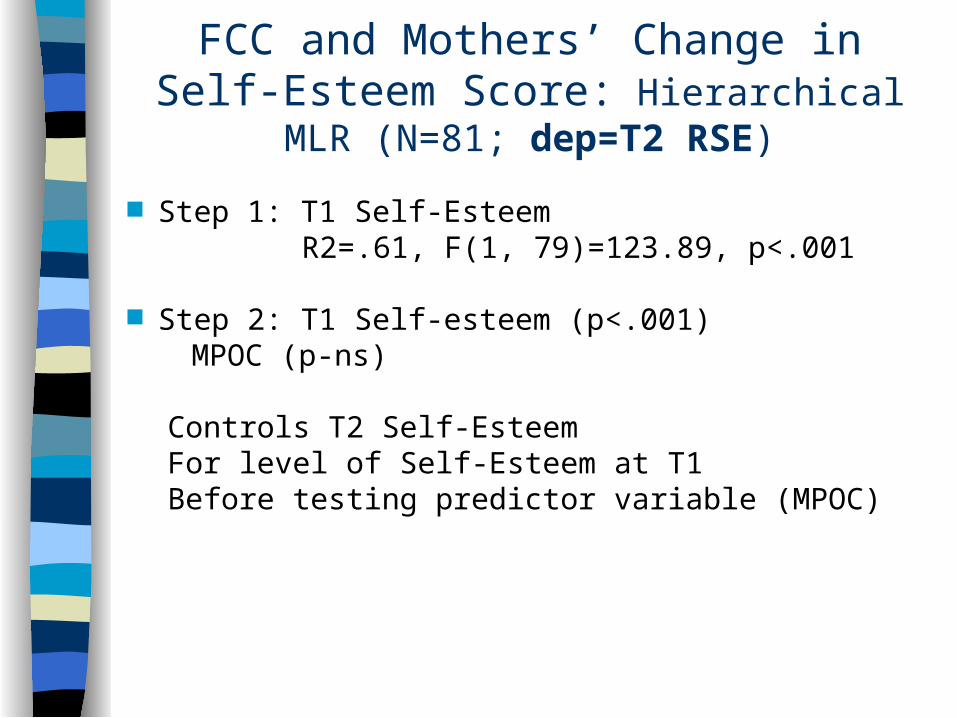
FCC and Mothers’ Change in Self-Esteem Score: Hierarchical MLR (N=81; dep=T2 RSE)
Step 1: T1 Self-EsteemR2=.61, F(1, 79)=123.89, p<.001
Step 2: T1 Self-esteem (p<.001)MPOC (p-ns)
Controls T2 Self-Esteem For level of Self-Esteem at T1Before testing predictor variable (MPOC)
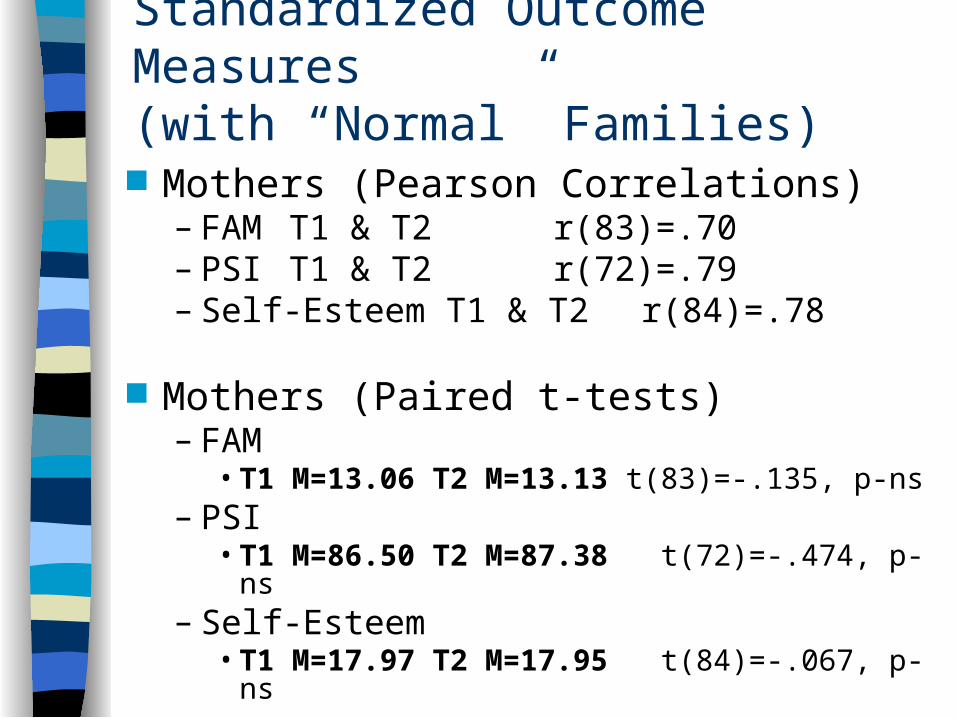
Standardized Outcome Measures (with “Normal” Families)
Mothers (Pearson Correlations)– FAM T1 & T2 r(83)=.70– PSI T1 & T2 r(72)=.79– Self-Esteem T1 & T2 r(84)=.78
Mothers (Paired t-tests)– FAM
• T1 M=13.06 T2 M=13.13 t(83)=-.135, p-ns– PSI
• T1 M=86.50 T2 M=87.38 t(72)=-.474, p-ns– Self-Esteem
• T1 M=17.97 T2 M=17.95 t(84)=-.067, p-ns
Model of FCC: LEVELS OF SERVICE COORDINATION (CASE MANAGEMENT) OUTCOMES in Children’s Services From Perspective of Parents
1. Family Resource Acquisition and Family Problem Solving
2. Improved Interpersonal Relations (e.g., parent-child)
3. Enhanced Family Environment(Vital Developmental Context for Young Children)
Level 1:Resource Acquisition and Family Problem Solving
Family Needs Survey (Bailey & Simeonsson, 1988)
Information (7 items) Family & Social Support (8 items) Financial (6 items) Explaining to Others (5 items) Child Care (3 items) Professional Support (3 items) Community Services (3 items)
– (items scored: yes, not sure, no)
Three Factor Solution for FNS
Need for Information (9 items)
Need for Help with Resource Management (12 items)
Need for Facilitative Counseling (12 items)
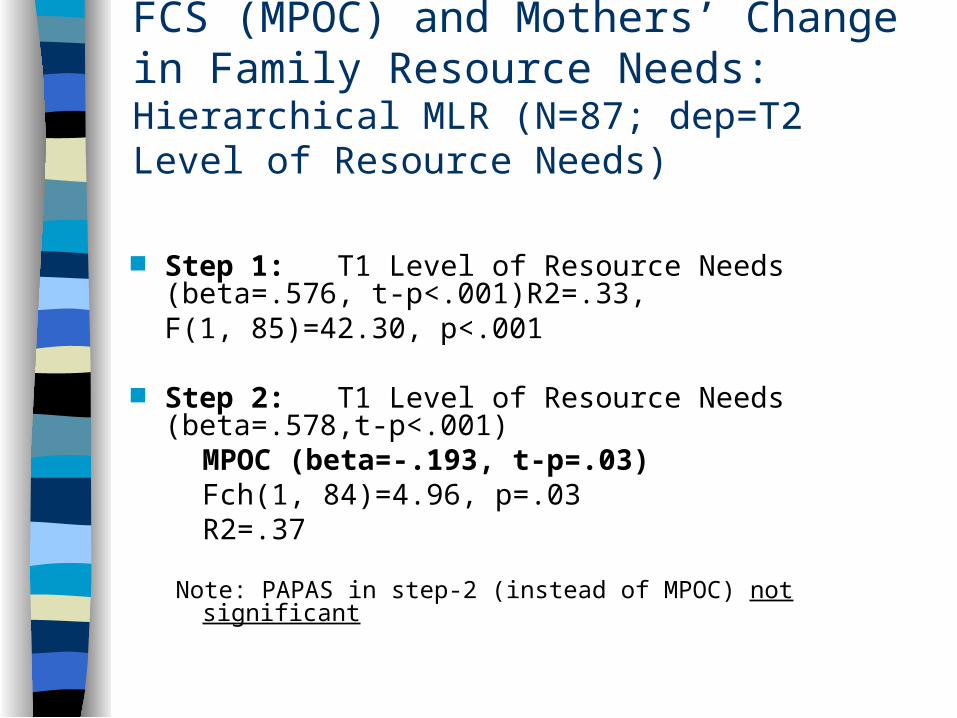
FCS (MPOC) and Mothers’ Change in Family Resource Needs: Hierarchical MLR (N=87; dep=T2 Level of Resource Needs)
Step 1: T1 Level of Resource Needs (beta=.576, t-p<.001)R2=.33, F(1, 85)=42.30, p<.001
Step 2: T1 Level of Resource Needs (beta=.578,t-p<.001)
MPOC (beta=-.193, t-p=.03) Fch(1, 84)=4.96, p=.03R2=.37
Note: PAPAS in step-2 (instead of MPOC) not significant
F-C Practice Implications Evidence suggests Working Alliance (WA) interwoven
with Capacity Building (CB): “Partnership-Enabling” (CanChild) or “Participatory Experiences” (Dunst, Trivette et al.)
We hypothesize that WA precedes CB in childhood disability services (must have WA to serve as a basis for CB, and must have skills for CB)
Alberta FSCD Act requires service plan (IFSP) which is a primary opportunity for CB
Social network and psychosocial supports vital to CB and are key assessment issues
First order of business in CB is information exchange, resource acquisition, and family problem solving





























