Embed Size (px)
Citation preview

Family Planning inA Review of National and District Policies and Budgets
Rwanda
Prepared by: Gitura Mwaura & Annette Mukiga



Abbreviations 4
1. Executive Summary 7
2. Introduction And Background 8
2.1 CountryProfile 9
2.2 Objectives Of The Study 11
3. Methodology 12
3.1 Research Methodology 12
3.2 Limitations 13
4. Findings And Analysis 14
4.1 Policy Analysis 14
4.1.1 Prioritization Of FP 17
4.1.2 Sustainability Of FP Programmes 18
4.1.3 Policy Responses to Unmet Need 18
4.1.4 ChallengestoImplementationFPProgrammes 19
4.2 Conclusion on Policy Analysis 20
4.3 Gatsibo District 20
4.3.1 DistrictProfile 20
4.3.2 Health Facility Analysis 21
4.3.3 Key FGD Findings 21
4.3.4 PolicyResponsestoUnmetNeedIssuesIdentifiedby
Communities 22
4.4 Budget Analysis 22
4.4.1 Overall National Budget Trends 22
4.4.1.1 Oecd Support 22
4.4.1.2 National Budget Trends 24
4.4.2 NationalFamilyPlanningBudget(Fy2009/10-Fy2013/14) 25
4.5 DistrictBudgetAnalysis 27
4.5.1 FPBudgetinGatsiboDistrict 27
4.5.2 FamilyPlanningUsersExperienceandOpinionon
Budgeting Process 27
4.6 Conclusion on Budget Analysis 27
5. Conclusions 28
5.1 Recommendations 29
6. References 30
3
A Review of National and District Policies and Budgets
Contents

2
Family Planning in Rwanda
Published by:
RWANDAWOMEN’SNETWORKKinyinyaSector,Gacuriro(nexttoSOSTechnicalSchool)KG 428 StreetP.OBox3157,Kigali,RWANDATel:+250788334257
Email:[email protected]/[email protected]:www.rwandawomennetwork.org
and
DSW(DeutscheStiftungWeltbevoelkerung)HatheruRoad,HatheruCourt(Lavington)
P.OBox2438-00202Nairobi,KenyaTel:+254202731398/203592302Mobile:+254726603768/736616491
Email:[email protected]:www.dsw-online.org
Authors:GituraMwaura&AnnetteMukiga
Cover photo credit:RwandaWomenNetwork
Layout and Design: SprintDesignwww.sprintdesign.com.pk
©RwandaWomenNetworkandDSW(DeutscheStiftungWeltbevoelkerung)
All forms of copies,reproductions, adaptations, andtranslations through mechanical,electrical, or electronic means,shouldacknowledgeRwandaWomenNetwork(RWN)as the source.
May 2014

5
A Review of National and District Policies and Budgets
Acknowledgements
RwandaWomen’sNetwork(RWN)wishestoexpressgratitudetotheRwandaReproductiveHealthandRightsConsortium(RHR)membersnamely,Benishyaka,Haguruka,HealthDevelopmentInitia-tive,ARBEF,AJPRODHOandUrunanaDCfortheiractiveparticipationinmakingthisanalysisareality.
TogetherwithRHRConsortium,wethanktheGovernmentofRwandaforprovidingthedatainformingthis policy and budget analysis. The government stands commended for the foundation it has already put in place towards enhancing family planning services in the country.
WeappreciateofficersandstaffatGatsiboDistrictHospital,KiziguroHospitalandGakenkeHealthCentrefortakingtimeofftheirbusyschedulestoshareinformationtoinformthisstudy.
RWNthanksDSW(DeutscheStiftungWeltbevoelkerung)fortheirpartnershipandcontinuedsupportthroughtheEuroleverageProject.WeareindebtedtotheDSWEuroleverageteamledbyMankaKway(ImpactTrackingCoordinator),andLuciaChebettLaboso(InternationalProgrammeCoordinator)fortheirsupportandfeedbackduringthereviewandreportingprocess.
We reserve our greatest appreciation especially, the women, men and youth of Kiramuruzi and Mu-rambiSectorswithoutwhomthepictureonthegroundmaynothavebeenclarifiedonFamilyPlanningand health issues directly affecting communities in Rwanda.
Thankyou!The Reproductive Health Rwanda Consortium
ARBEF-AssociationRwabdaiseleBeinEtreFamilialAJPRODHO - JIJUKIRWA
HAGURUKA NGO

AIDS AcquiredImmuneDeficiencySyndrome
ASRH AdolescentSexualandReproductiveHealth
CPR Contraceptive Prevalence Rate
EDPRS II EconomicDevelopmentandPovertyReduction
Strategy 2013–2018
FP Family Planning
FY Financial Year
HIV HumanImmunodeficiencyVirus
HMIS Health Management Information System
iHRIS Ministry of Health Human Resources Database
IUD Intrauterine devices
MCH Maternal and Child Health
MDG Millennium Development Goals
MMI Military Medical Insurance
MoH Ministry of Health
OECD OrganisationforEconomicCo-operationand
Development
PRSP Poverty Reduction Strategy Papers
RAMA LaRwandaised’AssuranceMaladie
RDHS Rwanda Demographic Health Survey
RH Reproductive Health
RIDHS Rwanda Interim Demographic Health Survey
RWF Rwandan Francs
SRH SexualandReproductiveHealth
TFR Total Fertility Rate
WHO World Health Organization
4
Family Planning in Rwanda
Acronyms

7
A Review of National and District Policies and Budgets
1. Executive Summary
The Family Planning Policy 2012 has received particular attention as a development priority to ensure maximumcontributiontoRwandaachievingofMDGsandoveralldevelopment.FPhasbeenhigh-lightedinrelatedpoliciesandintheVision2020andtheEconomicDevelopmentandPovertyReduc-tionStrategy2013–2018(EDPRSII).
Government commitment can be seen in the commendable achievements gained in FP. Modern con-traceptiveprevalenceratemorethanquadrupledfrom10%in2005to45%in2010.Thetotalfertilityrate decreased from 6.1 per woman in the same period to 4.6 children.
However, many challenges remain. Some of these challenges include myths, rumors and mispercep-tions about FP methods and their side effects, requiring efforts to address them with correct informa-tionandFPcounselingsessions.Therealsoexistgaps inSRHeducationatdifferent levels,whilesocio-culturalandreligiousinfluencesthataffectservicedemandfromthepopulation.
ThechallengeshavedefinedthenationalprioritiesarticulatedintheFPPolicy.Amongothers,thepri-orities include improving awareness of FP and access to FP services for women, men and youth using social communication and mobilization programs. Others are integrating FP in Safe Motherhood and ChildHealth services and strengtheningmen’s participation through community-based structures,organizationsandnetwork.
An assessment was conducted to establish the national FP trends as they manifest at the village level. This allowed for a deeper interrogation of the national policies from the grassroots perspective. The assessment is part of a regional study to establish the level of policy engagement and budget commit-ment at national and district level that address unmet needs of family planning.
GatsiboDistrictwasidentifiedasacasestudyforthisanalysisinRwanda,asitisrepresentativeofmostdistrictsacrossRwandaindemographyandsocio-culturalattitudes.
Findingsfromthedistrictreflectedthenationaltrends.Thekeyissuesofconcernidentifiedatdistrictlevel are youth pregnancies and high prevalence of myths and misperceptions about FP methods and their side effects.
The following recommendations for advocacy are therefore proposed enjoining the Government and internationalpartnerstoallocateadequateresources,bothfinancialandhumanto:
• Fightmisperceptions,mythsandrumorsaboutFPmethodsandtheirsideeffects, includingimprovementofmethodmixes,throughthemediaandatthecommunitylevel through CHWs;• ReachandinvolvetheyouthinrelevantRH&FPprogrammes;• AdvocatetowardsthegovernmenttoincreaseFPbudget,andtheinternationalcommunity tobeginofferingFPbudgetarysupportbystartofnextfinancialyear,2014/2015.

6
Family Planning in Rwanda

9
A Review of National and District Policies and Budgets
2.1 Country Profile
Asperthelastcensus(2010)Rwanda’spopulationstoodat10,537,222,upfrom8,128,553in2002.Thispresenteda29.6percentriseinthepopulationduringtheperiod.Annualpopulationgrowthratestoodat2.6percent,downfrom2.9percentin2002.Womenconstitute51.8percentofthetotalpopulation;downfromapproximately53percentin2002.Populationdensitygrewfrom321peoplepersquarekilometer in2002 to416 in2012.TheCensusput theaveragehouseholdsizeat4.37,reflectingadropinthefertilityrate,from5.5to4.6childrenperwomanby2010.
The infantmortality ratedecreasedfrom86per1,000 livebirths in2004to50per1,000 livebirthsin2010andtheunder-fivemortalityratedeclinedfrom152to76per1,000livebirthsoverthesameperiod (RwandaDemographicHealthSurvey [RDHS], 2010). The 2010RDHS shows a significantreductioninthematernalmortalityratiofrom750per100,000livebirthsin2005to476per100,000livebirthsin2010.Ifthepaceofthisdeclinecontinues,RwandaislikelytomeettheMDGsrelatedtochildandmaternalmortalityby2015.
HIVprevalencehasremainedconstantat3%between2005and2010.Therewasadeclineofma-lariaprevalencebyhalfsince2007–08from2.6%to1.4%amongchildrenage6to59months,andfrom1.4%to0.7%amongwomenaged15–49(RDHS2010).Notably, thesetwodiseasesplaceasignificantburdenonthehealthsystem.In2008,theyaccountedfor35%ofhospitalmortalitycases(RwandaInterimDemographicHealthSurvey[RIDHS],2007/2008).
WhileFPserviceshavebeen,andcontinuetobeprovidedfreeofcharge,approximately23%ofpa-tientshavetowalkformorethanonehourormorethan5kilometerstoreachthenearesthealthfacility(HealthManagementInformationSystem[HMIS];2009).TheWHOrecommendedmaximumtimetoaccesshealthcareis30minutes,withtheimplicationthatthereexistsaneedforcloserhealthservicestonearlyaquarterofallpatients.Onaverage,96%of thepopulationwascoveredbyCommunitybasedInsurancein2012(HMIS).Availabilityofhealthcareprofessionalshasimproved:in2011therewere625doctorsand8,513nurses/midwivesworkinginRwanda.Basedon2012datafromtheMin-istryofHealthHumanResourcesDatabase(iHRIS),thiscorrespondstoaratioof1doctorper15,428inhabitants, 1 midwife per 23,364 inhabitants, and 1 nurse per 1,138 inhabitants. For midwives, this representedanimprovementfromImidwifeper66,749inhabitantsin2010(AnnualReport,MinistryofHealth2012).
Family planning services are delivered largely within the public sector health system and include com-munity-baseddistribution(CBD)ofcontraceptives,thoughCBDofinjectablecontraceptivesisyettobefullyimplementedin10outofthe30districtsnationally.ImprovementofHIVandMNCHisalsoattributedtoimprovedaccesstoanti-retroviraldrugsandintegrationofhealthservices.
Despite commendable progress in meeting RH and FP needs of Rwandese people, there is still unmet needforFP.Oneoutoffive(19%)currentlymarriedwomenhasanunmetneedforFP(animprove-mentsince2005,whenthefigurewas38%):10%haveanunmetneedforspacingand9%haveanunmet need for limiting. Consequently, the total demand for FP among currently married women is

8
Family Planning in Rwanda
2. Introduction and Background
Reproductive health (RH) and family planning (FP) have received global and national recognitionnotonlyaskeytoindividualwell-being,butcollectivelytonationaldevelopment.TheGovernmentofRwanda(GoR)iscommittedtovariousinternationalpolicyprotocolswhichit issignatory, includingthe ICPD and Maputo Plan of Action, both of which relate to the MDGs. The Rwanda National Family PlanningPolicy2012aimstoensurethemaximumcontributiontoRwanda’sachievementofMDGsand overall national development relative to its population growth trends.

11
A Review of National and District Policies and Budgets
2.2 Objectives of the Study
The primary objectives of the study was to
• Assesstheextenttowhichfamilyplanningandotherreproductivehealthissuesareprioritized in broad development and health policies and strategies. • Understandkeypolicyandprogrammepriorities,includingpolicyimplementationchallenges and responses considered critical for the achievement of national policy objectives• Establishtheextenttowhichkeyfamilyplanningissuesidentifiedbycommunities’members arereflectedinthepolicies.
Thereporthighlightspolicygapsexistinginthenationalfamilyplanningprogrammeatthedistrictandgrassrootslevels(usingGatsibodistrictasacasestudy).Itdrawsoutpolicyandbudgetaryrecom-mendationsforadvocacybytheRwandaWomen’sNetworkandthecivilsocietyreproductivehealthand family planning platform in the country. . Importantly, the report also draws government attention to the issuesat thecommunity levelandalso identifiespriorityareas forboth thegovernmentanddevelopment partners at the grassroots level.

10
Family Planning in Rwanda
Key Rwandan Health Indicators
Population and Medical Personnel
• Totalpopulation:10,537,222(2012Census)• PerCapitaUtilizationofHealthFacilities:0.79visitspercapita• (HMIS,2012)–DHS2010reports1.8women,1.5men.• Doctors:1/15,428inhabitants(AnnualReportoftheMinistryofHealth2012)• Nurses:1/1,138inhabitants(AnnualReportoftheMinistryofHealth2012)
Key Health Indicators RDHS 2005 RDHS 2010
• NeonatalMortality(per1,000livebirths) 37 27• InfantMortality(per1,000livebirths) 86 50• Under5Mortality(per1,000livebirths) 152 76• Proportionofstuntedchildren 51 44• Proportionofwastedchildren 5 3• Proportionofunderweightchildren 18 11• MaternalMortality(per100,000livebirths) 750 487• ModernContraceptivePrevalenceRate(CPR) 10% 45%• TotalFertilityRate 6.1 4.6
HIV and AIDS and Other Epidemics
• HIVPrevalence:3%(DHS,2010)• TBcasedetectionrate27%(TRACPlus/WHO2009)• Malariaprevalenceinchildren<5:1.4%(RDHS,2010)• ChildrenunderfivesleepingunderLLIN:70%(RDHS,2010)
Rate of Enrolment in Community Based Health Insurance(Rwanda health statists Booklet, 2011 )
Insuranceenrolmentat96%asof2012
72%,andalmostthreequartersofthatdemand(74%)issatisfied.Thedemandforlimitingisslightlyhigherthanthedemandforspacing(39%and34%,respectively;RDHS2010).
In order to inform efforts towards meeting the demand for FP services and satisfying the unmet need forFP,thereisneedtounderstandtowhatextentthepolicyenvironmentforFPinRwandaisaddress-ingtheFPneedsofRwandesepeopleandtrackallocationofresourcesforFPatnationalandsub-national levels. To address this gap, a study was conducted in Rwanda as part of a regional policy and budgetanalysisofRHandFPinEastAfricatoestablishthelevelofpolicyengagementandbudgetcommitment at national and district level that address unmet needs of family planning.

13
A Review of National and District Policies and Budgets
Fourfocusgroupdiscussions(FGDs)comprisingtwowomenonlygroups,andonemenonlygroupand a youth only group. FGDs sought to draw out community perceptions on access and hurdles to FPservices.Keyinformantinterviews(KIIs)wereconductedwiththeHeadofBudgetsattheMinistryofFinance,HeadofFamilyPlanningatMinistryofHealth,GatsiboDistrictHealthOfficerandsub-districthealth supervisor. KIIs sought to provide an overview of policy implementation on the ground, includ-ing access and any hurdles thereof to FP services from the national to the grassroots levels.
A standard FGD guide developed for countries in the region under the DSW program was adapted tosuitaRwandanlocalcommunitysituation.Priorityissuesarisingwererankedasidentifiedbyeachgroupduring thediscussions. The ranked issues for all thegroupswere synthesized to drawoutsimilarities and crosscutting concerns to come up with representative community priorities. Similarly, a discussion guide was used to conduct KIIs and data collected thematically analyzed to bring out issuesofconvergenceregardingtheprioritiesidentifiedbytheFGDs.
ThepriorityissuessynthesizedfromtheFGDsandKIIswerethenanalyzedagainsttheexistingfamilyplanning policy and implementation strategy, including the national and district budgets, to draw out the advocacy issues.
GakenkeHealthCentreintheDistrictwasvisitedtosampleFPservicesofferedatthegrassrootslevel.Thehealthcenterwas identifiedas themostappropriateas itserviced thewidestcross-sectionofcommunity members in the district. A survey tool developed for the regional analysis was used.
3.2 Limitations
One of the study limitations was inability to obtain budget information from the MoH to analyze against the national budget allocation. The budgets available from the district were only Financial Years 2012/2013 and 2013/2014making it impossible to analyze trends. Time allocated to conduct theanalysiswasnotsufficient.Unliketheothercountries,theRwandateamconductedthestudyinonlyonedistrictwhilethestudycouldhavebenefitedfromexamininganotherdistrictwherecommunity-based FP services are not fully implemented

12
Family Planning in Rwanda
3. Methodology
3.1 Research Methodology
Thestudyundertookacasestudyapproach.Bothquantitativeandqualitativemethodswereusedtocollect data including:
Reviewofexistingpoliciesrelatedtoreproductivehealthandfamilyplanningandbudgetdocuments.These included the Vision 2020 and the Economic Development and Poverty Reduction Strategy2013–2018(EDPRSII);theNationalPopulationPolicyforSustainableDevelopment2003;theNationalHealth Policy 2004; the National Reproductive Health Policy 2003; and, the Family Planning Policy 2012. Other documents included national development plans, including those of Gatsibo District, the national demographic and health survey, newspaper reports, and the national and district budgets. PolicieswerereviewedtoexaminetheextenttowhichFPconcernsareaddressed.Budgetdocumentswere reviewed to identify any budgetary gaps and funding available for effective FP implementation.

15
A Review of National and District Policies and Budgets
OtherbroaderpoliciesthatrecognizethebenefitsofFPinclude,theVision2020,theEconomicDe-velopmentandPovertyReductionStrategy2013–2018(EDPRSII),NationalPopulationPolicyforSus-tainable Development 2003, National Health Policy 2004 and the National Reproductive Health Policy 2003.
TheVision2020isRwanda’sleadingplanningframework,whichisusedtoguideoveralldevelopmentinRwanda.Vision2020placesemphasisontheharmonizationofpopulationgrowthwiththecountry’seconomicdevelopmentandreductionofthemaincausesofmortality—specificallyaimingtoreducethetotalfertilityrate(TFR),decreaseinfantandmaternalmortality,andultimatelyreducingpopulationgrowth.Vision2020singlesoutFPascrucialforreducingbirthratesandtheprevalenceofHIVandAIDS if double protection is used as recommended.
TheEDPRSIIidentifieshighpopulationgrowthasamajorchallengeandarticulatingtheexistingas-sociationbetweenpovertyandpopulationdensity. IthighlightsFPasakey interventiontoaddressthischallenge.EDPRSIIsetitsprioritiesas:strengtheningreproductivehealth(RH)servicesandFP;ensuring free access to information, education and contraceptive services.
TheNationalPopulationPolicyforSustainableDevelopment2003takesintoaccountRwanda’sadop-tion of resolutions of the 1994 InternationalConference onPopulation andDevelopment inCairo.ThePolicypresentsamulti-sectoralapproachtoimprovingthepopulation’squalityoflife.Inadditionto reducing the population growth rate, this policy also focuses on economic growth, food security, health, education, human resource development, and rational management of the environment and good governance. It presents a number of quantitative targets consistent with those presented in Vision2020andthePovertyReductionStrategyPapers(PRSP).The2003PolicyaffirmsFPaimstoensuremaximumcontributiontoRwanda’sachievementofMDGsandoverallnationaldevelopment.
The National Health Policy outlines the roles of the central government, provincial and district struc-turesandemphasizesthenormsestablished in1998for theminimumpackageofactivities,whichincludesFP,andthecomplementarypackageofactivitiestobeprovidedatthehospitalandhealthcenter levels. This policy describes the role of FP as contributing positively to the health status of the family.Italsohighlightstheconceptofpartnershipsasakeymeansofachievingintegration,includinginter-sectoralintegrationofservices.TheNationalHealthPolicycallsforgreaterhealthsectorfinanc-ingandurgesinitiativestostrengthensolidarity,suchascommunity-basedhealthinsurance,prepaidhealth insurance and other health insurances. It establishes the principles of cost recovery and fee for service,whileensuringtheestablishmentoffinancingmethodsforthoseunabletopay.Aswiththeabove,NationalHealthPolicyaffirmsFPaimstoensuremaximumcontributiontoRwanda’sachieve-ment of MDGs and overall national development.

14
Family Planning in Rwanda
4. Findings and Analysis
4.1 Policy Analysis
ThissectionoffersanoverviewaswellasananalysisoftheexistingpoliciesrelatedtoRHandFP,andhowtheyrelatetoprioritiesidentifiedatthecommunitylevel.
TheGovernmentofRwanda(GoR)accords reproductivehealthand familyplanning importance tonational development. GoR is committed to the various international policy protocols and is signatory to the ICPD and Maputo Plan of Action, both of which relate to the MDGs (also see Table 2 below for summaryofprinciplesobserved).
TheNational Family Planning Policy 2012 aims to ensure themaximum contribution to Rwanda’sachievementofMDGsandoverallnationaldevelopment.TheFPresponsivepolicesaffirmaimatat-tainingMDG2(achievinguniversalprimaryeducation)andMDG3(promotinggenderequalityandempoweringwomen).ThisincludesMDG4(reducingchildmortality)andMDG5(improvingmaternalhealth).

17
A Review of National and District Policies and Budgets
Adolescent SRH information and services
Contraception
Sexualrights
Population Policy for Sustainable De-velopment 2003; National Health Policy 2004; National Reproductive Health Pol-icy 2003; Family Planning Policy 2012
ASRHisaffirmedinFPPolicy2012asabove noted
AffirmedintheFPPolicy2012asabovenoted
AffirmedintheFPPolicy2012asabovenoted
4.1.1 Prioritization of FP
TheFamilyPlanninghasreceivedparticularmentionasadevelopmentprioritytoensuremaximumcontribution to Rwanda achieving of MDGs and overall development. It is recognized that FP not only allows families to space and limit their births when desired, but it can also reduce the costs of meeting multiple MDGs as a crosscutting development issue.
FPhasbeenhighlightedinVision2020andtheEDPRSII.Vision2020singlesoutFPascrucialforreducingbirthratesandtheprevalenceofHIVandAIDS.UnderEDPRSIIhealthisgenerallyplacedundertheFoundationalSector in“Thepursuitof long-termpriorities inhealthandbasiceducation,macroeconomicstabilityandpublicfinancemanagement,justice,peaceandstability,foodsecurityandnutritionanddecentralizationthatconstitutetheplatformofRwanda’ssustainabledevelopment.”
Rwanda’sstrongpoliticalsupportforFPisnotedinthestatusreportonimplementationofthe2006–2010NationalFPPolicyandFive-YearStrategyandisakeydriverofgovernmentcommitmentforFP.The President has been at the forefront championing family planning agenda locally and internation-ally, most recently at the 2012 London Summit on Family Planning. However, while there is laudable political leadership on FP issues at all levels leaders should be continually reminded of their obliga-tions at the personal, local, national and global levels.
ItisduetotheexistingpoliticalwillthatFPreceiveshighpriorityunderMCH,includinghavingitsownnational policy and implementation strategy. However, the FP budget allocation has been declining in thelastthreeyears(seeBudgetAnalysis)implyinganeedtopushforanincreaseinprioritizationofFP in the MoH hierarchy.

16
Family Planning in Rwanda
Table 2: Summary of Policies against Principles observed
Principle observed Details of Policies
Advancing gender equality and equity and the empowerment of women, including education for girls
Population issues articulated are integral parts of eco-nomic and social development
Interrelationships and balance between population, resources and development are fully recognized as an integral part of sustainable development
All couples and individuals have the basic right to de-cide freely and responsibly the number and spacing of their children and to have the information and means to do so.
Allocation of least 15%of national annual budgets toimprove the health sector.
Policiesexplicitlyreaffirmcommitmentanduniversalaccess to:
Safe abortion
The FP responsive polices affirm toworking towards attainingMDG2, i.e.,achieving universal primary education and MDG 3, promoting gender equality and empowering women
Population issues are articulated in Vi-sion2020and theEconomicDevelop-ment and Poverty Reduction Strategy 2013–2018 (EDPRS II), including theNational Population Policy for Sustain-able Development 2003; the National Health Policy 2004; the National Re-productive Health Policy 2003; and, the Family Planning Policy 2012
The interrelationships are recognized in Vision2020andtheEDPRSII,andintheabove mentioned policies
The right to decide freely and respon-sibly the number and spacing of their children and to have the information and means to do so is articulated in the FP Policy 2012, synthesizing from the above mentioned policies.
Rwanda has achieved 18.8 per cent in the period 2010 – 2012 achieving the 2006 Abuja Declaration targets on health
Safeabortionaffirmedinthepenalcodeonly where the life of the mother is medi-cally proved to be in danger, though notexplicitlymentioned in theNational

19
A Review of National and District Policies and Budgets
Additional strategies towards the FP policy implementation, further to the above mentioned prioritized approaches:
• DesigninganddisseminatingappropriateFPmessagesformassmedia(radio,TV, newspapers,etc.),andinformation,educationandcommunication(IEC)/FPtools(posters, flyers,flipcharts,etc.)• RaisingFPawarenessamongmenduringpoliticalandadministrativemeetings• Involvingcommunity-basedassociationsandorganizationsofwomenandyouthinFP awareness-raisingactivities• IntegratingFPintrainingcurriculaatprimary,secondaryandhighereducationlevels,with thecollaborationoftheMinistryofEducation• Trainingandconductingrefreshertrainingofhealthprovidersincontraceptivemethods andcommunication/counselingtechniques;strengtheninglogisticsforcontraceptivesand related materials• Developingpostnatalcare,includingFPstrengtheningmen’sparticipationinFPprograms• Preventearlypregnancies(amongadolescentpopulations)aswellashighlightingbenefits ofFPuseamongmost-at-riskpopulations,suchassexworkers,throughcontraceptives offeringdualprotectionagainstpregnancyandHIV.
4.1.4 Challenges to implementation FP programs The main challenges for implementing FP include:
• Increasedcostofcontraceptionasdemandincreases.(TheGovernmentaimstoincrease contraceptiveuseto70percentfromthecurrent45percent)• Therearestillmyths,rumorsandmisperceptionsaboutFPmethodsandtheirsideeffects, requiring efforts to address them with correct information and FP counseling sessions.• TherestillexistsagapinSRHeducationatdifferentlevels,includinginfamiliesandschools, yet these represent a great window of opportunity for children and adolescents to learn about such issues at an early age.• Therestillexistsocio-culturalandreligiousinfluencesthataffectFPservicedemandfrom the population.• Lackofdecision-makingpowerofwomenaboutuseofFPandinsufficientsupport, participation and sometimes violence from their male partners.• PerceptionofFPas“limitationofbirths”andthereforeonlyappropriateformarriedpeople.• Impactofthegenocide(post-genocidedesiretoreplacethoselost).

18
Family Planning in Rwanda
4.1.2 Sustainability of FP Programs
FPisfundedfromrecurrentbudgetwithoutexternalsupport(seeOECDSupportbelow).Sustainabilityof the FP programme has been seen as a challenge. As noted above, there is recognition that as demand and use of FP services increases; it will become more and more of a challenge to cover the costs of contraception.
Plans to addressing the programme sustainability are implicit in achieving and maintaining high levels ofawareness,increasingliteracyamongwomenandgirls,genderequalityandsocio-economicem-powerment. And with the goal of attaining 70 percent CPR, it is inevitable that the costs of contracep-tionwillrisethatmaynecessitateexternalsupport.ThisunderscorestheaimforresourcemobilizationundertheEurolevarageproject.
4.1.3 Policy responses to unmet need
TheRDHS2010shows thatunmetneed forFP is19%.Theseareequally splitbetween theneedforspacing(10%)andtheneedforlimitingthenumberofchildren(9%).Whileimpressivegainsbymethodhavebeenreflectedovertime,thecurrentmethodmixdoesnotappeartoaddresswomen’swide range of fertility preferences.
According to the2010Survey, themethodmix isdominatedbyshort-actingmethods,particularlyinjectables (26%),but thecontributionofpills (7%)andcondoms(3%) isalsosignificant.Theonlylong-actingmethodthatcontributedsignificantlywasimplants(6%),withfemalesterilizationandintra-uterinedevices(IUDs)atlessthan1%,andtuballigationat0.8%.Thedataindicatethatmaleparticipa-tion is mainly through the use of condoms, mainly by youth and unmarried men.
TheFPPolicy2012observesthatdependenceonshort-actingmethods,inasettingwherethede-mandishighandunmetneedissignificant,callsforfurtherexamination.
The FP Policy 2012 aims to reduce unmet need for FP through a number of approaches:
• ImprovingawarenessofFPandaccesstoFPservicesforwomen,menandyouthusingsocial communication and mobilization programs• IntegratingFPinSafeMotherhoodandChildHealthservices• Strengtheningmen’sparticipationthroughcommunity-basedstructures,organizationsand network• ImprovingFPserviceproviders’skillsutilizingrecommendedeligibilitycriteriaforcontraceptive prescriptionfromtheWorldHealthOrganization(WHO)• IncreasingavailabilityandrevivalofFPservicesinallhealthfacilities(publicandprivate)• EstablishingasystemtomonitorFPactivitiesinallhealthcentersatalllevels(community, district,province,national);and• InvolvingpoliticalandadministrativeauthoritiesandcommunityleadersinFPmobilization.

21
A Review of National and District Policies and Budgets
4.3.2 Health Facility Analysis
GakenkeHealthCentreservingKirimuruziSectorwasvisitedtoassessthelevelofFPserviceprovisionatcommunitylevel.Thefollowingwerethefindings:
• FPserviceasidentifiedinthesurveytoolwasreadilyavailable• Staffingisinadequate,accordingtotheDirectoroftheHealthCentre• StaffathealthfacilityareawareofFP,ASRHpolicy,procedureandguidelines• StaffhavereceivedregularonjobtrainingonRH&FPasstipulatedinpoliciesandstrategies• Thereislowturnupatyouthcenter,whilereachingyouthattheirspacesisstillnewandneeds strengthening• AllFPmethodsareavailable,exceptcombinedinjectablecontraceptives• Thereareregularsupervisoryvisits,atleastonceamonth• IECmaterialsdisplayed,thoughnotawideselectiononFPmessages• Staffinterviewedagreedwiththeissuesidentifiedbythecommunity,includingwidespread misconceptions and myths on FP and youth inadequately accessing FP services
Priority issue for the health center is the shortage of staff, as articulated by the head of the facility. This hadanoveralleffectoncommunityoutreach,whichheidentifiedasakeychallenge.Thekeyrecom-mendationistostrengthenoutreachwithadditionalcommunityhealthworkers.
4.3.3 Key FGD findings
Focus group discussions were held in Kirimuruzi and Murambi Sectors in Gatsibo District and sought togainanin-depthunderstandingof:FPawarenessandattitude;Availabilityandaccess;andmaincauses of FP unmet need.
a) FP awareness and attitude: Though there has been an increase in FP awareness and service uptakeinthepastfewyears,therestillexistshighprevalenceofmisperceptions,mythsand rumors about FP methods and their side effects. Also prevalent is the perception of FP as a sourceofconflictwhenhusbandssireoutsidethefamily,despitewifelimitingbirths.
b) FP availability and access: FP services are readily available in Government health facilities, thoughthereislackofover-the-countercontraceptivesatprivatepharmacies,exceptfor condoms.
c) Causes of FP unmet need:Severalcausesofunmetneedwereidentified.Theseincludea gap in SRH information at different levels, especially in families and among the youth. The youthavoidapproachingCHWswhoareoftentheireldersandknowntothem.Another cause was widespread misconceptions and myths about the effects of FP.
d) Community recommendations to address above challenges include the following:

20
Family Planning in Rwanda
4.2 Conclusions from Policy Analysis
The FP Policy 2012 and the attendant policies have anticipated needs to ensure effective provision of FPservicesnationallyundertheexistingpoliticalwillandGovernmentcommitment.Theonlymajorchallenge appears to be the eventual inability to meet the costs as the demand increases. This results to a call for support from international partners. The target group in the FP policy 2012 is principally womenofreproductiveage(15–49years)andmen(15–59years).
4.3 District Analysis: Gatsibo
Gatsibo district serves as a case study to understand the perceptions of community members and services offered at the grassroots level.
4.3.1 District Profile
The status of RH and FP indicators in Gatsibo District for the most part closely mirrors the national level.HIVprevalencestandsat1.7percent,below thenationalaverageof3percent.36percentofpregnantwomengoforAntenatalCarecomparedto23.9percentnationalaverage.Totalfertilityrateisat4.9childrenperwoman,slightlyabovenationalaverageof4.6percent.
49.7percentofwomenbetweentheagesof15-49areusingmodernfamilyplanningcontraceptives,abovethenationalaverage45.1percent.Maternalmortalityrateper1000livebirthsis350/100,000comparedto487/100,000nationalaverage.Infantmortalityrateper1000livebirthsisat50/1000,simi-lartothenationalaverage.Childrenunder5yearsmortalityrateisat113/1000,belownationalaverage103/1000.Childrenfullyimmunizedstandsat94.8,abovenationalaverageof85.4%.Percentageof-womendeliveryinahealthfacilityisat63.9,belowthenationalaverage69.0%.
Gatsibodistrict isexperiencing rapidpopulationgrowthwhich is threatening tocurtailprogressonRHandFP indicators. ItsPopulationstoodat433,997ins2012.Thepopulation increasedby53.1percentbetween2002and2012.TheDistrictcurrentlyhasapopulationdensityof275personspersquarekilometer.Malesrepresent48percentofthepopulationandfemales52percent.Moreover,healthfacilitiesarenotequitablydistributedintheDistrict.Patientsoftenwalkover5kmtogettoahealthcenter,postorhospitaldiminishingaccesstohealthservices.Gatsibohas19healthcentres,adistrict pharmacy and 2 district hospitals at Kiziguro and Ngaram. There are 2,412 community health workersin11healthposts,witheachadministrativevillagehaving4CHWs.AccordingtotheDistrictdevelopmentPlan2013-2018“mostofthehealthcentersareinaverybadstateandurgentlyrequirerehabilitationorexpansion.”Availablelaboratoriesareinadequateinnumberandoftenlackthenec-essaryequipment.Thereisalsoanacuteshortageofhealthpersonnel-“insufficientbothintermsofquality(skills)andquantity.” Inadditiononly58.4percentof thepopulation iscoveredundercom-munity based health insurance.

23
A Review of National and District Policies and Budgets
US Dollars. Between 2006 and 2008 Rwanda received FP assistance amounting 3 million US Dollars – one million US Dollars for each year during the period. That family planning has received no support since2009clearlypointstoanadvocacyissue.
Table 1: OECD Development Assistance Disbursements
Official OECD Development Assistance (Disbursements) (Millions USD)
2005 2006 2007 2008 2009 2010 2011
Total 135 170 204 304 288 415 464
Health 11 15 16 31 24 17 34
Family 0 1 1 1 0 0 0PlanningRH/Population 4 8 7 11 18 6 4assistance
Reproductive 0 0 .. 0 0 0 0healthcare
STD&HIV/Aids 4 6 6 9 17 5 4
Source: Euroleverage, 2013
Health Disbursements (Millions USD)
2005 2006 2007 2008 2009 2010 2011
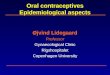
Europetotal 11 15 16 31 24 17 34
Belgium 6 9 11 18 16 2 21
France 1 .. .. 0 0 0 0
Germany 2 3 2 1 1 6 6
Ireland 0 0 1 0 0 0
Luxembourg 0 0 0 0 0 3 3
Spain 0 1 1 1 1 1 0
UnitedKingdom 1 0 0 10 5 4 3
EUInstitutions 1 1 1 1 0 1 0
Total 11 15 16 31 24 17 34
Source: Euroleverage, 2013
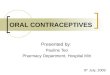
Table2belowshowshealthdisbursementsfor15countriesintheOECDandEUinstitutionscombinedfortheperiod2005to2011.Belgiumwastoalargeextentthehighestcontributor,followedbyUnitedKingdomandGermanyinthatorder(seeFigure1).Francecontributedin2005,andIrelandin2007.6ofthecountriesshownocontributionduringperiod2005to2011.
Table 2: OECD Health Disbursements

22
Family Planning in Rwanda
• Approachtheyouthintheirorganizedspaces,andemploypeerCHWs/counselors.The government should organize meetings and conversations, activities with the youth encouraging them to participate.• NGOstocollaboratewithGovernmentonsensitization,andinyouthemploymentaspoverty wasoneofthecausesofearlysex;advocacyonissuesontheground• InvolvechurchleadersandpastorsmoreindisseminatingFPmessages• Collaborationbetweendifferentstakeholders,includingdevelopmentpartners,Government and local authorities on provision FP services• LocalauthoritiesandCHWstoidentifyspecificcasesatvillagelevelthathavemanychildren butdon’tuseFP,ordon’tparticipateatcommunitymeetings,andengagethemindividually. Thereshouldbeincreaseduseexistingspaces,includingmonthlycommunitymeetingsto encourage and engage with men and women• Governmenttoinvestonfightagainstdrugabuseasitleadstoirresponsiblebehavioramong the youth. • Putmoreeffortintalkinganddiscussingissueswithchildren,parentsalsotobetrainedtotalk to their children
4.3.4 Policy Responses to Unmet need issues Identified by Communities
TheFPissuesidentifiedbythecommunitiesarereflectedintheFPPolicy2012andfoundresonancewith thekey informants, including theHeadof theGakenkeHealthFacility,GatsiboDistrictHealthOfficerandsub-districthealthsupervisor.ThissuggeststhattheDistrictandGovernmentareawareof the challenges and has anticipated how to address them as articulated in the FP Policy 2012. Com-munity recommendations are also implicit in the government plan to address the challenges nationally. Despitetheaboveconcernofdistrictprioritiesappearingtobeoverlookedbythegovernmentanddevelopment partners, not to mention the seeming decline in FP budget share nationally, there have been adequate FP supplies. However, the district has anticipated an increase in community mobiliza-tionwithconsequentdoublingofFPbudgetallocationsofRwf12,615,000forFY2014/2015fromthecurrentRwf.6,415,000forFY2013/2014.Itistothisthedistrictmustbeheldtoaccount.
4.4 Budget Analysis
4.4.1 Overall National Budget Trends
4.4.1.1 OECD Support
Between 2005 and 2011official development assistance toRwanda fromcountries under theOr-ganisationforEconomicCo-operationandDevelopment(OECD)amountedto1.98billionUSDollars(seeTable1).ThecountryhasreceivednodevelopmentassistanceforFamilyPlanningfrom2009todate,whichisreflectedinthenationalbudgetsunderthefinancialyearsunderreview.Totalamountdisbursedforhealthduringtheperiodwas148millionUSDollars,representing7.4%ofthetotalOECDsupport(Table1).“ReproductivehealthandPopulationAssistance”received58millionUSDollars,withreproductivehealthcarereceivingnosupport.“STDcontrolincludingHIV/Aids”received51million

25
A Review of National and District Policies and Budgets
0
5
10
2010/11 2011/12 2012/13 2013/14 2014/15
15
20
25
30
Billions
% share
Column 1
Table 4: Inflation rate 2009/10 – 2013/14
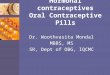
Figure 2: Real growth and percentage share in 2010/2011 - 2013/2014
Source: Ministry of Finance
Year 2009/2010 2010/2011 2011/2012 2012/2013 2013/2014
Inflation 2.3 5.7 6.3 3.5
Deflator 1 3.3 9 15.3 18.8
4.4.2 National Family Planning Budget (FY 2009/10 -FY 2013/14)
Notably, the national family planning expenditure and disbursements coincided during the period2009/10–2013/14,andthatFPinterventionswerecateredforundertheGovernmentrecurrentexpen-diture for the same period.
Inaddition, theFPbudget for financial year2010/2011 rose in real termsbyawhopping1,026%,withadramaticfallto2.2%inthefinancialyear2011/2012.Financialyears2012/13and2013/14sawnegative growths.
Table 5: Family planning budget 2009/10 – 2013/14
Source: Ministry of Finance
Year 2009/2010 2010/2011 2011/2012 2012/2013 2013/2014
FP 12,155,265 424,000,000 510,000,000 506,066,041 483,643,111(,000Rwf)
Nominal 411,844,735 86,000,000 -3,933,959 -22,422,930
3,388% 20.2% -0.77% -4.4%
Real 124,801,434 9,555,555 -257,121 -1,192,709
1,026% 2.2% -0.05 -0.23

24
Family Planning in Rwanda
Figure 1: OECD Health Disbursements
4.4.1.2 National Budget Trends
Therewasageneral increase in thenationalbudgeteachfinancial year from2009/10 to2013/14.Financialyear2012/2013showedthemostdramaticincreasewithanominalgrowthofover38%(seeTable3).Adjustedforinflation,however,therewasasignificantdecreaseinrealgrowth(seeTable4forinflationratesduringtheperiod).ItisnotablethatthoughRwandasufferedaidfreezefromEurope-andonorsduetoitspurportedmeddlingintheconflictineasternDemocraticRepublicofCongo,thebudgetgrewbyover13%inFY2011/2012and38%inFY2012/2013.Theaidfreeze,however,doubledinflationin2011/2012,andsawanincreaseduring2012/2013(seeTable4).Thishadaneffectontherealbudgetarygrowthinboththefinancialyearsasindicatedbelow.
Table 3: Overall total budget trends from 2009/10-2013/14
Health Disbursements (Millions USD)
Year 2009/2010 2010/2011 2011/2012 2012/2013 2013/2014
TotalBudget 898,962,483 984,022,047 1,116,851,388 1,549,859,475 1,653,467,462
(,000 $142percapita $155percapita $176percapita $245percapita $261percapita
Rwf)
Nominal 85,059,563 132,829,340 433,008,087 103,607,986,699
9.46% 13.5% 38.7% 6.68%
Real 25,775,635 14,758,815 28,301,182 5,511,063
2.86% 1.5% 2.53% 0.35%
Source: Ministry of Finance
0
5
10
Belgium France Germany Ireland Luxembourg Spain UK EUInstitutions
15
20
25
2005
2006
2007
2008
2009
2010
2011

27
A Review of National and District Policies and Budgets
4.5 District Budget Analysis
4.5.1 FP budget in Gatsibo District
Therewasno indicationof familyplanningbudget inFY2012/2013.Familyplanningactivitiesweresubsumed under the Health component under the Human Development and Social Sectors in the dis-trict’sEDPRSPriorities.However,familyplanninginGasiboDistrictwascategorizedunder“DiseaseControl”withabudgetofRwf.6,415,000,forthefinancialyear2013/2014.Communitymobilizationwas the main activity under the budget allocation. The reason for this is that FP consumables and equipment in all the districts are procured directly from the government. There is a projected increase inthenextfinancialyear(2014/2015)ofnearlydoublethisfinancialyear’satRwf12,615,000.Projec-tionsfor2015/2016aretripleatRwf18,815,000.
4.5.2 Family planning users experience and opinion on budgeting process
Thebudgeting process has been inclusive of all the stakeholders, from the grassroots communi-ties,community-basedorganizationsandlocalauthorities.Oneactivedevelopmentpartnerwascited,while others have lapsed over time.
Worthnotingwasanobservationbythekeyinformantsthatdespiteallbroad-basedstakeholderin-volvementinthebudgetingprocess,identifiedprioritiesatthedistrictleveltendedtobeoverlookedasanysupportfromthegovernmentordevelopmentpartnerswasthrough“anenvelope”,suggestingpre-determinedallocationsaccordingtotheavailabilityoffundsfromthegovernmentordevelopmentpartners.
4.6 Conclusions from Budget Analysis
There was a general increase in the national per capita health allocation from $12 during the FY 2010/2011to$20inFY2013/2014,reflectingtheincreaseinthenationalbudgeteachfinancialyearduring the same period. This however falls far short of the WHO recommended $44 per capita. On the otherhandbudgetallocationsforFPstagnatedataround0.5%ofthetotalMoHbudget.Theamountisminimalandcallsforanincreaseifthecontraceptiveuptakeistoreachtheprojected70%by2017.ItisnotablethatsolelythegovernmentasindicatedinthenationalbudgethasfinancedFP,withnosupportfrominternationalpartners.TheapparentlackofdonorsupportforFPinthebudgetdoesnotpreclude as support development partners may have provided in FP outside Government, which calls for further research. It nevertheless creates room to advocate for international partners to offer more budgetarysupportinFP,especiallyinanticipatedincreaseofupto70percentuptakeinFPservices.
Thoughthebudgetingprocesshasbeeninclusiveofallthestakeholdersatthedistrictlevel,boththegovernment and development partners should pay more heed to district priorities as collectively identi-fiedandnotmerelyofferan“envelope”.

26
Family Planning in Rwanda
RHandFPcategorizationsdidnotcoincideduringtheperiod(seeTable6).Duringthefinancialyear2009/2010 theywerecategorizedseparatelyas familyplanningand reproductivehealth. Between2010/2011and2012/2013theyweremergedandcategorized“ReinforcementofFamilyPlanningandReproductiveHealth”.Duringthefinancialyear2013/2014FPandRHwereincorporatedasonebud-getlineunder“MaternalandChildHealth”(Table7).ThisimpliesthatfamilyplanningreceivedgreatlyreducedshareduringFY2013/14.Generally,however,percapitaallocationintheoverallMoHbudgetfalls short of the WHO recommendation of $44.
Table 6: Family Planning Budget allocation by thematic areas (2009/10 – 2012/13)
Year 2009/2010 2010/2011 2011/2012 2012/2013
Total MOH 76,694,936,826 109,523,533,680 140,150,512,572Budget $12 per capita $17 per capita $22 per capita
Forcement of 1,246,300,000 3,404,847,550 2,994,194,752Family Planningand Reproductive Health
Family Planning 12,155,265 424,000,000 510,000,000 506,066,041 0.55%ofMoH 0.46%ofMoH 0.36%ofMoH budget budget budget Reproductive 12,155,265 822,300,000 2,894,847,550 2,488,128,711Health
Table7: Family Planning Budget allocation by thematic area (2013/14)
2013/2014
Total MOH Budget 127,642,972,458
$20 per capita
Maternal And Child Health 6,863,453,373
Family Planning And 483,643,111
Reproductive Health 0.38% of MoH budget
Maternal And Child 3,463,813,923
Health Improvement

29
A Review of National and District Policies and Budgets
Despite theCPRofmore45%andanoveralldecreaseof1.5childrenperwomancurrently,muchremainstobedone.UnmetFPneedstandsat19%,whilethecurrentmethodmixdoesnotappeartoaddresswomen’swiderangeoffertilitypreferences.Asthisstudyobserves,long-actingandperma-nentmethodsareprobablymostappropriate,whileover-relianceonshort-actingmethodsgenerallypresents higher rates of discontinuation. This potentially results in more unintended pregnancies. It is, however,notedthatinasettingwherethedemandishighandunmetneedsignificantitcallsforfur-therexamination.Thisunderscorestheneedfortechnical,inadditiontoincreasedfinancial,support.ItislikewiseclearthatmythsandmisperceptionsaboutFPanditseffects,alongwithsocio-culturalandreligiousinfluencesaffectFPservicedemandatthecommunitylevel.Themisperceptionisalsoapparentinthe“stigmatization”,demonstratedintheGatsiboDistrictBudgetthatitshouldfallunder“DiseaseControl.”ThisonlyservestosidelineFPasakeyissueintheDistrict.
5.1 Recommendations
Theforegoinganalysisandaccordingtothepriorityissuesidentifiedbythecommunities,werecom-mend three interrelated issues for advocacy, both at the district and nationally. That the Government andinternationalpartnersallocateadequateresources,bothfinancialandhumanto
• Fightmisperceptions,mythsandrumorsaboutFPmethodsandtheirsideeffects, includingimprovementofmethodmixes,throughthemediaandatthecommunitylevel through CHWs;• ReachandinvolvetheyouthinrelevantRH&FPprogrammes• LobbythegovernmenttoincreaseFPbudget,andtheinternationalcommunitytobegin offeringFPbudgetarysupportbystartofnextfinancialyear,2014/2015.
Youth inclusionandfightingmisperceptionswere identifiedbythecommunitiesastheirkey issuesofconcern,andhaveabearingoncommunityoutreach.Strongadvocacyefforts’targetingtheinter-national partners to allocate funds for FP services is paramount to build for wider and more effective community outreach as above articulated.

28
Family Planning in Rwanda
GatsiboDistrictreflectsnationaltrends,ofwhichRwandahasmadecommendableprogressinfamilyplanning.Notonlydidmoderncontraceptiveprevalenceratequadruple from10%in2005tomorethan45%in2010,but total fertilityratedecreasedfrom6.1childrenperwomanto4.6 inthesameperiod. While the Government aims to increase CPR to 70% by 2017, supply of contraceptives has continued to meet the demand. However, there is concern that with the increase the Government may not be able to sustain the demand with the anticipated increase in cost of providing FP services. This studyfindsthatRwandareceivednointernationalsupportforFPbeginning2009todate.Thislaysthefoundation for FP funding from international partners. International development partners therefore should be lobbied to offer their support in anticipation of any shortfall, especially in ensuring that strate-giestoaddressFPchallengescometofruition(see4.1.2.2).
5. Conclusions


30
Family Planning in Rwanda
6. References
• AnnualReport,MinistryofHealth(2012)
• EconomicDevelopmentandPovertyReductionStrategy2013–2018(EDPRSII)
• FamilyPlanningPolicy(2012)
• Gatsibo District Budget 2012 – 2013
• Gatsibo District Budget 2013 – 2014
• GatsiboDistrictDevelopmentPlan(2013-2018)
• MappingfundingforReproductiveHealthinRwanda,EuropeanOfficialDevelop-
mentAssistance,Euroleverage,2013
• MINECOFINAnnualBudgetExecutionReport2009-2010
• MINECOFINAnnualBudgetExecutionReport2010-2011
• MINECOFINAnnualBudgetExecutionReport2011-2012
• MINECOFINInflationRates1990-2013
• MINECOFINRevisedBudgetAnnexes2009-2010
• MINECOFINRevisedBudgetAnnexes2010-2011
• MINECOFINRevisedBudgetAnnexes2011-2012
• MINECOFINRevisedBudgetAnnexes2012-2013
• MINECOFINRevisedBudgetAnnexes2013-2014
• NationalHealthPolicy(2004)
• NationalPopulationPolicyforSustainableDevelopment(2003)
• NationalReproductiveHealthPolicy(2003)
• RwandaDemographicHealthSurvey(2010)
• RwandaInterimDemographicHealthSurvey(RIDHS),2007/2008
• Vision2020

RWANDA WOMEN’S NETWORKKinyinyaSector,Gacuriro(nexttoSOSTechnicalSchool)KG 428 StreetP.OBox3157,Kigali,RWANDATel:+250788334257Email:[email protected]/[email protected]:www.rwandawomennetwork.org
and
DSW (Deutsche Stiftung Weltbevoelkerung)HatheruRoad,HatheruCourt(Lavington)P.OBox2438-00202Nairobi,KenyaTel:+254202731398/203592302Mobile:+254726603768/736616491Email:[email protected]:www.dsw-online.org