Embed Size (px)
Citation preview

FAMILY PLANNING Action Plan for
2011-12Date: 20th April 2011
Presented by:Dr. P.N. Bora
State Programme ManagerNRHM, Assam

Indicator Assam India
MMR480
(Source 2004-06, RGI)
333
(Source 2009, CES, RRC-NE)
254(Source
2004-06, RGI)
IMR
61 (Source SRS, RGI, January
2011)
46
(Source 2009, CES, RRC-NE)
53 (Source SRS, RGI, October
2009)
TFR2.6
(Source RGI, 2009)
2.6(Source RGI,
2009)

Sl. No.
DistrictTotal unmet need
(%)For spacing (%) For limiting (%)
1 Barpeta 23.7 6.3 17.42 Baska 20.9 4.2 16.7
3 Bongaigaon 36.8 6.7 30.1
4 Cachar 23.7 5.4 18.35 Chirang 27.4 7.5 19.96 Darrang 15.6 5.2 10.47 Dhemaji 20.5 6.3 22.38 Dhubri 37.2 10.1 27.1
9 Dibrugarh 32.0 7.4 24.6
10 Goalpara 20.5 5.8 14.711 Golaghat 47.0 8.6 38.4
12 Hailakandi 21.4 5.6 15.8
13 Jorhat 22.7 5.9 16.8
14 Kamrup Metro 30.9 6.5 24.4

Sl. No.
DistrictTotal unmet need
(%)For spacing (%) For limiting (%)
15 Kamrup Rural 23.3 4.5 18.8
16 Karbi Anglong 16.2 2.6 13.6
17 Karimganj 26.3 6.6 19.7
18 Kokrajhar 32.8 8.5 24.3
19 Lakhimpur 36.6 9.2 27.4
20 Morigaon 34.4 9.2 25.221 N.C.Hills 23.3 4.2 19.122 Nagaon 21.5 5.7 15.823 Nalbari 21.2 6.4 14.824 Sivsagar 30.0 5.2 24.825 Sonitpur 32.1 7.1 25.026 Tinsukia 30.5 8.0 22.527 Udalguri 14.5 3.9 10.6
Assam 24.3 5.8 18.5

District wise Population & Decadal Growth Rate
Sl. No.
DistrictPopulation
(as per 2001)Population
(as per 2011)
Decadal Growth
Rate (1991-01)
Decadal Growth Rate
(2001-11)
Increase in Poplulation
1 Dhubri 15,66,396 19,48,632 23.40 24.40% 3,82,236
2 Morigaon 7,76,256 9,57,853 21.30 23.39% 1,81,597
3 Goalpara 8,22,035 10,08,959 23.10 22.74% 1,86,924
4 Nagaon 23,14,629 28,26,006 22.30 22.09% 5,11,377
5 Hailakandi 5,42,872 6,59,260 20.90 21.44% 1,16,388
6 Barpeta 13,94,755 16,93,190 18.50 21.40% 2,98,435
7 Karimganj 10,07,976 12,17,002 21.40 20.74% 2,09,026
8 Dhemaji 5,71,944 6,88,077 18.90 20.30% 1,16,133
9 Cachar 14,44,921 17,36,319 18.70 20.17% 2,91,398
10 Bongaigaon 6,12,665 7,32,639 12.20 19.58% 1,19,974
11 Darrang 7,59,858 9,08,090 15.80 19.51% 1,48,232
12 Kamrup ( M ) 10,59,578 12,60,419 25.80 18.95% 2,00,841
13 K-Anglong 8,13,311 9,65,280 22.60 18.69% 1,51,969

District wise Population & Decadal Growth Rate
Sl. No.
DistrictPopulation
(as per 2001)Population (as
per 2011)
Decadal Growth Rate
(1991-01)
Decadal Growth Rate
(2001-11)
Increase in Poplulation
14 Lakhimpur 8,89,010 10,40,644 18.30 17.06% 1,51,634
15 Kamrup (R) 13,11,698 15,17,202 25.80 15.67% 2,05,504
16 Sonitpur 16,65,125 19,25,975 17.80 15.67% 2,60,850
17 Tinsukia 11,50,062 13,16,948 19.50 14.51% 1,66,886
18 N.C.Hills 1,88,079 2,13,529 23.50 13.53% 25,450
19 Dibrugarh 11,85,072 13,27,748 12.40 12.04% 1,42,676
20 Golaghat 9,46,279 10,58,674 14.20 11.88% 1,12,395
21 Nalbari 6,89,053 7,69,919 12.00 11.74% 80,866
22 Chirang 4,33,061 4,81,818 12.20 11.26% 48,757
23 Baksa 8,57,947 9,53,773 12.00 11.17% 95,826
24 Udalguri 7,58,746 8,32,769 15.80 9.76% 74,023
25 Sivasagar 10,51,736 11,50,253 16.00 9.37% 98,517
26 Jorhat 9,99,221 10,91,295 15.80 9.21% 92,074
27 Kokrajhar 8,43,243 8,86,999 15.10 5.19% 43,756
Assam 1,29,68,332 1,45,67,546 18.90 12.33% 15,99,214

Population of 2011 : 13,27,748
EC (17% of Projected Population) : 225717
Unmet Need of Dibrugarh District: 32% of Eligible Couple = 72229
Unmet need for Limiting of Dibrugarh District: 24.6 % of Unmet Need of Population = 17768 i.e target of sterilization
Unmet need for Spacing of Dibrugarh District : 7.4 % of Unmet Need of Population = 5345 i.e target of IUCD
Hence ELA will be calculated as per resources.
Population of 2011 : 13,27,748
EC (17% of Projected Population) : 225717
Unmet Need of Dibrugarh District: 32% of Eligible Couple = 72229
Unmet need for Limiting of Dibrugarh District: 24.6 % of Unmet Need of Population = 17768 i.e target of sterilization
Unmet need for Spacing of Dibrugarh District : 7.4 % of Unmet Need of Population = 5345 i.e target of IUCD
Hence ELA will be calculated as per resources.

District level Quality Assurance Committee (FP) chaired by DC /Principal Secretary to be made functional
Doctors trained in Laparoscopic Sterilization / Mini lap / PPS / NSV are to be empanelled by Jt. DHS after getting certificate from the DQAC in order to get benefit of Insurance scheme.
To ensure uninterrupted supply of Nirodh / Oral Pills / E-Pills up to the village levels.
Claim for FP Insurance Scheme is to be submitted within one week after the incidence.
Monthly updating of eligible couple register at SC level and thereby conducting FP Counseling to the couple who are not using any modern FP methods are to be ensured.
Contd….
Important Issues to be taken up by the districts

JSY Beneficiaries are to be motivated for PPS / Minilap in the FRU and district where trained Doctors are there.
To Prepare District Level Action Plan indicating fix strategy and camp approach for sterilization (male and female) with schedule (date, place and time).
To ensure fixed day LS / PPS / Mini Lap / NSV operation every week in district hospital, SDCH and FRUs. Every two months CHC/PHC
To ensure IUD insertion every week in all health institution and in the Sub center in Govt. building where trained GNMs/ANMs are there.
Regular Male & Female sterilization camps at Block PHC, CHC, FRU bimonthly.
Important Issues to be taken up by the districts

TE and other private hospitals are to be accredited for family planning service, Specially for PPP Tea Garden ANM/GNM are to be trained for IUCD insertion, and after training IUCD Kits are to be provided.
MO, GNM and ANM of Boat Clinic are to be trained for IUCD insertion and after completion of training IUCD insertion Kit is to be provided
Important Issues to be taken up by the districts

To raise awareness amongst the couples and communities about the advantage of contraceptives and small family.
Activities Communication messages through Print Media, electronic media working jointly by DEMO, Dy DEMO & DME.
Information board for Male and Female Sterilization indicating compensation for the acceptor and motivator are to be placed in every institution where NSV and Female sterilization are performed.
IPC by ASHA / ASHA Facilitator / ANM in VHND and also during Home visit and OPD at Sub Center.
In all District Hospital a separate room naming “TIPS of Happy Family” has to be established.
STRATEGY 1

To raise awareness amongst the couples and communities about the advantage of contraceptives and small family.
Activities Updating of eligible Couple Register at Sub Center level by ANM and ASHA during Home Visit on Monday, Thursday and VHND and motivating the couple to adopt FP methods and to attend Sub center on Tuesday and Friday for counseling.
Counseling of the EC who had not adopted FP methods is to be done on Tuesday and Friday at SC and thereby enlisting there names as per their choice of FP method viz., IUCD, Oral Pill, Permanent Method(LS, Minilap, PPS, NSV) etc. Enlisted names for a permanent method are to be submitted to i/c BPHC at the end of the month so that He/She can arrange camps. IUCD and Distribution of Oral Pill, E-Pill, Nirodh is to be done at SC level.
STRATEGY 1

To incorporate Family Planning in Ante Natal Clinic, Post Natal Clinic and MCP Session.
ActivitiesDuring ANC 3rd and 4th visit examination of the breast of the pregnant women will be made mandatory to exclude crack nipple and retracted nipple.
Motivation and counseling of the pregnant women during ANC and PNC to initiate breast feeding within half an hour after delivery and to continue exclusive breast feeding upto six months. This LAM method will prevent pregnancy for 5 months.
Counseling of the mother after delivery to adopt PPS within 48 hrs. of delivery.
STRATEGY 2

To Increase the number of service delivery points.
Activities
ASHA is acting as FP depot holder having wider basket of contraceptives (OCP, ECP, and Nirodh). Regular replenishing of the contraceptives are to be ensured by DCM, BPM, ABPM and ASHA Facilitator. DCM will monitor the activity.
Fixed day (Friday) IUD insertion will have to be provided in Civil Hospitals and CHC/ FRU / BPHC/ PHC and Sub Center. IUD Kit is to be provided after completion of training
Facilities and Training for insertion of IUCD and Contraceptive Distribution will be made available in the Boat Clinic/PPP T.E. during 2011-12.
STRATEGY 3

To Increase the number of service delivery points.
Activities
To confirm retention of Copper-T, all ANMs are directed to examine the thread of Copper-T after 3 months, 6 months and 12 months. ASHA will bring the beneficiaries to the institution where Copper-T was inserted and not to the other institution for which ASHA will get the incentive.
MTP followed by IUD insertion will be ensured in all Health Institutions except sub center.
STRATEGY 3

Improve the service delivery to provide quality Family planning services by capacity building.
Activities• Minilap (PPS) will be conducted in all DHs/ SDCHs/ CHCs/
FRUs. It is expected that at least 5% of pregnant women coming for institutional delivery and availing JSY benefit will be motivated for Post partum sterilization.
• Fixed day FP service (LS/ Mini Lap / PPS / NSV / IUD insertion / Contraceptives) on Tuesday in all DH, SDCH, FRU and CHC where trained service provider are there. On that day, FP sterilization will get priority than other operation except emergency cases. Information board will be displayed regarding these activities in all BPHCs so that FP acceptors can be sent to the fixed day sterilization.
STRATEGY 4

• Fixed day FP service (LS/ Mini Lap / PPS / NSV / IUD insertion / distribution of condom / EC pill) on Thursday in 5 identified centers where service provider are not there. Service providers will be mobilized from DH or from other Institutions where available.
• District Administration (ADC- Health) will organize one special Family Planning Camp for 3 days, preferably in the CHC for performing FP sterilization (LS/ Mini Lap / PPS / NSV / IUD insertion / distribution of condom / EC pill) monthly. Extensive publicity to be given 15 days prior to the camp involving all Block level healthcare provider including ASHA, ASHA Facilitator, DFPC and DCM.
STRATEGY 4

Camp ApproachActivities:
– Block PHC and CHC where fixed day sterilization services are not possible will organise LS or NSV Camp once in two months. The enlisted beneficiaries at the SC are to be collected by i/c, BPHC every month.
STRATEGY 5

To Improve NSV ProgrammeActivities:
- Extensive Media Coverage of the sensitization meeting and NSV / other service camps
– By Changing the attitude of the officials
– Try to bridge the gap between the officials and common people.
– Starting of Intensive Training Programme • Doctors from Medical Colleges • M.O.s from District Hospital and PHCs.• Awarded Certificate for District Trainers and State
service provider
STRATEGY 6

Public Awareness Meetings on Population Explosion.
•Involvement of religious leaders and community leaders.
•Involving the women
•Involving public representatives
•Involvement of Media personals
•Involvement of local NGOs
•Involvement of Opinion leaders
STRATEGY 6

Agenda for Public Awareness Meetings.
–Deleterious impact of Population Explosion.
–Religious views regarding conservation of nature and ecology.
–Education, Particularly women education.
–Empowerment of the women.
Contd…
STRATEGY 6

Agenda for Public Awareness Meetings.
– Childhood marriage
– Multiple marriage
– Breast feeding for birth spacing (LAM method).
– Religious views for Family Planning, particularly Islamic views.
– Family Planning in Islamic Countries.
STRATEGY 6

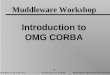
Comparative performance of NSV

Comparative performance of NSV

Comparative performance of NSV
DISTRICT Difference
Nagaon -1207
Barpeta -600
Udalguri -524
Cachar -519
Sonitpur -480
Darrang -260
Lakhimpur -231
Dhemaji -226
Tinsukia -156
Karimganj -145
Kamrup(R) -140
Nalbari -100
Sivasagar -75
Morigaon -69
Kokrajhar -60
Bongaigaon -55
Dhubri -43

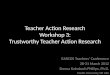
Comparative performance of NSV
Kamrup (M) 2843
Dibrugarh 289
Baska 179
Hailakandi 155
Jorhat 136
Golaghat 58
K-Anglong 56
Goalpara 31
Chirang 9
N.CHills 0

Village Level
–ASHA , ASHA Facilitator, AWW, ANM will conduct Family Planning Counseling to the eligible couples after updating the issue register in the VHND and also at the Subcenter at Tuesday and Friday.
–The updating of Eligible Couple is to be done during Home Visit by ANM along with ASHA on Monday and Thursday and also in VHND.
–IEC / BCC Materials are to be made available for ASHA, AWW and ANM.
–ASHA will act as a depot holder for Condom, Oral Pill and E-Pill. Regular replenishment of the contraceptives on exhaustion is to be ensured by ASHA Facilitator, DCM and Pharmacists of the Block.
ACTIVITES TO BE PERFORMED AT THE DIFFERENT LEVELS

Counseling and motivation of the eligible couples who had not adopted any FP methods, identified during updating of EC register is to be done on Tuesday and Friday. Enlisting of Eligible Couple as per their chosen method is to be done and list is to be sent to BPHC for organising camp for LS and NSV. Copper-T, Oral Pill, Condom, E-Pill are to be distributed in the SC itself.
JSY Beneficiaries are to be motivated for accepting Post Partum Sterilization (Mini Lap) and refer the acceptor to FRU/CHC/SDCH/DH where PPS can be done.
Sub Center Level

During Health Day disadvantages of early marriage (too early, too many and too frequently) are to be explained especially to adolescent girls with the help of opinion and religious leaders of the village.
On Tuesday and Friday of every week Family planning services including IUD Insertion (after training) are to be provided in the Sub Center itself.
All contraceptives (Condoms, Oral Pills, E-Pills) are to be made available throughout the year.
Sub Center Level

Fixed day for family planning counseling along with Ante Natal and Post Natal check up is to be ensured.
JSY Beneficiaries are to be motivated for accepting Post Partum Sterilization and refer the acceptor to FRU/CHC/SDCH/DH where PPS can be done.
All contraceptives (Condoms, Oral Pills, E-Pills) are to be made available throughout the year.
A day is to be fixed for IUD insertion.
All GNM and ANM will have to be trained in alternate methodology of Copper-T 380A
Doctors trained in MTP will perform safe abortion using MVA/EVA
IEC materials for NSV is to be distributed among the male member of the eligible couples
One NSV workshop cum training for MO is to be organised registering at least 20 acceptors (State Level Trainers is to be invited).
24 X 7 PHC Level Excluding BPHC

The list of ANM trained for IUD insertion are to be prepared and target is to be given after calculating ELA of a particular Sub Center. The ANM working in the Sub Center having Govt. Building are to be selected for IUCD Training.
Method and Technique of Counseling are to be taught to the ANM in the PHC level Review meeting engaging DME, DFPC and Medical Officers.
The list of Beneficiaries for LS and NSV are to be collected every month from Sub Centers.
Camps for LS and NSV are to be organised at the interval of 2 months. If facilities for LS camp is not available in the BPHC, the CHC under the Block is to be selected for LS Camp. Extensive IEC is to be done 15 days prior to the camp. Beneficiaries listed in the Sub Center are to be visited by ANM, ASHA, ASHA Facilitator to motivate for Sterilization and also to inform the date of sterilization camp.
Block PHC Level

Fixed day static- One day in a week is to be fixed for Family Planning activity in the BPHC for IUD insertion and distribution of contraceptives (Condoms, Oral Pills, E-Pills).
To confirm retention of Copper-T, all ANMs are directed to examine the thread of Copper-T after 3 months, 6 months and 12 months. ASHA will bring the beneficiaries to the institution where Copper-T was inserted and not to the other institution for which ASHA will get the incentive.
Record Keeping:
Block PHC Level
The Reporting Format (Next Slide) is to be submitted along with HMIS report . To fill up this format separate registers for Male and Female Sterilization, IUD with the columns as indicated in the reporting format are to be maintained strictly.

Supervision and Monitoring: All ANM in the Sub Center must complete updating of eligible couple register and listing of beneficiaries monthly. This process is to be regularly monitored by BEE, Health Educator, LHV, BPM, ABPM.
Follow up of FP Beneficiaries is mandatory. The responsibility is to be fixed to the ANM of the Sub center. She will have to visit all the FP Beneficiaries of her area on Thursday. This activity is to be supervised by LHV, Health Educator, BPM, ABPM and BEE. Failure cases, cases with complication after sterilization and death cases are to be enlisted and reported immediately so that benefit of insurance scheme can be provided in stipulated time.
VHND is the best platform for IPC and counseling of eligible couple. DCM, DME, BPM, ABPM, BEE, Health Educator will monitor and guide ANM how to perform IPC and Counseling to the Eligible Couple by visiting VHND regularly
Block PHC Level

Reporting of FP Activities from April 2011 as per following format
Total death reported after
the Sterilization
Total Conception/Failure after sterilization
Death/Failure Audit and Action taken , if any
BPHCduring
the Month
Cumulative for
the Year
during the
Month
Cumulative for the Year
REPORT ON No. of Camps (Male and Female Sterilization)YEAR:Month:
Sl BPHCNSV Camps during the
Month
Total Cumulative for
the Year
Female Sterilization
Camps during the Month
Total Cumulative for
the Year
1 2 3 4 5 6
FAILURE & DEATHS AFTER STERILISATIONYEAR:Month:

Reporting of FP Activities from April 2011 as per following format
Family Planning Reporting
1
No. of NSV conductedDuring the
reporting monthCumulative since
April
At fixed day static
No. of acceptors with 1-2 children
No. of acceptors with 3 children
No. of acceptors with 4 or more children
Total
At NSV Camp
No. of acceptors with 1-2 children
No. of acceptors with 3 children
No. of acceptors with 4 or more children
Total

Reporting of FP Activities from April 2011 as per following format
2
No. of Female Sterilization (Lap. Sterilization)During the reporting
monthCumulative since April
At fixed day staticNo. of acceptors with 1-2 children No. of acceptors with 3 children
No. of acceptors with 4 or more children
Total At LS Camp
No. of acceptors with 1-2 children No. of acceptors with 3 children
No. of acceptors with 4 or more children
Total
No. of Female Sterilization (PPS)During the reporting
monthCumulative since April
At fixed day staticNo. of acceptors with 1-2 children No. of acceptors with 3 children
No. of acceptors with 4 or more children
Total
No. of Female Sterilization (Minilap)During the reporting
monthCumulative since April
At fixed day static
No. of acceptors with 1-2 children

Reporting of FP Activities from April 2011 as per following format
No. of acceptors with 3 children
No. of acceptors with 4 or more children
Total
3
No. of IUCD (Copper-T) Acceptors During the
reporting monthCumulative since April
No. of acceptors with 1 children
No. of acceptors with 2 children
No. of acceptors with 3 children
Total No. of non retention of Copper-T in Acceptors confirmed after examination of thread
During the reporting month
Cumulative since April
After 3 months After 6 Months
After 1 Year
During the
reporting monthCumulative since April
4 Oral Pill User 5 C.C. User

Fixed day for family planning counseling along with Ante Natal and Post Natal check up is to be ensured.
JSY Beneficiaries are to be motivated for accepting Post Partum Sterilization.
All contraceptives (Condoms, Oral Pills, E-Pills) are to be made available throughout the year.
A day is to be fixed for IUD insertion.
Fixed day female sterilization (LS and PPS) is to be observed strictly
Doctors trained in MTP will perform safe abortion upto using MVA/EVA
IEC materials for NSV is to be distributed among the male member of the eligible couples
One NSV workshop cum training for MO is to be organised registering at least 20 acceptors (State Level Trainers is to be invited).
MO-MBBS are to be trained for conducting mini lap (PPS)
FRU/CHC Level

– One separate room is to be allotted in the outdoor
complex for family planning services where a sign board
mentioning “Tips for Happy family” should be placed in
front of the room. In that room family planning services
are to be rendered including distribution of contraceptives.
One staff nurse is to be engaged in that room during the
OPD hours (8:30 AM – 1:30 PM) in working days and
(8:30 AM to 12:00 PM) in Sundays and Holidays.
Contd..
District Hospital/ SDCH Level

Fixed day for family planning counseling along with Ante Natal and Post Natal check up is to be ensured.– JSY Beneficiaries are to be motivated for accepting Post
Partum Sterilization. – A day is to be fixed for IUD insertion. – Fixed day (once a week) female sterilization (LS , PPS
and NSV) is to be observed strictly– Doctors trained in MTP will perform safe abortion upto
using MVA/EVA– IEC materials for NSV is to be distributed among the
male member of the eligible couples – MO-MBBS are to be trained for conducting mini lap
(PPS)
District Hospital/ SDCH Level

Uninterrupted supply of contraceptives upto the Village level- As the district Stores for FP materials is maintained separately by storekeeper, Addl. CM&HO(FW) will have to utilize the service of District Drug Store Manager and Pharmacist in the BPHCs.
Wide Publicity of the new compensation package (mentioned below) is to be given in the entire district. An information board is to be hanged in each Health Institution where Male and Female Sterilization is done indicating compensation of acceptors and motivators. DME, DEMO or Dy. DEMO will design the board and will identify the Health Institution of the district.
Sensitization meeting for population explosion with special preference to male participation is to be organised in the remote areas where acceptance of FP methods are less. District Family Planning Bureau have to take the initiative.
Contd…
District Level

All guidelines are to be made available to all the institutions upto 24 X 7 PHC level. Important Guidelines like Standards for Female and Male sterilization Services (Oct. 2006), Manual for Family Planning Insurance Scheme (Jan 2008) and MTP Rules.
Compensation Money are to be made available in the institutions, where LS, PPS and IUD insertion are conducted. 50% of the camp money is to be released to the Block PHC at least 15 days ahead of the camp for preparation of Camp. MO, i/c PHC must ensure participation of required no. of acceptors as schedule.
Regular Monitoring by district and Block Monitoring Team are to be ensured.
Contd…
District Level

To provide training load of LS / Mini Lap / MTP / IUD insertion.
One day district workshop is to be organized by the District Family Welfare officials involving DC, Joint DHS, President- Zila Parishad (PRI), Opinion leaders, MNGO, CDPO, Mahila Samitee, to sensitize them on the role of male participation and promotion of NSV.
An implementation team for NSV will have to be constituted with DC, Joint DHS, Addl. CM&HO, DEMO/ Deputy DEMO, District NSV trainer.
Tea Garden Hospitals and Pvt. Hospitals where facilities are available are to be accredited for family planning services
District Level

Procedure of calculating equivalent sterilizationAgainst Condom user and Oral Pill/IUCD User
Condom
Net Condom user = Total pieces of condom distributed- Total pieces of condoms distributed to vasectomy acceptors

Procedure of calculating equivalent sterilizationAgainst Condom user and Oral Pill/IUCD User
Oral Pill
IUCD

Thank you