Embed Size (px)
Citation preview
Family and relatives as sources for improvement of ICU care
Dr Christina Jones
Nurse Consultant Critical Care Rehabilitation & Honorary Reader
Intensive Care, Whiston Hospital and Institute of Aging & Chronic Disease, University of Liverpool, UK
Needs and anxiety of relatives
While patients are in ICU– Family needs and situational anxiety related
(p < 0.0002) Rukholm et al Needs and Anxiety Levels of Relatives of Intensive Care Patients Journal of Advanced Nursing 1991;16(8):920-928
– Confiding support from nursing staff can reduce family anxiety levels
Jones C et al Social support in the ICU British Journal of Intensive Care. 1991;1(2):66-69.
Relative satisfaction with ICU
high level of satisfaction with– flexible visiting hours– high quality of treatment
Shortcomings– wanted the physician to be more available for regular
talks– relatives room uncomfortable– deficiencies in the preparations for transfer to a ward
Karlsson et al Family members' satisfaction with critical care: a pilot study Nursing in Critical Care 2011;16(1):11-18
Relatives experiences Four categories of experiences 1. Hovering - initial sense of confusion, stress, and uncertainty 2. Information seeking - to move out of the hovering state and
to identify the patient's progress3. Tracking - observing, analyzing, and evaluating patient care
and status and the family's own satisfaction with the environment and with care givers.
4. garnering of resources - act of acquiring what family members perceive as needed for themselves or their relative
Health care professionals can minimize stress by anticipating and addressing the family's needs for information and resources
Jamerson et al Experiences in the ICU. The experiences of families with a relative in the intensive care unit Heart & Lung 1996;25(6):467-474
Recommendations for future practice
Encourage the relatives to trust own coping ability and to use own resources
Give the relatives the experience of being accepted as they are Encourage the relatives to express their need to be cared about Give them opportunities to participate in the patient's treatment Invite them to share information and thoughts about the patient's
condition. Let the relatives encounter a sense of security. Let the relatives experience your commitment to the care of the
patient. Let the relatives be assured that the care given will be the best
care possible. Let the relatives experience good caring. Give the relatives opportunity for emotional and social guidance.
“LOVE” The program Leadership, Ownership,
Values, and Evaluation (LOVE)– developed over 10 years– Improving communication inside the
team– Improve information given to patients
and their relatives Carlet et al Managing intensive care units: make LOVE, not war! Journal of Critical Care 2010;25(2)
After effects for families of critical illness
Post Traumatic Stress Disorder
DSM IV-R American Psychiatric Association– Exposure to a traumatic event/s in which the
individual experienced/witnessed or was confronted with event/s involving actual or threatened death/serious injury or threat to the physical integrity of self/others AND responded with intense fear, helplessness or horror
– 3 symptom groups» Intrusion (nightmares, flashbacks)»Avoidance (avoiding reminders)»Hyperarousal (not sleeping)
– Symptoms are experienced for more than one month– Clinically significant distress/impairment in social,
occupational or other areas of functioning
Short-term reactions to ICU Early assessment
– 97% of relatives had high rates of anxiety and depression– 81% high levels of posttraumatic stress symptoms
At follow-up – 87% of relatives still had high levels of depression– 59% posttraumatic stress reaction
Factors related to distress– Women exhibited higher levels of distress and more persisting
symptoms – Trait anxiety most significant predictor of:-
» severity of depression (p < 0.001)» posttraumatic stress reaction (P<0.0001)
– Early anxiety was a predictor of the development of later posttraumatic stress symptomsPaparrigopoulos et al Short-term psychological impact on family members of intensive care unit patients. Journal of Psychosomatic Research 2006;61(5):719-722
Depression, anxiety and PTSD in relatives
Risk of developing PTSDAzoulay E et al. Risk of post-traumatic stress symptoms in family members of intensive care patients. American Journal of Respiratory and Critical Care Medicine 2005;171(9):987-994
High levels of anxiety and PTSD symptoms at 6 months
ICU Recovery Manual rehabilitation package– had no impact on relatives for:-
» HAD anxiety and depression scores between at 8 weeks and 6 months
» IES scores between study groups at 8 weeks and 6 monthsJones C et al. Post Traumatic Stress disorder-related symptoms in relatives of patients following intensive care. Intensive Care Medicine 2004;30(3):456-460– For patients
» Improved physical recovery» Had some impact on 8 week PTSD but effect loss at 6 months
Jones C et al. Rehabilitation after critical illness: A randomised, controlled trial. Critical Care Medicine 2003;31(10):2456-2461.
ICU Recovery Manual
http://nww.sthk.nhs.uk/pages/Guidelines.aspx?iPageId=4483
Depression, anxiety and PTSD in relatives
Strong correlation between relatives and patients level of anxiety & PTSD symptoms– At 6 month follow-up
» IES scores R = 0.40 p = 0.0001»HAD Anxiety scores R = 0.32 p = 0.001»HAD Depression scores R = 0.23 p = 0.015
Jones C et al. Post Traumatic Stress disorder-related symptoms in relatives of patients following intensive care. Intensive Care Medicine 2004;30(3):456-460
Impact of ICU on Quality of life of families
• Health-related quality of life– 90 days after ICU discharge or death in 21 French ICUs – SF-36 substantial impairments of:-
» emotional role» social functioning» Vitality» mental health
– 35.9% of relatives taking anxiolytics or antidepressants– 8.4% taking psychotropic agents – Factors associated with a worse mental score
» patient-related such as withdrawal of treatment decisions» older age, female gender, child of the patient, low income, chronic
disease» ICU experience (perceived conflicts between ICU staff and relatives)
Lemiale et al Health-Related Quality of Life in Family Members of Intensive Care Unit Patients Journal of Palliative Medicine 2010;13(9):1131-1137
Web-based information “Many people said that they had been completely dependent on
their relatives when they first came back home and needed help with normal daily activities. They said it was often a demanding and stressful time, particularly for their partners. One woman, whose husband had been in intensive care, said it was 'like having a child again' but she felt much better about looking after her husband at home than having him on a general ward. Some relatives we spoke to said their loved ones were 'different' when they first retuned home from hospital and that it took time to adjust to their changed personalities or mood swings.”
“Some of those who had been patients in ICU felt that more practical and emotional support would have benefited their partners and other close family members during this time. One man noted that, although everyone asked him how he'd been coping, no one ever asked about his partner's feelings, even though his illness had been a very difficult time for her as well. Some relatives we talked to said they would have liked more information on how best to look after their loved one once they were home.”http://www.healthtalkonline.org/Intensive_care/Intensive_care_Patients_experiences/Topic/1483/
What can we do to help families?
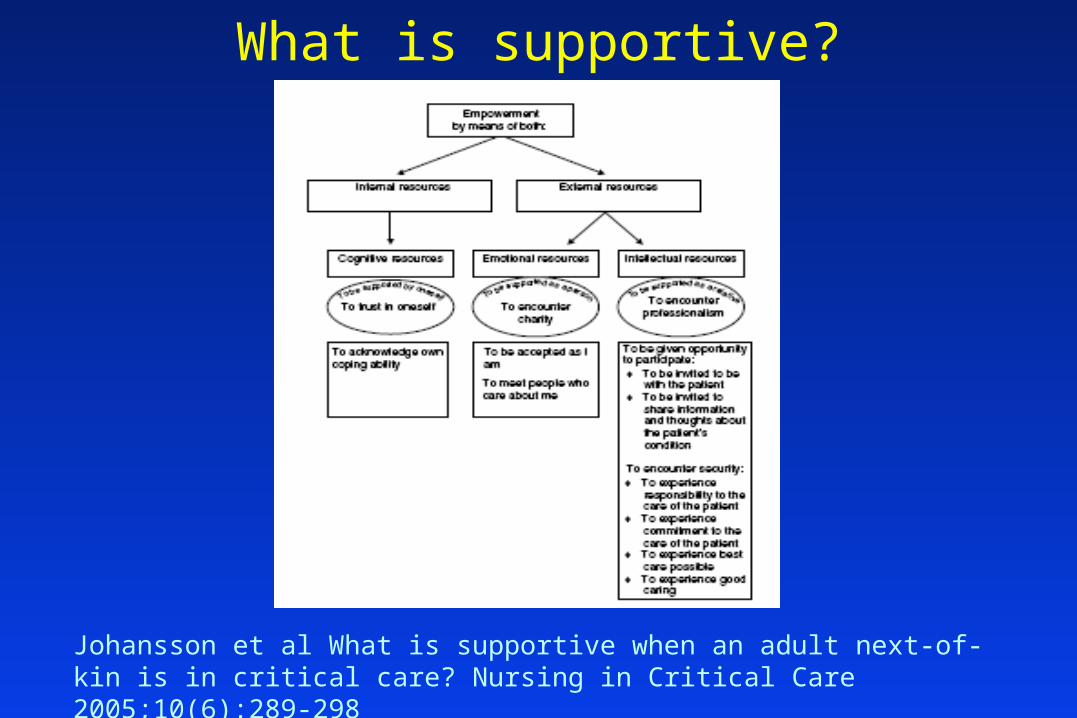
What is supportive?
Johansson et al What is supportive when an adult next-of-kin is in critical care? Nursing in Critical Care 2005;10(6):289-298
Leaving ICU The Call for Concern (C4C) project developed
– as part of Royal Berkshire Patient Safety initiative provides ICU step-down patients, and their
families, ability to call the Outreach team directly for support and advice
Relatives have knowledge of patients, and can pick up subtle signs physiological deterioration before staff
Information about how to make a call is given to patients and their family prior to being discharged from ICU to the ward– 90% of patients & relatives felt positive about the service– Led to a small number of calls but all appropriate
Odell M, Gerber K, Gager M. British Journal of Nursing 2010;19( 22):1390 - 1395
Patient and family support groups
Allows families to share:-– ICU experiences– Recovery advice and worries
Should not use a room in the hospital– Local pub in our case!!
Staff present to answer any medical questions Open access Relaxed atmosphere
Jones C, Macmillan RR, Griffiths RD. Providing psychological support to patients after critical illness. Clinical Intensive Care 1994;5(4):176-179.
Patient and family support groups patient-centred forum
– patients and relatives share experiences– drop-in sessions
Feedback from those attending– support was needed– patients and families benefited from sharing
http://www.icusteps.org/
Peskett & Gibb. Developing and setting up a patient and relatives intensive
care support group. Nursing in Critical Care 2009;14(1):4-10
ICU-steps websitehttp://www.icusteps.org/
ICU-steps – iPhone app http://www.icusteps.org/
UK NICE rehabilitation guidelines
http://www.nice.org.uk/CG83
NICE rehabilitation guidelines
Emphasis on family involvement– Family members become informal caregivers, and
this itself can exert a secondary toll of ill-health – family relationships can become altered and
financial security imperilled Discussion of short-term and medium-term
rehabilitation goals should include the family General guidance should be given
– what to expect and how to support the patient at home
– taking into account both the patient’s needs and the family’s/carer’s needs
ICU Diaries Patients really value what families write
in their dairy– Helps them understand how stressed their
relatives have been For families of dying patients it is their
chance to say goodbye– We have had diaries placed in the patient’s
coffin as a tangible sign of the family’s care for them
RACHEL II Diary study• To examine the impact of a diary on development of
PTSD • Randomised controlled trial• Study units
– Whiston Hospital, UK– Ferrara University Hospital, Italy– Haukeland University Hospital, Bergen, Norway– Ullevål Hospital, Oslo, Norway– Vrinnevishuset, Norrköping, Sweden– Gotenburg, Sweden– Malmo, Sweden– Hospital Pedro Hispano, Matosinhos, Porto, Portugal– Hospital Geral de Santo António, Porto, Portugal– Hillerød, Copenhagen, Denmark coordinating three ICUs
» Nordsjaelland, Odense, Skejby Hospitals
Experimental plan One month post ICU discharge
– Level of symptoms of PTSD using the PTSS-14Twigg E, Humphris G, Jones C, Bramwell R, Griffiths RD. Use of a screening questionnaire for post-traumatic stress disorder (PTSD) on a sample of UK ICU patients. Acta Anaesthesiol Scand 2008;52:202-208
– Randomised to study group– Intervention group
»allowed to choose when they want their diary. – Control group
»Given their diaries at the 3 month follow-up appointment after they have completed questionnaires
Three months post ICU discharge– Patients had clinic appointment or telephoned to
complete follow-up PDS for diagnosis of PTSDFoa EB et al. Psych Assess 1997;9:445-45
Results• Fewer intervention patients, compared
to controls, were diagnosed as having new onset PTSD at 3 months – 8/162 (5%) versus 21/160 (13.1%) (p =
0.02)
Jones C et al Intensive Care diaries reduce new onset PTSD following critical illness: a randomised, controlled trial Critical
Care 2010;14:R168
Impact of ICU diary for relatives
Two centres collected data for relatives– Whiston Hospital, UK– Vrinnevishuset, Norrköping, Sweden
Relatives completed PTSS-14– 1 month– 3 months
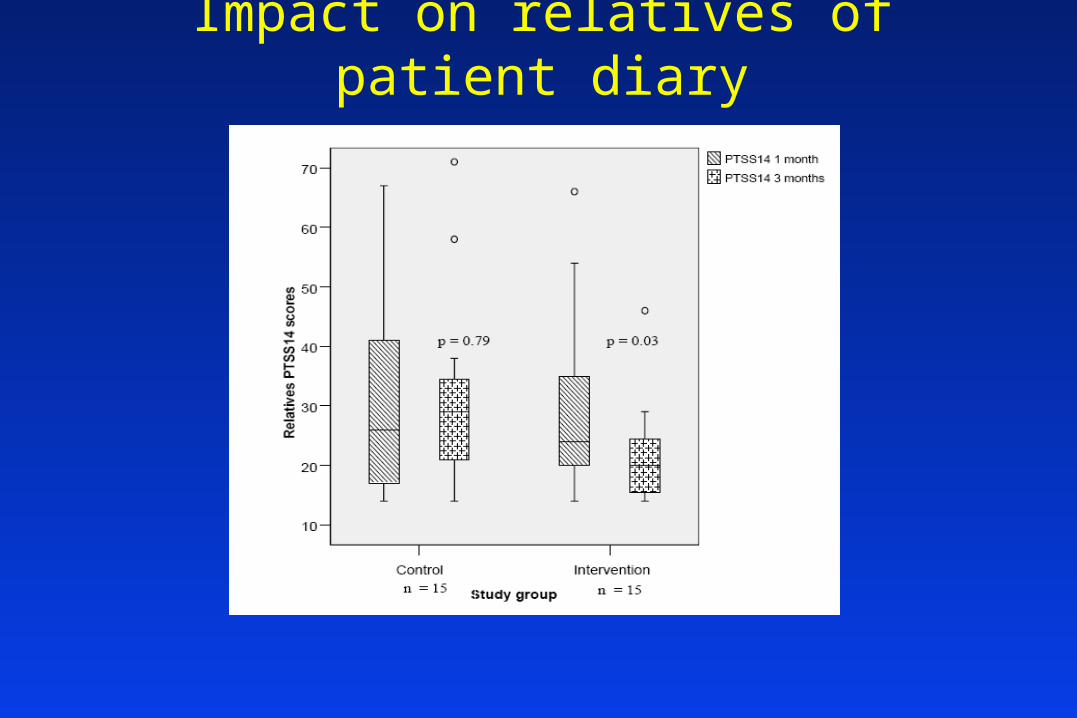
Impact on relatives of patient diary
Impact on relatives of deceased patients
All the relatives except one said the diary:-– helped them to return and adjust to everyday
life– made it easier to accept what had happened– help them to understand the seriousness of
the patient's injury or disease
Bergbom et al Patients' and relatives' opinions and feelings about diaries kept by nurses in an intensive care unit: pilot study. Intensive & Critical Care Nursing 1999;15(4):185-191
Acute post-traumatic reactions
Acute post-traumatic stress reactions in first month following traumatic event
– may resolve spontaneously in the first few weeks – regarded almost as a normal reaction to severe stress– high levels of symptoms a risk factor for developing
PTSD– The art of offering help to patients and their families
» recognising those who are not coping with their symptoms» offering appropriate and timely help» standing back from those who may come to terms with it
themselvesJones C, Griffiths RD. Patient and caregiver counselling after the intensive care unit: what are the needs and how should they be met? Current Opinion in Critical Care 2007;13:503-507
Psychological help• Helping with traumatic memories
– Screening for level of psychological distress» Watchful waiting» Refer for treatment if symptoms high» One off debriefing may make things worse
– Normalising traumatic memorieshttp://www.healthtalkonline.org/Intensive_care/
Intensive_care_Patients_experiences– Other family’s experiences
http://www.healthtalkonline.org/Intensive_care/Intensive_care_Patients_experiences/Topic/1483/– Cognitive behavioural therapy (CBT) aimed at trauma symptoms
» Systematic desensitisation» Anxiety management
– Eye Movement Desensitisation and Reprocessing (EMDR)» Processing traumatic memories
Foa et al. Journal of Clinical Psychology 1999; 60(suppl. 16): 1-76.UK NICE guideline for treatment :-http://guidance.nice.org.uk/CG26/guidance/pdf
Counselling service for ICU Relatives feel forgotten as patient recovers
– Severe anxiety, depression, PTSD– May hinder patients’ physical recovery
Unanswered questions when patient dies in ICU– Complicated grief
» Sudden death» Relationship problems» Guilt
Specialist counselling service effective
Jones C et al. Benchmarking a nurse-led ICU counselling initiative. Nursing Times 2008;104(38):32-34
Further information [email protected]