Embed Size (px)
Citation preview
liefs, and prior screening behavior among blacks and whites report-ing for prostate cancer screening. Urology. 1995;46:346 –351.
14. McCoy CB, Anwyl RS, Metsch LR, et al. Prostate cancer in Florida.Knowledge, attitudes, practices, and beliefs. Cancer Pract. 1995;3:88 –93.
15. Mainous AG, Hagen MD. Public awareness of prostate cancer andthe prostate-specific antigen test. Cancer Pract. 1994;2:217–221.
16. Zemencuk JK, Hayward RA, Skarupski KA, Katz SJ. Patients’ de-sires and expectations for medical care: a challenge to improvingpatient satisfaction. Am J Med Qual. 1999;14:21–27.
17. Zemencuk JK, Feightner JW, Hayward RA, et al. Patients’ desiresand expectations for medical care in primary care clinics. J GenIntern Med. 1998;13:273–276.
18. American Cancer Society. Cancer Facts and Figures. Atlanta, Ga:American Cancer Society; 1998.
19. American College of Physicians. Clinical guideline: part III. Screen-ing for prostate cancer. Ann Intern Med. 1997;126:480 – 484.
From the Center for Practice Management and Outcomes Research (JKZ,RAH), Ann Arbor VA Medical Center Health Services Research and De-velopment Field Program, the Departments of Internal Medicine andHealth Management and Policy (RAH, SJK), and the Consortium forHealth Outcomes, Innovation and Cost-Effectiveness Studies (CHOICES)(SJK), The University of Michigan, Ann Arbor, Michigan.
Supported by the Research and Education Foundation of the AmericanMedical Association and by the V.A. Center for Practice Management andOutcomes Research. Dr. Katz was a Robert Wood Johnson Generalist Fac-ulty Scholar at the time of this study. The opinions herein are those of theauthors and not necessarily those of the Robert Wood Johnson Foundationor the Department of Veterans Affairs.
Correspondence should be addressed to Judith K. Zemencuk, MA, Vet-erans Affairs’ Center for Practice Management and Outcomes Research,PO Box 130170, Ann Arbor, Michigan 48113-0170.
Manuscript submitted May 10, 2000, and accepted in revised formNovember 6, 2000.
Familial Periodic Feverand Amyloidosis Due to aNew Mutation in theTNFRSF1A GeneAnna Simon, MD, Catherine Dode, PhD,Jos W. M. van der Meer, MD, PhD,Joost P. H. Drenth, MD, PhD
Establishing a diagnosis in patients with recurrentepisodes of fever is often very difficult (1,2). Theepisodes of fever and signs of inflammation may
lead to a considerable morbidity, and to notable frustra-tion in patients and doctors as extensive diagnostic at-tempts often fail to reveal the cause. However, after rulingout infectious causes for the febrile attacks, one shouldconsider syndromal causes of periodic fever. At leastthree separate periodic fever syndromes have been recog-
nized: hyper-immunoglobulin (Ig)D and periodic feversyndrome (HIDS, MIM260920), the tumor necrosisfactor (TNF)-receptor associated periodic syndrome(TRAPS, MIM142680), and the best known and mostprevalent syndrome, familial Mediterranean fever (FMF,MIM249100). The identification of causative genes foreach of them (3–7) has greatly advanced diagnostic pos-sibilities and has implications for treatment as well.
We present the following observation as an example ofa typical familial case of periodic fever and amyloidosis.With the use of molecular tools we were able to make adefinitive diagnosis of TRAPS.
CASE REPORT
A 61-year old woman of Dutch-Indonesian ancestry wasreferred because of recurrent episodes of high fever andproteinuria. She had her first attack of fever as a 9-year-old child in Indonesia. At that time no elaborate diagnos-tic procedures were performed, and the recurrent feverwas attributed to attacks of malaria. She moved to theNetherlands at the age of 21 years, and shortly thereaftershe was admitted to a hospital because of a 3-week-longattack of fever, which subsided spontaneously. No perti-nent diagnosis could be made. From that time onward,the fever episodes occurred approximately twice a yearand generally lasted up to 3 weeks. Usually, a short courseof steroids was administered because the impression ex-isted that this ameliorated the attacks. Apart from fever,generalized myalgia, and fatigue during the attacks she
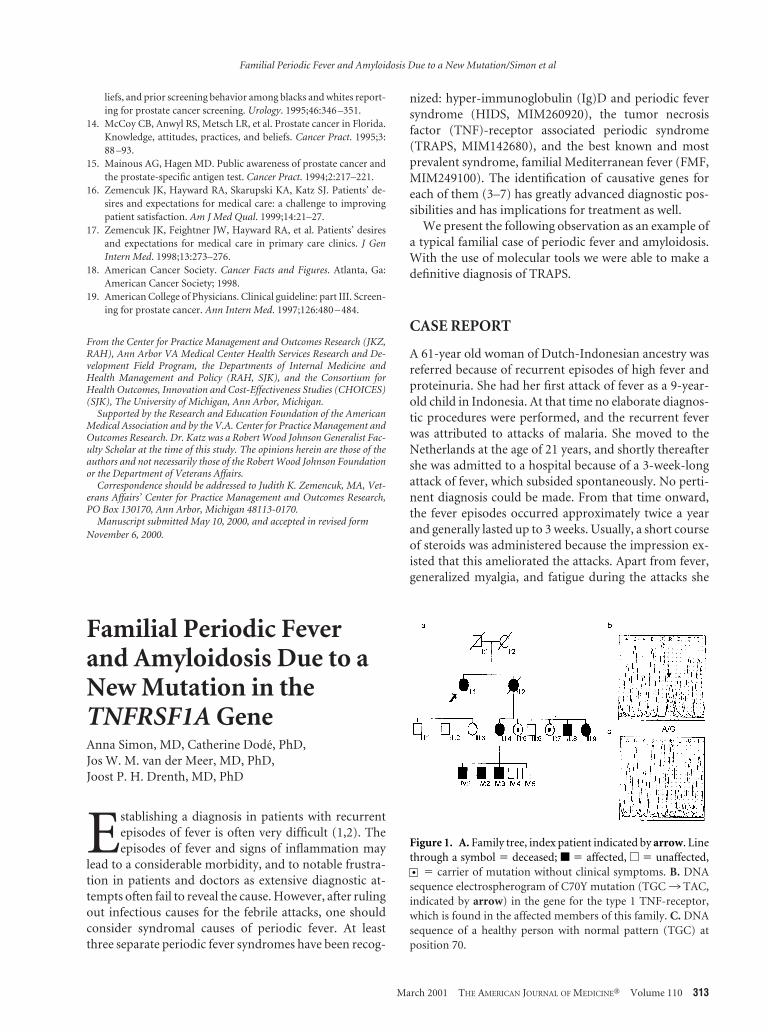
Figure 1. A. Family tree, index patient indicated by arrow. Linethrough a symbol 5 deceased; f 5 affected, e 5 unaffected,
5 carrier of mutation without clinical symptoms. B. DNAsequence electrospherogram of C70Y mutation (TGC3 TAC,indicated by arrow) in the gene for the type 1 TNF-receptor,which is found in the affected members of this family. C. DNAsequence of a healthy person with normal pattern (TGC) atposition 70.
Familial Periodic Fever and Amyloidosis Due to a New Mutation/Simon et al
March 2001 THE AMERICAN JOURNAL OF MEDICINEt Volume 110 313
had no specific symptoms. During each of her three (un-complicated) pregnancies she was free from symptoms,but after each delivery she experienced a severe febrilebout. Attacks could further be provoked by emotionaland physical stress. She gave a positive family history. Hersister, who died at age 47 due to breast carcinoma, hadexperienced similar febrile attacks during life. Three ofher sister’s six children and three of her sister’s five grand-sons were also affected (Figure 1). Symptoms and perti-nent laboratory results of our patient and four affectedrelatives are summarized in Table 1. There are notenough data available to determine definitely which ofthe parents of our patient transmitted the disease to theiroffspring. It is also unclear whether the disease originatedfrom the Dutch or Indonesian side of the family.
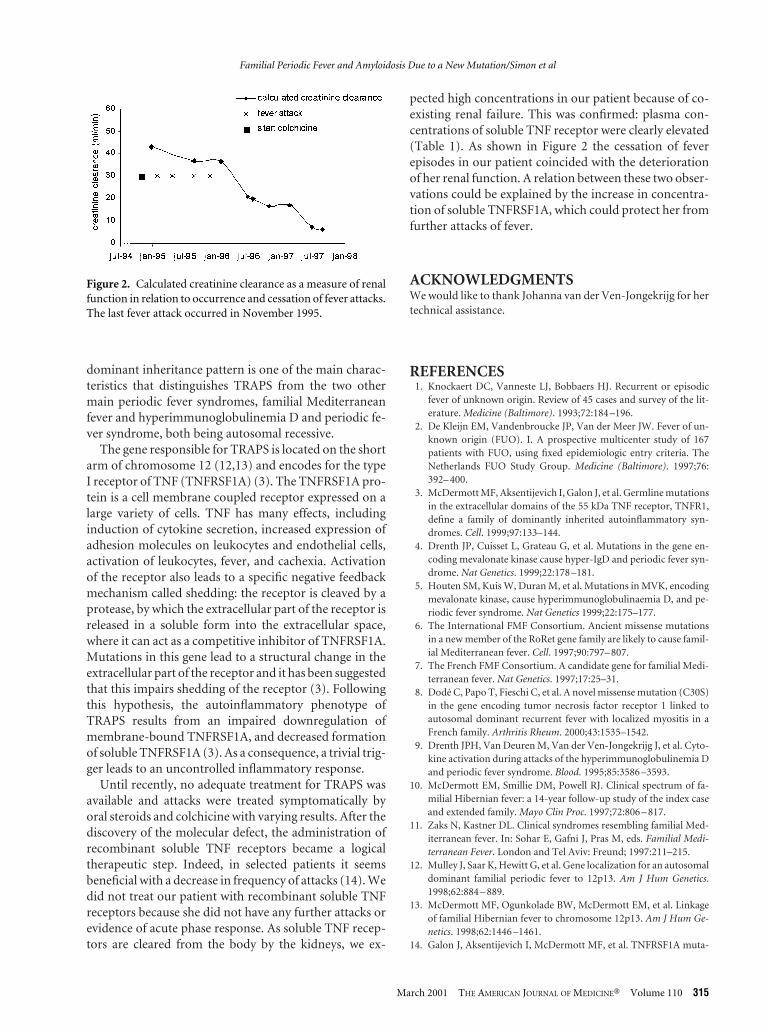
Our patient noticed an increase in the frequency of thefever attacks after reaching menopause to about 4 or 5times each year. In the following years she developed re-nal failure, despite colchicine treatment. Both rectal andrenal biopsies showed evidence of type AA amyloidosis.Since 1997 she has been dependent on intermittent he-modialysis. Most remarkably, the decrease of renal func-tion coincided with a cessation of fever episodes, andsince 1996 she has been free from attacks (Figure 2)
The autosomal dominant inheritance, the long dura-tion of attacks, and the (partial) response to steroids re-minded us of TRAPS. After sequencing the TNFRSF1Agene, which codes for the p55 TNF-receptor, the incrim-inated molecule in TRAPS (8), we discovered a novel mis-sense mutation in our patient: cystine replaces tyrosine atposition 70 of the amino acid sequence of the protein(C70Y, Figure 1). The C70Y mutation has been found in10 of 17 tested family members, 2 of whom remainasymptomatic up to this day, which suggests a penetranceof 80%. With the exception of our patient (II:1), the af-fected family members had low concentrations of solubleTNFRSF1A in their blood (Table 1) as measured by en-zyme-linked immunosorbent assay (9).
DISCUSSION
The acronym TRAPS was recently suggested by McDer-mott et al (3) to be used for a group of autosomal domi-nantly inherited periodic fever syndromes previouslyknown by several names (eg, familial Hibernian fever,familial periodic fever). Patients experience recurrent at-tacks of fever accompanied by abdominal pain, myalgia,skin lesions, and conjunctivitis. Nephropathic reactiveamyloidosis of the AA type has been reported in 4 patientsup till now (10,11). The attacks occur in varying fre-quency and generally last 2 to 3 weeks. Laboratory exam-ination reveals acute phase response. The autosomal Tab
le1.
Clin
ical
Feat
ure
san
dLa
bora
tory
Res
ult
sof
Aff
ecte
dFa
mily
Mem
bers
Indi
vidu
al
Age
(Yrs
)A
ttac
ksSy
mpt
oms
and
Sign
s
C-r
eact
ive
Pro
tein
(mg/
L)
Labo
rato
ryR
esu
lts
Cu
rren
tO
nse
tLe
ngt
h(D
ays)
Freq
uen
cyM
yalg
iaA
bdom
inal
Pai
nP
leu
ral
Pai
nR
ash
Red
Eye
sIn
guin
alH
ern
ia
Seru
mA
myl
oid
AP
rote
in(m
g/L)
Solu
ble
TN
FRSF
1A
(ng/
mL)
Solu
ble
TN
FRp7
5(n
g/m
L)
II:1
*61
921
†Y
esN
oN
oN
oN
oN
A2.
70.
910
.522
.0II
I:4
458
141x
/yr
Yes
Yes
Yes
Yes
Yes
NA
152.
50.
813.
23IV
:120
514
1x/y
rY
esY
esN
oY
esY
esN
o8
3.2
0.66
3.28
IV:2
180
141x
/yr
Yes
Yes
Yes
Yes
Yes
Yes
285.
91.
003.
80IV
:315
221
1-2x
/yr
No
Yes
Yes
Yes
Yes
No
105
110.
693.
15
Indi
vidu
alis
gen
erat
ion
and
nu
mbe
rfr
omfa
mily
tree
(Fig
ure
1).
*Pro
ban
dan
dm
ain
subj
ect
ofth
iscl
inic
alob
serv
atio
n.
†V
aryi
ng
freq
uen
cydu
rin
glif
e,n
own
oat
tack
san
ymor
e,se
ete
xtfo
rde
tails
.C
-rea
ctiv
epr
otei
n(n
orm
al,
2.7
mg/
L)‡
Mea
sure
din
seru
m;s
eru
mam
yloi
dA
prot
ein
(nor
mal
,4.
2m
g/L)
‡M
easu
red
inse
rum
;sT
NFR
5so
lubl
eT
NF-
rece
ptor
con
cen
trat
ion
sin
plas
ma;
p55
5ty
pe1
(mea
n5
1.50
ng/
mL)
;p75
5ty
pe2
(mea
n5
2.51
ng/
mL)
.All
labo
rato
rym
easu
rem
ents
wer
edo
ne
from
sam
ples
take
nin
the
atta
ck-f
ree
inte
rval
.
Familial Periodic Fever and Amyloidosis Due to a New Mutation/Simon et al
314 March 2001 THE AMERICAN JOURNAL OF MEDICINEt Volume 110
dominant inheritance pattern is one of the main charac-teristics that distinguishes TRAPS from the two othermain periodic fever syndromes, familial Mediterraneanfever and hyperimmunoglobulinemia D and periodic fe-ver syndrome, both being autosomal recessive.
The gene responsible for TRAPS is located on the shortarm of chromosome 12 (12,13) and encodes for the typeI receptor of TNF (TNFRSF1A) (3). The TNFRSF1A pro-tein is a cell membrane coupled receptor expressed on alarge variety of cells. TNF has many effects, includinginduction of cytokine secretion, increased expression ofadhesion molecules on leukocytes and endothelial cells,activation of leukocytes, fever, and cachexia. Activationof the receptor also leads to a specific negative feedbackmechanism called shedding: the receptor is cleaved by aprotease, by which the extracellular part of the receptor isreleased in a soluble form into the extracellular space,where it can act as a competitive inhibitor of TNFRSF1A.Mutations in this gene lead to a structural change in theextracellular part of the receptor and it has been suggestedthat this impairs shedding of the receptor (3). Followingthis hypothesis, the autoinflammatory phenotype ofTRAPS results from an impaired downregulation ofmembrane-bound TNFRSF1A, and decreased formationof soluble TNFRSF1A (3). As a consequence, a trivial trig-ger leads to an uncontrolled inflammatory response.
Until recently, no adequate treatment for TRAPS wasavailable and attacks were treated symptomatically byoral steroids and colchicine with varying results. After thediscovery of the molecular defect, the administration ofrecombinant soluble TNF receptors became a logicaltherapeutic step. Indeed, in selected patients it seemsbeneficial with a decrease in frequency of attacks (14). Wedid not treat our patient with recombinant soluble TNFreceptors because she did not have any further attacks orevidence of acute phase response. As soluble TNF recep-tors are cleared from the body by the kidneys, we ex-
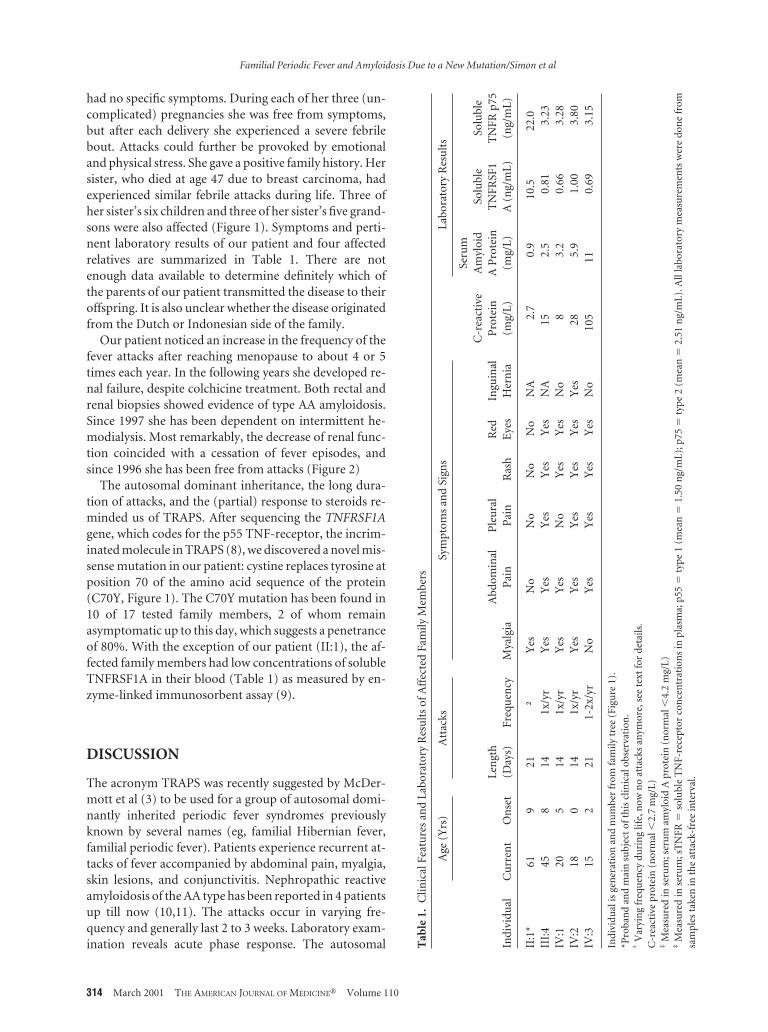
pected high concentrations in our patient because of co-existing renal failure. This was confirmed: plasma con-centrations of soluble TNF receptor were clearly elevated(Table 1). As shown in Figure 2 the cessation of feverepisodes in our patient coincided with the deteriorationof her renal function. A relation between these two obser-vations could be explained by the increase in concentra-tion of soluble TNFRSF1A, which could protect her fromfurther attacks of fever.
ACKNOWLEDGMENTSWe would like to thank Johanna van der Ven-Jongekrijg for hertechnical assistance.
REFERENCES1. Knockaert DC, Vanneste LJ, Bobbaers HJ. Recurrent or episodic
fever of unknown origin. Review of 45 cases and survey of the lit-erature. Medicine (Baltimore). 1993;72:184 –196.
2. De Kleijn EM, Vandenbroucke JP, Van der Meer JW. Fever of un-known origin (FUO). I. A prospective multicenter study of 167patients with FUO, using fixed epidemiologic entry criteria. TheNetherlands FUO Study Group. Medicine (Baltimore). 1997;76:392– 400.
3. McDermott MF, Aksentijevich I, Galon J, et al. Germline mutationsin the extracellular domains of the 55 kDa TNF receptor, TNFR1,define a family of dominantly inherited autoinflammatory syn-dromes. Cell. 1999;97:133–144.
4. Drenth JP, Cuisset L, Grateau G, et al. Mutations in the gene en-coding mevalonate kinase cause hyper-IgD and periodic fever syn-drome. Nat Genetics. 1999;22:178 –181.
5. Houten SM, Kuis W, Duran M, et al. Mutations in MVK, encodingmevalonate kinase, cause hyperimmunoglobulinaemia D, and pe-riodic fever syndrome. Nat Genetics 1999;22:175–177.
6. The International FMF Consortium. Ancient missense mutationsin a new member of the RoRet gene family are likely to cause famil-ial Mediterranean fever. Cell. 1997;90:797– 807.
7. The French FMF Consortium. A candidate gene for familial Medi-terranean fever. Nat Genetics. 1997;17:25–31.
8. Dode C, Papo T, Fieschi C, et al. A novel missense mutation (C30S)in the gene encoding tumor necrosis factor receptor 1 linked toautosomal dominant recurrent fever with localized myositis in aFrench family. Arthritis Rheum. 2000;43:1535–1542.
9. Drenth JPH, Van Deuren M, Van der Ven-Jongekrijg J, et al. Cyto-kine activation during attacks of the hyperimmunoglobulinemia Dand periodic fever syndrome. Blood. 1995;85:3586 –3593.
10. McDermott EM, Smillie DM, Powell RJ. Clinical spectrum of fa-milial Hibernian fever: a 14-year follow-up study of the index caseand extended family. Mayo Clin Proc. 1997;72:806 – 817.
11. Zaks N, Kastner DL. Clinical syndromes resembling familial Med-iterranean fever. In: Sohar E, Gafni J, Pras M, eds. Familial Medi-terranean Fever. London and Tel Aviv: Freund; 1997:211–215.
12. Mulley J, Saar K, Hewitt G, et al. Gene localization for an autosomaldominant familial periodic fever to 12p13. Am J Hum Genetics.1998;62:884 – 889.
13. McDermott MF, Ogunkolade BW, McDermott EM, et al. Linkageof familial Hibernian fever to chromosome 12p13. Am J Hum Ge-netics. 1998;62:1446 –1461.
14. Galon J, Aksentijevich I, McDermott MF, et al. TNFRSF1A muta-
Figure 2. Calculated creatinine clearance as a measure of renalfunction in relation to occurrence and cessation of fever attacks.The last fever attack occurred in November 1995.
Familial Periodic Fever and Amyloidosis Due to a New Mutation/Simon et al
March 2001 THE AMERICAN JOURNAL OF MEDICINEt Volume 110 315

tions, and autoinflamatory syndromes. Curr Opin Immunol. 2000;12:479 – 486.
From the Department of General Internal Medicine (AS, JWMVDM,JPHD), UMC St. Radboud, Nijmegen, The Netherlands; and Laboratoirede Biochimie et de Genetique Moleculaire Humaine (CD), Universite ParisV, Institut Cochin de Genetique Moleculaire, and Hopital Cochin, Assis-tance Publique-Hopitaux de Paris, Paris, France.
Supported by le Program Hospitalier de Recherche Clinique (1997). Dr.Simon is a recipient of a Dutch organization for Scientific Research Fellow-ship for Clinical Investigators (KWO nr. 920 – 03–116).
Correspondence should be addressed to Anna Simon, MD, Departmentof General Internal Medicine, 541, UMC St. Radboud, PO Box 9101, 6500HB Nijmegen, The Netherlands.
Manuscript submitted July 14, 2000, and accepted in revised form Oc-tober 27, 2000.
Familial Periodic Fever and Amyloidosis Due to a New Mutation/Simon et al
316 March 2001 THE AMERICAN JOURNAL OF MEDICINEt Volume 110