Embed Size (px)
Citation preview

Familial Hypercholesterolemia Canada Hypercholestérolémie Familiale Canada

Outline of this presentation
Introduction on FH FH Canada registry
Goals Inclusion criteria iCapture database
Increase awareness on FH Opening new sites Cascade screening strategy FH Canada website Update on Position Statement on FH Educational resources
•

FH is One of the Most Common of Inherited Diseases
Frequency per 1,000 births
Heterozygous FH
Haemophilia
Dominant ostosclerosis Adult polycstic kidney disease
Huntington’s disease Cystic fibrosis
Duchenne muscular dystrophy Sickle cell anemia
Phenylketonuria
0 1 2 3 4 5
Marfans syndrome
Heritable, autosomal co-dominant disorder
Usually due to mutations in LDL receptor gene > 1700 mutations LDLR mutation 1 in 250 - 500; 1/270 in Quebec ~ 84,000 patients in Canada: ~ 29,000 in Qc; ~ 55,000 ROC; with less than 5% of patients
diagnosed
Prevalence has been recently revised to 1 in 250 so in Canada = over 140,000 pts. Ref: Prevalence of FH in the 1999 to 2012 United States National Health and Nutrition Examination Surveys (NHANES). de Ferranti SD, Rodday AM, Mendelson
MM, Wong JB, Leslie LK, Sheldrick RC. Circulation. 2016;133(11):1067-72.
Familial Hypercholesterolemia
Nordestgaard B G et al. Eur Heart J 2013;34:3478-3490

Pathophysiology of HeFH
Nordestgaard B G et al. Eur Heart J 2013;34:3478-3490

Clinical manifestations
Genest J, Hegele RA, Bergeron J, Brophy J, Carpentier A, Couture P, et al. Canadian Cardiovascular Society position statement on familial hypercholesterolemia. The Canadian journal of cardiology. 2014;30(12):1471-81.
Bilateral xanthelasma
Arcus Cornae
Xanthomas within the Achilles tendons Xanthoma within extensor tendon of the hand

Aim of FH Canada registry
• The aim of the FH registry is to improve the detection and management of individuals and families with FH in Canada. Rare diseases of lipoprotein metabolism are also included (SMASH initiative)
• Initiated at University of British Columbia and became national in 2014.
• Over 90 clinicians and scientists in 18 academic centers across Canada form the “hubs” of FH Canada.
Clinicaltrials.gov: NCT02009345
The MISSION of the Canadian FH Registry is to bring together a multi-disciplinary group of physicians, basic and clinical researchers to improve the delivery of care to patients with severe lipoprotein disorders, especially FH, and to foster collaborative research.
Our VISION is to create a Canada-wide network of academic clinics, integrating lipid specialists, endocrinologists and cardiologists to treat patients with the highest standard of care and to create a collaborative research environment. Using a “hub and spoke” model, the registry will be extended in various communities to link primary care physicians with provincial academic centers.
The GOALS are to improve care to patients with FH and to reduce cardiovascular disease in this population at high risk.

FH Canada: Governance Structure
National Advisory Board International Advisory Board Scientific Board
Objective 2 Biomedical;
Genetics
Objective 3 Clinical Network
Objective 4 Health Systems Services
Outcomes and Economics
Objective 5 GE3LS; Knowledge
Translation
Ethics Rep. MD Rep.
Patient Reps: Legal Rep. Lay Rep.
Nursing Rep. Pharma Rep.
Dr. J. Knowles (US) Dr. GK. Hovingh (Netherlands)
Dr. M. Farnier (France) Dr. F. Civeira (Spain)
Dr. R Cramb (UK)
R. Hegele D. Gaudet J. Genest J. Engert G. Pare
D. Gaudet, J. Frohlich J. Mancini
J. Bergeron P. Couture
and other clinicians Peds population Homozygous FH
SMASH
J. Brophy M. Henderson
Patient Rep. D. Bewick M. Gupta
J. Genest J. Frohlich D. Gaudet R. Hegele J. Brophy
B. McCrindle
iCAPTURE Manager
Data Management
Coordinator I. Ruel
Objective 1: FH and SMASH Registry

FH Registry: Benefits
FH and SMASH Registry; Biomedical and Genetics; Clinical Network; Health Systems Services, Outcomes and Economics; GE3LS and Knowledge Translation
•Genetics, NextGen sequencing, gene-gene interactions, novel pathways •Orphan diseases of lipoprotein network •Clinical trials; investigator-initiated research, clinical research network •Health Outcomes, administrative database research •Health Economics •Resource utilisation, population studies, comparative effectiveness
Training and Knowledge Translation •Training basic students in translational research •Training residents with NLA certification •Conferences •CCS Position Statement on FH •Patient- and Physician-oriented Website
Benefits for BioPharmaceutical Industry •Access to experts in lipidology •Clinical network for industry-initiated research •Novel genes/targets •Health economics •Access to registry data
Benefits for Patients •Expert care •Optimal treatment •Access to clinical trials •Access to novel Rx •Consultation service •Cascade family screening
Benefits for Clinicians and Researchers •Standardized diagnostic •Expert advice •Investigator-initiated research •Biobanking and database •Multi-center studies
Health Care and Research Network Local, Provincial, National and International Collaborations
Benefits for Canada •Policies, consensus guidelines, pediatric guidelines •Collaborative research environment •Resource allocation (Federal and Provincial) •Health outcomes •Health economics •Genetic testing

Inclusion criteria: Canadian Definition
1st-degree relative with ↑ LDL-C OR
1st-degree relative with early onset ASCVD (<55 yr Men; <65 yr women)
Definite FH
Yes
Probable FH (Consider DNA testing)
*LDL-C ≥ 5.0 mmol/L (≥40 yr) LDL-C ≥ 4.0 mmol/L in <18 yr
LDL-C ≥ 4.5 mmol/L in ≥ 18 and <40 yr
+
Hypercholesterolemia (Consider DNA testing)
* Secondary causes ruled out (nephrotic syndrome, obstructive jaundice, hypothyroidism, drugs, other). **Mutation in LDL-r, ApoB or PCSK9; Presence of a DNA causing mutation in a proband is sufficient for a diagnosis of FH. Treatment decision should be at the discretion of the treating physician.
Known FH causing DNA Mutation in proband** or 1st-degree relative
OR Tendinous xanthomas
OR LDL-C ≥ 8.5 mmol/L
Maj
or C
riter
ia
FH S
cree
ning
C
riter
ia
Min
or C
riter
ia
No
Yes No
• The James Hogg Research Centre at St-Paul’s Hospital, UBC, Vancouver is providing the iCAPTURE platform used to capture the data from the FH Canada Registry.
• Data entry at each site (local) is performed using nominative information and coded specific to the institution (hospital ID number).
• Local site: all users receive secure login credentials (full access to all
local data for investigator and study coordinator; data entry only for clerk).
• In addition, a unique identifier is randomly assigned to each patient (0 to 999999) and only this number is used in the de-identified National registry, which will be used for health outcomes and health economic studies.
Entering data in iCapture
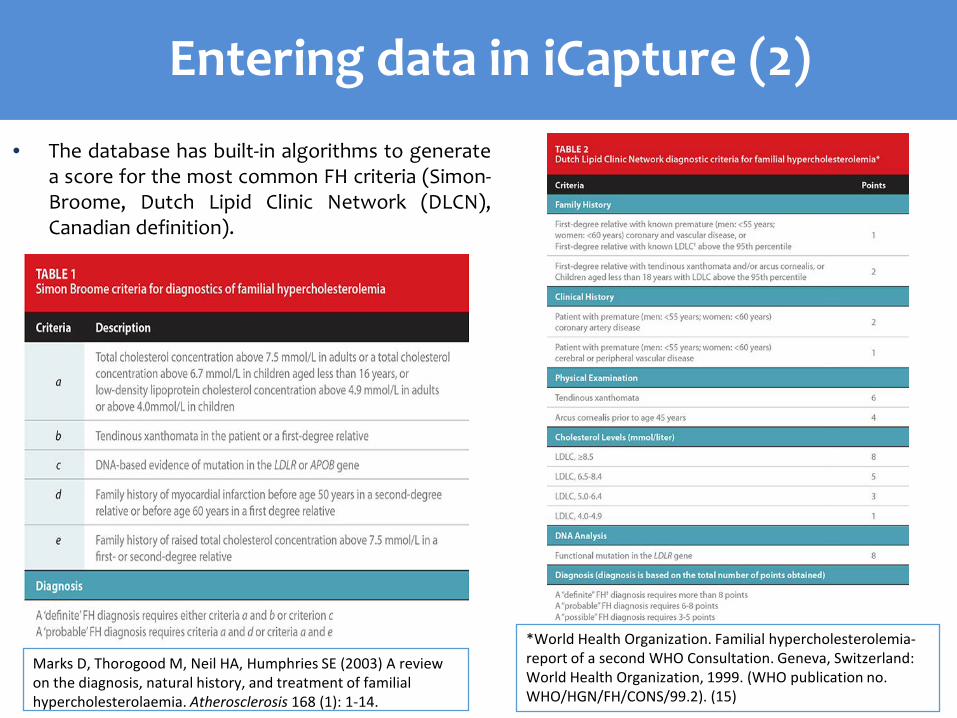
• The database has built-in algorithms to generate a score for the most common FH criteria (Simon-Broome, Dutch Lipid Clinic Network (DLCN), Canadian definition).
Marks D, Thorogood M, Neil HA, Humphries SE (2003) A review on the diagnosis, natural history, and treatment of familial hypercholesterolaemia. Atherosclerosis 168 (1): 1-14.
*World Health Organization. Familial hypercholesterolemia-report of a second WHO Consultation. Geneva, Switzerland: World Health Organization, 1999. (WHO publication no. WHO/HGN/FH/CONS/99.2). (15)
Entering data in iCapture (2)
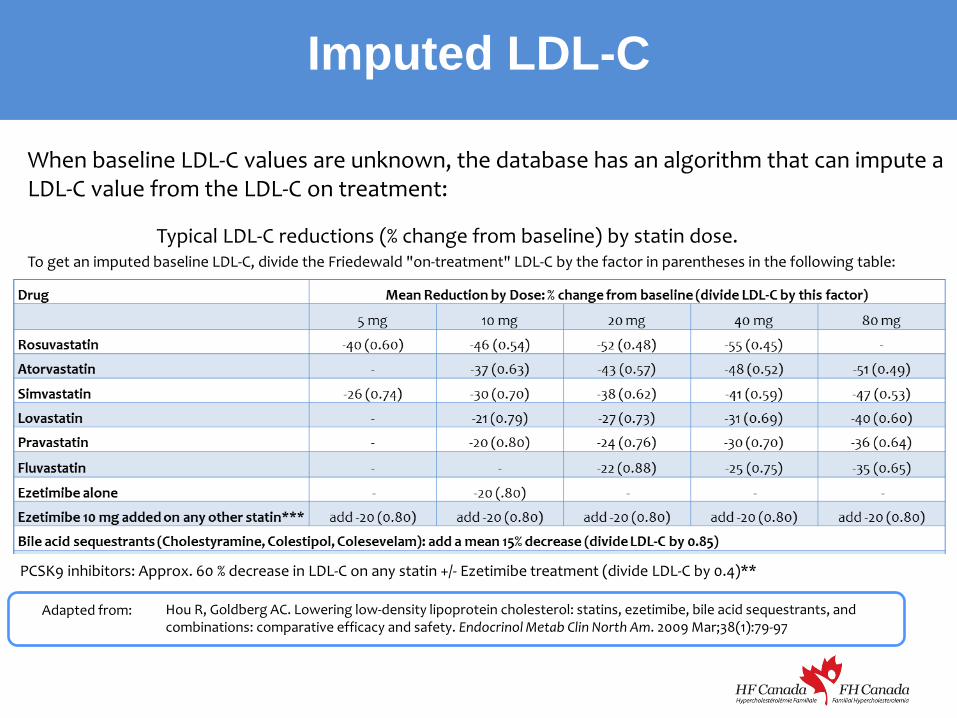
Imputed LDL-C
To get an imputed baseline LDL-C, divide the Friedewald "on-treatment" LDL-C by the factor in parentheses in the following table: Typical LDL-C reductions (% change from baseline) by statin dose.
Adapted from: Hou R, Goldberg AC. Lowering low-density lipoprotein cholesterol: statins, ezetimibe, bile acid sequestrants, and combinations: comparative efficacy and safety. Endocrinol Metab Clin North Am. 2009 Mar;38(1):79-97
PCSK9 inhibitors: Approx. 60 % decrease in LDL-C on any statin +/- Ezetimibe treatment (divide LDL-C by 0.4)**
When baseline LDL-C values are unknown, the database has an algorithm that can impute a LDL-C value from the LDL-C on treatment:
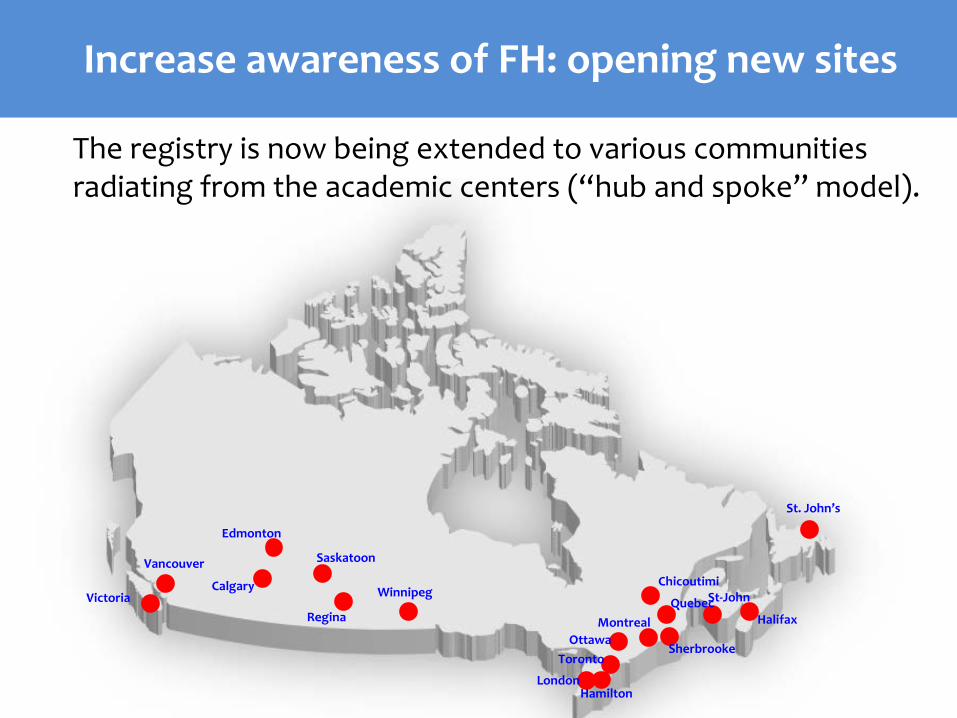
Increase awareness of FH: opening new sites
Vancouver
Victoria Calgary
Edmonton
Regina
Saskatoon
Winnipeg
Toronto Ottawa
Montreal Quebec
Chicoutimi
Sherbrooke
London Hamilton
St-John
St. John’s
Halifax
The registry is now being extended to various communities radiating from the academic centers (“hub and spoke” model).

Increase awareness of FH: Cascade screening strategy
1- The first patients to be recruited will be those with a high LDL-C already followed at the site clinic. 2- Then, family members and other undiagnosed patients (ex. siblings and cousins) are recruited from cascade screening and are referred to the nearest FH Canada participating site (www.fhcanada.net). 3- New patients will be recruited with the help of the FH Canada website and the increasing awareness of FH in Canada.

• Participating sites • Database access link • Apps (Canadian FH diagnosis, Imputed LDL-C) • Brochures • FH resources for patients and HCPs • …
Increase awareness of FH: Website www.fhcanada.net

Increase awareness of FH: Position Statement on FH

Increase awareness of FH: Position Statement on FH (2)
Will be updated because: • New Canadian definition of FH
• New information on cardiovascular risk in FH patients • New Canadian Cholesterol guidelines 2016 • Novel therapeutic approaches
New information on cardiovascular risk in FH patients
Amit V. Khera, Hong-Hee Won, Gina M. Peloso, Sekar Kathiresan, on behalf of investigators from the Myocardial I89nfarction Genetics and CHARGE Consortia
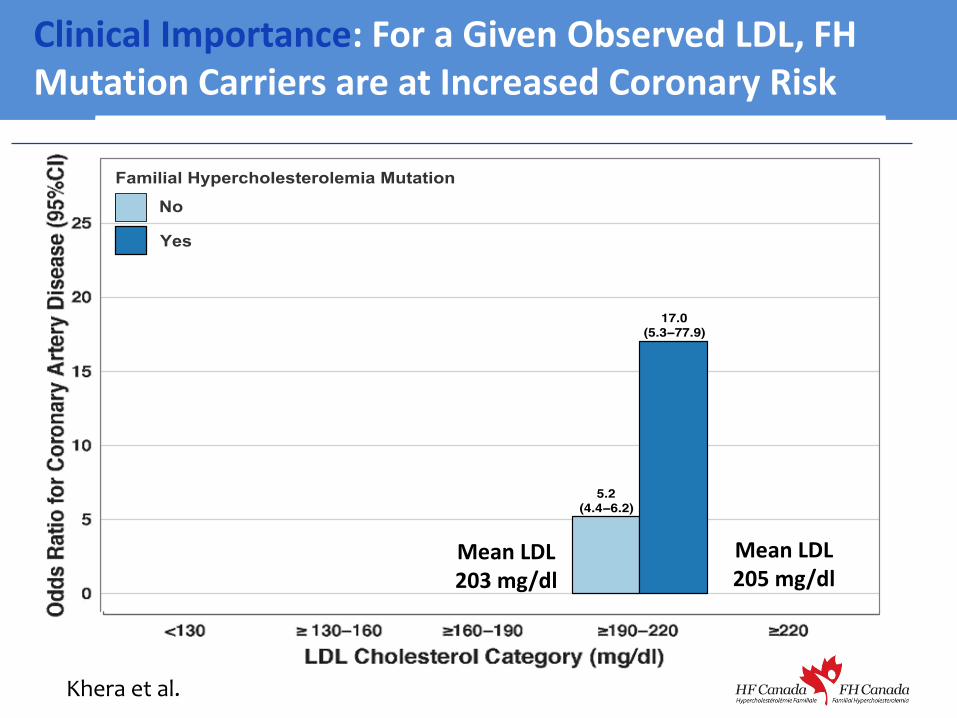
Clinical Importance: For a Given Observed LDL, FH Mutation Carriers are at Increased Coronary Risk
Mean LDL 203 mg/dl
Mean LDL 205 mg/dl
Khera et al.
Create an accredited teaching material on FH (slide kit) Revise the core curriculum in lipoprotein disorders (downloadable)
Both educational resources will be bilingual and freely available online, and
will include: • latest knowledge on FH • revised Canadian diagnostic criteria • imputed LDL-C tool (useful for assessing the degree of severity of FH
for new patients) • available treatments in Canada • results from the latest clinical trials and details on the on-going trials,
including the use of PCSK9 and CETP inhibitors • update of the fourth edition of the book “Dyslipoproteinemias: The
Clinical Approach” (Dr D. Gaudet) • summary of the CCS position statement on FH • a section on understanding the genetic basis of FH in Canada
including the unique LipidSeq and MLPA techniques
Increase awareness of FH: Educational resources
Educational material will be assessed and updated yearly, and will be downloadable for tablets, iPods and iPhones.
FH Canada registry is a unique network of more than 150 basic researchers, clinicians specializing in lipidology, endocrinology, pediatric endocrinology, obesity and cardiology, clinic coordinators and industry partners. If you have any questions about the registry, you may visit our website at www.fhcanada.net You may also contact the national coordinator: Isabelle Ruel PhD Research Institute of the McGill University Health Centre 1001 Decarie blvd, Block E #E01.2123 Montreal, Quebec H4A 3J1 514-934-1934, ext. 34852 [email protected]

FH Canada sponsors:
Thank you










![Pharmacogenetics: past, present and future · could explain individual differences in drug response [2] 1957 Kalow and Genest Characterisation of serum cholinesterase deficiency](https://img.pdfslide.us/doc/110x75/5f67b59097c12d03d5553b24/pharmacogenetics-past-present-and-future-could-explain-individual-differences.jpg)