Embed Size (px)
Citation preview

Technical Note
Falxuplication, a Novel Method for Wrap-Clipping a Fusiform Aneurysm: Technical
Note
Martin M. Mortazavi1, Tania Hassanzadeh2, Kianoush Khalili1, Sajid S. Suriya1, M. Asif Taqi1, Salman A. Fard1,R. Shane Tubbs3
-BACKGROUND: Various techniques have been used forwrap-clipping a ruptured, fusiform intracranial aneurysm;however, there is no available literature on use of the falxcerebri for wrap-clipping. We present a review of theliterature, with an illustrative case, of a ruptured fusiformpericallosal artery aneurysm firmly attached to the loweredge of the falx cerebri and not amenable to endovascularintervention.
-METHODS: Although the firm attachment between theinferior falx and the fusiform aneurysm was maintained, asection of the lower thinner part of the falx cerebri firmlyattached to the aneurysm was dissected and wrappedaround the fusiform aneurysm, and then stabilized with afenestrated clip. We chose a segment slightly longer thanthe length of the fusiform aneurysm to avoid pree andpostewrap-clipping stenosis.
-RESULTS: Postprocedure, except for a small area ofnumbness on the left distal anterolateral left leg, the pa-tient was neurologically intact and remained neurologi-cally intact at a 12-month follow-up.
-CONCLUSIONS: An inferior thin segment of the falx cer-ebri can be used for wrap-clipping of ruptured fusiformanterior cerebral artery aneurysms. Furthermore, the inferiorfalx can be wrapped around the attached fusiform anteriorcerebral artery aneurysm without compromising flow,offering a safe solution in these unusually complex cases.
Key words- Falx cerebri- Falxuplication- Fusiform aneurysm- Wrap-clipping
Abbreviations and AcronymsACA: Anterior cerebral arteryCT: Computed tomographySAH: Subarachnoid hemorrhage
40 www.SCIENCEDIRECT.com WORLD NE
INTRODUCTION
he overall prevalence of intracranial aneurysms is
approximately 2%e3%,1-3 with peak incidence during the
T sixth decade of life.1 Different reports estimate theoverall risk of aneurysmal rupture at 2e30/100,000 individualsper year.2,4-6 As classified by morphology, intracranial
aneurysms can be saccular, fusiform, or dissecting. Saccularaneurysms are the most common, accounting for 90% of cases
and for most of the morbidity and mortality associated withaneurysmal subarachnoid hemorrhage (SAH).7
Fusiform aneurysms, the focus of this article, are the secondmost common type. They can be defined as a circumferential
dilation of a segment of an intracranial artery lacking a definedorifice of flow, unlike saccular aneurysms.7 Because the inflow
and outflow are longitudinally separate in fusiform aneurysms,resulting in no clearly defined anatomic neck, surgical and
endovascular interventions are challenging.7 Without ananatomic neck akin to saccular aneurysms, fusiform aneurysms
are not easily amenable to clipping or coiling. The reportedprevalence is between 3% and 13% of all intracranial
aneurysms and has increased in recent years.8,9 Atheroscle-rotic fusiform aneurysms have a 5.2% annual mortality risk
owing to rupture or ischemic stroke, compared with 0.51% fornonatherosclerotic fusiform aneurysms.10 Fusiform aneurysm
risk progression is also greater in atherosclerotic patients; theannual risk is 12% for atherosclerotic fusiform aneurysms
versus 1.6% for nonatherosclerotic ones.10 The same studydemonstrated that atherosclerotic fusiform aneurysms are
more likely to be located in the posterior circulation and oflarger diameter, with a mean size of 11.6 mm versus 7.5 mm
for nonatherosclerotic ones.10 It has also been suggested thatarterial dissection can lead to the formation of fusiform
aneurysms.11
From the 1National Skull Base Center, Thousand Oaks, California; 2Banner University MedicalCenter-Tucson, Tucson, Arizona; and 3Seattle Science Foundation, Seattle, Washington, USA
To whom correspondence should be addressed: Martin M. Mortazavi, M.D.[E-mail: [email protected]]
Citation: World Neurosurg. (2018) 109:40-46.https://doi.org/10.1016/j.wneu.2017.09.059
Supplementary digital content available online.
Journal homepage: www.WORLDNEUROSURGERY.org
Available online: www.sciencedirect.com
1878-8750/$ - see front matter ª 2017 Elsevier Inc. All rights reserved.
UROSURGERY, https://doi.org/10.1016/j.wneu.2017.09.059
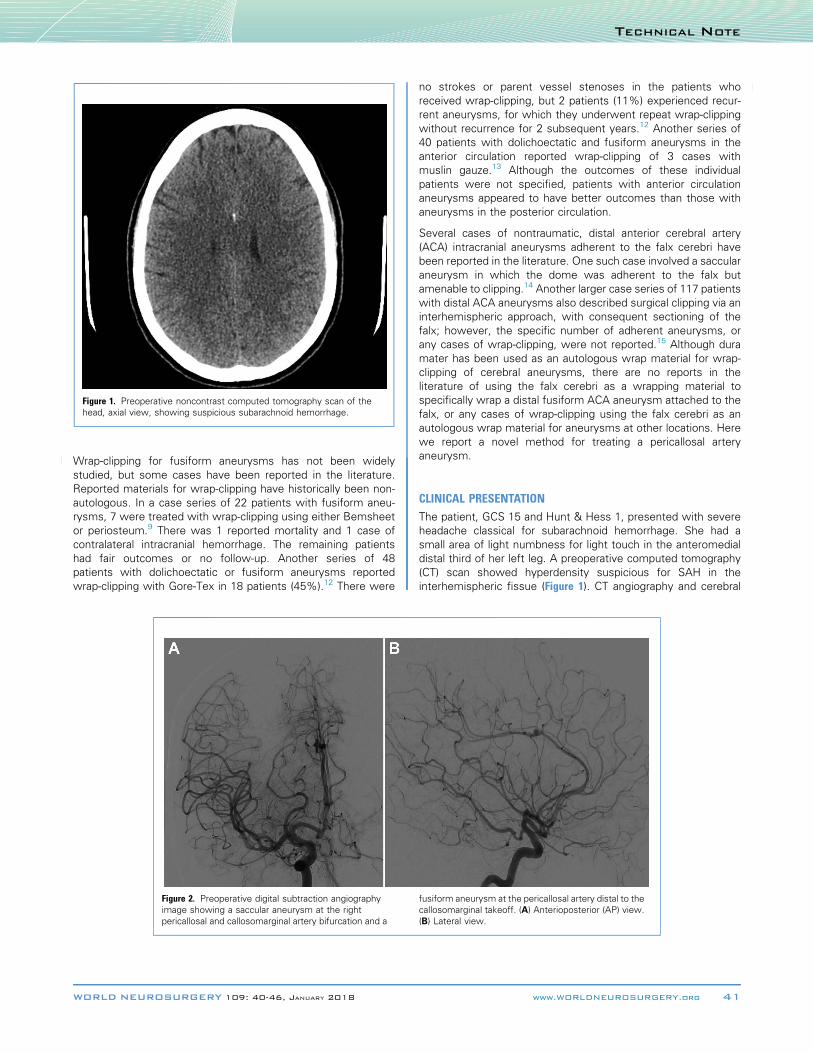
Figure 1. Preoperative noncontrast computed tomography scan of thehead, axial view, showing suspicious subarachnoid hemorrhage.
TECHNICAL NOTE
Wrap-clipping for fusiform aneurysms has not been widely
studied, but some cases have been reported in the literature.Reported materials for wrap-clipping have historically been non-
autologous. In a case series of 22 patients with fusiform aneu-rysms, 7 were treated with wrap-clipping using either Bemsheet
or periosteum.9 There was 1 reported mortality and 1 case ofcontralateral intracranial hemorrhage. The remaining patients
had fair outcomes or no follow-up. Another series of 48patients with dolichoectatic or fusiform aneurysms reported
wrap-clipping with Gore-Tex in 18 patients (45%).12 There were
Figure 2. Preoperative digital subtraction angiographyimage showing a saccular aneurysm at the rightpericallosal and callosomarginal artery bifurcation and a
WORLD NEUROSURGERY 109: 40-46, JANUARY 2018
no strokes or parent vessel stenoses in the patients who
received wrap-clipping, but 2 patients (11%) experienced recur-rent aneurysms, for which they underwent repeat wrap-clipping
without recurrence for 2 subsequent years.12 Another series of40 patients with dolichoectatic and fusiform aneurysms in the
anterior circulation reported wrap-clipping of 3 cases withmuslin gauze.13 Although the outcomes of these individual
patients were not specified, patients with anterior circulationaneurysms appeared to have better outcomes than those with
aneurysms in the posterior circulation.
Several cases of nontraumatic, distal anterior cerebral artery
(ACA) intracranial aneurysms adherent to the falx cerebri havebeen reported in the literature. One such case involved a saccular
aneurysm in which the dome was adherent to the falx butamenable to clipping.14 Another larger case series of 117 patients
with distal ACA aneurysms also described surgical clipping via aninterhemispheric approach, with consequent sectioning of the
falx; however, the specific number of adherent aneurysms, orany cases of wrap-clipping, were not reported.15 Although dura
mater has been used as an autologous wrap material for wrap-clipping of cerebral aneurysms, there are no reports in the
literature of using the falx cerebri as a wrapping material tospecifically wrap a distal fusiform ACA aneurysm attached to the
falx, or any cases of wrap-clipping using the falx cerebri as anautologous wrap material for aneurysms at other locations. Here
we report a novel method for treating a pericallosal arteryaneurysm.
CLINICAL PRESENTATION
The patient, GCS 15 and Hunt & Hess 1, presented with severeheadache classical for subarachnoid hemorrhage. She had a
small area of light numbness for light touch in the anteromedialdistal third of her left leg. A preoperative computed tomography
(CT) scan showed hyperdensity suspicious for SAH in theinterhemispheric fissue (Figure 1). CT angiography and cerebral
fusiform aneurysm at the pericallosal artery distal to thecallosomarginal takeoff. (A) Anterioposterior (AP) view.(B) Lateral view.
www.WORLDNEUROSURGERY.org 41
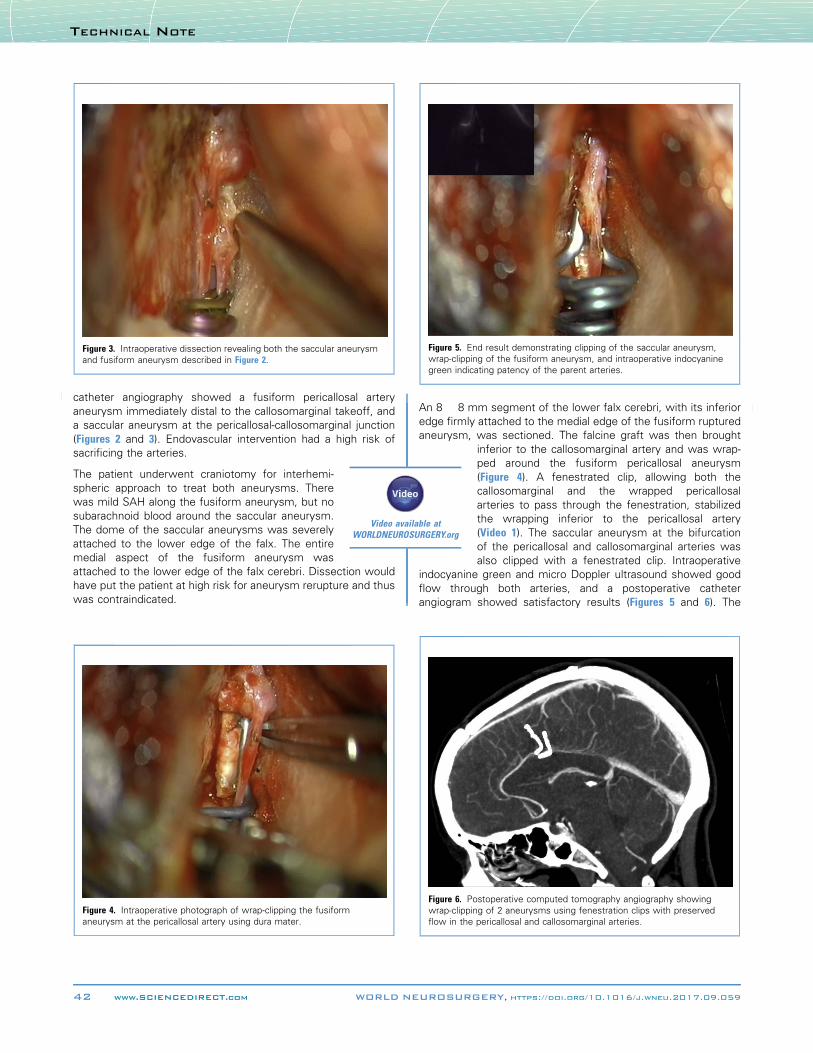
Figure 3. Intraoperative dissection revealing both the saccular aneurysmand fusiform aneurysm described in Figure 2.
Figure 5. End result demonstrating clipping of the saccular aneurysm,wrap-clipping of the fusiform aneurysm, and intraoperative indocyaninegreen indicating patency of the parent arteries.
TECHNICAL NOTE
catheter angiography showed a fusiform pericallosal artery
aneurysm immediately distal to the callosomarginal takeoff, anda saccular aneurysm at the pericallosal-callosomarginal junction
(Figures 2 and 3). Endovascular intervention had a high risk of
Video available atWORLDNEUROSURGERY.org
sacrificing the arteries.
The patient underwent craniotomy for interhemi-
spheric approach to treat both aneurysms. Therewas mild SAH along the fusiform aneurysm, but no
subarachnoid blood around the saccular aneurysm.The dome of the saccular aneurysms was severely
attached to the lower edge of the falx. The entiremedial aspect of the fusiform aneurysm was
attached to the lower edge of the falx cerebri. Dissection wouldhave put the patient at high risk for aneurysm rerupture and thus
was contraindicated.
Figure 4. Intraoperative photograph of wrap-clipping the fusiformaneurysm at the pericallosal artery using dura mater.
42 www.SCIENCEDIRECT.com WORLD NE
An 8 � 8 mm segment of the lower falx cerebri, with its inferior
edge firmly attached to the medial edge of the fusiform rupturedaneurysm, was sectioned. The falcine graft was then brought
Figure 6. Powrap-clippinflow in the
UROSURG
inferior to the callosomarginal artery and was wrap-ped around the fusiform pericallosal aneurysm
(Figure 4). A fenestrated clip, allowing both thecallosomarginal and the wrapped pericallosal
arteries to pass through the fenestration, stabilizedthe wrapping inferior to the pericallosal artery
(Video 1). The saccular aneurysm at the bifurcationof the pericallosal and callosomarginal arteries was
also clipped with a fenestrated clip. Intraoperative
indocyanine green and micro Doppler ultrasound showed goodflow through both arteries, and a postoperative catheterangiogram showed satisfactory results (Figures 5 and 6). The
stoperative computed tomography angiography showingg of 2 aneurysms using fenestration clips with preservedpericallosal and callosomarginal arteries.
ERY, https://doi.org/10.1016/j.wneu.2017.09.059
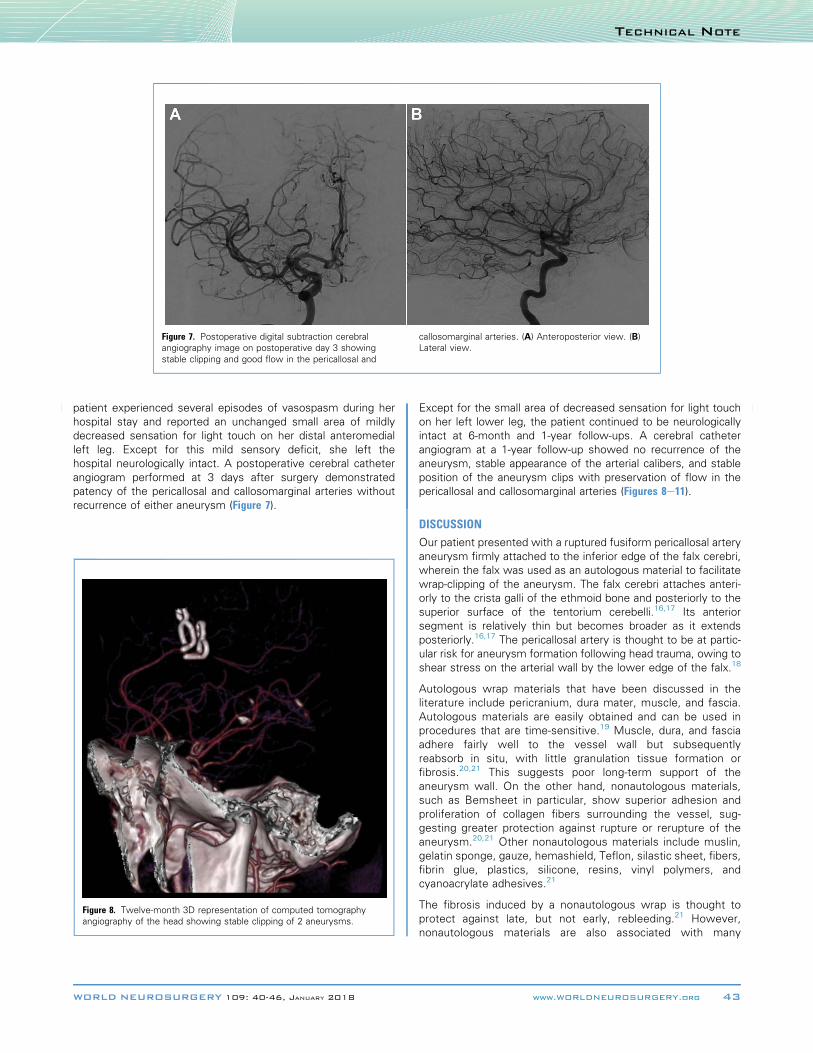
Figure 7. Postoperative digital subtraction cerebralangiography image on postoperative day 3 showingstable clipping and good flow in the pericallosal and
callosomarginal arteries. (A) Anteroposterior view. (B)Lateral view.
TECHNICAL NOTE
patient experienced several episodes of vasospasm during her
hospital stay and reported an unchanged small area of mildlydecreased sensation for light touch on her distal anteromedial
left leg. Except for this mild sensory deficit, she left thehospital neurologically intact. A postoperative cerebral catheter
angiogram performed at 3 days after surgery demonstratedpatency of the pericallosal and callosomarginal arteries without
recurrence of either aneurysm (Figure 7).
Figure 8. Twelve-month 3D representation of computed tomographyangiography of the head showing stable clipping of 2 aneurysms.
WORLD NEUROSURGERY 109: 40-46, JANUARY 2018
Except for the small area of decreased sensation for light touch
on her left lower leg, the patient continued to be neurologicallyintact at 6-month and 1-year follow-ups. A cerebral catheter
angiogram at a 1-year follow-up showed no recurrence of theaneurysm, stable appearance of the arterial calibers, and stable
position of the aneurysm clips with preservation of flow in thepericallosal and callosomarginal arteries (Figures 8e11).
DISCUSSION
Our patient presented with a ruptured fusiform pericallosal artery
aneurysm firmly attached to the inferior edge of the falx cerebri,wherein the falx was used as an autologous material to facilitate
wrap-clipping of the aneurysm. The falx cerebri attaches anteri-orly to the crista galli of the ethmoid bone and posteriorly to the
superior surface of the tentorium cerebelli.16,17 Its anteriorsegment is relatively thin but becomes broader as it extends
posteriorly.16,17 The pericallosal artery is thought to be at partic-ular risk for aneurysm formation following head trauma, owing to
shear stress on the arterial wall by the lower edge of the falx.18
Autologous wrap materials that have been discussed in theliterature include pericranium, dura mater, muscle, and fascia.
Autologous materials are easily obtained and can be used inprocedures that are time-sensitive.19 Muscle, dura, and fascia
adhere fairly well to the vessel wall but subsequently
reabsorb in situ, with little granulation tissue formation orfibrosis.20,21 This suggests poor long-term support of the
aneurysm wall. On the other hand, nonautologous materials,such as Bemsheet in particular, show superior adhesion and
proliferation of collagen fibers surrounding the vessel, sug-gesting greater protection against rupture or rerupture of the
aneurysm.20,21 Other nonautologous materials include muslin,gelatin sponge, gauze, hemashield, Teflon, silastic sheet, fibers,
fibrin glue, plastics, silicone, resins, vinyl polymers, andcyanoacrylate adhesives.21
The fibrosis induced by a nonautologous wrap is thought to
protect against late, but not early, rebleeding.21 However,nonautologous materials are also associated with many
www.WORLDNEUROSURGERY.org 43
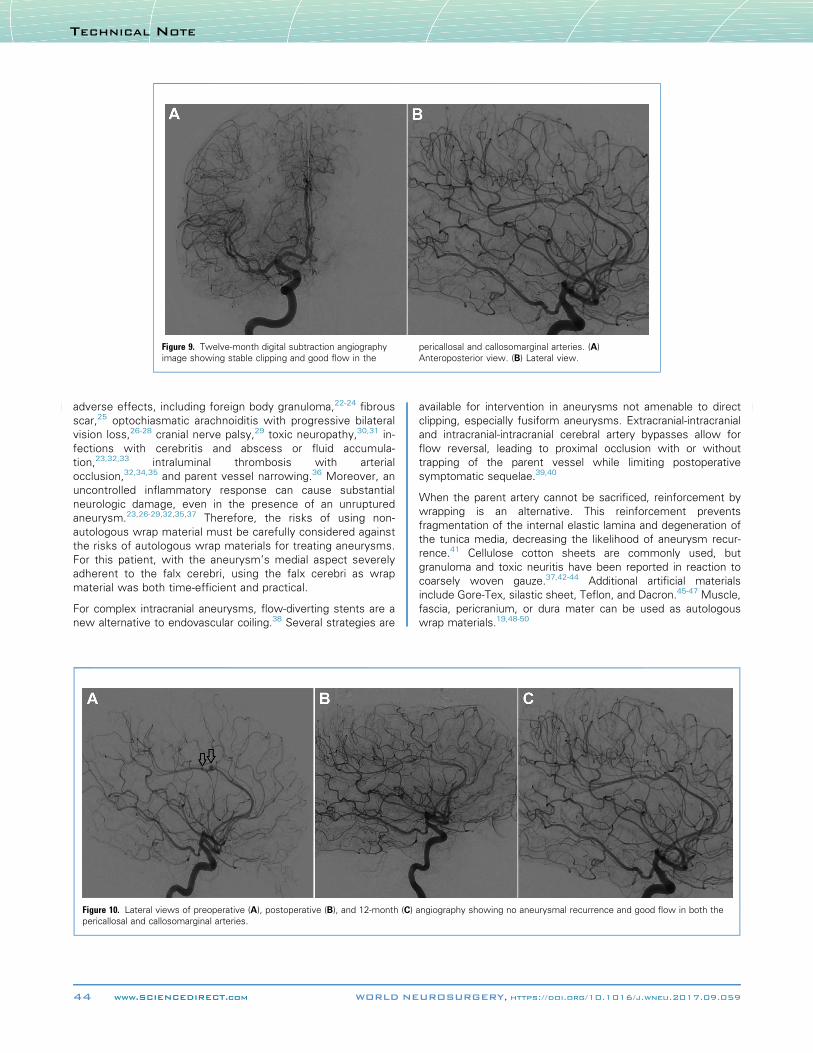
Figure 9. Twelve-month digital subtraction angiographyimage showing stable clipping and good flow in the
pericallosal and callosomarginal arteries. (A)Anteroposterior view. (B) Lateral view.
TECHNICAL NOTE
adverse effects, including foreign body granuloma,22-24 fibrous
scar,25 optochiasmatic arachnoiditis with progressive bilateralvision loss,26-28 cranial nerve palsy,29 toxic neuropathy,30,31 in-
fections with cerebritis and abscess or fluid accumula-tion,23,32,33 intraluminal thrombosis with arterial
occlusion,32,34,35 and parent vessel narrowing.36 Moreover, anuncontrolled inflammatory response can cause substantial
neurologic damage, even in the presence of an unrupturedaneurysm.23,26-29,32,35,37 Therefore, the risks of using non-
autologous wrap material must be carefully considered againstthe risks of autologous wrap materials for treating aneurysms.
For this patient, with the aneurysm’s medial aspect severelyadherent to the falx cerebri, using the falx cerebri as wrap
material was both time-efficient and practical.
For complex intracranial aneurysms, flow-diverting stents are anew alternative to endovascular coiling.38 Several strategies are
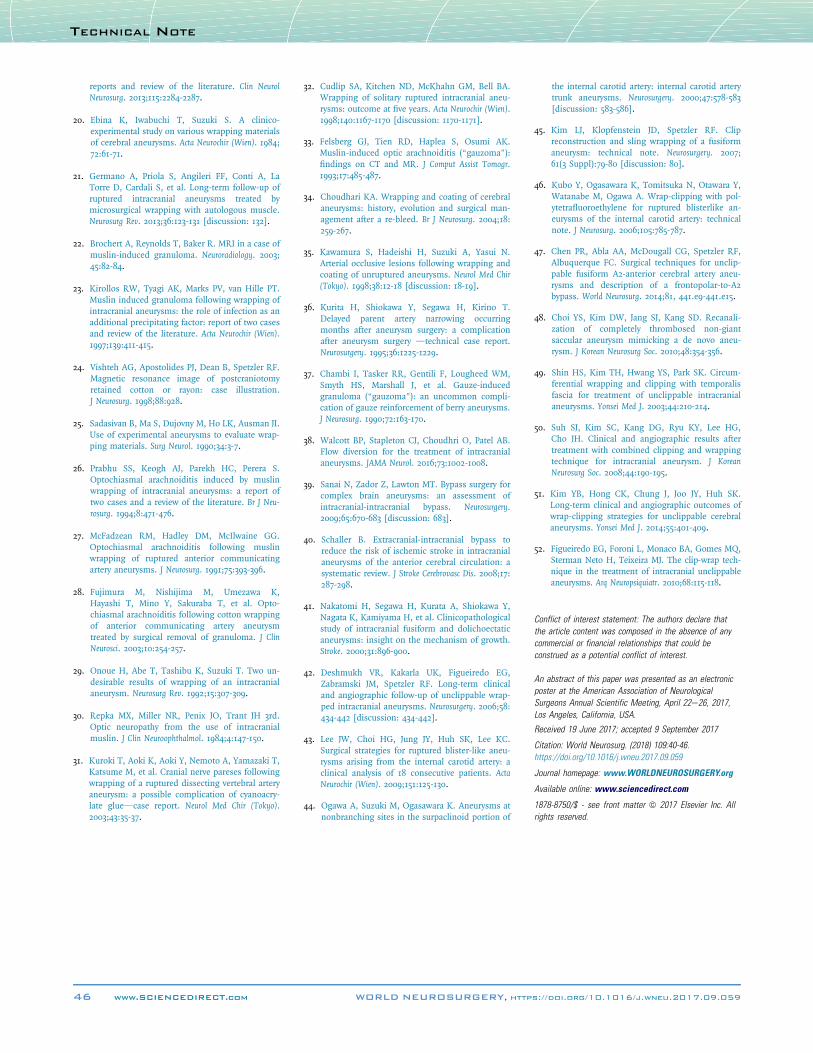
Figure 10. Lateral views of preoperative (A), postoperative (B), and 12-month (C)pericallosal and callosomarginal arteries.
44 www.SCIENCEDIRECT.com WORLD NE
available for intervention in aneurysms not amenable to direct
clipping, especially fusiform aneurysms. Extracranial-intracranialand intracranial-intracranial cerebral artery bypasses allow for
flow reversal, leading to proximal occlusion with or withouttrapping of the parent vessel while limiting postoperative
symptomatic sequelae.39,40
When the parent artery cannot be sacrificed, reinforcement bywrapping is an alternative. This reinforcement prevents
fragmentation of the internal elastic lamina and degeneration ofthe tunica media, decreasing the likelihood of aneurysm recur-
rence.41 Cellulose cotton sheets are commonly used, butgranuloma and toxic neuritis have been reported in reaction to
coarsely woven gauze.37,42-44 Additional artificial materialsinclude Gore-Tex, silastic sheet, Teflon, and Dacron.45-47 Muscle,
fascia, pericranium, or dura mater can be used as autologouswrap materials.19,48-50
angiography showing no aneurysmal recurrence and good flow in both the
UROSURGERY, https://doi.org/10.1016/j.wneu.2017.09.059

Figure 11. Anteroposterior views of preoperative (A),postoperative (B), and 12-month (C) angiography
showing no aneurysmal recurrence and good flow inboth the pericallosal and callosomarginal arteries.
TECHNICAL NOTE
One case series by Kim et al.51 examined longitudinal
outcomes following wrap-clipping with cellulose cotton fab-ric in 24 patients, 10 of whom had fusiform aneurysms. The
authors reported that 87.5% had either healed or stableaneurysms at a 10- to 75-month follow-up.51 Another 9-patient
series reported by Figueiredo et al.52 with 33% fusiformaneurysms used Rayon for wrap-clipping ruptured aneu-
rysms and reported no rebleeding at 2-year mean follow-up(range, 1 month to 3 years). Finally, Cudlip et al.32 explored
wrap-clipping in 15 patients with solitary ruptured aneu-rysms, and found no rebleeding at 1- and 4-year follow-ups
and a Glasgow outcome score of 4 or 5, excluding 1patient from the latter group who died due to myocardial
infarction.
WORLD NEUROSURGERY 109: 40-46, JANUARY 2018
CONCLUSIONSThe inferior thin part of the falx cerebri can safely be used as anautologous material for wrap-clipping of ruptured fusiform anterior
cerebral artery aneurysms, without compromising blood flowthrough the ACA. The length of wrap material used should be
carefully considered, because too short a graft could predispose thepatient to rerupture, and too long a graft could predispose to arterial
stenosis. In this case, an 8 � 8 mm section of the falx was suc-cessfully used to wrap the falx-adherent pericallosal artery without
aneurysm rebleed or recurrence over a 12-month follow-up period.This technique has been termed “falxuplication” to emphasize its
origin and purpose, and to avoid conflict with other techniques. Amultiarm randomized controlled trial comparing falx cerebri with
dura and nonautologous materials is warranted.
REFERENCES
1. Vlak MH, Algra A, Brandenburg R, Rinkel GJ.Prevalence of unruptured intracranial aneurysms,with emphasis on sex, age, comorbidity, country,and time period: a systematic review and meta-analysis. Lancet Neurol. 2011;10:626-636.
2. Rinkel GJ, Djibuti M, Algra A, van Gijn J. Preva-lence and risk of rupture of intracranial aneu-rysms: a systematic review. Stroke. 1998;29:251-256.
3. Vernooij MW, Ikram MA, Tanghe HL, Vincent AJ,Hofman A, Krestin GP, et al. Incidental findingson brain MRI in the general population. N Engl JMed. 2007;357:1821-1828.
4. Ingall T, Asplund K, Mähönen M, Bonita R.A multinational comparison of subarachnoidhemorrhage epidemiology in the WHO MONICAstroke study. Stroke. 2000;31:1054-1061.
5. Diringer MN. Management of aneurysmal sub-arachnoid hemorrhage. Crit Care Med. 2009;37:432-440.
6. Zacharia BE, Hickman ZL, Grobelny BT,DeRosa P, Kotchetkov I, Ducruet AF, et al.Epidemiology of aneurysmal subarachnoid hem-orrhage. Neurosurg Clin N Am. 2010;21:221-233.
7. Daroff R, Jankovic J, Mazziotta J, Pomeroy S.Bradley’s Neurology in Clinical Practice. 7th ed. Phila-delphia: Elsevier; 2016.
8. al-Yamany M, Ross IB. Giant fusiform aneurysmof the middle cerebral artery: successful Hunter-ian ligation without distal bypass. Br J Neurosurg.1998;12:572-575.
9. Park SH, Yim MB, Lee CY, Kim E, Son EI. Intra-cranial fusiform aneurysms: its pathogenesis,clinical characteristics and managements. J KoreanNeurosurg Soc. 2008;44:116-123.
10. Sacho RH, Saliou G, Kostynskyy A, Menezes R,Tymianski M, Krings T, et al. Natural history andoutcome after treatment of unruptured intraduralfusiform aneurysms. Stroke. 2014;45:3251-3256.
11. Day AL, Gaposchkin CG, Yu CJ, Rivet DJ,Dacey RG Jr. Spontaneous fusiform middle cere-bral artery aneurysms: characteristics and a pro-posed mechanism of formation. J Neurosurg. 2003;99:228-240.
12. Safavi-Abbasi S, Kalani MY, Frock B, Sun H,Yagmurlu K, Moron F, et al. Techniques andoutcomes of microsurgical management ofruptured and unruptured fusiform cerebral aneu-rysms. J Neurosurg. 2017:1-8.
13. Anson JA, Lawton MT, Spetzler RF. Characteris-tics and surgical treatment of dolichoectatic andfusiform aneurysms. J Neurosurg. 1996;84:185-193.
14. Katsuno M, Murai Y, Teramoto A. Acute subduralhematoma without subarachnoid hemorrhagefollowing rupture of a distal anterior cerebral ar-tery aneurysm: a case report. No To Shinkei. 2003;55:435-438 [in Japanese].
15. Lee JW, Lee KC, Kim YB, Huh SK. Surgery fordistal anterior cerebral artery aneurysms. SurgNeurol. 2008;70:153-159 [discussion: 159].
16. Jinkins JR. Atlas of Neuroradiologic Embryology,Anatomy, and Variants. Phildelphia: LippincottWilliams & Wilkins; 2000.
17. Zimmerman RD, Yurberg E, Russell EJ, Leeds NE.Falx and interhemispheric fissure on axial CT: I.Normal anatomy. AJR Am J Roentgenol. 1982;138:899-904.
18. Yuge T, Shigemori M, Tokutomi T, Kuga S,Kuramoto S. Diffuse axonal injury associated withmultiple traumatic aneurysms of the distal ante-rior cerebral artery: case report. Neurol Med Chir(Tokyo). 1990;30:412-416.
19. Feng YG, Li SF, Zhang PN, Xin T, Meng QH,Tang WZ, et al. Clip-on-wrapping with dura materto treat intracranial aneurysm neck avulsion: case
www.WORLDNEUROSURGERY.org 45
TECHNICAL NOTE
reports and review of the literature. Clin NeurolNeurosurg. 2013;115:2284-2287.
20. Ebina K, Iwabuchi T, Suzuki S. A clinico-experimental study on various wrapping materialsof cerebral aneurysms. Acta Neurochir (Wien). 1984;72:61-71.
21. Germano A, Priola S, Angileri FF, Conti A, LaTorre D, Cardali S, et al. Long-term follow-up ofruptured intracranial aneurysms treated bymicrosurgical wrapping with autologous muscle.Neurosurg Rev. 2013;36:123-131 [discussion: 132].
22. Brochert A, Reynolds T, Baker R. MRI in a case ofmuslin-induced granuloma. Neuroradiology. 2003;45:82-84.
23. Kirollos RW, Tyagi AK, Marks PV, van Hille PT.Muslin induced granuloma following wrapping ofintracranial aneurysms: the role of infection as anadditional precipitating factor: report of two casesand review of the literature. Acta Neurochir (Wien).1997;139:411-415.
24. Vishteh AG, Apostolides PJ, Dean B, Spetzler RF.Magnetic resonance image of postcraniotomyretained cotton or rayon: case illustration.J Neurosurg. 1998;88:928.
25. Sadasivan B, Ma S, Dujovny M, Ho LK, Ausman JI.Use of experimental aneurysms to evaluate wrap-ping materials. Surg Neurol. 1990;34:3-7.
26. Prabhu SS, Keogh AJ, Parekh HC, Perera S.Optochiasmal arachnoiditis induced by muslinwrapping of intracranial aneurysms: a report oftwo cases and a review of the literature. Br J Neu-rosurg. 1994;8:471-476.
27. McFadzean RM, Hadley DM, McIlwaine GG.Optochiasmal arachnoiditis following muslinwrapping of ruptured anterior communicatingartery aneurysms. J Neurosurg. 1991;75:393-396.
28. Fujimura M, Nishijima M, Umezawa K,Hayashi T, Mino Y, Sakuraba T, et al. Opto-chiasmal arachnoiditis following cotton wrappingof anterior communicating artery aneurysmtreated by surgical removal of granuloma. J ClinNeurosci. 2003;10:254-257.
29. Onoue H, Abe T, Tashibu K, Suzuki T. Two un-desirable results of wrapping of an intracranialaneurysm. Neurosurg Rev. 1992;15:307-309.
30. Repka MX, Miller NR, Penix JO, Trant JH 3rd.Optic neuropathy from the use of intracranialmuslin. J Clin Neuroophthalmol. 1984;4:147-150.
31. Kuroki T, Aoki K, Aoki Y, Nemoto A, Yamazaki T,Katsume M, et al. Cranial nerve pareses followingwrapping of a ruptured dissecting vertebral arteryaneurysm: a possible complication of cyanoacry-late gluedcase report. Neurol Med Chir (Tokyo).2003;43:35-37.
46 www.SCIENCEDIRECT.com
32. Cudlip SA, Kitchen ND, McKhahn GM, Bell BA.Wrapping of solitary ruptured intracranial aneu-rysms: outcome at five years. Acta Neurochir (Wien).1998;140:1167-1170 [discussion: 1170-1171].
33. Felsberg GJ, Tien RD, Haplea S, Osumi AK.Muslin-induced optic arachnoiditis (“gauzoma”):findings on CT and MR. J Comput Assist Tomogr.1993;17:485-487.
34. Choudhari KA. Wrapping and coating of cerebralaneurysms: history, evolution and surgical man-agement after a re-bleed. Br J Neurosurg. 2004;18:259-267.
35. Kawamura S, Hadeishi H, Suzuki A, Yasui N.Arterial occlusive lesions following wrapping andcoating of unruptured aneurysms. Neurol Med Chir(Tokyo). 1998;38:12-18 [discussion: 18-19].
36. Kurita H, Shiokawa Y, Segawa H, Kirino T.Delayed parent artery narrowing occurringmonths after aneurysm surgery: a complicationafter aneurysm surgery dtechnical case report.Neurosurgery. 1995;36:1225-1229.
37. Chambi I, Tasker RR, Gentili F, Lougheed WM,Smyth HS, Marshall J, et al. Gauze-inducedgranuloma (“gauzoma”): an uncommon compli-cation of gauze reinforcement of berry aneurysms.J Neurosurg. 1990;72:163-170.
38. Walcott BP, Stapleton CJ, Choudhri O, Patel AB.Flow diversion for the treatment of intracranialaneurysms. JAMA Neurol. 2016;73:1002-1008.
39. Sanai N, Zador Z, Lawton MT. Bypass surgery forcomplex brain aneurysms: an assessment ofintracranial-intracranial bypass. Neurosurgery.2009;65:670-683 [discussion: 683].
40. Schaller B. Extracranial-intracranial bypass toreduce the risk of ischemic stroke in intracranialaneurysms of the anterior cerebral circulation: asystematic review. J Stroke Cerebrovasc Dis. 2008;17:287-298.
41. Nakatomi H, Segawa H, Kurata A, Shiokawa Y,Nagata K, Kamiyama H, et al. Clinicopathologicalstudy of intracranial fusiform and dolichoectaticaneurysms: insight on the mechanism of growth.Stroke. 2000;31:896-900.
42. Deshmukh VR, Kakarla UK, Figueiredo EG,Zabramski JM, Spetzler RF. Long-term clinicaland angiographic follow-up of unclippable wrap-ped intracranial aneurysms. Neurosurgery. 2006;58:434-442 [discussion: 434-442].
43. Lee JW, Choi HG, Jung JY, Huh SK, Lee KC.Surgical strategies for ruptured blister-like aneu-rysms arising from the internal carotid artery: aclinical analysis of 18 consecutive patients. ActaNeurochir (Wien). 2009;151:125-130.
44. Ogawa A, Suzuki M, Ogasawara K. Aneurysms atnonbranching sites in the surpaclinoid portion of
WORLD NEUROSURGERY, http
the internal carotid artery: internal carotid arterytrunk aneurysms. Neurosurgery. 2000;47:578-583[discussion: 583-586].
45. Kim LJ, Klopfenstein JD, Spetzler RF. Clipreconstruction and sling wrapping of a fusiformaneurysm: technical note. Neurosurgery. 2007;61(3 Suppl):79-80 [discussion: 80].
46. Kubo Y, Ogasawara K, Tomitsuka N, Otawara Y,Watanabe M, Ogawa A. Wrap-clipping with pol-ytetrafluoroethylene for ruptured blisterlike an-eurysms of the internal carotid artery: technicalnote. J Neurosurg. 2006;105:785-787.
47. Chen PR, Abla AA, McDougall CG, Spetzler RF,Albuquerque FC. Surgical techniques for unclip-pable fusiform A2-anterior cerebral artery aneu-rysms and description of a frontopolar-to-A2bypass. World Neurosurg. 2014;81, 441.e9-441.e15.
48. Choi YS, Kim DW, Jang SJ, Kang SD. Recanali-zation of completely thrombosed non-giantsaccular aneurysm mimicking a de novo aneu-rysm. J Korean Neurosurg Soc. 2010;48:354-356.
49. Shin HS, Kim TH, Hwang YS, Park SK. Circum-ferential wrapping and clipping with temporalisfascia for treatment of unclippable intracranialaneurysms. Yonsei Med J. 2003;44:210-214.
50. Suh SJ, Kim SC, Kang DG, Ryu KY, Lee HG,Cho JH. Clinical and angiographic results aftertreatment with combined clipping and wrappingtechnique for intracranial aneurysm. J KoreanNeurosurg Soc. 2008;44:190-195.
51. Kim YB, Hong CK, Chung J, Joo JY, Huh SK.Long-term clinical and angiographic outcomes ofwrap-clipping strategies for unclippable cerebralaneurysms. Yonsei Med J. 2014;55:401-409.
52. Figueiredo EG, Foroni L, Monaco BA, Gomes MQ,Sterman Neto H, Teixeira MJ. The clip-wrap tech-nique in the treatment of intracranial unclippableaneurysms. Arq Neuropsiquiatr. 2010;68:115-118.
Conflict of interest statement: The authors declare thatthe article content was composed in the absence of anycommercial or financial relationships that could beconstrued as a potential conflict of interest.
An abstract of this paper was presented as an electronicposter at the American Association of NeurologicalSurgeons Annual Scientific Meeting, April 22e26, 2017,Los Angeles, California, USA.
Received 19 June 2017; accepted 9 September 2017
Citation: World Neurosurg. (2018) 109:40-46.https://doi.org/10.1016/j.wneu.2017.09.059
Journal homepage: www.WORLDNEUROSURGERY.org
Available online: www.sciencedirect.com
1878-8750/$ - see front matter ª 2017 Elsevier Inc. Allrights reserved.
s://doi.org/10.1016/j.wneu.2017.09.059