Embed Size (px)
Citation preview

Failure to Implement Respiratory Isolation: Why Does It Happen? • Author(s): Kentaro Iwata , MD; Barbara A. Smith , RN, MPA; Eloisa Santos , RN, MEd; BrucePolsky , MD; Emilia M. Sordillo , MD, PhDSource: Infection Control and Hospital Epidemiology, Vol. 23, No. 10 (October 2002), pp. 595-599Published by: The University of Chicago Press on behalf of The Society for Healthcare Epidemiologyof AmericaStable URL: http://www.jstor.org/stable/10.1086/501977 .
Accessed: 14/05/2014 08:54
Your use of the JSTOR archive indicates your acceptance of the Terms & Conditions of Use, available at .http://www.jstor.org/page/info/about/policies/terms.jsp
.JSTOR is a not-for-profit service that helps scholars, researchers, and students discover, use, and build upon a wide range ofcontent in a trusted digital archive. We use information technology and tools to increase productivity and facilitate new formsof scholarship. For more information about JSTOR, please contact [email protected].
.
The University of Chicago Press and The Society for Healthcare Epidemiology of America are collaboratingwith JSTOR to digitize, preserve and extend access to Infection Control and Hospital Epidemiology.
http://www.jstor.org
This content downloaded from 193.104.110.108 on Wed, 14 May 2014 08:54:09 AMAll use subject to JSTOR Terms and Conditions

Vol. 23 No. 10 INFECTION CONTROL AND HOSPITAL EPIDEMIOLOGY 595
FAILURE TO IMPLEMENT RESPIRATORY ISOLATION:WHY DOES IT HAPPEN?
Kentaro Iwata, MD; Barbara A. Smith, RN, MPA; Eloisa Santos, RN, MEd; Bruce Polsky, MD; Emilia M. Sordillo, MD, PhD
BACKGROUND: Respiratory isolation for 90% of individu-als with acid-fast bacillus (AFB)-smear–positive tuberculosis (TB)is a recommended performance indicator in recent InfectiousDiseases Society of America and Centers for Disease Control andPrevention guidelines. However, compliance with respiratory iso-lation reported from multiple centers in the United States andEurope falls short of that goal.
OBJECTIVE: To identify missed clues in TB patients whoare not appropriately isolated.
DESIGN: Retrospective survey.SETTING: A 900-bed voluntary hospital.PATIENTS: All patients with AFB-smear–positive TB
admitted between January 1995 and December 1999 who were notappropriately isolated.
RESULTS: There were 173 TB cases admitted, including106 with pulmonary TB. AFB smears were positive in 82 cases; 24(29%) of these were not appropriately isolated. During the study
period, the number of TB cases declined, but the proportion ofappropriately isolated patients did not change. Most isolation fail-ure cases were men (median age, 45.5 years); 21 of these patientswere black, 2 were Hispanic white, and 1 was Asian, but none wasnon-Hispanic white. All isolation failure cases had at least one char-acteristic predictive of TB that could have been elicited at admis-sion (eg, abnormal chest radiograph findings consistent with TB,fever, weight loss, a history of TB, a positive result on tuberculinskin test, hemoptysis, and human immunodeficiency virus infec-tion).
CONCLUSION: Consistent with experiences at other hos-pitals, we found that the rate of isolation failure remainedunchanged despite an overall decline in TB cases. In our experi-ence, almost all isolation failures could be avoided by carefulreview of the history, physical examination, and chest radiographfor characteristics classically considered predictive of TB (InfectControl Hosp Epidemiol 2002;23:595-599).
In the early 1990s, there were multiple reports oftransmission of tuberculosis (TB) in healthcare settings inthe United States.1-6 Coupled with the emergence of mul-tidrug-resistant strains of Mycobacterium tuberculosis, theseoutbreaks contributed to a frightening increase in TBcases. In response, the Centers for Disease Control andPrevention (CDC) provided several guidelines.7-9 However,nosocomial TB outbreaks were reported even after theseguidelines were published.10,11
It is well established that TB transmission occurswhen patients have not been placed in, or do not adhere to,respiratory isolation.10,11 Prompt and adequate isolation ofindividuals suspected of having TB is one of the mostimportant measures to reduce the risk of nosocomialtransmission.7 A recent report has highlighted that TBtransmission can occur despite fit testing and the availabil-ity of personal protective devices such as particulate air fil-ters in the absence of isolation of patients with TB in neg-ative-pressure ventilation isolation rooms.10 In recentguidelines from the Infectious Diseases Society of Americaand the CDC,12 respiratory isolation for 90% of individualswith acid-fast bacillus (AFB)-smear–positive TB is a rec-
ommended performance indicator. However, in reportsfrom multiple centers in the United States and Europe,adherence to respiratory isolation has ranged from 47% to88% (Table 1).
Although our institution has an aggressive isolationpolicy and a “rule-out” ratio of isolated patients without TBto those with TB (rule-out ratio = 14.1:1 during a prospec-tive study in 1995–1996)18 that is similar to those reportedby other institutions (8:119,20 to 12:121), we recently notedseveral failures to isolate patients later found to have AFB-smear–positive TB. We therefore reviewed all cases duringthe previous 5 years in which airborne precautions or res-piratory isolation were not instituted promptly, to identifycommon and potentially correctable factors.
METHODS
This study was performed in compliance with insti-tutional, federal, and local guidelines for human subjectresearch. We used infection control and laboratory recordsto identify all patients with AFB-smear–positive TB admit-ted to the St. Luke’s Division of St. Luke’s-RooseveltHospital Center between January 1995 and December
Drs. Iwata, Polsky, and Sordillo are from the Department of Medicine; Drs. Polsky and Sordillo, Ms. Smith, and Ms. Santos are from the Divisionof Infectious Diseases and Epidemiology; and Dr. Sordillo is from the Department of Pathology and Laboratory Medicine, St. Luke’s-Roosevelt HospitalCenter, College of Physicians & Surgeons, Columbia University, New York, New York.
Address reprint requests to Emilia M. Sordillo, MD, PhD, St. Luke’s-Roosevelt Hospital Center, 1111 Amsterdam Avenue, New York, NY 10025.Presented in part at the 11th Annual Meeting of the Society for Healthcare Epidemiology of America; April 1-3, 2001; Toronto, Ontario, Canada.
ABSTRACT
This content downloaded from 193.104.110.108 on Wed, 14 May 2014 08:54:09 AMAll use subject to JSTOR Terms and Conditions
596 INFECTION CONTROL AND HOSPITAL EPIDEMIOLOGY October 2002
1999. Data collected included admission date and time;admitting diagnosis; symptoms of fever, cough, and hemop-tysis; weight loss; human immunodeficiency virus (HIV)infection status; purified protein derivative tuberculin skintest (TST) status; bacille Calmette–Guérin vaccination sta-tus; immigration status; race; housing status; family histo-ry; chest radiograph; basic blood counts and chemistries atadmission; and promptness of isolation. Laboratoryrecords were reviewed to identify all patients with culture-positive TB.
An isolation failure case was defined as a patient withan AFB-smear–positive sputum or other respiratory speci-men from which M. tuberculosis was isolated, but for whomrespiratory isolation or airborne precautions were not insti-tuted at the time of the initial interaction in the emergencydepartment or at admission.
Following recognition of an isolation failure case,possible nosocomial transmission was evaluated. Allexposed healthcare workers with negative two-step TSTresults at baseline were evaluated by TST immediately afterrecognition of the exposure and 10 to 12 weeks later.Exposed healthcare workers with positive TST results atbaseline were evaluated for symptoms and by chest radi-ograph as indicated during the same period. Exposedpatients and families were notified through the attending orhouse staff physician and evaluated by TST at baseline and10 to 12 weeks; follow-up was requested at 6 and 12 monthsfrom each patient’s physician.
RESULTS
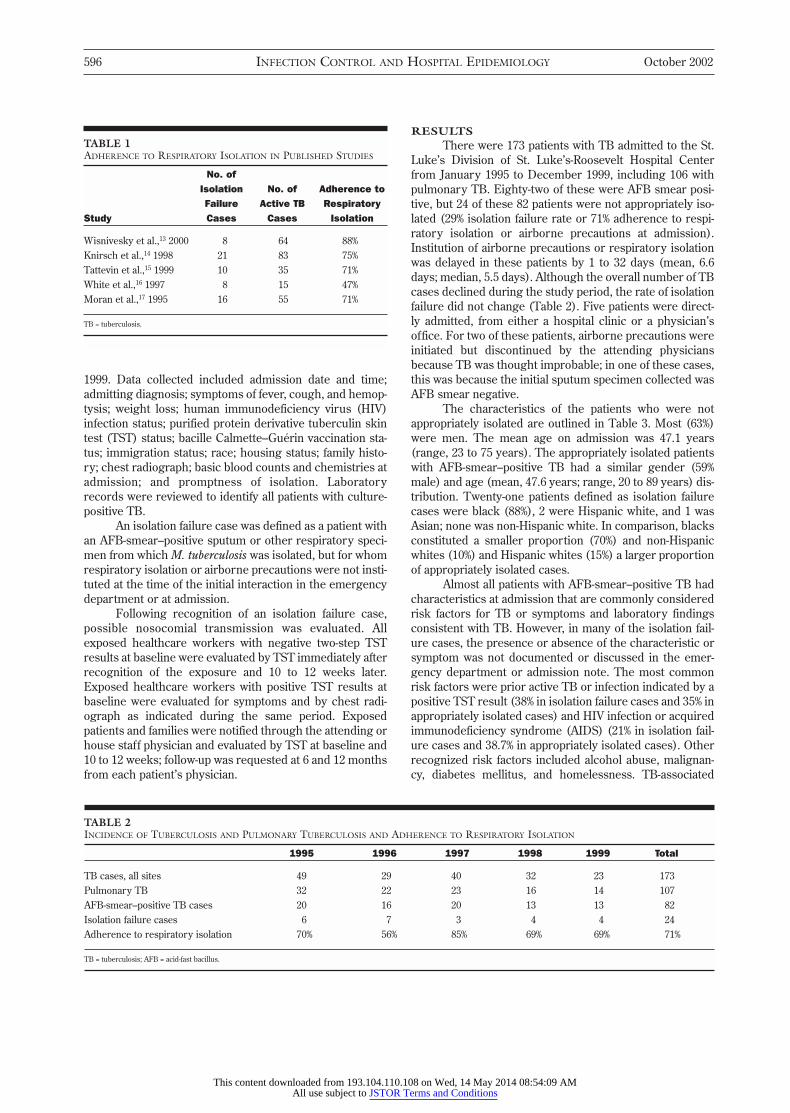
There were 173 patients with TB admitted to the St.Luke’s Division of St. Luke’s-Roosevelt Hospital Centerfrom January 1995 to December 1999, including 106 withpulmonary TB. Eighty-two of these were AFB smear posi-tive, but 24 of these 82 patients were not appropriately iso-lated (29% isolation failure rate or 71% adherence to respi-ratory isolation or airborne precautions at admission).Institution of airborne precautions or respiratory isolationwas delayed in these patients by 1 to 32 days (mean, 6.6days; median, 5.5 days). Although the overall number of TBcases declined during the study period, the rate of isolationfailure did not change (Table 2). Five patients were direct-ly admitted, from either a hospital clinic or a physician’soffice. For two of these patients, airborne precautions wereinitiated but discontinued by the attending physiciansbecause TB was thought improbable; in one of these cases,this was because the initial sputum specimen collected wasAFB smear negative.
The characteristics of the patients who were notappropriately isolated are outlined in Table 3. Most (63%)were men. The mean age on admission was 47.1 years(range, 23 to 75 years). The appropriately isolated patientswith AFB-smear–positive TB had a similar gender (59%male) and age (mean, 47.6 years; range, 20 to 89 years) dis-tribution. Twenty-one patients defined as isolation failurecases were black (88%), 2 were Hispanic white, and 1 wasAsian; none was non-Hispanic white. In comparison, blacksconstituted a smaller proportion (70%) and non-Hispanicwhites (10%) and Hispanic whites (15%) a larger proportionof appropriately isolated cases.
Almost all patients with AFB-smear–positive TB hadcharacteristics at admission that are commonly consideredrisk factors for TB or symptoms and laboratory findingsconsistent with TB. However, in many of the isolation fail-ure cases, the presence or absence of the characteristic orsymptom was not documented or discussed in the emer-gency department or admission note. The most commonrisk factors were prior active TB or infection indicated by apositive TST result (38% in isolation failure cases and 35% inappropriately isolated cases) and HIV infection or acquiredimmunodeficiency syndrome (AIDS) (21% in isolation fail-ure cases and 38.7% in appropriately isolated cases). Otherrecognized risk factors included alcohol abuse, malignan-cy, diabetes mellitus, and homelessness. TB-associated
TABLE 1ADHERENCE TO RESPIRATORY ISOLATION IN PUBLISHED STUDIES
No. of Isolation No. of Adherence to Failure Active TB Respiratory
Study Cases Cases Isolation
Wisnivesky et al.,13 2000 8 64 88%Knirsch et al.,14 1998 21 83 75%Tattevin et al.,15 1999 10 35 71%White et al.,16 1997 8 15 47%Moran et al.,17 1995 16 55 71%
TB = tuberculosis.
TABLE 2INCIDENCE OF TUBERCULOSIS AND PULMONARY TUBERCULOSIS AND ADHERENCE TO RESPIRATORY ISOLATION
1995 1996 1997 1998 1999 Total
TB cases, all sites 49 29 40 32 23 173Pulmonary TB 32 22 23 16 14 107AFB-smear–positive TB cases 20 16 20 13 13 82Isolation failure cases 6 7 3 4 4 24Adherence to respiratory isolation 70% 56% 85% 69% 69% 71%
TB = tuberculosis; AFB = acid-fast bacillus.
This content downloaded from 193.104.110.108 on Wed, 14 May 2014 08:54:09 AMAll use subject to JSTOR Terms and Conditions

Vol. 23 No. 10 FAILURE TO IMPLEMENT RESPIRATORY ISOLATION 597
symptoms common among isolation failure cases werefever (63%), weight loss (58%), and cough (42%); othersymptoms included dyspnea and hemoptysis. Only 4 isola-tion failure cases did not have any of these symptoms atadmission.
Abnormal findings on chest radiograph consistentwith a diagnosis of TB were common in both appropriatelyisolated cases (93%) and isolation failure cases (92%).However, in contrast to appropriately isolated patients, forwhom the abnormal findings on chest radiograph were rec-ognized in the emergency department or at admission, theabnormal findings on chest radiograph were recognized atadmission for only 13 (54%) of the patients with isolationfailure. Surprisingly, for 7 (29%) of the isolation failurecases, a chest radiograph either was not ordered at admis-sion or was not read in the emergency department. In 5 iso-lation failure cases (21%), the final chest radiograph read-ing differed from the initial reading.
During the study period, there were 6 patients withAFB-smear–positive TB who had normal findings on chestradiograph; all were HIV positive. Although HIV status wasknown for only 5 patients at admission, the sixth patientwas noted to have other TB risk factors, including home-lessness and ethanol abuse. Four of these patients wereappropriately isolated based on documented recognition ofa history of TB or a positive TST result, or symptoms sug-gestive of TB. In the 2 of these cases that were isolation fail-ures, the significance of symptoms suggestive of TBdespite normal findings on chest radiograph was not rec-ognized.
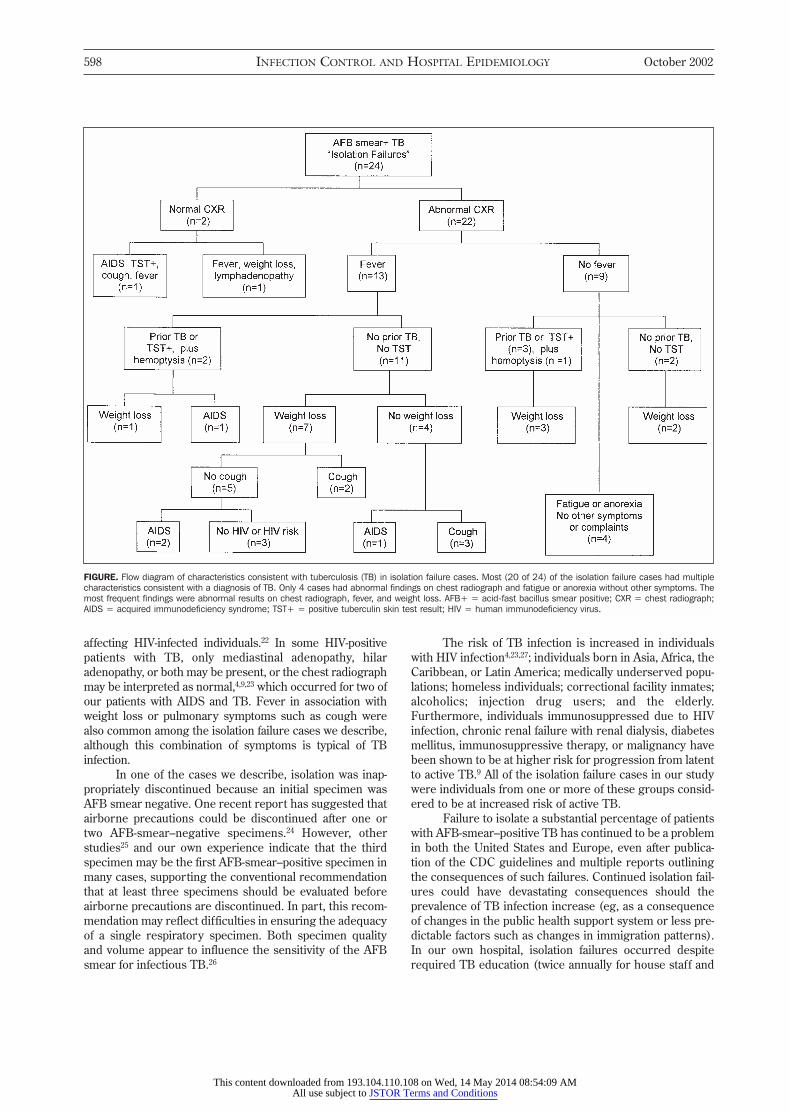
Most (20 of 24) of the isolation failure cases had mul-tiple characteristics classically considered consistent withTB (Figure), and thus could potentially have been recog-nized at the initial encounter. If these patients had been iso-lated, overall adherence to respiratory isolation at our insti-tution would have been 95%, rather than 71%. In the 4remaining cases, represented by the box in the lower rightcorner of the figure, the chest radiograph findings wereabnormal (cystic air disease, upper lobe density, bilateralground-glass infiltrates, and extensive bilateral infiltrates)and potentially consistent with TB. However, althoughthese 4 patients complained of anorexia and malaise, theywere without fever, respiratory symptoms, or known HIVrisk factors. In the absence of other TB risk factors or sug-gestive symptoms, it is unlikely that airborne precautionswould have been instituted for these patients.
A review of infection control records indicated thatthere were no cases of nosocomial TB transmission orhealthcare worker TST conversions attributable to theseisolation failures.
DISCUSSION
In reports of TB transmission in hospitals and otherhealthcare settings, the failure to isolate one or more infec-tious patients is a common theme. Thus, a high index ofsuspicion for TB and rapid institution of respiratory isola-tion or airborne precautions have been prominent amongrecommendations for prevention of TB.7,9 In recent guide-
lines, a target of respiratory isolation for 90% or more ofindividuals infected with AFB-smear–positive TB is recom-mended by the CDC.12
However, reports from several institutions in a vari-ety of settings suggest that adherence to this performanceindicator is rarely achieved.13-17 Although those reportshave not specifically examined the characteristics of thepatients with AFB-smear–positive TB who were not isolat-ed, several have addressed patient characteristics that areassociated with prompt institution of isolation. A chest radi-ograph consistent with TB and complaints of fever, cough,and weight loss were the factors most often associated withprompt isolation in several studies. We also found thatrecognition of a chest radiograph consistent with TB or ofsymptoms consistent with TB in patients with normal find-ings on chest radiograph led to appropriate isolation.
Similarly, in our current study, failure to obtain a chestradiograph and a delayed response to abnormal findings onchest radiograph were overwhelmingly the most commonelements among patients with AFB-smear–positive TB whowere not appropriately isolated. Failure to recognize thatchest radiograph findings are consistent with TB is welldescribed in reports of TB outbreaks, particularly those
TABLE 3CHARACTERISTICS OF PATIENTS WITH ACID-FAST BACILLUS-SMEAR–POSITIVE TUBERCULOSIS WHO WERE NOT APPROPRIATELY
ISOLATED (N = 24)
Characteristic No. of Cases (%%)
Mean age, y (range) 47.1 (23 to 75)Gender (male:female) 15:9Risk factors
HIV/AIDS 5 (21)Prior TB 3 (13)PPD positive 3 (13)Diabetes 1 (4)Malignancy 3 (13)Alcoholism 3 (13)Black, Hispanic, or Asian 24 (100)Homeless or shelter resident 1 (4)Prison stay 0
SymptomsCough 10 (42)Fever (> 37.8°C or 100°F) 15 (63)Hemoptysis 3 (13)Night sweats 0 (0)Weight loss 14 (58)Shortness of breath 8 (33)No symptoms 4 (17)
Other findingsAbnormal chest radiograph findings 22 (92)WBC > 10,400/µL 3 (13)WBC < 4,700/µL 9 (38)
HIV = human immunodeficiency virus; AIDS = acquired immunodeficiency syndrome; PPD =purified protein derivative; WBC = white blood cell count.
This content downloaded from 193.104.110.108 on Wed, 14 May 2014 08:54:09 AMAll use subject to JSTOR Terms and Conditions
598 INFECTION CONTROL AND HOSPITAL EPIDEMIOLOGY October 2002
affecting HIV-infected individuals.22 In some HIV-positivepatients with TB, only mediastinal adenopathy, hilaradenopathy, or both may be present, or the chest radiographmay be interpreted as normal,4,9,23 which occurred for two ofour patients with AIDS and TB. Fever in association withweight loss or pulmonary symptoms such as cough werealso common among the isolation failure cases we describe,although this combination of symptoms is typical of TBinfection.
In one of the cases we describe, isolation was inap-propriately discontinued because an initial specimen wasAFB smear negative. One recent report has suggested thatairborne precautions could be discontinued after one ortwo AFB-smear–negative specimens.24 However, otherstudies25 and our own experience indicate that the thirdspecimen may be the first AFB-smear–positive specimen inmany cases, supporting the conventional recommendationthat at least three specimens should be evaluated beforeairborne precautions are discontinued. In part, this recom-mendation may reflect difficulties in ensuring the adequacyof a single respiratory specimen. Both specimen qualityand volume appear to influence the sensitivity of the AFBsmear for infectious TB.26
The risk of TB infection is increased in individualswith HIV infection4,23,27; individuals born in Asia, Africa, theCaribbean, or Latin America; medically underserved popu-lations; homeless individuals; correctional facility inmates;alcoholics; injection drug users; and the elderly.Furthermore, individuals immunosuppressed due to HIVinfection, chronic renal failure with renal dialysis, diabetesmellitus, immunosuppressive therapy, or malignancy havebeen shown to be at higher risk for progression from latentto active TB.9 All of the isolation failure cases in our studywere individuals from one or more of these groups consid-ered to be at increased risk of active TB.
Failure to isolate a substantial percentage of patientswith AFB-smear–positive TB has continued to be a problemin both the United States and Europe, even after publica-tion of the CDC guidelines and multiple reports outliningthe consequences of such failures. Continued isolation fail-ures could have devastating consequences should theprevalence of TB infection increase (eg, as a consequenceof changes in the public health support system or less pre-dictable factors such as changes in immigration patterns).In our own hospital, isolation failures occurred despiterequired TB education (twice annually for house staff and
FIGURE. Flow diagram of characteristics consistent with tuberculosis (TB) in isolation failure cases. Most (20 of 24) of the isolation failure cases had multiplecharacteristics consistent with a diagnosis of TB. Only 4 cases had abnormal findings on chest radiograph and fatigue or anorexia without other symptoms. Themost frequent findings were abnormal results on chest radiograph, fever, and weight loss. AFB+ = acid-fast bacillus smear positive; CXR = chest radiograph;AIDS = acquired immunodeficiency syndrome; TST+ = positive tuberculin skin test result; HIV = human immunodeficiency virus.
This content downloaded from 193.104.110.108 on Wed, 14 May 2014 08:54:09 AMAll use subject to JSTOR Terms and Conditions
Vol. 23 No. 10 FAILURE TO IMPLEMENT RESPIRATORY ISOLATION 599
annually for attending physicians), designation of a physi-cian–nurse team that reviews the management of TB andsuspected TB patients, and targeted feedback regardingisolation failures to physician and nursing staff. We are cur-rently expanding our TB education program to includecase-based sessions targeting attending physicians andhouse staff in the emergency department and theDepartment of Medicine and specifically addressing thecauses of each isolation failure in our hospital.
Factors that may explain the lack of nosocomialtransmission in association with these isolation failuresinclude the high baseline TST positivity (approximately30%) among healthcare workers and patients at our hospi-tal and the widespread implementation of improved engi-neering controls. These engineering controls included notonly increasing the number of respiratory isolation rooms(12 air exchanges per hour) and monitoring negative pres-sure, but also increasing air exchanges (6 to 8 airexchanges per hour) in the emergency department, wait-ing areas, hallways, and regular patient rooms. It has beensuggested that adequate ventilation can decrease the riskof TB transmission even in the absence of personal respi-ratory protection by minimizing the concentration of infec-tious aerosol.28
Our findings suggest that careful attention to the his-tory, physical examination, and chest radiograph, as well ascharacteristics classically considered predictive of TB, canprevent most isolation failures. The Infectious DiseasesSociety of America and the CDC performance indicator ofrespiratory isolation for 90% of cases with AFB-smear–pos-itive TB is an achievable goal.
REFERENCES 1. Pearson ML, Jereb JA, Frieden TR, et al. Nosocomial transmission of
multi-resistant Mycobacterium tuberculosis: a risk to patients and healthcare workers. Ann Intern Med 1992;117:191-196.
2. Centers for Disease Control and Prevention. Outbreak of multidrug-resistant tuberculosis at a hospital: New York City, 1991. MMWR1993;42:427-434.
3. Center for Disease Control. Nosocomial transmission of multidrug-resistant tuberculosis among HIV-infected persons: Florida and NewYork, 1988-1991. MMWR 1991;40:585-591.
4. Edlin BR, Tokars JI, Grieco MH, et al. An outbreak of multidrug-resis-tant tuberculosis among hospitalized patients with the acquired immun-odeficiency syndrome. N Engl J Med 1992;326:1514-1521.
5. Coronado VG, Beck-Sague CM, Hutton MD, et al. Transmission of mul-tidrug-resistant Mycobacterium tuberculosis among persons with humanimmunodeficiency virus infection in an urban hospital: epidemiologicand restriction fragment length polymorphism analysis. J Infect Dis1993;168:1052-1055.
6. Busillo CP, Lessnau KD, Sanjana V, et al. Multidrug resistant Myco-bacterium tuberculosis in patients with human immunodeficiency virusinfection. Chest 1992;102:797-801.
7. Center for Disease Control. Guidelines for preventing the transmissionof tuberculosis in health-care settings, with special focus on HIV-related
issues. MMWR 1990;39(RR-17):1-29.8. Center for Disease Control. Screening for tuberculosis and tuberculous
infection in high-risk populations: recommendations of the AdvisoryCommittee for Elimination of Tuberculosis. MMWR 1990;39(RR-8):1-7.
9. Centers for Disease Control and Prevention. Guidelines for preventingthe transmission of Mycobacterium tuberculosis in health-care facilities,1994. MMWR 1994;43(RR-13):1-132.
10. Kenyon TA, Ridzon R, Luskin-Hawk R, et al. A nosocomial outbreak ofmultidrug-resistant tuberculosis. Ann Intern Med 1997;127:32-36.
11. Nivin B, Nicholas P, Gayer M, Frieden TR, Fujiwara PI. A continuing out-break of multidrug-resistant tuberculosis, with transmission in a hospi-tal nursery. Clin Infect Dis 1998;26:303-307.
12. Horsburgh CR Jr, Feldman S, Ridzon R. Practice guidelines for the treat-ment of tuberculosis. Clin Infect Dis 2000;31:633-639.
13. Wisnivesky JP, Kaplan J, Henschke C, McGinn TG, Crystal RG.Evaluation of clinical parameters to predict Mycobacterium tuberculosisin inpatients. Arch Intern Med 2000;160:2471-2476.
14. Knirsch CA, Jain NL, Pablos-Mendez A, Friedman C, Hripcsak G.Respiratory isolation of tuberculosis patients using clinical guidelinesand an automated clinical decision support system. Infect Control HospEpidemiol 1998;19:94-100.
15. Tattevin P, Casalino E, Fleury L, Egmann G, Ruel M, Bouvet E. Thevalidity of medical history, classic symptoms, and chest radiographs inpredicting pulmonary tuberculosis: derivation of a pulmonary tubercu-losis prediction model. Chest 1999;115:1248-1253.
16. White AH, Khatib R, Riederer KM, Flood M. Respiratory isolation in ateaching hospital with low-to-moderate rate of tuberculosis: compliancewith Centers for Disease Control and Prevention guidelines for identify-ing patients who may have active tuberculosis. Am J Infect Control 1997;25:467-470.
17. Moran GJ, McCabe F, Morgan MT, Talan DA. Delayed recognition andinfection control for tuberculosis patients in the emergency department.Ann Emerg Med 1995;26:290-295.
18. Tokars JI, McKinley GF, Otten J, et al. Use and efficacy of TB infectioncontrol practices at hospitals with previous outbreaks of multidrug-resis-tant tuberculosis. Infect Control Hosp Epidemiol 2001;22:449-455.
19. Blumberg HM, Watkins DL, Berschling JD, et al. Preventing the noso-comial transmission of tuberculosis. Ann Intern Med 1995;122:658-663.
20. Bock NN, McGowan JE Jr, Ahn J, Tapia J, Blumberg HM. Clinical pre-dictors of tuberculosis as a guide for a respiratory isolation policy. Am JRespir Crit Care Med 1996;154:1468-1472.
21. Roy MC, Fredrickson M, Good NL, Hunter SA, Nettleman MD.Correlation between frequency of tuberculosis and compliance with con-trol strategies. Infect Control Hosp Epidemiol 1997;18:28-31.
22. Pitchenik AE, Rubinson HA. Radiographic appearance of tuberculosis inpatients with the acquired immune deficiency syndrome (AIDS) andpre-AIDS. American Review of Respiratory Disease 1985;131:393-396.
23. Selwyn PA, Hartel D, Lewis VA, et al. A prospective study of the risk oftuberculosis and intravenous drug users with human immunodeficiencyvirus infection. N Engl J Med 1989;320:545-550.
24. Craft DW, Jones MC, Blanchet CN, Hopfer RL. Value of examining threeacid-fast bacillus sputum smears for removal of patients suspected ofhaving tuberculosis from the “Airborne Precautions” category. J ClinMicrobiol 2000;38:4285-4287.
25. Nelson SM, Deike MA, Cartwright CP. Value of examining multiple spu-tum specimens in the diagnosis of pulmonary tuberculosis. J ClinMicrobiol 1998;36:467-469.
26. Warren JR, Battacharya M, De Almeida KN, Trakas K, Peterson LR. Aminimum 5.0 ml of sputum improves the sensitivity of acid-fast smear forMycobacterium tuberculosis. Am J Respir Crit Care Med 2000;161:1559-1562.
27. Di Perri G, Cruciani M, Danzi MC, et al. Nosocomial epidemic of activetuberculosis among HIV-infected patients. Lancet 1989;2:1502-1504.
28. Fenelly KP, Nardell EA. The relative efficacy of respirators and roomventilation in preventing occupational tuberculosis. Infect Control HospEpidemiol 1998;19:754-759.
This content downloaded from 193.104.110.108 on Wed, 14 May 2014 08:54:09 AMAll use subject to JSTOR Terms and Conditions