Embed Size (px)
Citation preview
150
centres of population and important seaports, the
explanation may be that clinics are inadequate or
badly sited, or that there is not a proper liaison withother departments of the hospitals concerned. The latemanifestations of venereal disease are commonly to befound among general medical cases and in other specialdepartments. If the venereologist has the right degreeof interest in his work his colleagues will be anxious toseek his advice and help. If, on the other hand, he belongsto some other special subject and has only perfunctoryinterest in venereology no-one will want his advice.The result will be a poor standard and a break-up of theorganisation which has been built up gradually withlabour and tears and has produced such excellent results.
CLAUDE NICOL.St. Bartholomew’s Hospital,
London, E.C.1.
1. Molhuysen, J. A., Gerbrandy, J., Vries, L. A., Jong, J. C., Lenstra,J. B., Turner, K. P., Borst J. G. G. Lancet, 1950, ii, 381.
2. Groen, J., Pelser, H. E., Frenkel, M., Kamminga, C. E., Wille-brands, A. F. J. clin. Invest. 1952, 31, 87.
3. Groen, J.. Pelser, H. E., Willebrands, A. F., Kamminga, C. E.New Engl. J. Med. 1950, 244, 471.
4. Card, W. I., Mitchell, W., Strong, J. A., Taylor, N. R. W.,Tompsett, S. L., Wilson, J. M. G. Lancet, 1953, i, 663.
5. Parish, A. E., Alpert, L. K. Amer. J. Med. 1953, 14, 522.6. Pelser, H. E., Willebrands. A. F., Frenkel, M., Van der Heide,
R. M., Groen, J. Metabolism, 1953 2, 322.7. Calvert, It. J. Lancet, 1954, i, 805.
FAILURE OF GLYCYRRHETINIC ACID TOCONTROL ADRENAL INSUFFICIENCY
SIR,—Since Molhuysen et al.1 in 1950 first reportedthe deoxycortone-like activity of liquorice extract, a
number of papers have appeared describing the effectsof liquorice and liquorice extracts in patients withadrenal insufficiency. Several authors 2- have describedpatients with Addison’s disease who have been main-tained satisfactorily on liquorice extract or glycyrrhetinicacid.
In a previous communication 4 we described a patient,a woman of 45 with Addison’s disease, whose responseto the administration of 50 mg. of glycyrrhetinic acidfour times daily was in some respects similar to herprevious response to deoxycortone injections and cortisone
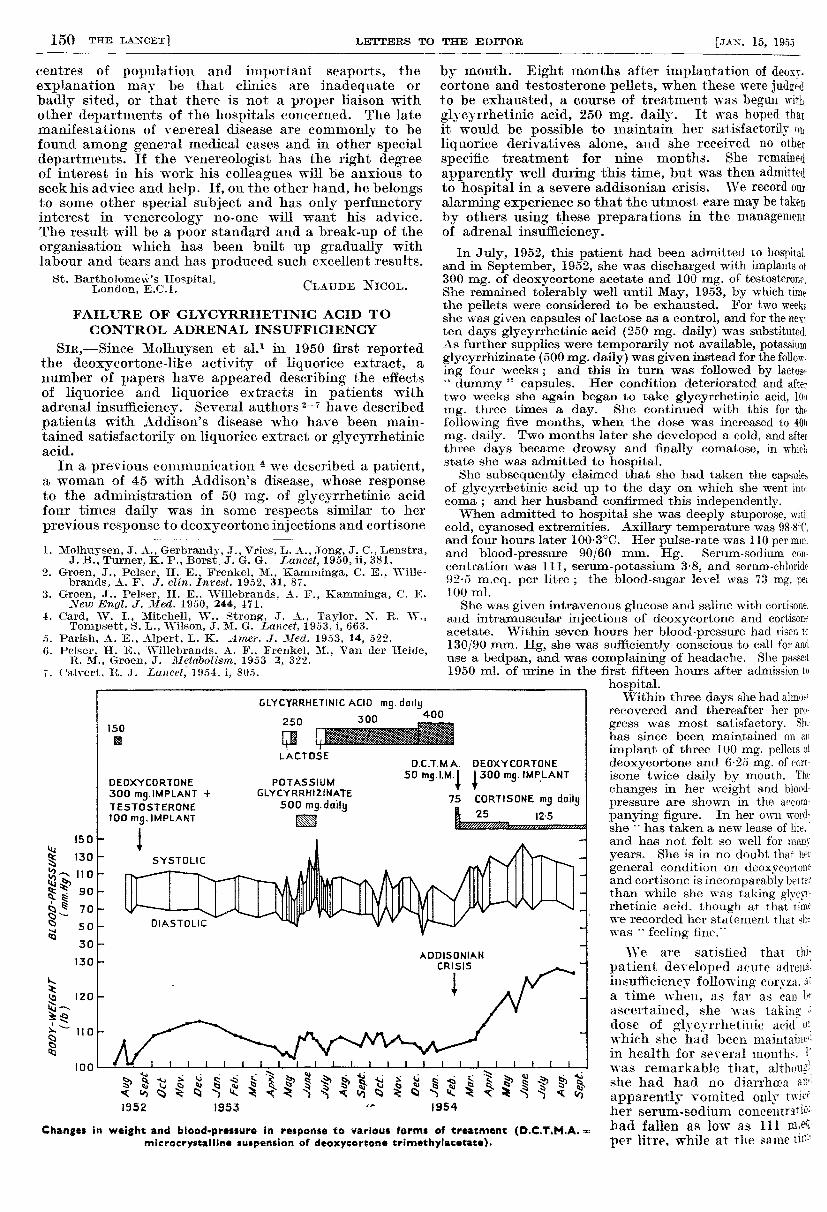
Changes in weight and blood-pressure In response to various forms of treatment (D.C.T.M.A.microcrystalline suspension of deoxycortone trimethylacetate).
by mouth. Eight months after implantation of deoxy-cortone and testosterone pellets, when these were judgedto be exhausted, a course of treatment was begun withglycyrrhetinic acid, 250 mg. daily. It was hoped thatit would be possible to maintain her satisfactorily onliquorice derivatives alone, and she received no otherspecific treatment for nine months. She remampdapparently well during this time, but was then admittedto hospital in a severe addisonian crisis. We record our
alarming experience so that the utmost eare may be takenby others using these preparations in the managementof adrenal insufficiency.
In July, 1952, this patient had been admitted to hospital.and in September, 1952, she was discharged with implants ot300 mg. of deoxycortone acetate and 100 mg. of testosterone.She remained tolerably well until May, 1953, by which timethe pellets were considered to be exhausted. For two weeksshe was given capsules of lactose as a control, and for the nex-ten days glycyrrhetinic acid (250 mg. daily) was substituted.As further supplies were temporarily not available, potassiumglycyrrhizinate (500 mg. daily) was given instead for the follow.ing four weeks ; and this in turn was followed by lactoa-"
dummy " capsules. Her condition deteriorated and aftertwo weeks she again began to take glycyrrhetinic acid, 10))
mg. three times a day. She continued with this for thefollowing five months, when the dose was increased to 400mg. daily. Two months later she developed a cold, and afterthree days became drowsy and finally comatose, in whiel,state she was admitted to hospital.
She subsequently claimed that she had taken the capsule:,of glycyrrhetinic acid up to the day on which she went intocoma ; and her husband confirmed this independently.When admitted to hospital she was deeply stuporose. with
cold, cyanosed extremities. Axillary temperature was 988=C,and four hours later 1003°C. Her pulse-rate was 110 per mm.and blood-pressure 90/60 mm. Hg. Serum-sodiumeon-centration was 111, serum-potassium 3-8, and serum-chloride92-5 m.eq. per litre ; the blood-sugar level was 73 mg. per100 ml.She was given intravenous glucose and saline with cortisone.
and intramuscular injections of deoxycortone and cortisoneacetate. Within seven hours her blood-pressure had risen t(130/90 mm. Hg, she was sufficiently conscious to call for anduse a bedpan, and was complaining of headache. She passed1950 ml. of urine in the first fifteen hours after admission to
hospital.Within three days she had almost
recovered and thereafter her pro-gress was most satisfactory. Shthas since been maintained on an
implant of three 100 mg. pellets oideoxycortone and 6.25 mg. of cort-isone twice daily by mouth. The
changes in her weight and blood-pressure are shown in the accom-
panying figure. In her own word-she .. has taken a new lease of life.
*
and has not felt so well for manyyears. She is in no doubt that he’’
general condition on deoxycortoneand cortisone is incomparably betterthan while she was taking glycye-rhetinic acid, though at that timewe recorded her statement that shewas
"
feeling fine.
We are satisfied that thispatient developed acute adrena-insufficiency following’ cor.’za. ;1;a time when, as far as call 1.’ascertained, she was tahing =
dose of glycyrrhetinic acid which she had been maintainedin health for several months. J’was remarkable that, althoughshe had had no diarrhœa andapparently vomited only twiceher serum-sodium concentrattionhad fallen as low as 111
per litre. while at the same IH"-"
151
her serum-potassium concentration was also depressedto 3.S m.eq. per litre, and later fell as low as 24 m.eq.per litre. We attribute the initial low serum-potassiumconcentration in this patient with Addison’s diseaseto The glycyrrhetinic acid, but this deoxycortone-likeeffeut conflicts with its failure to prevent the serum-sodium from falling to the unusually low figure of
III m.eq. per litre. A similar paradox was noted byParish and Alpert 5 in one patient treated with syrupf liquorice who showed increased potassium excretionwith alternate positive and negative sodium balance.
lu view of the patient’s subsequent progress, it isdear that when she was having glycyrrhetinic acid hercondition was much less satisfactory than when, later,Ac was given deoxycortone and cortisone. It is unwisero generalise on experience with one patient, but wefeel that glycyrrhetinic acid alone is not a suitablesubstitute for conventional treatment in more severecases of Addison’s disease. We- do not suggest thatglycyrrhetinic acid or crude liquorice preparations arenot pharmacologically active, but rather that for somepatients they may be inadequate as the sole form oftreatment, much as deoxycortone alone is inadequatefor the proper maintenance of patients with adrenalinsufficiency. Neither deoxycortone nor glycyrrhetinicacid has any appreciable effect on carbohydrate meta-bolism, and cortisone or hydrocortisone is required tol’oneet this deficiency. Molhuysen et al.1 and Borstet al.8 found that some patients with Addison’s diseasefailed to respond to treatment with liquorice derivatives,and it is possible that with the development of the diseaseour patient had become unresponsive to the drug.Borst et al. have described a synergism between
glycyrrhetinic acid and cortisone, though Hart andLeonard 9 were unable to confirm this. We wondertlieiefore whether those patients with adrenal insufficiencywho have apparently been satisfactorily maintained forlong periods on glycyrrhetinic acid may not in fact havebeen secreting small amounts of adrenal cortical hormone,which without the addition of glycyrrhetinic acidwould have been insufficient to prevent symptoms ofadrenal insufficiency. There is, of course, the possibilitythat our patient had neglected to take the drug ; ; or,
alternatively, that if the dose had been considerablylarger she might not have developed an addisoniancrisis.We are grateful to Dr. Wm. Mitchell, of Messrs. Stafford
Allen Co., Ltd., for supplies of the liquorice derivatives used.J. A. STRONGJ. M. G. WILSON.
Western General Hospital,Edinburgh.
Borst. J. G. G., ten Holt, S. P., Molhuysen, J. A., Vries, L. A.Ibid. 1953, i, 657.
Host. F. D., Leonard, J. C. Ibid, 1954, i, 804.
FLUOROACETATE POISONING
M. A. PHILLIPSConsulting Chemist.
SIR,—As you say in your annotation of Dec. 18 onthe control of rats and mice, sodium monofluoroacetatei, dangerous to mammals. Yet, if properly handled bytrained personnel, it can perform its function and do noharm to man or domestic animals. This, anyhow, is theexperience of one group of commercial specialists overtwo years, during which there has been no evidence oftoxicity to the operators or to animals other than ratsand mice.
Latterly, we have been working on a derivative of sodiumfluoroacetamide, which tested pharmacologically
rats and mice proves to have an L.D’50 about twice that offluoroacetate (about 4 mg. per kg. for the amide,
t-2 mg. per kg. for the sodium salt) and, moreover, to produceruy mild symptoms of toxicity and none of the epileptiformconvulsions characteristic of sodium-fluoroacetate poisoning.Fr ihi& reason, fluoroacetamide has now been suggested as a’-"!d rodenticide in place of sodium fluoroacetate, and details.1i shortly be published. Although its toxicity is less than’:.-it of the sodium salt, it is, it appears, quite sufficient tomake it an effective rodenticide.
It is now well established by the work of Sir Rudolph Peters 1that the toxicity of sodium fluoroacetate is due to formationin vivo of fluorocitric acid, and it is our suggestion thatfluoroacetamide is only slowly converted into this toxin ascompared with sodium fluoroacetate, thus giving only smallblood-concentrations of fluorocitrate (sufficient to kill rodentsbut not sufficient to cause violent death) and a larger marginof safety in use. It is, of course, to be hoped that antidotes tofluoroacetate poisoning will continue to be sought ; fluoro-acetamide may be more likely to yield to treatment thansodium fluoroacetate in view of the probably lower bloodconcentrations of fluorocitrate when amide is used.
It is well known that the higher mammals are less susceptibleto fluoroacetate poisoning than are rodents ; Professor Adrianhas taken a dose of sodium fluoroacetate sufficient to producea urine toxic to guineapigs. For monkeys the L.D’50 is about15 mg. per kg.Recently Saunders and Hughes 2 have shown that enzyme
degradation of a C-F bond is possible ; this, too, leads us to amore optimistic view about the possibility of antidotes tofluoroacetamide and fluoroacetate poisoning.
M. A. PHILLTPSRomford, Essex. Consulting Chemist.
1. Endeavour, July, 1954, p. 147.2. Saunders, B. C., Hughes, G. M. K. Chem. & Ind. (Rev.),
Sept. 9, 1954, p. 1265.3. Lancet, 1954, ii, 489.
HEAT TO THE HEART
SIR,- Some eighteen months ago I discovered that heatapplied to the cardiac area very quickly relieved an attackof angina, and if applied sufficiently soon it would com-pletely abort it. The means used were either an electricpad (the smaller the better) such as are sold for use inbed, or a face cloth or handkerchief wrung out in veryhot water. The latter method is quicker but requiresfrequent renewals, and the handkerchief must be 110°Fon application to be effective (just a little hotter thancan comfortably be tolerated on one’s own bare arm-not by a nurse’s hand). The handkerchief may be usedwhile the electric pad is heating up. The relief obtainedis augmented by sips of hot water or hot tea. The painis relieved much more quickly, though perhaps not morecertainly, than by glyceryl trinitrate, and the method ismore reassuring to the patient and may be preferable ;in some circumstances it may be the only one available(even if the patient is out in a car a handkerchief can bedipped in the radiator or hot water obtained from a nearbyhouse).
There is also no doubt that cold can precipitate an attack.That there may be a fundamental principle involved is nowsuggested by the work of Andjus at Belgrade, confirmed bySmith et al. and quoted in your survey on experimental deephypothermia.3 Andjus found that in extreme hypothermiacardiac arrest in animals occurred at 6°C and that by warmingthe whole body, plus artificial respiration, the animals couldnot be revived; and they all died. He then discovered, however,that if heat were first applied locally to the cardiac area (forexample, by putting a
" heated metal object " on the skin) andif this was combined with artificial respiration, the heart
began to beat again and the animals recovered. Thus, therisk of anoxia of tissues (including the brain) during re-warmingcould be avoided. That is to say, keep the general metabolismof the animal (patient) as low as possible, supply oxygen andstimulate only metabolism of the heart, and spontaneousrevival becomes possible.Angina may be regarded as a threatened cardiac arrest, and
cardiac arrest may be induced by hypothermic and hypo-tensive drugs. In any of these threatened emergencies itwould therefore seem logical to apply heat locally to the cardiacarea as a first step, accompanied by full use of oxygen andperhaps cooling of the head by ice-cold water in order toreduce cerebral metabolism, and so perhaps avoid the cerebralsequelae that may follow recovery. People are more rightthan they wot of when they say there was a struggle betweenhis heart and his head. There is always intense competitionin the last resort between the two for glucose and oxygen, andif the heart is in extremis it is surely desirable to lessen thiscompetition, and give the cardiac muscle a favourable balancefor a few minutes.