Embed Size (px)
Citation preview

Faculty of Nursing-IUG
Chapter (6)Assessment of Skin, Hair and Nails

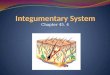
Structure of the Integument The skin is the largest organ of the body comprising 15
percent of total body weight. Layers of the skin A. Epidermis B. Dermis C.
Subcutaneous tissueEpidermal appendagesHairNailsGlands: two types of skin glands: 1. Sweat Gland Eccrine sweat glands: are widely distributed and
open directly onto the skin surface Apocrine sweat glands: open into hair follicle in
axillary and genital areas2. Sebaceous glands: Produce sebum(oily secretion)

3

Functions of skin and epidermal appendages
Barrier to water and electrolyte loss
Regulation of body heat
Sensory organ for touch, temperature, and Pain
Production of protective skin film by eccrine and
sebaceous glands
Participation in production of vitamin
Wound repair
4

Assessing the Integument
1. Subjective data
Skin infection, rashes, lesions, itching.
Precipitating factors: stress, weather, drugs
Changes in skin color, lesions
Amount of sun exposure
Scalp lesions, itching, and infections.
Changes in texture and amount of hair.
Changes in nails and cuticles nail breaking 5

2. History of current symptom Are you having experience of skin problem, such as
rashes, lesionDescribe any birthmarks, tattoos, or molesHave you noticed any changed in your ability to feel
pain, pressure, light touch, or temperature changed? Have you had any hair loss or change in the
condition of your hair?Have you had any change in the condition or
appearance of your nails? Describe any previous problem within the skin, hair
or nails ( past history)Have you ever had any allergic skin reaction to food,
medication, plants? Has anyone in your family had a recent illness, rash,
or other skin problem? (Family history)

3. Physical Assessment
Equipment Penlight Tongue depressor Centimeter rule
Gloves Magnifying glass Flashlight Wood’s lamp
Technique to examination of skin Inspection Palpation Inspections and palpation of skin Color Moisture Temperature
Thickness Turgor Vascular changes Edema
Lesions Skin odors are usually noted in the skin fold. 7

8

Inspection color of skin
Skin color varies from body part to body part and
from person to person. Assessment first involves area of skin not
exposed to the sun e.g. palms of the hands. Pallor easily perceived in the buccal “mouth”
mucosa particularly in individuals with dark skin. Cyanosis readily seen in area of least
pigmentation e.g. lips, nail beds conjunctiva and palm.
Jaundice or Yellow seen in client’s sclera.
Erythema may indicate circulatory changes9

10

Palpation moisture of skin
Skin is normally smooth and dry. Skin folds e.g. axillae are normally moist. In presence of lesions or ooze fluid, nurse must
wear gloves to prevent exposure to infections drainage
Moisture indicates: 1- Degree of client’s hydration 2- Condition of the outer lipid layer of the skin
surface
Dry (xerosis): Vitamin A def. and Myxedema
Oily: Acne11

Palpation of TemperatureTemperature of skin depends on the amount of
blood circulating through dermis.
Generalized warmth: (Fever, Hyperthyroidism)
Local warmth: (Inflammation)
Coolness: (Hypothyroidism, Frost bite,
Hypothermia, Shock, Low cardiac output)
Palpation of skin with dorsum of the hand.
Assessment of skin is critical point in some
conditions such as: after cast application, or after
vascular surgery. 12

Palpation of TextureTexture of skin normally smooth, soft and flexible
If any abnormalities in texture found you must ask
the client is he exposed to any recent injury to the
skin?
Nurse determines whether the client’s skin is smooth
or rough, thin or thick, tight or supple (flexible).
Very Soft: (Thyrotoxicosis)
Tight: (Scleroderma = hard skin)
Rough: (Hypothyroidism)
13

Palpation of Turgor
Turgor: is the skin elasticity diminished by edema or dehydration.
Assessment of turgor done by pinching skin between the thumb and forefinger and released.
Normally skin return immediately to its position.
Failure of this process means dehydration.
Decrease in turgor predisposes the client to skin breakdown.

Palpation of Vascularity Vascularity: Assessment of circulation of skin E.g.
petechiae may indicate serous blood clotting disorders, drug reactions or liver disease.
Inspection and Palpation of EdemaEdema : "Build up of fluid in tissues“Inspected for location, color, and shape. Palpates areas of edema to determine mobility,
consistency, and tenderness
Inspection and Palpation of LesionsNormally skin free of lesions except common freckles. If lesion present, inspection must done for distribution,
arrangement, morphology, color and sizePalpation for lesion’s mobility, contour (flat, raised or
depressed) and consistency (soft or hard are indicated). Cancerous lesions frequently undergo changes in color and
size.

Hair and Scalp
Assessment done for distribution, thickness, texture,
and lubrication of the hair.
Some events which affect the distribution of hair over
the body e.g. client with hormone disorders, woman
with hirsutism
Amount of hair covering extremities may be reduced
as a result of aging and arterial insufficiency especially
in lower limbs.
Scaliness or dryness of the scalp is frequently caused
by dandruff or psoriasis. 16

Nails Assessment
Nails reflect an individual's general state of health, state of nutrition, and occupation.
Nails are normally transparent, smooth, and convex, with a nail bed angle of about 160 degrees.
The surrounding cuticles are smooth, intact and without inflammation.
Nail bed is normally firm on palpation.
Nails normally grow at a constant rate.

Abnormal condition of nailAnonychia: complete absence of nails
Platunychia: flatting nails
Koilonychia : nails like spoon shape (iron deficiencies
anemia)
Racket nail: fattened and expanded nails
Onycholysis: separation of nail form nail bed
(thyrotoxicosis)
Melanoychia: presence of brown color in nails plate
Paronychia: inflammation of tissue surrounding the nail
18

19