Embed Size (px)
Citation preview
MINUTES FACULTY COUNCIL
Case Western Reserve University School of Medicine
November 18, 2013 - 4:00 p.m., Room T-501 A) Minutes from the Faculty Council meeting of October 14, 2013, were approved. B) Dr. Mark Chance reported on the SOM Strategic Plan Process and status of the plan. Four committees representing people, research, education, and community worked separately and then came together to identify a common set of strengths and opportunities. Strengths included: affiliates, location in university circle, collaboration and translation. Town halls to present the final plan are scheduled for early in 2014. Highlights for faculty consideration were the areas of investment and opportunities for growth in research. Discussion focused on modification of current classroom space (to be vacated by the move-out of medical students) for graduate students. Dr. Chance promised to return and report again to Faculty Council to provide opportunity for discussion on the adopted strategic plan. C) Matt DeVries, Research Compliance Specialist, and Dr. Chris Flask, Interim Director, Scientific Core Steering Committee, reported on the Core Facilities retreat and on-going plans for the development of the core facilities. The SOM held a retreat gathering Core Facilities stakeholders for an open agenda meeting. A survey of faculty with 345 responses helped to focus issues, and the retreat was attended by more than 100 interested faculty members. Chris Flask has been appointed as the interim chair of a committee to continue work on core facility identification, etc. There is no current plan to centralize the more than 40 cores that have been identified, each having unique structure and characteristics. The Core Facilities White Paper is attached to these Minutes. D) Stuart Youngner, Chair, Basic Science Chairs WR2 Curriculum Work Group, reported on the group’s work. The basic science department chairs feel estranged from the MD core curriculum. Accordingly, each chair appointed one person to serve on this committee and charged it to meet with new medical education leadership and engage it to involve the chairs in teaching and the curriculum. The group seeks clarification of what is expected of basic science departments regarding hours of teaching and the metrics for evaluation. Dr. Younger will report back to Faculty Council on further developments. E) A proposal to establish a PhD program in Clinical Translational Science reached the Faculty Council with a recommendation for approval by Council’s ad hoc review committee chaired by Dr. John Mieyal. Dr. James Spilsbury and Dr. Li Li, program proponents, presented the proposal (see PowerPoint slides attached to these minutes) and answered questions. Dr. Spilsbury clarified that they would not be multiple classes of students but that students would be recruited from nursing and dental medicine schools as well as from medical schools. The PhD in clinical translational science would be formally awarded by the school of graduate studies. From 6 to 10 students would be admitted each year. Following a discussion of these and other
elements, the faculty council voted unanimously, with the exception of three abstentions, to recommend approval of the program. The program will be reviewed next by the dean who is expected to forward it to the faculty senate for its review. F) Dr. Paul MacDonald, Associate Dean for Graduate Education, summarized a report (attached) on a proposed SOM Individual Development Plan policy for graduate students and postdocs. He explained that the National Institutes of Health have requested that such a policy be established. Dr. MacDonald believes that such plans are a positive aid for the students. He asked the Council members to review the draft and forward their comments to him. A Council member reported that his department already has a similar requirement and it works well. G) Dr. John Fredieu, SOM Representative, Faculty Senate Executive Committee, provided the attached Report on Faculty Senate Activities. H): No new business was introduced. I) The Council adjourned. Respectfully submitted, Dan Anker Associate Dean for Faculty Development and Human Resources
SOM:ORA - DRAFT 10/8/13
SOM:ORA - DRAFT 10/8/13
White Paper: School of Medicine Core Facilities Action Plan In a continuing effort to enhance user science, develop efficiencies, and productively coordinate activities within and among the various core facilities at the School of Medicine, in November 2012 the Vice Dean for Research approached leaders from the SOM, the Case Comprehensive Cancer Center, the Center for AIDS Research, and the Clinical and Translational Science Collaborative to advocate a retreat on the topic of core facilities. This effort would require the support of these key leaders to ensure that the event, and future policies regarding core facilities, was in tune with the concerns and goals of core facility directors, users, administrators, and other stakeholders. These leaders gave their support, and in January 2013, a planning group for the retreat was convened, consisting of administrators from the major centers, core facility managers and directors, and a member from an outside partner institution. The committee developed a list of Scientific Core Facilities, defined as an administrative unit that provides access to specialized technologies, services, and expertise that are necessary and important to the scientific mission of the institution, not easily available in an individual research laboratory, and servicing multiple departments, schools, and/or institutions. This definition delineated approximately 40 facilities to include in the retreat planning. After further vetting by the Vice Dean for Research and other key stakeholders, targeting a retreat to this group of cores offered the most potential gain to the institution in terms of customer service, recruiting, grantsmanship, and cost effectiveness, while serving the widest interests of the School of Medicine community. The committee immediately engaged the larger SOM community to guide the discussion at the retreat and for any future decision-making and planning. In June 2013, a survey was deployed via REDCap to assess what topics and issues regarding core facilities needed open discussion and dissection. After collecting over 345 responses, the committee analyzed and synthesized the responses and constructed the retreat agenda. Additionally, the survey responses were used to define a set of goals and action plans for the SOM core facilities. These goals were to be discussed at the retreat and refined into a timeline of actions. The retreat was held on August 26th, 2013, with 110 people in attendance including core facility directors and managers, core facility users, center and department administrators, school leadership, and key partners outside the School of Medicine. The program consisted of moderated panels on Identification, Access, and Visibility; Coordination, Reporting, and Billing; and Investment and New Core Development. In addition, breakout sessions centered on Leadership Coordination; Metrics, Reporting, and Administrative Tools; Instrumentation Grants; Creative ways to make Core Facilities more efficient; CTSC Pilot Grants; and Core Facility Roles and Responsibilities. A poster session for core facilities was also scheduled, 40 cores responded and presented highlights of both their services and accomplishments. Proposed Follow on Actions Five themes at the retreat were crystallized into action steps presented to the attendees at the close of the event: Create a Centralized Core Infrastructure, Establish a Core Advisory Committee, Provide Transparency, Establish a Research Support Director, and Measures to Increase Investment. The action steps are outlined below.
1. Definitions of Core Facilities The School of Medicine will refine the definitions of Scientific Core Facilities by first establishing the concept of
expectations for productivity, participating in policy discussions, and promoting core facility use to benefit faculty grants and faculty recruiting, an Institutional Scientific Core is eligible for investment from the SOM. As
SOM:ORA - DRAFT 10/8/13
SOM:ORA - DRAFT 10/8/13
such definitions will drive many of the decisions to be made over the coming year(s), the following three definitions are proposed: a. Institutional Scientific Core Facilities - An institutional unit that provides access to specialized
technologies, services, and expertise that are necessary and important to the scientific mission of the institution, not easily available in an individual research laboratory, and servicing multiple departments, schools, and/or institutions. An Institutional Scientific Core Facility will be eligible for investment by the School based on criteria and metrics to be set forth by an advisory committee of Scientific Core Facility Managers and Department and Center Administrators, and agreed to by the Vice Dean for Research.
b. Departmental Scientific Core Facilities - A departmental resource that provides access to specialized technologies, services, and expertise that are necessary and important to the scientific mission of the department. Access and investment are entirely within the purview of Departmental Leadership.
c. Service Centers - Provide a discrete technical, engineering, or support service either to individual departments or school-wide that is typically transactional in nature. Examples of these would be the Scientific Instrument Repair Center, departmental centrifuge or tissue culture rooms, or vendor supply closets.
2. Visibility Visibility and Access are key components of core success. The action steps listed below will help cores capture data for reporting, provide important information to users, allow users to interact directly with cores, and provide advertising for services and products.
a. Website - A comprehensive website is going to be developed housed on the Office of Research
centers a i. As of now, existing information on the retreat, including goals, slides and other information, are
posted. ii. Over the next 6 months - Cores will be identified and web content enhanced. Enhanced information
and progress related to this increased visibility will ease navigation. iii. Over the next year: Solutions will be discussed in consultation with Central ITS, SOM ITS, and other
stakeholders around a common web-presence that will ultimately be a requirement of an Institutional Core Facility. This must serve as a discovery and access tool for prospective and current end users, while satisfying the needs and requirements of the various centers and grants that support the facility, as well as be flexible enough to serve the needs of the facility
b. Core news and updates Updates will be developed for dispersal to the School of Medicine. One type of dissemination for this which spotlights a single facility every 2 weeks, describing their services and capabilities, and celebrating their achievements in publishing, presenting, and grantsmanship. A second will be short updates on the plasma screens. This will be rolled out before the end of the year
3. Core Steering Committee and Research Support Director Coordination and Investment will allow leadership to understand common issues and concerns, disseminate successful strategies, and provide ongoing feedback. New infrastructure will allow coordination and investment to be performed seamlessly. The new positions are listed below.
a. Core Focus Committees - will be established and will be based on loose discipline commonalities for core facilities. Some current suggestions include: -omics, animals, biostatistics/bioinformatics, cellular imaging, clinical and translational imaging, drug development, and biophysics/structural biology. A representative for each committee will be identified. The representative must be a core facility director and faculty member. The representative will be responsible for collecting and representing the views of the facilities represented by their committee.
SOM:ORA - DRAFT 10/8/13
SOM:ORA - DRAFT 10/8/13
b. Steering Committee - An Institutional Scientific Core Facility Steering Committee will be established, made up of Center/Department Administrators and the Core Focus Committees representatives. This body will be charged with: i. Establishing common metrics for Institutional Scientific Core Facilities ii. Sharing best practices iii. Communicating between cores iv. Representing cores in policy planning v. Conducting periodic core reviews vi. Reviewing/recommending new core requests vii. Developing tracking metrics
4. Transparency Transparency was identified as a key issue in creating a more cohesive, efficient standards for core facilities. Specific steps to increase the transparency of the investments in, and operation of, core facilities are proposed:
a. This white paper will be included in the School of Medicine Strategic Plan and cores will be an established part of strategic planning going forward.
b. Investment criteria to determine eligibility as an Institutional Scientific Core Facility will be determined and disseminated by the Steering Committee, with input from the Dean and senior school leadership.
c. Current investments in cores will be made public, and future investments will be publicized. 5. Billing
In support of transparency and visibility, a committee of administrators will review current billing practices and procedures. The committee will investigate tools that may support common workflow and billing practices. The committee will make recommendations to the Core Steering Committee regarding the standardization of billing practices and procedures.
6. Reporting Committee of administrators will be convened to assess current approach to reporting to the SOM and funding agencies regarding core utilization and efficiencies of cores. The committee will make recommendations to the Core Steering Committee regarding reporting best practices and reporting requirements for Institutional Scientific Core Facilities. Proposed Timeline
October 2013: The white paper will be complete and submitted to school leadership with the aim of including it in the School of Medicine Strategic Plan.
November 2013: During this month, the white paper will be presented to and reviewed by school leadership, stakeholder groups including basic science chairs, the research committee, faculty council, and center directors. Their input and advice will be considered and added to the plan.
December 2013: Core definitions will be instituted and publicized, including the review process, metrics and other requirements to be considered an Institutional Scientific Core Facility. Facilities at this time will be invited to declare as an Institutional Scientific Core Facility.
January - March 2014: The Institutional Scientific Core Facility Steering Committee will begin meeting to establish a charge and procedures. The website upgrades will be moving ahead. Work will begin on the 2014 Scientific Core Facilities Retreat.
March-June 2014: Data and metrics will be collected by the Institutional Scientific Core Facility Steering Committee by March 2014. The Committee will analyze the data and make recommendations to senior leadership.
August 2014: Core Retreat II
Proposed PhD Program in
Clinical Translational Science
Prepared by the PhD in Clinical Investigation Steering Committee Li Li, MD, PhD (Program Director)
Eugene Blackstone, MD (Associate Director) Jim Spilsbury, PhD (Associate Director)
Clifford Harding, MD, PhD Shirley Moore, PhD, RN, FAAN
Richard Rudick, MD Kurt Stange, MD, PhD
1
November 18, 2013
Faculty Council Meeting
PhD Clinical Translational Science: Rationale
• Clinical Translational Science is a new discipline to reduce lag between ‘discovery’ and ‘practice’ – Unique theory, skills, methodologies – New scientific journals dedicated to this area – Competencies for this field developed nationally – > 20 existing PhD programs nationwide, and number is
growing
• Demonstrated need for this program at CWRU – Expressed interest by K awardees & MS graduates – Fills gap in current dual MD-PhD program (CTSTP)
2
PhD Clinical Translational Science Competency Domains
• Theory-based problem assessment & formulation
• Critical literature review & synthesis
• Study design & measurement
• Study implementation • Statistical approaches • Health informatics
• Translational & patient-oriented research
• Team science • Leadership • Scientific
communication • Cultural diversity • Funding
3
PhD Clinical Translational Science: Research Orientation & Focus
• Primary goal = produce successful clinical-translational researchers
• Research theory & methods emphasized in curriculum by 3 new courses – Translational and patient-oriented research theory – Meta-analysis and evidence synthesis – Seminar in multidisciplinary clinical and translational research
• Mentored research experiences – Practicums – Dissertation
4
PhD Clinical Translational Science: Rigorous Curriculum
• Minimum of 54 credit hours – 36 course credit hrs (24 graded) – 18 dissertation credit hrs
• Meets all CWRU School of Graduate Studies’ requirements
• Consistent with core competencies developed nationally for Clinical Translational Science
5
PhD Clinical Translational Science: Faculty
• 22 Core Faculty Members
• Provides expertise in clinical translational domains
• Active program/track record of funded research
• Highly multidisciplinary – Case School of Medicine, Francis Payne Bolton School
of Nursing, the School of Law, Weatherhead School of Management, other schools and depts.
• Multi-institutional – CWRU, Cleveland Clinic Lerner College of Medicine,
MetroHealth Medical Center, University Hospitals, Louis Stokes Veterans Administration
6
PhD Clinical Translational Science: Mentoring
• Transdisciplinary nature of field requires expertise from multiple disciplines
• Two-mentor model – Primary mentor
• Field of interest & expertise matches student’s dissertation area • Primary responsibility for guiding PhD research & training
– Co-mentor • Assigned based on student’s scientific interests • Provides complementary guidance on overall course of study, career plans,
professional development
– Additional mentors as needed
• > 40 faculty have agreed to serve as mentors
7
PhD Clinical Translational Science: Program Cohesion
• Required monthly seminar to foster cohesion and interaction among students and faculty
• Retreats, journal clubs
• Social events
8
PhD Clinical Translational Science: Target Applicants
• Individuals with advanced clinical degree seeking rigorous training in clinical translational science
• Individuals enrolled in dual clinical-research degree programs (e.g., MSTP-CTSTP and DMD-PhD programs) whose interests and career goals align with PhD in Clinical Translational Science
• Individuals with existing MS in a health-related field who seek a PhD in Clinical Translational Science.
9
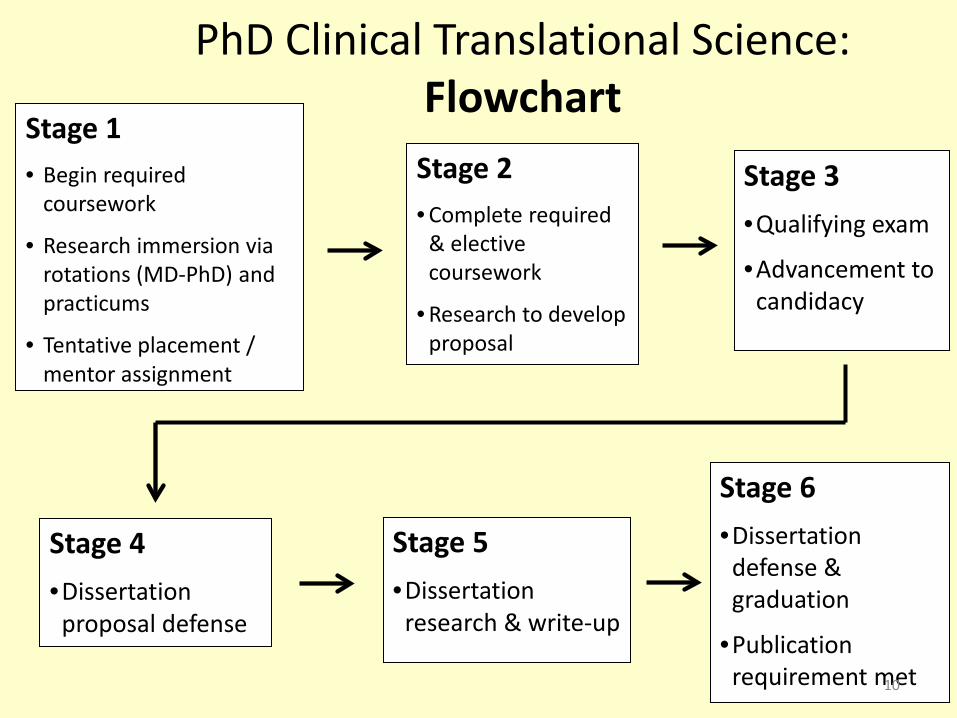
Stage 1 • Begin required
coursework
• Research immersion via rotations (MD-PhD) and practicums
• Tentative placement / mentor assignment
Stage 2 • Complete required
& elective coursework
• Research to develop proposal
Stage 3 •Qualifying exam
•Advancement to candidacy
Stage 4 •Dissertation
proposal defense
Stage 5 •Dissertation
research & write-up
Stage 6 •Dissertation
defense & graduation
•Publication requirement met
PhD Clinical Translational Science: Flowchart
10
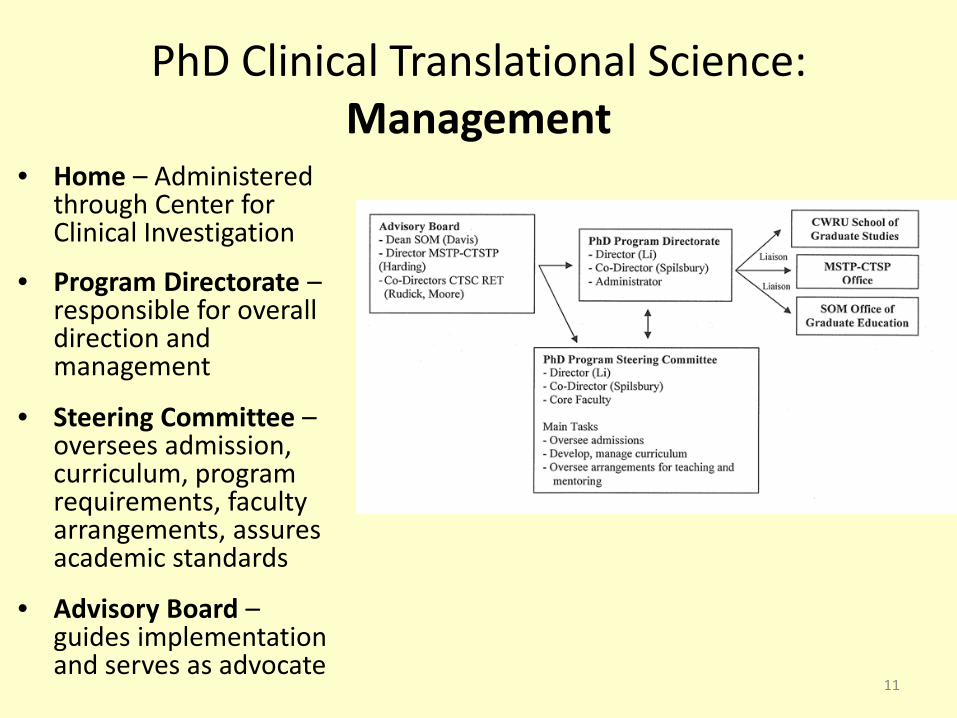
PhD Clinical Translational Science: Management
• Home – Administered through Center for Clinical Investigation
• Program Directorate – responsible for overall direction and management
• Steering Committee – oversees admission, curriculum, program requirements, faculty arrangements, assures academic standards
• Advisory Board – guides implementation and serves as advocate
11
PhD Clinical Translational Science: Financial Model
• Institutional (SOM) Support – Salary and administrative support – Publicity, recruitment, programmatic activity support
• Financial Support for Students – Dual Degree students fully funded – Existing T/K training mechanisms – Development of proposal for T32 support – Self-supporting students
12
Thank You!
13
October 2013
What is an IDP ?
The Individual Development Plan (IDP) concept is commonly used in industry to help employees define and pursue their career goals.
An individual development plan (IDP) helps mentees explore career possibilities and set goals to follow the career path that best fits.

October 2013
Why a policy?
• NIH is encouraging grantees to develop institutional policies that require an IDP for every graduate student and postdoctoral researcher supported by any NIH grant by October 1, 2014 (NOT-OD-13-093).
• NIH will encourage grantees to include in their progress reports current practices documenting IDPs are used to help manage the training of these individuals.
October 2013
Why is it important?
• Visual representation/reminder of how mentee will spend time achieving your goals
• Helps them to identify both short-term and long-term goals – pushes them toward action
• Milestones along the way can be acknowledged and celebrated
• Serves as a communication tool between mentee, faculty mentor, and others
• Helps identify and develop additional career paths beyond academic research
October 2013
What is the value added?
• people who develop and implement strategies to pursue career- specific goals achieve greater career success: salary, promotions, and level of responsibility • greater career satisfaction
• rate themselves as more successful compared to peers without IDPs
• postdocs developing IDPs with their advisers at the start of their appointments reported: greater satisfaction, published more papers, fewer conflicts
October 2013
myIDP website myIDP, a Web-based career-planning tool created to help graduate students and postdocs in the sciences define and pursue their career goals. • Exercises to help you examine your skills, interests, and values • A list of 20 scientific career paths with a prediction of which
ones best fit your skills and interests • A tool for setting strategic goals for the coming year, with
optional reminders to keep you on track • Articles and resources to guide you through the process
SOM Policy Statement on Individual Development Plans (Draft 3, 11/2013) Preamble: The CWRU School of Graduate Studies and the School of Medicine Graduate Education Office recognize the benefits that postdoctoral scholars and graduate students experience by using Individual Development Plans (IDPs) in setting career goals and in ensuring that conversations between the student and mentor about these goals occur on a regular basis. Recently, the significance of IDPs in training of the biomedical workforce has been stressed at the national level. NIH is encouraging grantees to develop institutional policies that require an IDP for every graduate student and postdoctoral researcher supported by any NIH grant by October 1, 2014 (NOT-OD-13-093). NIH will encourage grantees to include in their progress reports current practices documenting IDPs are used to help manage the training of these individuals. Thus, the Graduate Program Directors and the School of Medicine Graduate Education Office recommend that the following policy be adopted regarding the use of IDPs for Ph.D. students and postdoctoral fellows and scholars: Policy: All Ph.D. students in the SOM will complete an IDP within 6 months of arrival in their permanent mentor’s lab. Postdoctoral fellows and scholars will complete an IDP within 3 months of their initial appointment. Completing an IDP is an interactive process that involves face-to-face meetings and frank discussions between the junior researcher and mentor. The IDP will evolve through annual meetings between mentee and mentor during the trainee’s tenure at the SOM. Copies of all graduate student and postdoctoral IDPs as well as all annual updates will be submitted to the CWRU SOM Graduate Education Office and then forwarded from there to the School of Graduate Studies. This policy takes effect January 1, 2014 and it includes all current SOM Ph.D. trainees, postdoctoral fellows, postdoctoral scholars, and their mentors. Initial IDPs for all SOM trainees will be due July 1, 2014. Compliance: Departmental Chairs and Graduate Program Directors in the School of Medicine will be notified annually of compliance with this policy. A SOM Graduate Education Office website will track compliance in each Department. Annual reappointment of postdoctoral scholars and fellows will require that an updated, annual IDP be filed. Recommended IDP Format: myIDP, http://myidp.sciencecareers.org/ Training and implementation: A workshop developed by the SOM Graduate Education Office in conjunction with the Postdoctoral Office in the School of Graduate Studies will be held on 3 separate occasions throughout the Spring 2014 semester to familiarize students, postdoctoral researchers, and faculty with the new policy and IDP process. The workshop will be continuously repeated in the Spring, Summer and Fall semesters for new arrivals to the SOM. An IDP page will be developed for the SOM Graduate Education Office website as a resource for mentors and mentees in developing their IDPs.
Report on Faculty Senate activities- 11/18/2013 John Fredieu, SOM Representative, Faculty Senate Executive Committee, [email protected] 1. President Snyder asked for patience and restraint in regards to the recent media coverage of the Law School's difficulties and the reported lawsuit. She offered no information to the Faculty Senate. 2. Dr. Sandra Russ has stepped up to fill the role of Chair of the Faculty Senate after the death of Dr. Steven Garverick. She leaves a vacancy in the chair-elect position. Efforts are being made to fill that position. 3. The Faculty Handbook states that each of the representatives of the different schools on the Faculty Senate Executive Committee also become members, ex officio, of the Executive Committee of the Faculty in his/her own school. The Senate Executive Committee discussed the ongoing non-compliance of the SOM to allow the Faculty Senate SOM Executive Committee member onto the FC Steering Committee. They discussed the Steering Committee members’ view that they do not constitute an Executive Committee of the SOM Faculty. During this discussion, it was noted that the Steering Committee of the Faculty Council does not keep minutes, but is bound by the SOM Bylaws to "report all actions and recommendations to the Faculty Council". This was a concern in that there is no written record of actions and recommendations made by the FC Steering Committee. 4. There was concern expressed of course content offered by non-UPF that overlap courses offered by UPF. UPF are voting members of the University Faculty who have a primary or joint appointment in at least one of these four constituent faculties, or in the Department of Physical Education and Athletics, or in one of the Departments in the School of Medicine that offer undergraduate majors. There was a request for information from faculty on concerns of course overlap in graduate studies. 5. The University has rolled out Wellness Initiatives that provide a Health Risk Appraisal and Biometric Screening. In addition, faculty can submit a Tobacco Attestation Form. Completion of these three components enables the faculty to enjoy a $25/month premium reduction incentive. Screenings are happening this month, so check the Benefits website. 6. There is a 5-year review of the Faculty Handbook, Senate By-laws, and School Bylaws initiated this year. If faculty have suggestions for changes in the Handbook or Bylaws, please pass them on the your Faculty Council Representative, SOM Faculty Senator, or directly to the Chair of the Faculty Senate. 7.There was a discussion of the MS in Medical Physiology Off-Site Program at the Senate Executive Committee meeting. It is to be discussed at the upcoming Faculty Senate Meeting (11/25/2013). If any faculty would like to comment or express concerns, please talk to an SOM Faculty Senator before that meeting. 8. The University is reviewing its Tobacco-Free Campus policy and needs input into details, concerns, and enforcement. Once again, please direct comments to the SOM Faculty Senators. School of Medicine Faculty Senators Joseph Baar Hematology/Oncology [email protected] Matthias Buck Physiology/Biophysics [email protected] Colleen Croniger Nutrition [email protected] Nicole Deming Bioethics [email protected] Thomas Egelhoff Physiology/Biophysics [email protected] John Fredieu Anatomy [email protected] Thomas Kelley Pediatrics [email protected] William Merrick Biochemistry [email protected] Alan Tartakoff Pathology [email protected] Richard Zigmond Neurosciences [email protected]