Embed Size (px)
Citation preview
1
A Team Approach to Wound Care
on the Lower LimbA Physical Therapist’s Perspective
James G. Spahn, MD, FACS
Sharon Lucich, PT , CWS
Jaimee Haan, PT, CWS
1
FACTSFACTS
Pressure ulcers are the result of an
ischemic event, and not a crush injury
Soft tissue distortion leads to
Ischemic necrosis (pressure ulcer).
2
FACTSFACTS
Contact with a support surface causes
either volumetric support of the body or
distortion of the soft tissue trapped
between the bony prominence and the
support surface.
Since the body is three-dimensional,
volumetric support (flotation) is
needed to maintain proper tissue
orientation.
3

2
FACTSFACTS
Nutritionally and mobility impaired
patients are at risk for developing
pressure ulcers.
4
FACTSFACTS
Pressure ulcers may start immediately,
but often are not recognized until 3-7
days later.
High incidence of pressure ulcers may
occur on bed, surgery, ER, transportation
cart, and seating surfaces.
5
FACTSFACTS
Continuum of care is needed during
the acute, sub-acute, and chronic
levels of care.
Patients at risk are usually discharged
to rehab, since they are not
rehabilitated at time of discharge.
6

3
FACTSFACTS
Protocols decrease incidence by 50% 1
Usage of pressure-reducing devices
alone can cause an increase in
incidence.2
1. Moody BL, Fanale JE, Thompson M. Vaillancourt D, Symonds G, Bonasoro C. Impact of staff
education on pressure sore development in elderly hospitalized patients. Archives of Internal
Medicine. 1988; 148:2241-2243.
2. Lyder CH, Preston J, Grady JN, Scinto J, Allman R, Bergstrom N, Rodeheaver G. Quality of care
for hospitalized medicare patients at risk for pressure ulcers. Archives of Internal Medicine. 2001;
161: 1549-1544.
7
Clinical Protocols
NutritionMobilization
Ambulate
TurnPassive Range of Motion
Support SurfaceBed, Chair, Cart, Emergency Room, Operating Room
Incontinence CareWound CareContinuum of Care
Treatment of other generalmedical conditions
8
FACTSFACTS
Heel ulcers constitute 30% of all
pressure ulcers in hospital settings.
The heel consistently ranks as the
second most common location for
pressure ulcers.
Acute care heel prevalence is between
8-17% (1992)
15-23% (1997)
(Dekeyser, Dejarger, Meyst and Evers, 1994)
(Barczak, Barnett, Childs, Bosley, 1997)
9

4
FACTSFACTS
Heel ulcers constitute 30% of all
pressure ulcers in hospital settings.
The heel consistently ranks as the
second most common location for
pressure ulcers.
Acute care heel prevalence is between
8-17% (1992)
15-23% (1997)
(Dekeyser, Dejarger, Meyst and Evers, 1994)
(Barczak, Barnett, Childs, Bosley, 1997)
What’s Wrong With This Picture?
10
Hospital Bed Simulation
Pressure = 19mmHg
(3” high density foam, air mattress and bed. Clothing)
11
12

5
13
60
50
40
30
20
10
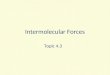
New Pressure UlcersIschial Tuberosity
Heel
Board 2” Foam 3” Foam 4” Foam Static
Air
Air on
FoamStrain % on Various Surface Type
50.1
10
4244
8.5
24.525.1
11.3
31.1
25
10.1
27.9
83
11.7
8
1.2
10.5
Greater Trochanter
Source: “Hospital Replacement
Mattresses.” “Journal of ET Nursing.”
Johnson, Daily & Franciscus.
Heel
Greater
Trochanter
Ischial Tuberosity
14
Criteria for lower extremity protectionCriteria for lower extremity protection
In a horizontal In a horizontal postionpostion::
1.1. Provide volumetric support of calfProvide volumetric support of calf
(circulation)(circulation)
2.2. Protect skin (address bony Protect skin (address bony
prominences)prominences)
3.3. Maintain skeletal integrity (Maintain skeletal integrity (footdropfootdrop
& lateral rotation)& lateral rotation)
15

6
Remember!RememberRemember!
No support surface by itself
adequately protects the heel
at all times.
16
17
18
7
19
20
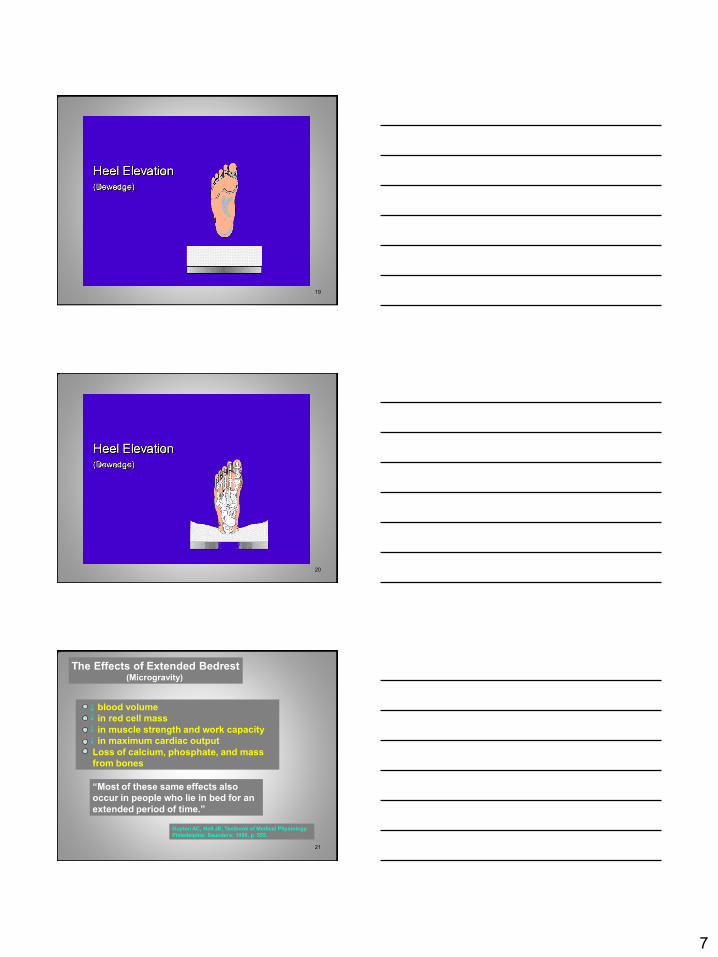
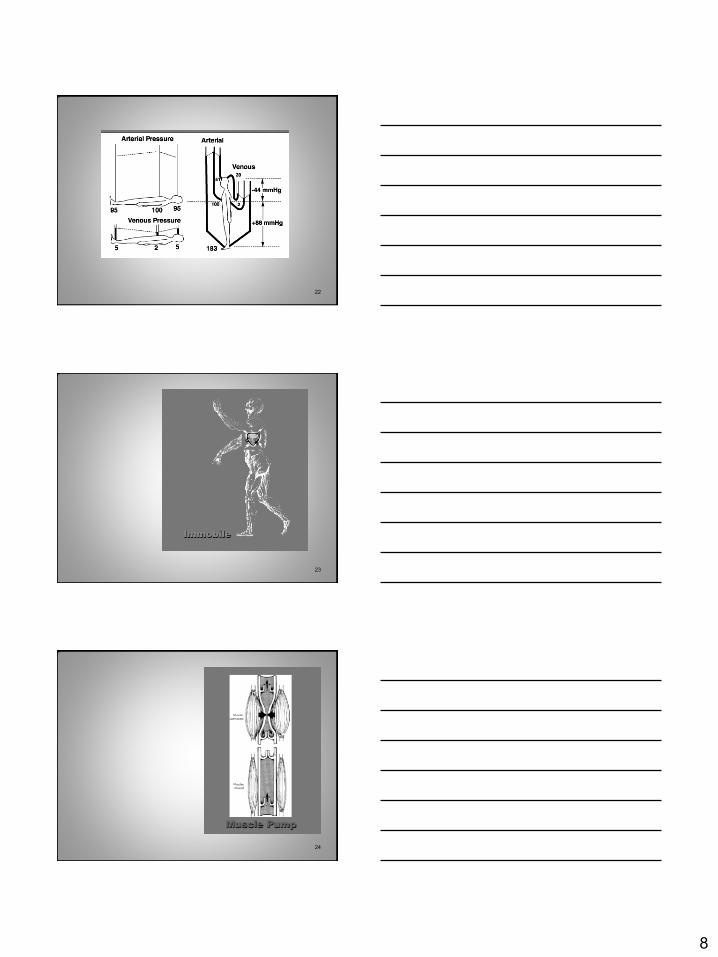
The Effects of Extended BedrestThe Effects of Extended Bedrest(Microgravity)
blood volume
in red cell mass
in muscle strength and work capacity
in maximum cardiac output
Loss of calcium, phosphate, and mass
from bones
“Most of these same effects also
occur in people who lie in bed for an
extended period of time.”
Guyton AC, Hall JE, Textbook of Medical Physiology.
Philadelphia: Saunders; 1996, p. 555.
21
8
22
23
24

9
Mobility Rating
Self Mobility
Assisted Mobility
Active Range of Motion
Passive Range of Motion
Immobility
25
NeutralNeutral
26
Venous
Dependency
27

10
28
29
30

11
31
Contouring Static Air
(Flotation)Contouring Solid
(Distortion)
32
Maintain Skeletal Integrity
Foot Drop
Lateral Rotation
Fractures
33

12
Foot Risk AwarenessFoot Risk Awareness
Peripheral vascular
Contracture of leg
Deformity of foot
Skin viability
Shape of heel
Arterial
Venous
General health
Durability
No Yes
34
Foot Risk AwarenessFoot Risk Awareness
Mobility of patientMobility of patient
+
=
Foot Risk assessment scaleFoot Risk assessment scale
Mobility of patientMobility of patient
Ambulatory
Ambulatory with assistance
Non-ambulatory
35
Clinical Protocols
Nutrition
Mobilization
Support Surface
Incontinence Care
Wound Care
Continuum of Care
Treatment of other general medical conditions
Ambulate
Turn
Passive Range of Motion
Bed, Chair, Cart, Emergency Room, Operating Room
Lower Extremity
Protection
36

13
Product Should:
Elevate heel (Dewedge)
Protect sides of foot and ankle
Neutralize weight of lower extremity (Delever)
Maintain and promote circulation
Address foot drop and lateral rotation of ankle
Allow access to the foot for
inspection/treatment
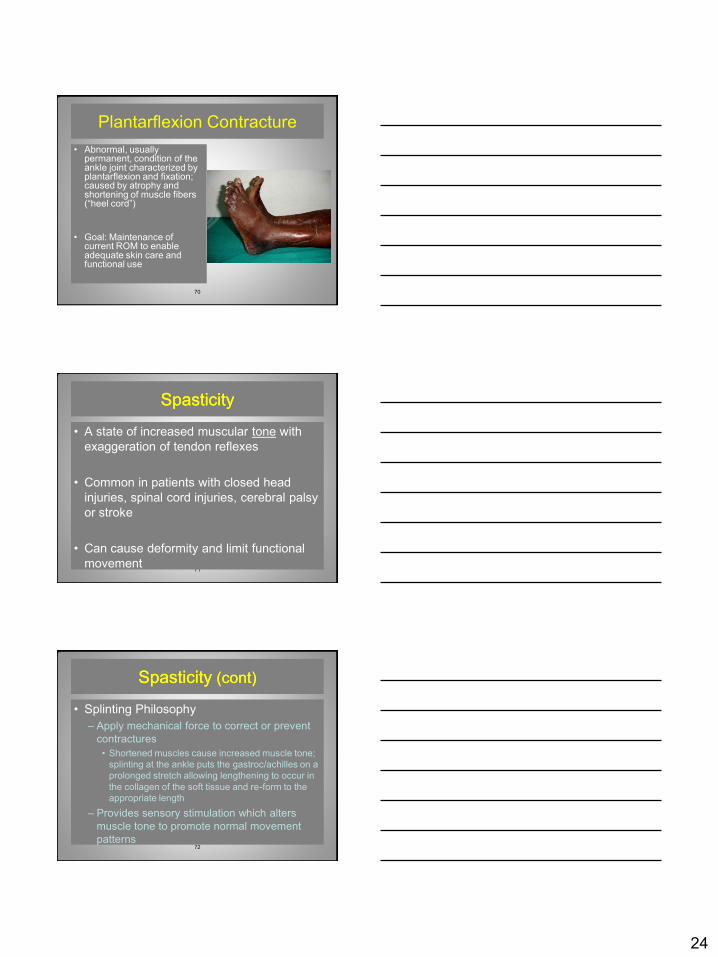
Facilitate the musculoskeletal pump
Fulfill regulatory requirements
37
38
Physical Therapy Physical Therapy Perspective on Ankle Foot Perspective on Ankle Foot
OrthosisOrthosis (AFO’s)(AFO’s)
JaimeeJaimee HaanHaan, PT CWS, PT CWS Sharon Lucich, PT CWSSharon Lucich, PT CWS
39
Basic Anatomy of the Basic Anatomy of the Lower ExtremityLower Extremity
14
40
General General TerminologyTerminology
•• Dorsal:Dorsal: (Dorsum)(Dorsum)–– Top of the footTop of the foot
•• Plantar: Plantar: –– Bottom of the footBottom of the foot
•• Medial:Medial:–– Towards midlineTowards midline
•• Lateral: Lateral: –– Away from midlineAway from midline
•• Proximal: Proximal: –– Nearer to the trunk Nearer to the trunk
•• Distal:Distal:–– Farther away from the trunkFarther away from the trunk Moore, K, Dalley, A: Clinically Oriented Anatomy, 5th Ed., 2006
41
Bones of the LegBones of the Leg
• Hip
– Pelvis
– Femur
• Thigh
– Femur
• Lower Leg
– Tibia
– Fibula
42
Bones of the Ankle and FootBones of the Ankle and Foot
Hoppenfeld, Stanley: Physical Examination of the Spine and Extremities, 1976

15
43
Main Muscles of the LegMain Muscles of the Leg
ANTERIOR:ANTERIOR:
• Knee extensors
– Quadriceps Femoris
•• Ankle Ankle DorsiflexorsDorsiflexors
– Anterior Tibialis
– Extensor Hallicus Longus
– Extensor Digitorum Longus
44
Main Muscles of the LegMain Muscles of the Leg
POSTERIOR:POSTERIOR:
•• Hip extensorsHip extensors–– Gluteus Gluteus MaximusMaximus (Buttock )(Buttock )
•• Knee flexors Knee flexors (Hamstrings)(Hamstrings)
–– Biceps Biceps FemorisFemoris
–– SemitendonosusSemitendonosus
–– SemimembranosusSemimembranosus
•• Ankle Ankle PlantarflexorsPlantarflexors
–– GastrocnemiusGastrocnemius
–– SoleusSoleus
–– Achilles TendonAchilles Tendon
45
Biomechanics of the Lower Biomechanics of the Lower ExtremityExtremity

16
46
Joint MotionJoint Motion
• Range of Motion: (ROM)
– The amount of motion available at a joint
• Active Range of Motion (AROM):
– Amount of motion available at a joint by a
subject during unassisted voluntary
movement
• Passive Range of Motion (PROM):
– Amount of motion available at a joint attained
by an examiner without the assistance of the
subject
47
• Goniometry:
– Measurement of joint
angles created by the
bones of the body
• Goniometer:
– Tool used for
goniometry
0o
45o
Knee ROM
30o
0o
Ankle ROM
48
ROM of the HipROM of the Hip
• Flexion:
– Bending of the hip joint
• Extension:
– Straightening of the hip
Joint

17
49
ROM of the HipROM of the Hip
• Abduction:
– Movement of the femur away
from midline
• Adduction:
– Movement of the femur
towards midline
50
ROM of the HipROM of the Hip
• External (or Lateral) Rotation:– Rotation of the femur away
from midline
• Internal (or Medial) Rotation:– Rotation of the femur toward
midline
• Neutral Position: – No internal or external rotation
51
ROM of the KneeROM of the Knee
• Flexion:
– Bending of the knee
• Extension:
– Straightening of the kneeHoppenfeld, Stanley: Physical Examination of the
Spine and Extremities, 1976
Hyperextension:Knee extension beyond
neutral

18
52
Common Types of Knee Common Types of Knee DeformityDeformity
• Genu Varum:
• Genu Valgum:
• Genu Recurvatum:
Hoppenfeld, Stanley: Physical Examination of the Spine and Extremities, 1976
53
ROM of the Foot and AnkleROM of the Foot and Ankle
• Plantarflexion:
– Ankle joint flexion
– Movement of the bottom of
the foot in the caudal (tail)
and posterior direction
• Dorsiflexion:
– Ankle joint extension
– Movement of the top of the
foot in the cranial (head)
and anterior direction
54
ROM of the Foot and ROM of the Foot and AnkleAnkle
• Abduction:
– Movement in a sideways
direction away from
midline of the foot
• Adduction:
– Movement in a sideways
direction towards midline

19
55
ROM of the Foot and AnkleROM of the Foot and Ankle
• Pronation:
– Rotation of the foot so that the sole of the foot faces a lateral (away from midline of the body) direction
• Supination:
– Rotation of the foot so that the sole of the foot faces a medial (toward midline of the body) direction
56
ROM of the Foot and AnkleROM of the Foot and Ankle
• Inversion:
– A combination of
supination and
adduction of the foot
• Eversion:
– A combination of
pronation and
abduction
57
Ankle AlignmentAnkle Alignment
• Neutral Position:– The ankle is considered to be
“in neutral” when the foot is at a right angle with the tibia
• Subtalar Neutral:– The point at which the
subtalar joint is fully supinated and then carried two-thirds of the way through maximum pronation
Relevance: when positioning a foot in a splint Relevance: when positioning a foot in a splint the goal is to achieve neutral alignment of the the goal is to achieve neutral alignment of the ankle and the ankle and the subtalarsubtalar jointjoint

20
58
59
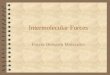
Gait Cycle
60
Standing Alignment and Standing Alignment and BalanceBalance
Base of Support

21
61
Phases of Gait CyclePhases of Gait CycleSTANCE PHASE SWING PHASE
62
Abnormal Gait PatternsAbnormal Gait Patterns
• Foot slap
– Weak dorsiflexors
cause foot to slap
down
– Occurs at the
beginning of heel
strike
63
Abnormal Gait PatternsAbnormal Gait Patterns
• Toe scuff
– Lack of dorsiflexion
– Occurs during midswing

22
64
Abnormal Gait Patterns
• High steppage gait
– Loss of dorsiflexion
– Inability to decelerate
dorsiflexors
– Knee lifts higher than normal
to allow foot to clear the floor
– Occurs during midswing
• Leg Length discrepancy ?
65
Abnormal Gait PatternsAbnormal Gait Patterns
• Hip hike
• Leg Length discrepancy?
66
Abnormal Gait PatternsAbnormal Gait Patterns
• Balance issues

23
67
Common Foot/Ankle Common Foot/Ankle
Impairments Requiring the Impairments Requiring the
Use of an AFO Use of an AFO
68
Foot DropFoot Drop
•• An abnormal neuromuscular An abnormal neuromuscular condition of the lower leg and condition of the lower leg and foot characterized by an inability foot characterized by an inability to to dorsiflexdorsiflex or or evertevert the footthe foot
•• May be due to damage to the May be due to damage to the Common Common PeronealPeroneal Nerve or Nerve or dorsiflexorsdorsiflexors
•• AFO can be used for treatment if AFO can be used for treatment if surgery not an optionsurgery not an option
69
Foot Drop Foot Drop (cont)(cont)
• Splinting Philosophy
– Stabilize ankle in neutral position to maintain
functional ankle range of motion to allow
standing and ambulation (walking)
– Provide medial and lateral stabilization of the
hip joint (Use stabilization bar if available on
the AFO)
24
70
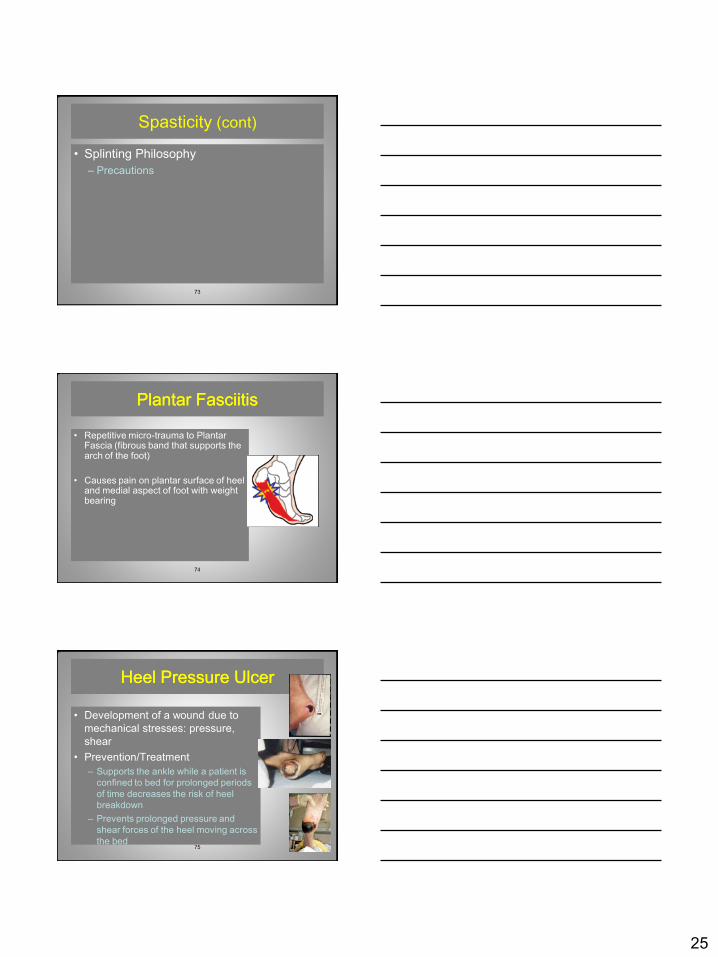
Plantarflexion Contracture
• Abnormal, usually permanent, condition of the ankle joint characterized by plantarflexion and fixation; caused by atrophy and shortening of muscle fibers (“heel cord”)
• Goal: Maintenance of current ROM to enable adequate skin care and functional use
71
SpasticitySpasticity
• A state of increased muscular tone with
exaggeration of tendon reflexes
• Common in patients with closed head
injuries, spinal cord injuries, cerebral palsy
or stroke
• Can cause deformity and limit functional
movement
72
Spasticity Spasticity (cont)(cont)
• Splinting Philosophy
– Apply mechanical force to correct or prevent
contractures
• Shortened muscles cause increased muscle tone;
splinting at the ankle puts the gastroc/achilles on a
prolonged stretch allowing lengthening to occur in
the collagen of the soft tissue and re-form to the
appropriate length
– Provides sensory stimulation which alters
muscle tone to promote normal movement
patterns
25
73
Spasticity (cont)
• Splinting Philosophy
– Precautions
74
Plantar FasciitisPlantar Fasciitis
• Repetitive micro-trauma to Plantar Fascia (fibrous band that supports the arch of the foot)
• Causes pain on plantar surface of heel and medial aspect of foot with weight bearing
75
Heel Pressure UlcerHeel Pressure Ulcer
• Development of a wound due to
mechanical stresses: pressure,
shear
• Prevention/Treatment
– Supports the ankle while a patient is
confined to bed for prolonged periods
of time decreases the risk of heel
breakdown
– Prevents prolonged pressure and
shear forces of the heel moving across
the bed

26
76
General Splinting
Terminology and
Techniques
77
Common TerminologyCommon Terminology
• Splint:
– An orthopedic device for immobilization,
restraint, or support of any part of the body
• Orthosis:
– A force system designed to control, correct, or
compensate for a bone deformity, deforming
forces, or forces absent from the body
78
Traditional OrthoticsTraditional Orthotics
• Posterior leaf spring AFO
• Patellar-tibia bearing AFO
• Floor reaction AFO
• Conventional AFO

27
79
Traditional Orthotics
• Foot or Shoe Orthotic (Insole)– Diabetics
– Pronated/Supinated foot
• Hinged ankle foot orthosis
• Rigid ankle foot orthosis
80
Rigid Ankle Foot Rigid Ankle Foot OrthosisOrthosis (AFO)(AFO)
• Static Splints
– Immobilize
– Help prevent further
deformity
– Help prevent
contractures
Heel Heel PresurePresure Relieving Ankle Relieving Ankle
Foot Foot OrthosisOrthosis (AFO)(AFO)
81

28
Heel Heel PresurePresure Relieving Ankle Relieving Ankle
Foot Foot OrthosisOrthosis (AFO)(AFO)
82
83
Splinting (AFO) PrecautionsSplinting (AFO) Precautions
• Fit
– An ill-fitting ankle-foot orthosis can cause harm to the patient
– The ankle joint should be positioned in the splint at the correct therapeutic angle
– When a patient wears an AFO with padding in supine (lying on their back), the distal tibia is elevated relative to the proximal tibia and femur; This encourages knee hyperextension
– Signs of improper fit: skin redness, edema (swelling), joint stiffness, pain, skin rash, decreased circulation
84
Splinting (AFO) PrecautionsSplinting (AFO) Precautions
• Skin Assessment
– The clinician should don the AFO properly and leave in place for 20-30 minutes
– Red areas should not be present 20 minutes after removal of AFO
– Educate patient/family to report any rashes or other skin reactions
• Edema Assessment
– If AFO straps are applied too tight, issues with edema above and below straps may result and can cause skin breakdown.
29
85
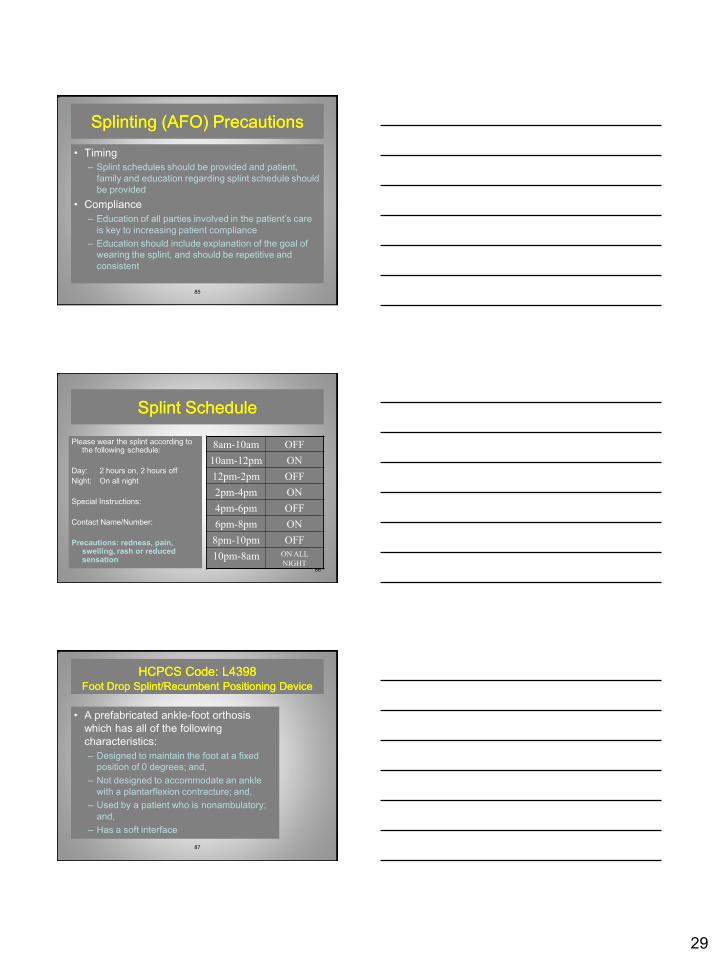
Splinting (AFO) PrecautionsSplinting (AFO) Precautions
• Timing
– Splint schedules should be provided and patient,
family and education regarding splint schedule should
be provided
• Compliance
– Education of all parties involved in the patient’s care
is key to increasing patient compliance
– Education should include explanation of the goal of
wearing the splint, and should be repetitive and
consistent
86
Splint ScheduleSplint Schedule
Please wear the splint according to the following schedule:
Day: 2 hours on, 2 hours off
Night: On all night
Special Instructions:
Contact Name/Number:
Precautions: redness, pain, swelling, rash or reduced sensation
8am-10am OFF
10am-12pm ON
12pm-2pm OFF
2pm-4pm ON
4pm-6pm OFF
6pm-8pm ON
8pm-10pm OFF
10pm-8am ON ALL
NIGHT
87
HCPCS Code: L4398HCPCS Code: L4398Foot Drop Splint/Recumbent Positioning DeviceFoot Drop Splint/Recumbent Positioning Device
• A prefabricated ankle-foot orthosis
which has all of the following
characteristics:
– Designed to maintain the foot at a fixed
position of 0 degrees; and,
– Not designed to accommodate an ankle
with a plantarflexion contracture; and,
– Used by a patient who is nonambulatory;
and,
– Has a soft interface
30
88
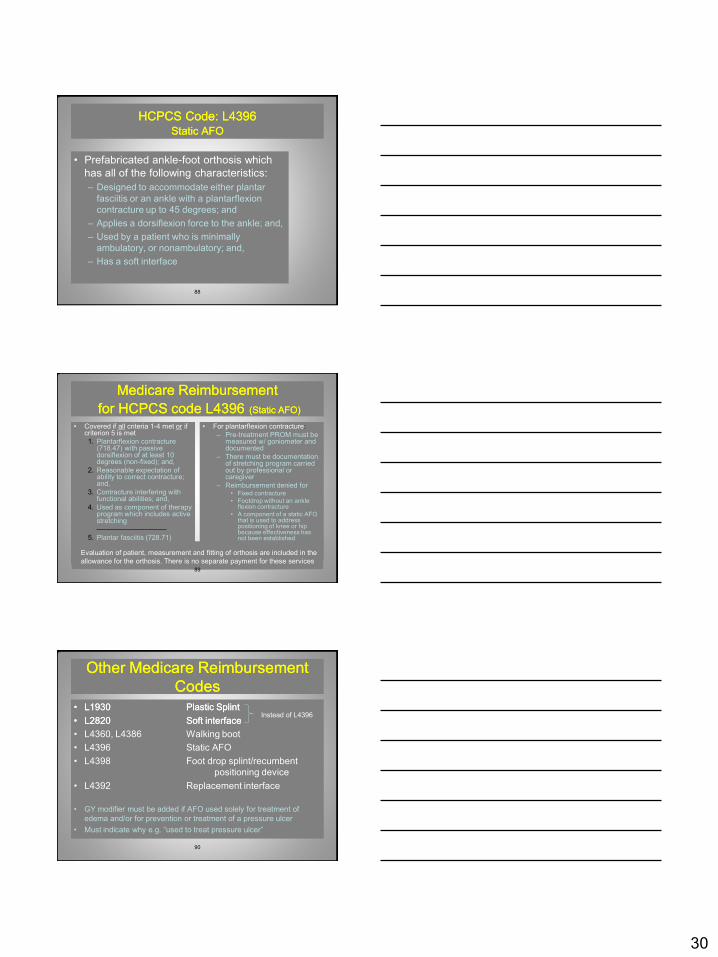
HCPCS Code: L4396HCPCS Code: L4396Static AFOStatic AFO
• Prefabricated ankle-foot orthosis which
has all of the following characteristics:
– Designed to accommodate either plantar
fasciitis or an ankle with a plantarflexion
contracture up to 45 degrees; and
– Applies a dorsiflexion force to the ankle; and,
– Used by a patient who is minimally
ambulatory, or nonambulatory; and,
– Has a soft interface
89
Medicare ReimbursementMedicare Reimbursement
for HCPCS code L4396for HCPCS code L4396 (Static AFO)(Static AFO)
• Covered if all criteria 1-4 met or if criterion 5 is met
1. Plantarflexion contracture (718.47) with passive dorsiflexion of at least 10 degrees (non-fixed); and,
2. Reasonable expectation of ability to correct contracture; and,
3. Contracture interfering with functional abilities; and,
4. Used as component of therapy program which includes active stretching
5. Plantar fasciitis (728.71)
• For plantarflexion contracture:
– Pre-treatment PROM must be measured w/ goniometer and documented
– There must be documentation of stretching program carried out by professional or caregiver
– Reimbursement denied for• Fixed contracture
• Footdrop without an ankle flexion contracture
• A component of a static AFO that is used to address positioning of knee or hip because effectiveness has not been established
Evaluation of patient, measurement and fitting of orthosis are included in the
allowance for the orthosis. There is no separate payment for these services
90
Other Medicare Reimbursement Other Medicare Reimbursement
CodesCodes
•• L1930 L1930 Plastic SplintPlastic Splint
•• L2820 L2820 Soft interfaceSoft interface
• L4360, L4386 Walking boot
• L4396 Static AFO
• L4398 Foot drop splint/recumbent
positioning device
• L4392 Replacement interface
• GY modifier must be added if AFO used solely for treatment of
edema and/or for prevention or treatment of a pressure ulcer
• Must indicate why e.g. “used to treat pressure ulcer”
Instead of L4396

31
91
Questions??Questions??
92
Thank You!Thank You!
Jaimee Haan, PT, CWS [email protected]
Sharon Lucich, PT, CWS [email protected]