Embed Size (px)
Citation preview

Factors Determining the Activity of lschemic Heart Disease
STEPHEN CAMPBELL, B.Sc., M.R.C.P. MICHAEL B. ROCCO, M.D. ELIZABETH G. NABEL, M.D. JOAN BARRY, B.A. GEORGE S. REBECCA, M.D. JOHN E. DEANFIELD, M.R.C.P. ANDREW P. SELWYN, M.D.
Boston, Massachusetts
From the Department of Medicine (Cardiovascular Division), Brigham and Women’s Hospital, Harvard Medical School, Boston, Massachusetts. This work was done during the tenure of a British-American Research Fellowship of the American Heart Asso- ciation and the British Heart Foundation, with Dr. Stephen Campbell the recipient. Requests for re- prints should be addressed to Dr. Andrew P. Sel- wyn, Cardiovascular Division, Brigham and Wom- en’s Hospital, 75 Francis Street, Boston, Massa- chusetts 02115.
Transient regional myocardial ischemia appears to underlie symp toms such as angina pectoris and represents a key pathophysio- logic step, since it is an objective marker of disease activity and is capable of causing disabling symptoms and damage to left ventric- ular myocardium. A study of the characteristics of transient ische- mia in and out of the hospital has shown that symptoms are an inconsistent underestimation of these events. lschemia is generally prolonged, mostly asymptomatic, and usually accompanied by a regional decrease in myocardial perfusion. Studies out of the hospi- tal have also shown that these episodes are frequently triggered by a wide range of ordinary everyday activities. These new features of transient ischemia are worth noting when searching for relevant causes that are present during everyday life and when trying to choose more rational therapy. More detailed studies of patient activ- ity have shown that different levels of mental arousal are the most common triggering mechanism causing ischemia out of the hospi- tal. In addition, the occurrence of transient ischemia during every day life displays a circadian rhythm, with an increase and peak oc- currence between 6:00 A.M. and 12 noon each day. The day-to-day variability of ischemia is marked, indicating functional disturbances of coronary stenoses against a background of a severe reduction in cross-sectional area. The examination of proximal stenoses has shown that (1) the reduction in cross-sectional area is usually un- derestimated by conventional angiography; (2) pressure gradients across coronary stenoses are common and, with reduced postste- notic blood pressure, can jeopardize perfusion; (3) disturbances of vessel caliber and antegrade flow can accompany many of the ordi- nary everyday activities known to trigger ischemia detected in Hol- ter tapes studied out of the hospital; and (4) there is clear-cut evi- dence of endothelial dysfunction in these patients, with reversal of the normal dilator response to acetylcholine and paradoxical con- striction of stenoses. This evidence of endothelial dysfunction in humans could be central to the problems of atheromatous narrow- ing, thrombus, and disturbed vasomotion.
Despite evidence of a recent decline [I ,2] in ischemic heart disease, it remains the major cause of mortality in the United States, accounting for 500,000 deaths annually [3], many of which are sudden and unexpected. This mortality rate is overwhelmingly due to coronary atherosclerosis that develops over two or three decades [4] with no clinical manifestations until plaque development is sufficient to cause significant reductions in the cross-sectional areas of epicardial coronary arteries [5]. Despite the
April 30, 1986 The American Journal of Medicine Volume 80 (suppl 4C) 9

SYMPOSIUM ON EXPLORING MYOCARDIAL ISCHEMIA-CAMPBELL ET AL
Afegofve F&back
1 Descefdhg 5 H-TNeuron
-I h Dorso/afero/
Funicu/us
- - Primary -
\tt- Sympafiefk _
Figure 7. Schematic diagram of path- ways that are likely to participate in car- diac nociception. Free nerve endings of ventricular sympathetic afferents are ex- cited by a variety of chemical and me- chanical stimuli that may be produced during ischemia. Modulation of the sen- sory input may then occur at a spinal segmental level by both local and de- scending inputs. The latter may involve a system that is proposed to descend from the periaqueductal gray (PAG) of the midbrain via the nucleus raphe magnus (NRM) of the medulla and involve enkephalin (E) and serotonergic (5H-T) neurons. This system would act to inhibit the primary nociceptive afferents and may be stimulated by secondary afferent fibers via the reticular formation and nu- cleus raphe magnus, thus forming a neg- ative feedback loop for modulation of pain sensation.
many therapeutic modalities currently available, the out- look for patients with coronary disease is quite different from that of a population with normal coronary arteries [6]. It is, therefore, reasonable to search for those factors that determine the onset of “activity” of ischemic heart dis- ease-i.e., the point at which previously clinically silent coronary atherosclerosis becomes complicated by the occurrence of transient regional myocardial ischemia that may result in symptoms and damage to the ventricular myocardium [7].
The aims of this article are to reexamine the role of chest pain in the assessment of clinical ischemic heart disease activity; to consider the new information available concerning the nature and causes of transient ischemic activity that occurs out of the hospital and that underlies the symptoms of coronary artery disease; and to examine what is known about the changing pathology of coronary
atherosclerosis and how it may cause the exacerbations and remissions of ischemic heart disease activity ob- served in most patients.
PATHOPHYSIOLOGY OF CARDIAC PAIN
Cardiac nociception is believed to be subserved mainly by primary sympathetic afferents [8-111. These run in the cardiac nerves to the upper five thoracic sympathetic gan- glia and thence, primarily via white rami communicantes to the upper five thoracic dorsal roots of the spinal cord [8,9]. Within the cord, the sympathetic afferents synapse with secondary afferents of the spinothalamic tract that ascend to the thalamus, from which projections may pass to the cortex. Some contribution from vagal afferents may also play a role, especially in referred pain [9].
The precise nature of the nociceptors remains un- known, but they are probably free nerve endings that may
10 April 30, 1988 The American Journal of Medicine Volume 80 (suppl 4C)

SYMPOSIUM ON EXPLORING MYOCARDIAL ISCHEMIA-CAMPBELL ET AL
Faiher Q
82 to S9 one minute b;e;fOrb
Ewv 0 d 0
ACW77-Y Driving a cai
Tgurc? 2. Ari example of 2 typical lo-minutb e&ode of painless ST-segment depression that occurred while a patient wit; angina and coronary attery disease was driving a car.
be responsive to both mechanical and local chemical stimuli [9]. These local chemical stimuli probably include bradykinin [9,12], potassium [13], and acids [9,14], all of which are produced during ischemia [15-171. These stim- uli appear to exhibit threshold and interactive effects that may be important in niodujating bain at the level of the receptor. In addition, there is, now considerable exljeri- mental evidence that nociceptive stimuli may be extenz sively modulated within the central nervous system via both segmental [18] and higher mechanisms. [I g-211. Some of the mechanisms proposed would appear to in- volve endogenous opioid neurotransmitters [19:21], al- though nonopioid systems are probably also involved [2i]. Thus, the potential for modulation of cardiac pain exists at many levels, as illustrated schematically in Fig& 1; therefore, it should not be surprising that pain may be a very unpredictable symptom on the basis of these mecha- nisms alohe.
PAIN AS A MARKET 6~ ISCHEMIA
In clinical practice, chest pain is still used as a guide to disease “activity” in patients with ischemic heart disease, although the development of ischemia unaccompanied by pain has frequently been observed during various forms of stress testing [23-261. Numerous studies using ambula- tory monitoring of the ST-T segment in symijtomatic pa- tients tvith known or probable coronary artery disease [27- 33] have shown that the majority of ischemfc episodes (59
April 30, 1988 The American Journal of Medicine Volume 80 (suppl 4C)
to 87 percent) that occur during normal daily activities are, in fact, asymptomatic. Figure 2 illustrates this point. In addition, the 30-year follow-up of the Framingham Study [34] confirmed that more, than 25 percent of myocardial infarctions in a “general population” may occur unrecog- nizedi and about half of these may be silent.
Thus, although ischemia .may indeed result in chest pain, the relationship betwe,&, the two is unpredictable. Accordingly, chest pain must now be regarded as an un- reliable marker of the frequency, and perhaps the sever- ity, of ischemic events in patients with coronary artery dis- ease.
MYOCARdlAL ISCHEMIA Il’i CilNlCAL PRACTiCE
fvluch has been learned from.the experimental laboratory about the effects of transient regional ischemia on the myocardium [7,35] and its evolution to myocardial infarc- tion [36]. However, beyond the useful principle of imbdl- ahce between’ supply and demand, it seems cieai that there is no satisfactory experimental model for the charac- ter or causes of ischemic heart disease activity in humans. The severity of angina pecioris [371 and the ability to elicit evidence of ischemia during stress testing, especially at low workloads [38] and even in the absence of symptoms [39,40], are now kho?n to be associated with an adverse prognosjs. This evidence of ischemjc heart disease activ- ity can therefore be used to assess prognosis without ie- gard to coronary anatomy and left ventricular function.
11

SYMPOSIUM ON EXPLORING MYOCARDIAL ISCHEMIA-CAMPBELL ET AL
CONTROL SMOKING
EXERCISE POST.
15 MINS POST.
-
Indeed, the traditional use of the assessment of coronary occlusive disease and the extent of damage to ventricular function takes into account only established and appar- ently fixed changes in epicardial coronary arteries and contractile function of the heart, whereas the study and understanding of transient ischemia addresses a poten- tially damaging, but reversible, aspect of the disease.
Transient ST-segment depression ,during ambulatory monitoring has been validated as a reasonable and quan- titative marker of isctiemic heart disease activity in people with typical angina and proven, coronary disease [33]. It has been demonstrated that these patients commonly have asymptomatic myocardial ischemia that is surpris- ihgly prolonged and that js triggered by a variety of every- day activities [28,29,31,32]. This raises the issue in each patient of the “total ischemic activity,” which may need management apart from the traditional approach to the relief of chest pain.
Positron emission tomography has been used to mea- sure the regional myocaibial uptake of rubidium-82 as a marker of regional coronary blood flow [32,33,41]. Normal subjects show homogeneous increases in regional myo- cardial perfus/on with exposure to cold, mental arithmetic, and exercise, whereas patients with angina and coronary disease show inhomogeneous regional perfusion charac- terized by increased perfusion in remote areas and abso- lute decreases in perfusion in poststenotic segments of the myocardium [33]. As shown in the examples (hgbres 3 and 4), ischemic disturbances in regional myocardial perfusion may occur spontaneously or in response to a
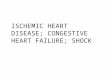
Figure 3. Positron emission tomograms dembnstrating changes in regipnal myo- cardial uptake of rubidium-82 during smoking and exercise. Note thai the con- trol scan shows uniform uptdke; with smoking and exercise, .defects appear in the anterior and free walls of the left ven- tricle (arrows) and resolve thereafter.
variety of stimuli (exercise, mental arithmetic, cold expo- sure, cigarette smoking), but neariy always include an absolute decrease in perfusion in the affected segment (Figure 5). This may occur because of a pathologic de- crease in poststenotic perfusion pressure and a failure of endocardial perfusion, both caused by an increased myo- cardial oxygen demand and dilation of the resistance ves- sels in the presence of fixed critical stenoses; collapse of the distal stenosis and poststenotic epicardial coronary artery segment owing to a pathologic decrease in the poststenotic distending pressure; sympathetically medi- ated constriction of epicardial coronary arteries around a critical segmental narrowing due to atherosclerosis; or an inappropriate reaction of critically stenosed epicardial cor- onary arteries to neurohumoral and/or cellular factors because of vasomotor dysfunction resulting from the presence of atherosclerotic lesions (to be discussed later).
The examples shown in the figures demonstrate that different patterns of disturbed regional perfusion can de- velop in each patient. Stimuli such as exercise cause in- creased perfusion in remote areas of the myocardium, presumably in response to the increase in the double product and myocardial oxygen demand. At the same time, the affected segment shows-a decrease in perfusion [32,33], This type of response appears to be associated with both chest pain and electrocardiographic signs of is- chemia [32,33]. Conversely, cold exposure and spontane- ous ischemia are associated with a much smaller increase in the double product and, therefore, less of an increase in
12 April 30, 1988 The American Journal of Medicine Volume 80 (suppl 4C)

SYMPOSIUM ON EXPLORING MYOCARDIAL ISCHEMIA-CAMPBELL E-f AL
Figure 4. Regional myocardial cfistribu- tion of rubidium-82 in positron emission tomograms during spontaneous epi- sodes of ischemia and mental arithmetic stress in a patient with previous anterior infarction. Note the fixed anterior defect; during the spontaneous and stress- induced episodes, the defect enlarges (arrows) to include the septum. These changes are reversible, as seen after administration of isosorbide dinitrate (ISDN).
perfusion in remote areas of the myocardium; however, these types of ischemia still show a decrease in perfusion in the affected segment. This sequence of events is usu- ally “silent” [32,33]. The rational approach to the treat: ment of these ischemic disturbances in regional coronary blood flow must consider the invariably occurring de- creases in regional perfusion. Since the occurrence of pain and electrocardiographic signs of ischemia seem to depend on the affected segment’s being subjected to both decreased perfusion and increased demand [32], therapy should probably be directed toward both mechanisms.
THE “ACTIVE” CORONARY LESION
The vast majority of patients presenting with clinical signs of ischemic heart disease already have important ather- omatous narrowing of at least one epicardial coronary ar- tery [42]. The severity of these lesions is underestimated by conventional at-teriography [43-453. However, quanti- tative arteriography has shown that the minimum cross- sectional area appears to be the major static factor affect- ing flow [5], although determinants such as lesion length, eccentricity [46], and collaterals [47] are also important. Nevertheless, this simple understanding does not explain the fluctuating exacerbations and remissions in disease activity that typically affect these patients. Recent experi- mental, pathologic, and clinical research has elucidated a number of pathophysiologic features in the evolution of atheromatous lesions that might well explain the fluctuat- ing clinical activity. These physical, humoral, and cellular factors may be central not only to the further development of atheroma but also to the functional disturbances that lead to the “active ischemic state,” with all its attendant symptoms, morbidity, and mortality.
DEVELOPMENT OF PLAQUE
The processes responsible for atherogenesis [4] result in disease progression that eventually may produce fixed stenosis that is sufficient to produce impairment of flow. This impairment initially occurs in the context of increased demand; eventually, it occurs even at rest. This process is usually gradual, but plaques can enlarge rapidly. Evi- dence of disease progression in vivo has been demon- strated in a series of patients restudied angiographically shortly after an episode of unstable angina [48]. Stenoses in unstable angina also have been noted to be more com- plex and associated with thrombus more often than ste- noses occurring in patients with stable symptoms [49,50]. Plaque development changes the normal elastic proper- ties of a vessel wall, and fissuring, hemorrhage, and rup- ture can abruptly worsen the lesion [51].
THROMBOSIS
The role of platelets in classic stable angina related to increased myocardial oxygen demand is uncertain [52-- 541, but platelets have been implicated in unstable angina [55], myocardial infarction [SS], and sudden death [57]. Indeed, platelet deposition, with subsequent aggregation and release of thromboxane A2 and other vasoactive sub- stances, including platelet-derived growth factor [58], may play a pivotal role in the development of acute ischemic syndromes [40]. These processes are normally inhibited by the presence of an intact endothelium; this may be due, in part, to the production of prostacyclin, but also may be attributable to an endothelial-dependent dilatation trig- gered by platelet products [40]. This tends to lead to in- creased flow and inhibition of further aggregation. When
April 30, 1986 The American Journal of Medicine Volume 60 (suppi 4C) 13

SYMPOSIUM ON EXPLORING MYOCARDIAL ISCHEMIA-CAMPBELL ET AL
Control Exercise Control Spontaneous
I 1 SepWlTl Apex Free Wall Septum Apex Free Wall
Regions of Myocardium
Figure 5. Patient with three-vessel coro- nary artery disease had tomograms (scans) of the heart recorded before arid after exercise (left), and before and dur- ing spontaneous ST-segment depressidn (right). Arrows indicate the ischemic decrease in regional perfusion affecting the free wall of the left ventricle. The graphic scale below shows the perfusion in each segment of the scan and demori- strates decreased perfusion that occurs due to exercise and duritig unbroifoked events. However, perfusion in remote areas increases only with. exercise. This example demonstrates two different eat- tenis of disturbed coronary blood flow, both leading to ischemia in’ the same pa- tient.
the endothelium is not intact, as may be the case in the vicinity of an atheromatous plaque, these protective pechanisms can break down; this !eads to platelet aggre- gation, vasoconstriction, and, possibly, generation of p!atelet mitiroemboli, resulting in physical ,and vasocon- strictive obstnictions in downstream vessels [40,59].
This hypothesis is supported by the fact that elevated throtnboxane B2 levels (the inactive metabolite of throm- boxane AZ) have been found in the coronary sinus effluent of patients with unstable angina [bO]. iutthermore, Animal studies @I,621 have demonstrated cyclic reductions in flow resulting from platelet deposition at the site of severe exp&imehtaily produced coronary stenoses; these reduc- tions can be abolished by aspirin and dazoxiben. Finally, daily administration of 324 rnd of aspirin h&s been shown to reduce the mortality rate aiid risk of myocardial infarc: tion after an episode of unstable angina [63].
Plaielets may also influetlce disease activity by their participation in the actual process of atherogenesis, as pqstulated in the “response t? injury” hypothesis [64].
Coagulation’is also undoubtedly important in the devel- opment of acute manifest&ohs of ischemic heart disease [65,66] and may be a major factor in disease progression [65]. The role of thrombosis in the pathophysiology of cor- onary artery disease has b&en recognized for many years and was classically described by Herrick [67] in 1912.
Occlusive coronary thrombus has been found in up to 90 percent df patients dying shortly after infarction [51]; based qn these fivdings, there have been many recent trials of early acute thrombolysis [68,69].
Thrombdsis, usually nonocclusive and possibly oc+- ring iri a layered fashion, has also been noted in unstable angina [5b]. Two interventibnal studies of the role of thrombosis in unstable angina demonstrated a therapeu- tic benefit qf fibrinol#ic ‘and apticoagulant therapy in pre- venting death an,d/or infarction [70,71].
VASOMOTION OF EPlCARi+L CORONARY ARTERIES
Epicardiai doronary arteries constrict and relax in re- sponse to a wide variety of humoral and neural factors [72], everl when they are severely diseased [73].Tfiis vas- omotor activity is part’of their normal function and usually of little consequenke, but it may lead to severe ischemia, especially in the presence of critical atheromatljus nar- rowing [74-771. Many-of the external stimuli,known to trig- ger myocardial ischemia d,uring daily life produce sympa- thetically mediated constriction of these epicardial vessels [72]; this, in turn, causes a critical increase in resistance and a decrease in flow, even when modesi constriction occurs, in or around an atheromatous stenosis. The con- striction of epicardial vessels may be mediated vi” alpha, sympathetic activity, alterations in vessel reactivity due to
14 April 30, 1988 The American Journal of Medicine Volume 80 (suppl 4C)

SYMPOSIUM ON EXPLORING MYOCARDIAL ISCHEMIA-CAMPBELL ET AL
incorporation of cholesterol into smooth muscle cells, a decrease in the number of affinity or inhibitory alpha2 re- ceptors, or platelet vessel wall interactions resulting in the release of various vasoactive substances [78].
ENDOTHELIAL-DEPENDENT DILATION OF EPICARDIAL ARTERIES
Even more exciting is the recent evidence that normal di- lation of muscular arteries such as epicardial coronary ar- teries occurs in response to a varfety of physiologic stimuli but is dependent upon intact and functioning endothelium [78,79]. Endothelial dysfunction may inhibit this dilator response and even lead to paradoxical constriction. Furchgott [79] postulated the release of an endothelial- dependent relaxant factor, and this notion has been closely examined in a variety of experimental models [80]. More recently, Ludmer et al [81] demonstrated that this mechanism is active and important in patients with an- gina, positive exercise test results, and atheromatous le- sions in epicardial coronary arteries. The release of this endothelial-dependent relaxant factor is stimulated by a variety of substances, such as acetylcholine, adenosine diphosphate, histamine, thrombin, and various physio- logic peptides [80]. This relaxant factor has a very short half-life (six seconds) and appears to act by elevating lev- els of smooth muscle cell cyclic guanosine monophos- phate, an intracellular inhibitor of smooth muscle cell con- traction.
ENDOTHELIAL DYSFUNCTION AS A CENTRAL PATHOPHYSIOLOGIC PROBLEM
There is much evidence that endothelial dysfunction or disruption may be the necessary first step in the develop- ment of atherosclerosis [4,64]. Additionally, there is evi- dence that local endothelial injury promotes platelet depo- sition and thrombosis [40] and that a dysfunctional endo-
thelium also results in disturbed vasomotion, failure of normal dilation, and even paradoxical constriction. All this evidence suggests that endothelial dysfunction may be a central pathophysiologic event, determining the tendency for thrombosis and disturbed vasomotion, as well as ath- erogenesis. It is, therefore, particularly interesting that clinical research to date has identified the development of atheromatous lesions, the tendency for thrombosis, and disturbed vasomotion as the pathophysiologic mecha- nisms most important in and most likely to give rise to the activation of ischemic heart disease, producing symp- toms, morbidity, and mortality.
COMMENTS
In conclusion, an important goal of the management of coronary artery disease is to understand and treat mani- festations of ischemia before the atheromatous occlusion of vessels and damage to left ventricular myocardium occur. Observations in patients with angina have already shown frequent and prolonged ischemic activity that is predominantly silent and associated with ordinary activi- ties that represent extrinsic trigger mechanisms.
The fluctuating activity of ischemic heart disease cannot be due only to these external stimuli; it also must be due to intrinsic pathophysiologic factors in the atherosclerotic epicardial vessels. There is evidence of endothelial dys- function at the site of atheromatous lesions in the coro- nary arteries of patients with angina and active ischemic heart disease that may account for the challenging prob- lems of worsening stenosis due to atheroma, the ten- dency for thrombosis, and disturbed vasomotion. Future research must determine the optimal treatment for this ischemic activity. It may be that understanding and treat- ing endothelial dysfunction, and thus promoting healing of active atheromatous lesions, are necessary to achieve control of ischemia.
REFERENCES
1. Feinleib M, Havlik RJ, Thorn TJ: The changing pattern of ische- mic head disease. J Cardiovasc Med 1982; 7: 139-148.
2. Goldman L, Cook EF: The decline in ischemic heart disease mortality rates. An analysis of the comparative effects of med- ical interventions and changes in lifestyle. Ann Intern Med 1984; 101: 825-836.
3. U.S. Bureau of the Census statistical abstract of the United States: 1985 (105th edition). Washington, DC, 1984; 74-77.
4. McGill HC Jr: Persistent problems in the pathogenesis of ather- osclerosis. George Lyman Duff Memorial Lecture. Arterio- sclerosis 1984; 4: 443-451.
5. Harrison DG, White CW, Hiratzka LF, et al: The value of lesion cross-sectional area determined by quantitative coronary angiography in assessing the physiologic significance of prox- imal left anterior descending coronary arterial stenoses. Cir- culation 1984; 69: 1111-l 119.
6. Cohn PF, Braunwald E: Chronic ischemic heart disease. In: Braunwald E, ed. Heart disease, a textbook of cardiovascular medicine. Philadelphia: WB Saunders, 1984; 1334-l 383.
7. Sobel BE, Braunwald E: Coronary blood flow and myocardial ischemia. In: Braunwald E, ed. Heart disease, a textbook of
April 30, 1986 The American Journal of Medicine Volume 80 (Suppi 4C)
8.
9.
10.
11.
12.
13.
14.
15.
cardiovascular medicine. Philadelphia: WB Saunders, 1984; 1235-1261.
White JC: Cardiac pain. Anatomic pathways and physiologic mechanisms. Circulation 1957; 16: 644-655.
Malliani A, Lombardi F: Consideration of the fundamental mech- anisms eliciting cardiac pain. Am Heart J 1982; 103: 575- 578.
Lindgren I, Olivecrona H: Surgical treatment of angina pectoris. J Neurosurg 1947; 4: 19-39.
Brown AM: Excitation of afferent cardiac sympathetic nerve fi- bers during myocardial ischaemia. J Physiol (Land) 1967; 190: 35-53.
Uchida Y, Murao S: Bradykinin-induced excitation of afferent cardiac sympathetic nerve fibers. Jpn Heart J 1974; 15: 84- 91.
Uchida Y, Murao S: Potassium-induced excitation of afferent cardiac sympathetic nerve fibers. Am J Physiol 1974; 226 (3): 603-607.
Uchida Y, Murao S: Acid-induced excitation of afferent cardiac sympathetic nerve fibers. Am J Physiol 1975; 228: 27-33.
Kimura E, Hashimoto K, Furukawa S, Hayakawa H: Changes in
15

SYMI POSIUM ON EXPLORING MYOCARDIAL ISCHEMIA-CAMPBELL ET AL
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37. Hultgren HN, Peduzzi P: Relation of severity of symptoms to 59.
bradykinin level in coronary sinus blood after the experimental occlusion of a coronary artery. Am Heart J 1973; 85: 63% 647.
Haddy FJ, Scott JB: Bioassay and other evidence for participa- tion of chemical factors in local regulation of blood flow. Circ Res 1971; 28-29 (suppl I): l-86-1-92.
Cobbe SM, Poole-Wilson PA: Continuous coronary sinus and arterial pH monitoring during pacing-induced ischaemia in coronary artery disease. Br Heart J 1982; 47: 369-374.
Melzack R, Wall PD: Pain mechanisms: a new theory. Science 1965; 150: 971-979.
Mense S: Basic neurobiologic mechanisms of pain and analge- sia. Am J Med 1983; 75 (suppl 5A): 4-14.
Edmeads J: The physiology of pain: a review. Prog Neuro- psychopharmacol Biol Psychiat 1983; 7: 413-419.
Fields HL: Neurophysiology of pain and pain modulation. Am J Med 1984; 77 (suppl 3A): 2-8.
Watkins LR, Mayer DJ: Organization of endogenous opiate and nonopiate pain control systems. Science 1982; 216: 1185 1192.
Lindsey HE Jr, Cohn PF: “Silent” myocardial ischemia during and after exercise testing in patients with coronary artery dis- ease. Am Heart J 1978; 95: 441-447,
Berman DS, Sale1 AF, DeNardo GL, Mason DT: Noninvasive detection of regional myocardial ischemia using rubidium-81 and the scintillation camera. Circulation 1975; 52: 619-626.
Helfant RH, Forrester JS, Hampton JR, Haft JI, Kemp HG, Gor- lin R: Coronary heart disease. Differential hemodynamic, met- abolic, and electrocardiographic effects in subjects with and without angina pectoris during atrial pacing. Circulation 1970; 42: 801-810.
Borer JS, Kent KM, Bacharach SL, et al: Sensitivity, specificity and predictive accuracy of radionuclide cineangiography dur- ing exercise in patients with coronary artery disease. Compar- ison with exercise electrocardiography. Circulation 1979; 60: 572-580.
Stern S, Tzivoni D: Early detection of silent ischaemic heart dis- ease by 24-hour electrocardiographic monitoring of active subjects. Br Heart J 1974; 36: 481-486.
Allen RD, Gettes LS, Phalan C, Avington MD: Painless ST- segment‘depression in patients with angina pectoris. Chest 1976; 69: 467-473.
Schang SJ Jr, Pepine CJ: Transient asymptomatic ST-segment depression during daily activity. Am J Cardiol 1977; 39: 396- 402.
Fox K, Selwyn A, Shillingford J: Precordial exercise mapping: improved diagnosis of coronary artery disease. Br Med J 1978; 2: 1596-1598.
Cecchi AC, Dovellini EV, Marchi F, Pucci P, Santoro GM, Faz- zini PF: Silent myocardial ischemia during ambulatory electro- cardiographic monitoring in patients with effort angina. J Am Coll Cardiol 1983; 1: 934-939.
Deanfield JE, Selwyn AP, Chierchia S, et al: Myocardial ischae- mia during daily life in patients with stable angina: its relation to symptoms and heart rate changes. Lancet 1983; II: 754- 758.
Deanfield JE, Shea M, Ribiero P, et al: Transient ST-segment depression as a marker of myocardial ischemia during daily life. Am J Cardiol 1984; 54: 1195-1200.
Kannel WB, Abbott RD: Incidence and prognosis of unrecog- nized myocardial infarction. N Engl J Med 1984; 311: 1144- 1147.
Braunwald E, Kloner RH: The stunned myocardium: prolonged, postischemic ventricular dysfunction. Circulation 1982; 66: 1146-1149.
Reimer KA, Lowe JE, Rasmussen MM, Jennings RB: The wave- front phenomenon of ischemic cell death. 1. Myocardial infarct size vs duration of coronary occlusion in dogs. Circulation 1977; 56: 786-794.
38.
39.
40.
41.
42.
43.
44.
45.
46.
47.
48.
49.
50.
51.
52.
53.
54.
55.
56.
57.
58.
prognosis in stable angina pectoris. Am J Cardiol 1984; 54: 988-993.
Ellestad MH, Wan MKC: Predictive implications of stress test- ing. Follow-up of 2700 subjects after maximum treadmill stress testing. Circulation 1975; 51: 363-369.
Theroux P, Waters DD, Halphen C, Debaisieux J-C, Mizgala HF: Prognostic value of exercise testing soon after myocardial in- farction N Engl J Med 1979; 301: 341-345.
Willerson JT, Campbell WB, Winniford MD, et al: Conversion from chronic to acute coronary artery disease: speculation regarding mechanisms. Am J Cardiol 1984; 54: 1349-1354.
Selwyn AP, Allan RM, L’Abbate A, et al: Relation between re- gional myocardial uptake of rubidium-82 and perfusion: abso- lute reduction of cation uptake in ischemia. Am J Cardiol 1982; 50: 112-121.
Hamby RI, Katz S, Hoffman I: Arteriography of coronary disease at clinical onset. Chest 1980; 78: 686-693.
Arnett EN, lsner JM, Redwood DR, et al: Coronary artery nar- rowing in coronary heart disease: comparison of cineangio- graphic and necropsy findings. Ann Intern Med 1979; 91: 350- 356.
DeRouen TA, Murray JA, Owen W: Variability in the analysis of coronary arteriograms. Circulation 1977; 55: 324-328.
White CW, Wright CB, Doty DB, et al: Does visual interpretation of the coronary arteriogram predict the physiologic impor- tance of a coronary stenosis? N Engl J Med 1984; 310: 819- 824.
Young DF, Cholvin NR, Roth AC: Pressure drop across artifi- cially induced stenoses in the femoral arteries of dogs. Circ Res 7975; 36: 735-743.
Elayda MA, Mathur VS, Hall RJ, Massumi GA, Garcia E, deCastro CM: Collateral circulation in coronary artery dis- ease. Am J Cardiol 1985; 55: 58-60.
Moise A, Theroux P, Taeymans Y, et al: Unstable angina and progression of coronary atherosclerosis. N Engl J Med 1983; 309: 685-689.
Ambrose JA, Winters SL, Stern A, et al: Angiographic morphol- ogy and the pathogenesis of unstable angina pectoris. J Am Coll Cardiol 1985; 5: 609-616.
Mandelkorn JB, Wolf NM, Singh S, et al: lntracoronary thrombus in nontransmural myocardial infarction and in unstable angina pectoris. Am J Cardiol 1983; 52: l-6.
Davies MJ, Thomas AC: Plaque fissuring-the cause of acute myocardial infarction, sudden ischaemic death, and cre- scendo angina. Br Heart J 1985; 53: 363-373.
Mehta J, Mehta P, Pepine CJ, Conti CR: Platelet function stud- ies in coronary artery disease. VII. Effect of aspirin and tachy- cardia stress on aortic and coronary venous blood. Am J Car- diol 1980; 45: 945-951.
Green LH, Seroppian E, Handin RI: Platelet activation during exercise-induced myocardial ischemia. N Engl J Med 1980; 302: 193-l 97.
Mathis PC, Wohl H, Wallach SR, Engler RL: Lack of release of platelet factor 4 during exercise-induced myocardial ische- mia. N Engl J Med 1981; 304: 1275-1278.
Sobel M, Salzman EW, Davies GC, et al: Circulating platelet products in unstable angina pectoris. Circulation 1981; 63: 300-306.
Smitherman TC, Milam M, Woo J, Willerson JT, Frenkel EP: Elevated beta thromboglobulin in peripheral venous blood of patients with acute myocardial ischemia: direct evidence for enhanced platelet reactivity in vivo. Am J Cardiol 1981; 48: 395-402.
Haerem JW: Platelet aggregates in intramyocardial vessels of patients dying suddenly and unexpectedly of coronary artery disease. Atherosclerosis 1972; 15: 199-213.
Berk BC, Brock TA, Webb RC, et al: Epidermal growth factor, a vascular smooth muscle mitogen, induces rat aortic contrac- tion. J Clin Invest 1985; 75: 1083-1086.
Vanhoutte PM, Houston DS: Platelets, endothelium, and vaso-
16 April 30, 1986 The American Journal of vedicine Volume 80 (suppl 4C)

SYMPOSIUM ON EXPLORING MYOCARDIAL ISCHEMIA-CAMPBELL ET AL
60.
61.
62.
63.
64.
65.
66.
67.
68.
69.
70.
spasm. Circulation 1985; 72: 728-734. Hirsh PD, Hillis LD, Campbell WB, Firth BG, Willerson JT: Re-
lease of prostaglandins and thromboxane into the coronary circulation in patients with ischemic heart disease. N Engl J Med 1981; 304: 685-691.
Folts JD, Crowell EB Jr, Rowe GG: Platelet aggregation in par- tially obstructed vessels and its elimination with aspirin. Circu- lation 1976; 54: 365-370.
Bush LR, Campbell WB, Buja LM, Tilton GD, Willerson JT: Ef- fects of the selective thromboxane synthetase inhibitor dazoxiben on variations in cyclic blood flow in stenosed ca- nine coronary arteries. Circulation 1984; 69: 1161-I 170.
Lewis HD, Davis JW, Archibald DG, et al: Protective effects of aspirin against acute myocardial infarction and death in men with unstable angina. N Engl J Med 1983; 309: 396-403.
Ross R, Glomset JA: The pathogenesis of atherosclerosis. N Engl J Med 1976; 295: 420-425.
Epstein SE, Palmeri ST: Mechanisms contributing to precipita- tion of unstable angina and acute myocardial infarction: impli- cations regarding therapy. Am J Cardiol 1984; 54: 1245 1252.
Meade TW: Thrombosis and ischaemic heart disease. Br Heart J 1985; 53: 473-476.
Herrick JB: Clinical features of sudden obstruction of the coro- nary arteries. JAMA 1912; 59: 2015-2020.
Ganz W, Geft I, Shah PK, et al: Intravenous streptokinase in evolving acute myocardial infarction. Am J Cardiol 1984; 53: 1209-1216.
Van de Werf F, Ludbrook PA, Bergmann SR, et al: Coronary thrombolysis with tissue-type plasminogen activator in pa- tients with evolving myocardial infarction. N Engl J Med 1984; 310: 609-613.
Lawrence JR, Shepherd JT, Bone I, Rogen AS, Fulton WFM:
71.
72. 73.
74.
75.
76.
77.
78.
79.
80.
81.
Fibrinolytic therapy in unstable angina pectoris. A controlled clinical trial. Thromb Res 1980; 17: 767-777.
Telford AM, Wilson C: Trial of heparin versus atenolol in preven- tion of myocardial infarction in intermediate coronary syn- drome. Lancet 1981; I: 1225-1228.
Feigl EO: Coronary physiology. Physiol Rev 1983; 63: 1-12. Brown BG, Bolson EL, Dodge HT: Dynamic mechanisms in
human coronary stenosis. Circulation 1984; 70: 917-922. Oliva PB, Potts DE, Pluss RG: Coronary arterial spasm in
Prinzmetal angina. Documentation by coronary arteriography. N Engl J Med 1973; 288: 745-751.
Maseri A, Mimmo R, Chierchia S: Coronary artery spasm as a cause of acute myocardial ischemia in man. Chest 1975; 68: 625-633.
Maseri A, Chierchia S: Coronary artery spasm: demonstration, definition, diagnosis, and consequences. Prog Cardiovasc Dis 1982; 25: 169-192.
Epstein SE, Cannon RO Ill, Watson RM, Leon MB, Bonow RO, Rosing DR: Dynamic coronary obstruction as a cause of an- gina pectoris: implications regarding therapy. Am J Cardiol 1985; 55: 61 B-68B.
Shepherd JT, Vanhoutte PM: Spasm of the coronary arteries: causes and consequences (the scientists viewpoint). Mayo Clin Proc 1985; 60: 33-46.
Furchgott RF: Role of endothelium in responses of vascular smooth muscle. Circ Res 1983; 53: 557-573.
Griffith TM, Edwards DH, Collins P, Lewis MJ, Henderson AH: Endothelium-derived relaxant factor. J Royal Coll Phys Lond 1985; 19: 74-79.
Ludmer PL, Selwyn AP, Wayne RR, Mudge GM, Alexander RW, Ganz P: Impaired endothelial-dependent coronary dilation in patients with coronary artery disease (abstr). J Am Coll Car- diol 1986; 7:209A.
April 30, 1986 The American Journal of Medicine Volume 80 (suppl 4C) 17