Embed Size (px)
Citation preview

ETHICAL MATTERS
Factors Associated with the Withdrawal of Life-SustainingTherapies in Patients with Severe Traumatic Brain Injury:A Multicenter Cohort Study
Nicolas Cote • Alexis F. Turgeon • Francois Lauzier • Lynne Moore •
Damon C. Scales • Francis Bernard • Ryan Zarychanski • Karen E. A. Burns •
Maureen O. Meade • David Zygun • Jean-Francois Simard • Amelie Boutin •
Jacques G. Brochu • Dean A. Fergusson
Published online: 26 October 2012
� Springer Science+Business Media New York 2012
Abstract
Purpose To identify factors associated with decisions to
withdraw life-sustaining therapies in patients with severe
traumatic brain injury (TBI).
Materials and Methods We conducted a 2-year multicenter
retrospective cohort study (2005–2006) in mechanically ven-
tilated patients aged 16 years and older admitted to the
intensive care units (ICUs) of six Canadian level I trauma
centers following severe TBI. One hundred and twenty charts
were randomly selected at each center (n = 720). Data on ICU
management strategies, patients’ clinical condition, surgical
procedures, diagnostic imaging, and decision to withdraw life-
sustaining therapies were collected. The association of factors
pertaining to the injury, interventions, and management strat-
egies with decisions to withdraw life-sustaining therapies was
evaluated among non-survivors.
Results Among the 228 non-survivors, 160 died following
withdrawal of life-sustaining therapies. Patients were pre-
dominantly male (69.7 %) with a mean age of 50.7 (±21.7)
years old. Brain herniation was more often reported in
patients who died following decisions to withdraw life-sus-
taining therapies (odds ratio [OR] 2.91, 95 % confidence
interval [CI] 1.16–7.30, p = 0.02) compared to those who
This study was performed in six level I trauma centers in Canada:
Quebec (Centre Hospitalier Affilie Universitaire de Quebec—Hopital
de l’Enfant-Jesus, Hopital du Sacre-Coeur de Montreal), Ontario
(Hamilton General Hospital, Sunnybrook Health Science Centre,
St-Michael’s Hospital); Alberta (Foothill Medical Centre).
N. Cote � A. F. Turgeon � F. Lauzier � J. G. Brochu
Division of Critical Care Medicine, Department of
Anesthesiology, Universite Laval, Quebec, QC, Canada
A. F. Turgeon (&) � F. Lauzier � L. Moore � J.-F. Simard �A. Boutin
Centre de Recherche FRQ-S du Centre Hospitalier Affilie
Universitaire de Quebec (Hopital de l’Enfant-Jesus),
Traumatologie—Urgence—Soins Intensifs (CHA-Research
Center [Enfant-Jesus Hospital], Trauma—Emergency—Critical
Care Medicine Unit), Universite Laval, 1401, 18e rue,
Local H-012a, Quebec, QC G1J 1Z4, Canada
e-mail: [email protected]
F. Lauzier
Department of Medicine, Universite Laval,
Quebec, QC, Canada
L. Moore
Department of Social and Preventive Medicine,
Universite Laval, Quebec, QC, Canada
D. C. Scales
Interdepartmental Division of Critical Care Medicine,
University of Toronto, Toronto, ON, Canada
F. Bernard
Department of Internal Medicine, Universite de Montreal,
Montreal, QC, Canada
R. Zarychanski
Department of Internal Medicine, Section of Critical Care
Medicine, University of Manitoba, Winnipeg, MB, Canada
K. E. A. Burns
Department of Critical Care Medicine, St-Michael’s Hospital,
University of Toronto, Toronto, ON, Canada
M. O. Meade
Department of Critical Care Medicine, McMaster University,
Hamilton, ON, Canada
D. Zygun
Department of Critical Care Medicine, University of Calgary,
Calgary, AB, Canada
D. A. Fergusson
Clinical Epidemiology Unit, Ottawa Hospital Research Institute,
University of Ottawa, Ottawa, ON, Canada
123
Neurocrit Care (2013) 18:154–160
DOI 10.1007/s12028-012-9787-9

died due to other causes (e.g., cardiac arrest, shock, etc.).
Epidural hematomas (OR 0.18, 95 % CI 0.06–0.56,
p < 0.01), craniotomies (OR 0.12, 95 % CI 0.02–0.68,
p = 0.02), and other non-neurosurgical procedures (OR
0.08, 95 % CI 0.02–0.43, p < 0.01) were less often asso-
ciated with death following withdrawal of life-sustaining
therapies than death from other causes.
Conclusions Death following decisions to withdraw life-
sustaining therapies is associated with specific patient and
clinical factors, and the intensity of care.
Keywords Withdrawal of life-sustaining therapy �Mortality � Traumatic brain injury � Risk factors �End-of-life
Introduction
Traumatic brain injury (TBI) is a major health and socio-
economic problem. Among individuals under 40 years of
age, TBI is the most common cause of death and disability
[1]. Despite the establishment of specialized intensive care
units (ICUs) and advances in treatment and monitoring,
TBI mortality remains high [2–5]. Previous studies have
found that 40–70 % of all deaths in ICUs follow a decision
to withdraw life-sustaining therapies [6–14]. Withdrawal of
life-sustaining therapies is, therefore, a major determinant
of death following TBI. In a previous study, we observed
significant variation in both mortality and incidence of
withdrawal of life-sustaining therapies in patients with
severe TBI among six level I trauma centers across Canada
[14].
Efforts have been made to understand factors contrib-
uting to decisions to withdraw life-sustaining therapies in
other critically ill populations [6–11, 15–21]. Several
determinants, including patient characteristics, the disease
process, therapeutic interventions, the acute care center, the
physician, and the surrogate decision-makers, have been
associated with decisions to withdraw or withhold life-
sustaining therapies in the critically ill [6–11, 15–21].
However, the overall critically ill populations studied to
date differ from the population of patients with severe TBI,
who are generally younger and without prior comorbidities
or explicit advanced care directives [12–14, 22]. To date,
little is known about the factors associated with decisions
to withdraw life-sustaining therapies in severe TBI patients
[12–14, 22]. We hypothesized that not only factors related
to the severity of injury, but also the use of certain inter-
ventions and management strategies, are associated with
decisions to withdraw life-sustaining therapies in critically
ill patients with severe TBI. The primary objective was to
identify the factors that were associated with decisions to
withdraw life-sustaining therapies among non-survivors.
Materials and Methods
We conducted a Canadian multicenter retrospective cohort
study of patients with severe TBI admitted to six level I
trauma centers in Canada (Hopital de l’Enfant-Jesus,
Hopital du Sacre-Coeur de Montreal, Hamilton General
Hospital, Sunnybrook Health Science Centre, St-Michael’s
Hospital and Foothill Medical Centre) from January 2005
to December 2006. Data on the variation in mortality and
the incidence of withdrawal of life-sustaining therapies, in
this cohort, were previously published [14]. The with-
drawal of life-sustaining therapies was defined as the
withdrawal of mechanical ventilation, of dialysis or con-
tinuous renal replacement therapy, or of vasopressors or
inotropes. We included mechanically ventilated patients,
aged 16 years and older who were admitted to an ICU
following a severe blunt TBI, defined as a Glasgow Coma
Scale (GCS) score B8, documented in the emergency room
or at ICU admission. Research Ethics Board approval was
obtained at each study site.
Patient Identification and Case Report Form
Development
Patients were identified using the International Classifica-
tion of Diseases 10 Codes for TBI (S06.0–S06.9). A
standardized case report form was developed by a group of
critical care physicians, clinical researchers, and research
nurses with experience in chart review and data abstraction.
The case report form was pre-tested in two of the partici-
pating institutions prior to the study initiation. A detailed
operations manual helped to unify the approach to data
collection across sites. Data were retrieved from the med-
ical record by trained abstractors having received a half-
day formation on the use of the case report form.
Data Collection
We collected the following baseline characteristics: age,
gender, injury severity score, cause of trauma, associated
traumatic injuries (c-spine, abdomen/pelvic content, chest,
bones other than c-spine), and referral. We also collected
daily data on vital signs, neurological exam findings, use of
jugular venous saturation monitoring or intracranial pressure
monitoring, and other laboratory tests from the time of
arrival in the emergency room until day 14 while in the ICU.
Data were also collected daily on management, including the
use of induced hypothermia, osmotic agents (mannitol,
hypertonic saline), vasopressors, sedation, paralytic agents,
seizure prophylaxis, intravenous insulin infusion, and deep
venous thrombosis prophylaxis. CT scan data were collected
on admission according to the official radiological reports.
Subsequent improvement or worsening CT scan was
Neurocrit Care (2013) 18:154–160 155
123

recorded. Data on surgical procedures were collected up to
28 days. Decisions to withdraw life-sustaining therapies
were collected.
Sample Size
The study sample size of 720 patients was originally
determined to estimate mortality rates and the proportion of
deaths related to decisions to withdraw life-sustaining
therapies with a precision of 10 % [14]. In order to avoid
season and calendar year variability, 60 patients per year
per center (n = 120 per center) were randomly selected
from all eligible patients.
Statistical Analysis
In order to evaluate the impact of various factors with the
decision to withdraw life-sustaining therapies in patients at
risk of in-hospital death, we restricted our study to the
cohort of non-survivors within the entire cohort of patients.
We thus compared patients who died following withdrawal
of life-sustaining therapies to patients who died due to
other causes (not following a decision to withdraw life-
sustaining therapies). This approach allowed identifying
patients with the highest risk of death and how deaths
following a decision to withdraw life-sustaining therapies
are different to other deaths when considering the severity
of the injury, interventions provided, and management.
We built a multivariable logistic regression model that
included gender and three baseline factors (age, GCS motor
score, and pupillary reflex at ICU admission) known to be
associated with prognosis in patients with severe TBI [23–
25]. Fractional polynomials and multiple different cate-
gorical divisions strategies were used to transform age and
GCS motor score variables in categorical variables. Age
was dichotomized as lower or equal to 55 years or greater
than 55 years old. Categories of GCS motor score were 1,
2–3, and 4–5–6. Pupil reflex was dichotomized as present
(bilateral or unilateral) or absent.
First, factors related to the injury were added to this
baseline model. Due to the large number of potential
explanatory variables, we used a manual backward elimi-
nation technique to select variables with p < 0.2 [26]. In a
second step, variables related to interventions and man-
agement strategies (e.g., craniotomy) were also added to
the model and selected applying the same backward
elimination technique. The four baseline variables were
never considered for elimination.
Variables associated with a p < 0.05 were considered
to be statistically significant factors related to decisions to
withdraw life-sustaining therapies. Multivariate analyses
were adjusted for clustering by trauma center using a
random intercept. Data are presented as mean ± standard
deviation (SD) for continuous variables, as median with
interquartile range (IQR) for ordinal variables and as odds
ratios (ORs) with 95 % confidence interval (CI) for the
regression analysis. Associations between categorical
variables were evaluated using Pearson v2 test. Statistical
analysis was performed using SAS version 9.2 (SAS
Institute, Cary, North Carolina).
Results
Mortality in the entire study cohort was 31.7 % (228/720)
and more than two-thirds (n = 160) of deaths were asso-
ciated with a decision to withdraw life-sustaining therapies
(Table 1). No patient for whom decisions to withdraw life-
sustaining therapies was taken survived. Among non-sur-
vivors (n = 228), 225 patients were considered in the final
multivariate analysis, following removal of 3 patients with
missing data for motor GCS score. Among variables of
baseline characteristics, only the cause of trauma was
missing for four patients (1.8 %) in the withdrawal of life-
sustaining therapies group. The mean age of patients
included in the analysis was 50.7 (±21.7) years. Patients
were predominantly male (69.7 %) and most trauma
involved a motor vehicle collision (57.3 %). Median GCS
was 3 (IQR: 3–4). Timing of death was comparable in both
patients who died following a decision to withdraw life-
sustaining therapies (median 3.0 days; IQR: 1.0–7.0) and
patients who died due to other causes (median: 2.0 days;
IQR: 1.0–6.0).
Factors Associated with Withdrawal of Life-Sustaining
Therapy
Injury Related Factors
In multivariate analyses, only two variables related to the
injury were significantly associated with decisions to
withdraw life-sustaining therapies: herniation on the initial
CT scan was associated with increased odds of decisions to
withdraw life-sustaining therapies (OR 2.91, 95 % CI
1.16–7.30, p = 0.02), whereas the presence of an epidural
hematoma on the initial CT scan was associated with a
reduction in the odds of withdrawal of life-sustaining
therapies in non-surviving patients (OR 0.18, 95 % CI
0.06–0.56, p < 0.01) (Table 2).
Interventions and Management Related Factors
In multivariate analyses (Table 2), only craniotomy (OR
0.12, 95 % CI 0.02–0.68, p = 0.02) and other surgical
procedures, excluding tracheotomy or a percutaneous
endoscopic gastrostomy tube insertion (ex. laparotomy,
156 Neurocrit Care (2013) 18:154–160
123
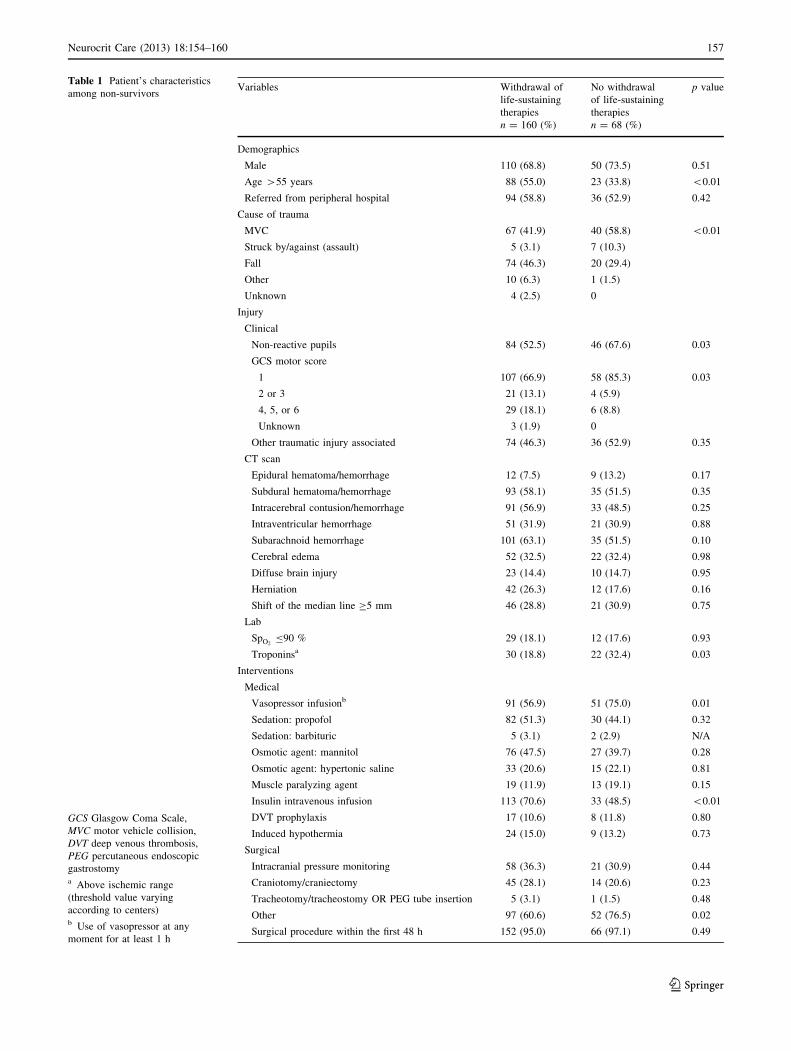
Table 1 Patient’s characteristics
among non-survivors
GCS Glasgow Coma Scale,
MVC motor vehicle collision,
DVT deep venous thrombosis,
PEG percutaneous endoscopic
gastrostomya Above ischemic range
(threshold value varying
according to centers)b Use of vasopressor at any
moment for at least 1 h
Variables Withdrawal of
life-sustaining
therapies
No withdrawal
of life-sustaining
therapies
p value
n = 160 (%) n = 68 (%)
Demographics
Male 110 (68.8) 50 (73.5) 0.51
Age >55 years 88 (55.0) 23 (33.8) <0.01
Referred from peripheral hospital 94 (58.8) 36 (52.9) 0.42
Cause of trauma
MVC 67 (41.9) 40 (58.8) <0.01
Struck by/against (assault) 5 (3.1) 7 (10.3)
Fall 74 (46.3) 20 (29.4)
Other 10 (6.3) 1 (1.5)
Unknown 4 (2.5) 0
Injury
Clinical
Non-reactive pupils 84 (52.5) 46 (67.6) 0.03
GCS motor score
1 107 (66.9) 58 (85.3) 0.03
2 or 3 21 (13.1) 4 (5.9)
4, 5, or 6 29 (18.1) 6 (8.8)
Unknown 3 (1.9) 0
Other traumatic injury associated 74 (46.3) 36 (52.9) 0.35
CT scan
Epidural hematoma/hemorrhage 12 (7.5) 9 (13.2) 0.17
Subdural hematoma/hemorrhage 93 (58.1) 35 (51.5) 0.35
Intracerebral contusion/hemorrhage 91 (56.9) 33 (48.5) 0.25
Intraventricular hemorrhage 51 (31.9) 21 (30.9) 0.88
Subarachnoid hemorrhage 101 (63.1) 35 (51.5) 0.10
Cerebral edema 52 (32.5) 22 (32.4) 0.98
Diffuse brain injury 23 (14.4) 10 (14.7) 0.95
Herniation 42 (26.3) 12 (17.6) 0.16
Shift of the median line C5 mm 46 (28.8) 21 (30.9) 0.75
Lab
SpO2B90 % 29 (18.1) 12 (17.6) 0.93
Troponinsa 30 (18.8) 22 (32.4) 0.03
Interventions
Medical
Vasopressor infusionb 91 (56.9) 51 (75.0) 0.01
Sedation: propofol 82 (51.3) 30 (44.1) 0.32
Sedation: barbituric 5 (3.1) 2 (2.9) N/A
Osmotic agent: mannitol 76 (47.5) 27 (39.7) 0.28
Osmotic agent: hypertonic saline 33 (20.6) 15 (22.1) 0.81
Muscle paralyzing agent 19 (11.9) 13 (19.1) 0.15
Insulin intravenous infusion 113 (70.6) 33 (48.5) <0.01
DVT prophylaxis 17 (10.6) 8 (11.8) 0.80
Induced hypothermia 24 (15.0) 9 (13.2) 0.73
Surgical
Intracranial pressure monitoring 58 (36.3) 21 (30.9) 0.44
Craniotomy/craniectomy 45 (28.1) 14 (20.6) 0.23
Tracheotomy/tracheostomy OR PEG tube insertion 5 (3.1) 1 (1.5) 0.48
Other 97 (60.6) 52 (76.5) 0.02
Surgical procedure within the first 48 h 152 (95.0) 66 (97.1) 0.49
Neurocrit Care (2013) 18:154–160 157
123
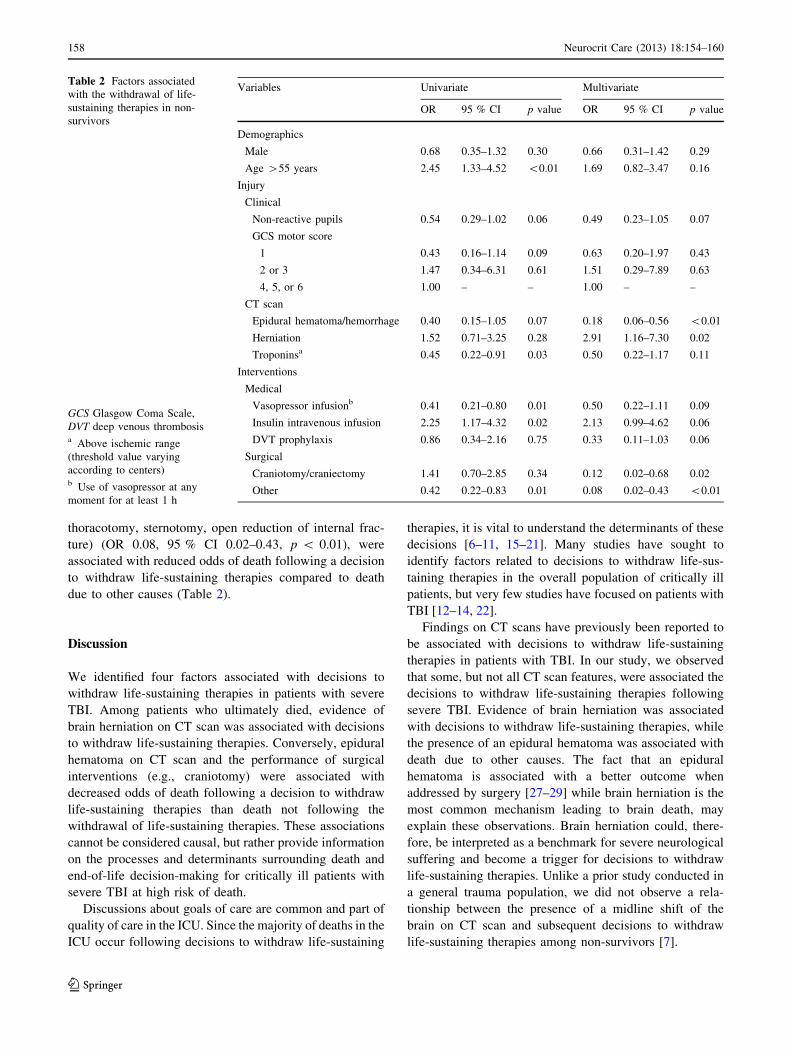
thoracotomy, sternotomy, open reduction of internal frac-
ture) (OR 0.08, 95 % CI 0.02–0.43, p < 0.01), were
associated with reduced odds of death following a decision
to withdraw life-sustaining therapies compared to death
due to other causes (Table 2).
Discussion
We identified four factors associated with decisions to
withdraw life-sustaining therapies in patients with severe
TBI. Among patients who ultimately died, evidence of
brain herniation on CT scan was associated with decisions
to withdraw life-sustaining therapies. Conversely, epidural
hematoma on CT scan and the performance of surgical
interventions (e.g., craniotomy) were associated with
decreased odds of death following a decision to withdraw
life-sustaining therapies than death not following the
withdrawal of life-sustaining therapies. These associations
cannot be considered causal, but rather provide information
on the processes and determinants surrounding death and
end-of-life decision-making for critically ill patients with
severe TBI at high risk of death.
Discussions about goals of care are common and part of
quality of care in the ICU. Since the majority of deaths in the
ICU occur following decisions to withdraw life-sustaining
therapies, it is vital to understand the determinants of these
decisions [6–11, 15–21]. Many studies have sought to
identify factors related to decisions to withdraw life-sus-
taining therapies in the overall population of critically ill
patients, but very few studies have focused on patients with
TBI [12–14, 22].
Findings on CT scans have previously been reported to
be associated with decisions to withdraw life-sustaining
therapies in patients with TBI. In our study, we observed
that some, but not all CT scan features, were associated the
decisions to withdraw life-sustaining therapies following
severe TBI. Evidence of brain herniation was associated
with decisions to withdraw life-sustaining therapies, while
the presence of an epidural hematoma was associated with
death due to other causes. The fact that an epidural
hematoma is associated with a better outcome when
addressed by surgery [27–29] while brain herniation is the
most common mechanism leading to brain death, may
explain these observations. Brain herniation could, there-
fore, be interpreted as a benchmark for severe neurological
suffering and become a trigger for decisions to withdraw
life-sustaining therapies. Unlike a prior study conducted in
a general trauma population, we did not observe a rela-
tionship between the presence of a midline shift of the
brain on CT scan and subsequent decisions to withdraw
life-sustaining therapies among non-survivors [7].
Table 2 Factors associated
with the withdrawal of life-
sustaining therapies in non-
survivors
GCS Glasgow Coma Scale,
DVT deep venous thrombosisa Above ischemic range
(threshold value varying
according to centers)b Use of vasopressor at any
moment for at least 1 h
Variables Univariate Multivariate
OR 95 % CI p value OR 95 % CI p value
Demographics
Male 0.68 0.35–1.32 0.30 0.66 0.31–1.42 0.29
Age >55 years 2.45 1.33–4.52 <0.01 1.69 0.82–3.47 0.16
Injury
Clinical
Non-reactive pupils 0.54 0.29–1.02 0.06 0.49 0.23–1.05 0.07
GCS motor score
1 0.43 0.16–1.14 0.09 0.63 0.20–1.97 0.43
2 or 3 1.47 0.34–6.31 0.61 1.51 0.29–7.89 0.63
4, 5, or 6 1.00 – – 1.00 – –
CT scan
Epidural hematoma/hemorrhage 0.40 0.15–1.05 0.07 0.18 0.06–0.56 <0.01
Herniation 1.52 0.71–3.25 0.28 2.91 1.16–7.30 0.02
Troponinsa 0.45 0.22–0.91 0.03 0.50 0.22–1.17 0.11
Interventions
Medical
Vasopressor infusionb 0.41 0.21–0.80 0.01 0.50 0.22–1.11 0.09
Insulin intravenous infusion 2.25 1.17–4.32 0.02 2.13 0.99–4.62 0.06
DVT prophylaxis 0.86 0.34–2.16 0.75 0.33 0.11–1.03 0.06
Surgical
Craniotomy/craniectomy 1.41 0.70–2.85 0.34 0.12 0.02–0.68 0.02
Other 0.42 0.22–0.83 0.01 0.08 0.02–0.43 <0.01
158 Neurocrit Care (2013) 18:154–160
123

Age and GCS are prognostic factors in patients with
severe TBI that have been shown to be associated with
decisions to withdraw life-sustaining therapies in general
ICU and trauma populations [7, 11, 17, 18, 21]. However,
we found no evidence that these factors were associated
with decisions to withdraw life-sustaining therapies in TBI
populations. No medical interventions were significantly
associated with decisions to withdraw life-sustaining ther-
apies. This is not surprising since it might be expected that
patients will be treated according to guidelines until a
decision to withdraw life-sustaining therapies is taken. On
the other hand, surprisingly few patients who died in our
cohort actually had an intracranial pressure monitor inser-
ted (34.6 %).
Strengths and Limitations
Our study has several strengths. First, it involved highly
standardized data abstraction across centers using trained
data abstractors and an operation manual to minimize
measurement bias. Second, our analyses were adjusted for
the most important known factors associated with prog-
nosis in severe TBI patients (age, GCS motor score, and
pupillary reflex) [23–25], thereby controlling for potential
variation in the risk of death due to the severity of brain
injury. Third, we restricted our cohort to non-survivors,
also reducing the potential for confounding by disease
severity.
Our study also has limitations. Due to the retrospective
design of our study, the observed data were limited to the
information detailed in the patients’ charts, including the
decision to withdraw life-sustaining therapies. Poor docu-
mentation may have resulted in underestimation of the
incidence of withdrawal of life-sustaining therapies [30].
However, considering the medico-legal importance of this
information, it is unlikely that it would be missing in a
significant number of charts. In addition, we used available
information from CT scan reports, and thus did not have
information on scoring system (i.e., Marshall score), which
could have been a good way to categorize the severity of
the brain injury on CT scan. Second, since our model was
based on non-survivors, it does not represent the entire
population of severe TBI patients at risk of withdrawal of
life-sustaining therapies who survived. This may also
explain some of the divergences of our results with those of
previous studies [16, 17]. Third, our study was not
designed to understand whether deaths following the
withdrawal of life-sustaining therapies happened following
a thoughtful process or not, but to aim understanding what
factors were associated with these decisions to withdraw
life-sustaining therapies, notwithstanding if it was due to a
self-fulfilling prophecy or not [31]. Finally, our study
aimed to identify factors related to death following
decisions to withdraw life-sustaining therapies, but was not
designed to evaluate all factors potentially related to the
determinants of decisions to withdraw life-sustaining
therapies in critically ill patients with severe TBI, for
example estimations of patients’ preferences and values.
Although we agree that reasons and processes leading to a
decision to withdraw life-sustaining therapies are complex,
variable, and likely multifactorial [7, 8, 18, 32], we focused
on specific factors related to the injury and therapeutic
interventions.
Conclusion
Evidence of epidural hematoma or brain herniation on CT
scan and specific surgical interventions were associated
with decisions to withdraw life-sustaining therapies among
non-survivors of severe TBI. Considering the high rate of
decisions to withdraw life-sustaining therapies among
patients with severe TBI, further research is required to
understand the processes and determinants associated with
decisions to withdraw life-sustaining therapies in this
population.
Acknowledgments The authors would like to thank Tran Cong
Dung MD, MSc; Mohana Ratnapalan HBSc, Stephanie Todd BSc,
MBT, John Harlock MD, Frederic Morin RN and David Simonyan
MD MSc, for their help in data acquisition; Valerie Murat MSc for
her participation in the data cleaning process; Mrs. Valerie Boucher
for her secretarial assistance. This work was presented in part at the
Intensive Care and Emergency Medicine Symposium (Brussels,
Belgium, March 2011). The work was supported in part by the
Fondation de l’Hopital de l’Enfant-Jesus (Enfant-Jesus Hospital
Foundation) who had no role in any part of conduct of the study or
preparation of the manuscript. Drs. Turgeon and Lauzier are recipi-
ents of a Research Career Award from the Fonds de RechercheQuebec-Sante (FRQ-S). Drs. Moore, Scales, and Fergusson are
recipients of New Investigator Awards from the Canadian Institutesfor Health Research (CIHR). Dr. Zarychanski is a recipient of a CIHR
RCT Mentorship Award. Dr. Burns holds a Clinician Scientist Phase
2 Award from the CIHR.
References
1. National Scientific Advisory Committee. Identifying priorities for
research and capacity development in injury as a multi-institute
strategic initiative within the Canadian Institutes of Health
Research. In: Listening for direction on injury: final report
Instituts canadiens de recherche en sante; 2004.
2. Coronado VG, Xu L, Basavaraju SV, et al. Surveillance for
traumatic brain injury-related deaths—United States, 1997–2007.
MMWR Surveill Summ. 2011;60:1–32.
3. Masson F, Thicoipe M, Aye P, et al. Epidemiology of severe
brain injuries: a prospective population-based study. J Trauma.
2001;51:481–9.
4. Murray GD, Teasdale GM, Braakman R, et al. The European
Brain Injury Consortium survey of head injuries. Acta Neurochir
(Wien). 1999;141:223–36.
Neurocrit Care (2013) 18:154–160 159
123

5. Myburgh JA, Cooper DJ, Finfer SR, et al. Epidemiology and
12-month outcomes from traumatic brain injury in Australia and
New Zealand. J Trauma. 2008;64:854–62.
6. Spronk PE, Kuiper AV, Rommes JH, Korevaar JC, Schultz MJ.
The practice of and documentation on withholding and with-
drawing life support: a retrospective study in two Dutch intensive
care units. Anesth Analg. 2009;109:841–6.
7. Cooper Z, Rivara FP, Wang J, MacKenzie EJ, Jurkovich GJ.
Withdrawal of life-sustaining therapy in injured patients: varia-
tions between trauma centers and nontrauma centers. J Trauma.
2009;66:1327–35.
8. Azoulay E, Metnitz B, Sprung CL, et al. End-of-life practices in
282 intensive care units: data from the SAPS 3 database. Inten-
sive Care Med. 2009;35:623–30.
9. Zahuranec DB, Morgenstern LB, Sanchez BN, Resnicow K, White
DB, Hemphill JC III. Do-not-resuscitate orders and predictive
models after intracerebral hemorrhage. Neurology. 2010;75:
626–33.
10. Rocker G, Cook D, Sjokvist P, et al. Clinician predictions of
intensive care unit mortality. Crit Care Med. 2004;32:1149–54.
11. Becker KJ, Baxter AB, Cohen WA, et al. Withdrawal of support
in intracerebral hemorrhage may lead to self-fulfilling prophecies.
Neurology. 2001;56:766–72.
12. Rocker GM, Cook DJ, Shemie SD. Brief review: practice vari-
ation in end of life care in the ICU: implications for patients with
severe brain injury. Can J Anaesth. 2006;53:814–9.
13. O’Callahan JG, Fink C, Pitts LH, Luce JM. Withholding and
withdrawing of life support from patients with severe head injury.
Crit Care Med. 1995;23:1567–75.
14. Turgeon AF, Lauzier F, Simard JF, et al. Mortality associated
with withdrawal of life-sustaining therapy for patients with severe
traumatic brain injury: a Canadian multicentre cohort study.
CMAJ. 2011;183:1581–8.
15. Varelas PN, Abdelhak T, Hacein-Bey L. Withdrawal of life-
sustaining therapies and brain death in the intensive care unit.
Semin Neurol. 2008;28:726–35.
16. Cook D, Rocker G, Marshall J, et al. Withdrawal of mechanical
ventilation in anticipation of death in the intensive care unit.
N Engl J Med. 2003;349:1123–32.
17. Esteban A, Gordo F, Solsona JF, et al. Withdrawing and with-
holding life support in the intensive care unit: a Spanish
prospective multi-centre observational study. Intensive Care Med.
2001;27:1744–9.
18. Diringer MN, Edwards DF, Aiyagari V, Hollingsworth H. Factors
associated with withdrawal of mechanical ventilation in a neu-
rology/neurosurgery intensive care unit. Crit Care Med. 2001;29:
1792–7.
19. Ferrand E, Robert R, Ingrand P, Lemaire F. Withholding and
withdrawal of life support in intensive-care units in France: a
prospective survey. French LATAREA Group. Lancet. 2001;357:
9–14.
20. Mayer SA, Kossoff SB. Withdrawal of life support in the neu-
rological intensive care unit. Neurology. 1999;52:1602–9.
21. Keenan SP, Busche KD, Chen LM, McCarthy L, Inman KJ,
Sibbald WJ. A retrospective review of a large cohort of patients
undergoing the process of withholding or withdrawal of life
support. Crit Care Med. 1997;25:1324–31.
22. Thompson HJ, Rivara FP, Jurkovich GJ, Wang J, Nathens AB,
MacKenzie EJ. Evaluation of the effect of intensity of care on
mortality after traumatic brain injury. Crit Care Med. 2008;36:
282–90.
23. Perel P, Arango M, Clayton T, et al. Predicting outcome after
traumatic brain injury: practical prognostic models based on large
cohort of international patients. BMJ. 2008;336:425–9.
24. Murray GD, Butcher I, McHugh GS, et al. Multivariable prog-
nostic analysis in traumatic brain injury: results from the
IMPACT study. J Neurotrauma. 2007;24:329–37.
25. Steyerberg EW, Mushkudiani N, Perel P, et al. Predicting out-
come after traumatic brain injury: development and international
validation of prognostic scores based on admission characteris-
tics. PLoS Med. 2008;5:e165. discussion e165;1251–61.
26. Harrell FE Jr, Lee KL, Califf RM, Pryor DB, Rosati RA.
Regression modelling strategies for improved prognostic pre-
diction. Stat Med. 1984;3:143–52.
27. Brain Trauma Foundation. Guidelines for the Surgical Manage-
ment of Traumatic Brain Injury. Neurosurgery. 2006;58:S2-1–3.
28. Brain Trauma Foundation. Early indicators of prognosis in severe
traumatic brain injury. In: Management and prognosis of severe
traumatic brain injury. American Association of Neurological
Surgeons; 2000.
29. Brain Trauma Foundation. Guidelines for the Management of
Severe Traumatic Brain Injury. 3rd ed. New York: Brain Trauma
Foundation; 2007.
30. Ratnapalan M, Cooper AB, Scales DC, Pinto R. Documentation
of best interest by intensivists: a retrospective study in an Ontario
Critical Care Unit. BMC Med Ethics. 2010;11:1–7.
31. Wilkinson D. The self-fulfilling prophecy in intensive care. Theor
Med Bioeth. 2009;30:401–10.
32. Ho KM, Liang J. Withholding and withdrawal of therapy in New
Zealand intensive care units (ICUs): a survey of clinical directors.
Anaesth Intensive Care. 2004;32:781–6.
160 Neurocrit Care (2013) 18:154–160
123





























