Embed Size (px)
Citation preview

Resident: Date:
SCOTT FALL RISK SCREENING TOOL for Residential Care©
Reason for completing tool (circle one): 1. New admission; 2. Change of status; 3. Yearly review; 4. Serious fall injury/multiple falls. [TO BE COMPLETED BY RN, LPN or PT/OT]
RISK FACTOR PRESENT CIRCLE POSSIBLE STRATEGIES More than 2 falls in previous 6 months 6 Review circumstances of prior falls from fall reports.
Impaired mobility, balance or gait 2 Refer for PT/OT assessment / provide hip protectors.
Altered mental state (e.g., delirium, brain injury, dementia, depression)
2 Monitor daily for change in mental status and ability to remember and follow instructions.
Attempts to unsafely get out of bed due to lack of understanding, agitation or restlessness
2 If confused with impaired mobility, assess for bed alarm / mats / monitoring.
Move to facility in past month 1 Screen for fall risk / assess for mobility.
Dizziness or vertigo 1 Check for orthostatic hypotension, dehydration and vestibular problems. Refer for medical assessment.
Generalized weakness (see back page for indicators)
1 Assess for insomnia, pain, malnutrition, hypoxia or disuse. Refer for medical assessment.
Alternations in urinary and bowel elimination (frequency, urgency, incontinence, etc.)
1 Bladder/bowel routine / bedside commode or light if unsafe at night.
Greater than 7 medications, especially narcotics, anti-depressants, anti-psychotics, diuretics
1 Regular review of medications.
Any prescribed benzodiazepine or psychotropic medications
1 Refer to pharmacist/ physician for reduced dose or alternatives to benzodiazepine or psychotropic meds.
Immobile (unable to walk or stand unaided) -5 Precautions for falling from bed or chair. Plan for fracture risk related to osteoporosis.
TOTAL Risk Assessment Total Score *see reverse for further guidelines for item completion * Score <7 – universal precautions for falls. Score > 7 – deemed to be at high risk for falls. Score >12 – deemed to be at high risk for falls and unsafe ambulation. IF resident score <7:
IF resident score >7:
Follow universal fall prevention plan, including: bed in low position call bell in place good fitting footwear incontinence precautions environment uncluttered, good lighting, accessible
grab bars, non-slip floors apply strategies based on risk items above
In addition to universal fall prevention plan, develop tailored falls prevention plan based on risk items above and put in chart, including: bedside safety plan put in prominent location in room include high risk status in shift report & chart least restraint precautions hip protectors, bed / chair alarm, as needed notify family of fall risk through letter / brochure
IF unsafe ambulation with score >12: In addition to above, assess for appropriate wheelchair use / least restraints / hip protectors / personal alarm systems Notify family through letter and/or brochure regarding unsafe ambulation and fall risk Comments: Signature Date
Facility: __________________________________________________________________
SCOTT FALL RISK SCREENING TOOL: RESIDENTIAL CARE. August 25, 2009, V. Scott, Senior Advisor Fall & Injury Prevention, B.C. Injury Research & Prevention Unit. Not to be used without permission of the author at: [email protected]
1

2
GUIDELINES FOR COMPLETION OF FALL RISK ASSESSMENT PREVENTION PLAN: Develop a plan that reflects the individual’s risk factors, i.e., if dizziness and vertigo are circled above, implement the suggested strategies. Keep an updated summary of the fall prevention care plan in the resident’s room where it can be easily seen by care aids, nurses and others who provide care. PRIOR FALLS: Prior falls are the greatest predictor of future falls. Design a tailored prevention plan related to individual’s risk as indicated in reports of prior falls, e.g., falls related to balance, pain, health status, activity, footwear, environment, etc. It is recommended that a Fall Report1 be completed for each fall to assist with understanding the contributing factors that can be targeted for prevention. Refer for medical assessment of underlying medical contributors and physio/OT for mobility and assistive device use. DIZZINESS OR VERTIGO: Unsteady on feet, particularly when rising from a lying or sitting position – refer for medical assessment of underlying cause. RN to assess for orthostatic hypotension by taking a lying blood pressure (BP) followed by a sitting BP and then a standing BP. ALTERED MENTAL STATUS: Unable to follow instructions, impaired short-term memory, impaired thought processes (psychosis) or conditions which increase agitation and aggression – refer for assessment and treatment. ATTEMPTS TO UNSAFELY GET OUT OF BED: Poor judgment and safety awareness. Attempts to get out of bed could related to dementia, poor pain control, language barrier, need to toilet, alcohol, or cognitive deficits – refer for assessment and treatment of medical contributors; assess and address other issues. IMPAIRED MOBILITY: Impaired gait (shuffling, small steps, slow pace, hangs onto walls or furniture) and/or impaired balance / unsteadiness while standing – refer to OT/PT for assessment and intervention. Ensure environment is safe for ambulation – good lighting, non-slippery, walking aides in reach with brakes on, appropriate footwear (non-slip, good fit), and no objects to trip over. GENERALIZED WEAKNESS: Resident verbalizes that they feel weak. Assess and address if: unable to stand unassisted by side of bed for 2 to 3 minutes or unable to do 2 or more of the following:
• get off and on toilet independently • sit to stand and back to sit without assistance • able to dress and groom independently • walk across room ( 20 feet ), turn and walk back without assistance ( may use mobility aide ) • transfer / move in bed
ALTERATIONS IN URINARY & BOWEL ELIMINATION: Frequency, urgency, nocturia, occasional or regular incontinence, constipation - especially important at nights / assess medications which can alter elimination patterns. Ensure a safe environment between bed, chair and bathroom, i.e., good lighting, non-slip flooring, accessible grab bars and call bells. Document elimination patterns in order to anticipate need for assistance. MORE THAN 7 MEDICATIONS or TAKING BENZODIAZEPINES or PSYCHOTROPICS: Include such meds as narcotics, sedatives, anti-depressives, anti-psychotics, anti-hypertensives, diuretics. Do not include such items as vitamins, herbal pills, eye ointments, skin creams etc. Benzodiazepine and psychotropic mediations are highly associated with fall and injury risk, i.e., taking Valium, Ativan, Serax, Paxil, Elavil, Zoloft, Loxapine, etc. Refer for medication review on routine basis. IMMOBILE: 1) Patient who is unable to initiate movement and thus would not get up & fall out of bed. 2) Patients who are unable to walk or weight bear but may use a wheelchair for mobility and are not able to transfer themselves. A negative score of 5 is assigned to prevent automatic assignment of high risk. Monitor for fracture risk due to osteoporosis. NOTE: if a patient is immobile, do not score patient as “impaired mobility “. FRACTURE RISK: If resident has had a fracture in the prior five years they are at increased risk for future fractures. Offer hip protectors to reduce the risk of fall-related hip fractures. Consider bedside mats where appropriate. Refer for assessment of osteoporosis.
1 The Fall Report developed by Scott, et al. is available to licensed LTC facilities. For information on how to obtain copies contact Dr. Vicky Scott at [email protected]

Morse Fall Scale
Fall Risk is based upon Fall Risk Factors and it is more than a Total Score. Determine Fall Risk Factors and Target Interventions to Reduce Risks. Complete on admission, at change of condition, transfer to a new unit, and after a fall.
Variables Score Admission Date
Review Date
Review Date
History of Falling
No Yes
0 25
Secondary Diagnosis
No Yes
0 15
None/bedrest/nurse assist
0
Crutches/cane/walker
15
Ambulatory Aid
Furniture
30
IV or IV access
No Yes
0 20
Normal/bedrest/wheelchair
0
Weak
10
Gait
Impaired
20
Mental Status
Knows own limits 0
Overestimates or forgets limits
15
Total
Signature & Status
To obtain the Morse Fall Score add the score from each category.
Morse Fall Score High Risk 45 and higher Moderate Risk 25-44 Low Risk 0-24 Note: Complete checklist for resident assessed based on level of risk.

TUG Guidelines Last Update: May 26, 2008
Timed Up and Go (TUG) Practice Guidelines for Assisted Living Residences
TUG test is a screen for general mobility (strength and balance). This test provides a measure of the functional ability of Assisted Living residents and should be conducted for all new residents and repeated at times of change in health status or after a fall, as well as on annual reassessment. This form can be used for both initial assessment and re-assessment. Equipment:
Arm chair Tape measure
Small cone Stop watch
For consistency across repeated tests it is important to use similar equipment, therefore, please note the type of chair used and any features of the chair that need to be considered in future tests, e.g., client’s favorite blue arm chair in the living room. This test can also be conducted in a corridor or other common area with a standard chair used for all residents. Pre-test:
1. Have the resident sitting in a chair with arm rests with their back against the back of the chair (chair preferably as close to a 46 cm seat height and 64 cm arm rest height as possible). The chair should be stable and positioned such that it will not move when the subject gets up.
2. Place a cone on the floor 3 meters away from the front of the chair so that it is easily seen by the resident but does not create a trip hazard.
Instructions to the Resident:
“On the word GO, stand up and walk at your normal and comfortable pace to the marker on the floor, then turn around and walk back to the chair and sit down”
Guidelines for Clinicians:
1. Demonstrate walking around the cone, without going too far beyond the cone,, turning, and walking back.
2. Start timing on the word “GO” and stop timing when the subject is seated again correctly in the chair with their back resting on the back of the chair.
3. The subject wears their regular footwear and may use any gait aid that they normally use during ambulation.
4. There is no time limit. They may stop and rest (but not sit down) if they need to. 5. If the subject is unable to perform the test or unable to perform without being assisted by
another person, then do not perform the test and mark the test as “unable to perform”. 6. The subject is allowed a practice trial that is not timed before testing. (The need for the
practice trial to be determined by the test administrator).
Time Score Guidelines:
♦ Most Assisted Living residents take longer than 15 seconds to complete the task.1 A score of 15 seconds or more indicates a higher risk for falling.2
1 The Promoting Active Living (PAL) Project Findings. BC Injury Research and Prevention Unit. 2 Whiney JC, Lord SR, Close JCT (2005). “Streamlining assessment and intervention in a falls clinic using the Timed Up and Go Test and Physiological Profile Assessments”. Age and Ageing; 34:567-571

TUG Guidelines Last Update: May 26, 2008
Timed Up and Go (TUG) Test
Resident Name: ________________________________ Room #: ___________________ Date of Initial Test: (dd-mm-yy)
Date of Re-assessment: (dd-mm-yy)
Time of Day Test Conducted: (24hr)
Time of Day Test Conducted: (24hr)
Unable to perform TUG Describe reason: ___________________
Unable to perform TUG Describe reason: ___________________
Arm chair used Describe: _________________________
Arm chair used Describe: _________________________
Mobility aide used: No mobility aide used Cane Two canes 2 crutches Solid Walker – no wheels Walker – 2 wheels Walker – 4 wheels Other: ___________________________
Mobility aide used: No mobility aide used Cane Two canes 2 crutches Solid Walker – no wheels Walker – 2 wheels Walker – 4 wheels Other: ___________________________
Observation of Gait & Stability: Guidelines for the clinician: Observe how client stands up, with/without using arms; observe stability on turning and any assistance required; observe postural stability, gait pattern and sway; hearing, vision & cognition Getting up from Sitting: Attempted to get up a few times Using both arms � Using no/one arm Other Walking: Steady � Unsteady Limping � Stiff knees Other � Dragging the leg Turning: Steady � Unsteady Difficulty moving the walker Other Sitting down: Using both arms � Using no/one arm Near miss of chair Other
Getting up from Sitting: Attempted to get up a few times Using both arms � Using no/one arm Other Walking: Steady � Unsteady Limping � Stiff knees Other � Dragging the leg Turning: Steady � Unsteady Difficulty moving the walker Other Sitting down: Using both arms � Using no/one arm Near miss of chair Other
TUG Score in Seconds:
TUG Score in Seconds:
Examiner Signature: Examiner Signature:

Sit To Stand Test (Muscular Strength)
In this test, the time taken to complete a single sit to stand, as well as the time taken to complete five consecutive sit to stands, are recorded. Instruction for Administration of the Sit to Stand Test: The participant is asked to sit in a standard straight-backed chair (seat height 46 cm & arm height approximately 65 cm) with his/her back against the back of the chair. The chair should be placed against a wall to prevent slipping/sliding. If a standard chair is not available, use a kitchen chair with arms if possible. Once seated in a comfortable position, he/she is asked to stand up as quickly as possible to a fully erect position and sit back in the chair. No other instructions are given regarding hand position. This is helpful to establish the initial or spontaneous category of hand assistance. Time taken to complete one sit to stand is recorded to the nearest second. The person is then asked to stand up and sit down 5 times with as little hand assistance as possible. Record: Time in seconds required to complete one sit to stand and five consecutive sit to stands; one practice sit to stand is allowed before being timed; note the extent of hand assistance required to complete five sit to stands. Instructions for Administering the test: Complete one practice trial.
Time taken to complete one sit to stand (nearest second): ______________________
Time taken to complete five consecutive sit to stands (nearest second): ____________
Level of hand assistance required to do five sit to stands?
Placing both hands on the arms of the chair
Placing right hand on the arm of the chair in the first trial only
Placing right hand on the arm of the chair in all the five trials
Placing left hand on the arm of the chair in the first trial only
Placing left hand on the arm of the chair in all the five trials
No hand assistance required
Comments: ____________________________________________________________
Reference: Csuka, M., & McCarty, D.J. (1985). Simple method for measurement of lower extremity muscle strength. American Journal of Medicine, 78, 77-81.

Berg Balance Test Name Date Location Rater GENERAL INSTRUCTIONS Please demonstrate each task and/or give instructions as written. When scoring, please record the lowest response category that applies for each item. In most items, the subject is asked to maintain a given position for specific time. Progressively more points are deducted if the time or distance requirements are not met, if the subject's performance warrants supervision, or if the subject touches an external support or receives assistance from the examiner. Subjects should understand that they must maintain their balance while attempting the tasks. The choices of which leg to stand on or how far to reach are left to the subject. Poor judgment will adversely influence the performance and the scoring. Equipment required for testing are a stopwatch or watch with a second hand, and a ruler or other indicator of 2, 5 and 10 inches (5, 12.5 and 25 cm). Chairs used during testing should be of reasonable height. Either a step or a stool (of average step height) may be used for item #12.
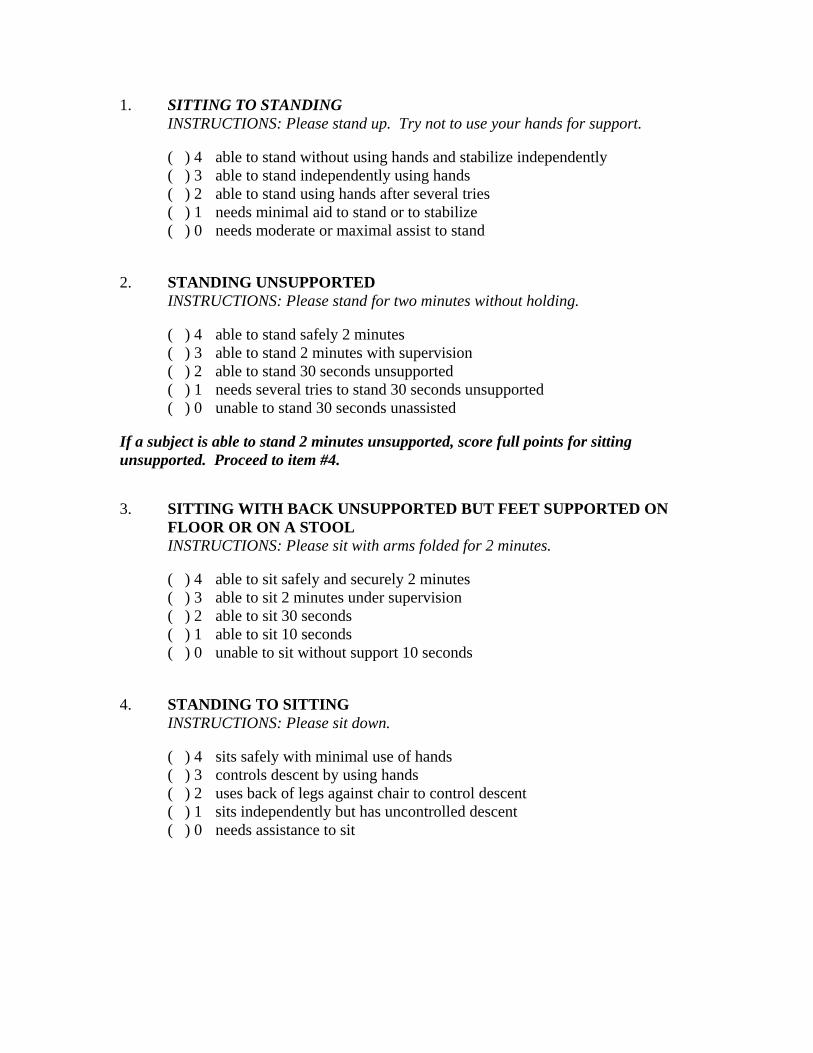
1. SITTING TO STANDING INSTRUCTIONS: Please stand up. Try not to use your hands for support. ( ) 4 able to stand without using hands and stabilize independently ( ) 3 able to stand independently using hands ( ) 2 able to stand using hands after several tries ( ) 1 needs minimal aid to stand or to stabilize ( ) 0 needs moderate or maximal assist to stand 2. STANDING UNSUPPORTED INSTRUCTIONS: Please stand for two minutes without holding. ( ) 4 able to stand safely 2 minutes ( ) 3 able to stand 2 minutes with supervision ( ) 2 able to stand 30 seconds unsupported ( ) 1 needs several tries to stand 30 seconds unsupported ( ) 0 unable to stand 30 seconds unassisted If a subject is able to stand 2 minutes unsupported, score full points for sitting unsupported. Proceed to item #4. 3. SITTING WITH BACK UNSUPPORTED BUT FEET SUPPORTED ON
FLOOR OR ON A STOOL INSTRUCTIONS: Please sit with arms folded for 2 minutes. ( ) 4 able to sit safely and securely 2 minutes ( ) 3 able to sit 2 minutes under supervision ( ) 2 able to sit 30 seconds ( ) 1 able to sit 10 seconds ( ) 0 unable to sit without support 10 seconds 4. STANDING TO SITTING INSTRUCTIONS: Please sit down. ( ) 4 sits safely with minimal use of hands ( ) 3 controls descent by using hands ( ) 2 uses back of legs against chair to control descent ( ) 1 sits independently but has uncontrolled descent ( ) 0 needs assistance to sit
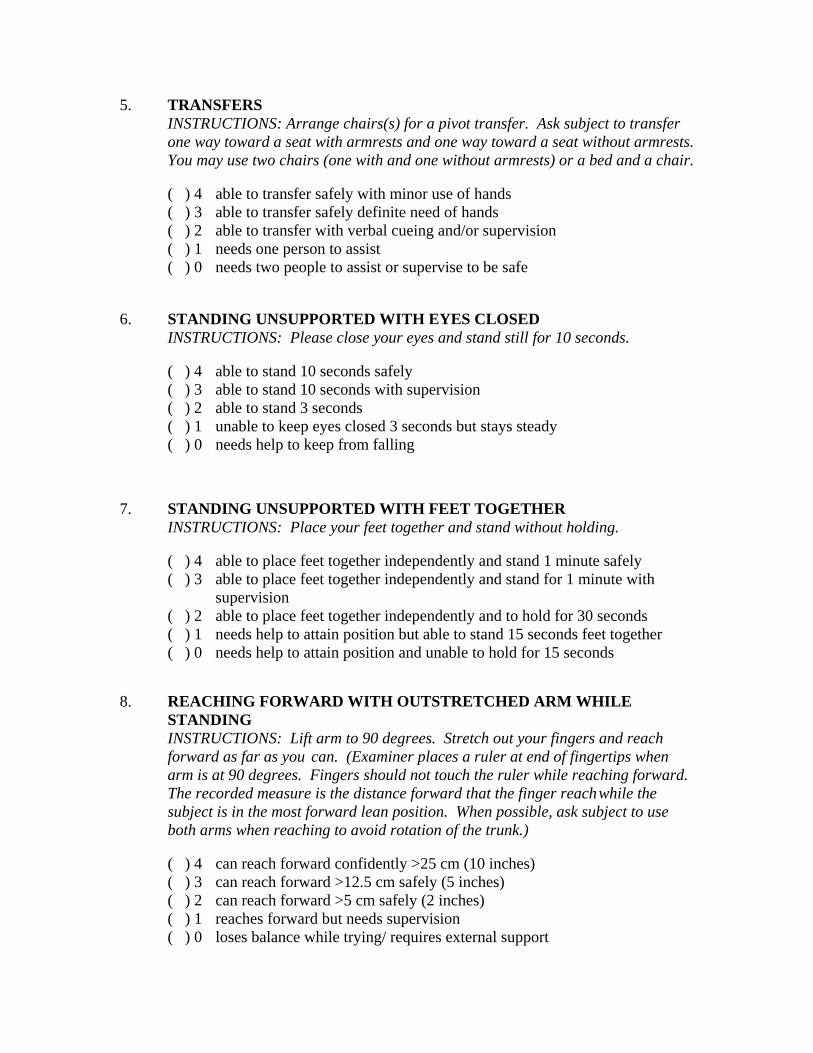
5. TRANSFERS INSTRUCTIONS: Arrange chairs(s) for a pivot transfer. Ask subject to transfer one way toward a seat with armrests and one way toward a seat without armrests. You may use two chairs (one with and one without armrests) or a bed and a chair. ( ) 4 able to transfer safely with minor use of hands ( ) 3 able to transfer safely definite need of hands ( ) 2 able to transfer with verbal cueing and/or supervision ( ) 1 needs one person to assist ( ) 0 needs two people to assist or supervise to be safe 6. STANDING UNSUPPORTED WITH EYES CLOSED INSTRUCTIONS: Please close your eyes and stand still for 10 seconds. ( ) 4 able to stand 10 seconds safely ( ) 3 able to stand 10 seconds with supervision ( ) 2 able to stand 3 seconds ( ) 1 unable to keep eyes closed 3 seconds but stays steady ( ) 0 needs help to keep from falling 7. STANDING UNSUPPORTED WITH FEET TOGETHER INSTRUCTIONS: Place your feet together and stand without holding. ( ) 4 able to place feet together independently and stand 1 minute safely
( ) 3 able to place feet together independently and stand for 1 minute with supervision
( ) 2 able to place feet together independently and to hold for 30 seconds ( ) 1 needs help to attain position but able to stand 15 seconds feet together ( ) 0 needs help to attain position and unable to hold for 15 seconds 8. REACHING FORWARD WITH OUTSTRETCHED ARM WHILE STANDING INSTRUCTIONS: Lift arm to 90 degrees. Stretch out your fingers and reach forward as far as you can. (Examiner places a ruler at end of fingertips when
arm is at 90 degrees. Fingers should not touch the ruler while reaching forward. The recorded measure is the distance forward that the finger reach while the
subject is in the most forward lean position. When possible, ask subject to use both arms when reaching to avoid rotation of the trunk.) ( ) 4 can reach forward confidently >25 cm (10 inches) ( ) 3 can reach forward >12.5 cm safely (5 inches) ( ) 2 can reach forward >5 cm safely (2 inches) ( ) 1 reaches forward but needs supervision ( ) 0 loses balance while trying/ requires external support

9. PICK UP OBJECT FROM THE FLOOR FROM A STANDING POSITION INSTRUCTIONS: Pick up the shoe/slipper which is placed in front of your feet. ( ) 4 able to pick up slipper safely and easily ( ) 3 able to pick up slipper but needs supervision ( ) 2 unable to pick up but reaches 2-5cm (1-2 inches) from slipper and keeps balance independently ( ) 1 unable to pick up and needs supervision while trying ( ) 0 unable to try/needs assist to keep from losing balance or falling 10. TURNING TO LOOK BEHIND OVER LEFT AND RIGHT SHOULDERS WHILE STANDING INSTRUCTIONS: Turn to look directly behind you over toward left shoulder. Repeat to the right. (Examiner may pick an object to look at directly behind the subject to encourage a better twist turn.) ( ) 4 looks behind from both sides and weight shifts well ( ) 3 looks behind one side only other side shows less weight shift ( ) 2 turns sideways only but maintains balance ( ) 1 needs supervision when turning ( ) 0 needs assist to keep from losing balance or falling 11. TURN 360 DEGREES
INSTRUCTIONS: Turn completely around in a full circle. Pause. Then turn a full circle in the other direction.
( ) 4 able to turn 360 degrees safely in 4 seconds or less ( ) 3 able to turn 360 degrees safely one side only in 4 seconds or less
( ) 2 able to turn 360 degrees safely but slowly ( ) 1 needs close supervision or verbal cueing ( ) 0 needs assistance while turning 12. PLACING ALTERNATE FOOT ON STEP OR STOOL WHILE STANDING UNSUPPORTED INSTRUCTIONS: Place each foot alternately on the step/stool. Continue until each foot has touched the step/stool four times. ( ) 4 able to stand independently and safely and complete 8 steps in 20 seconds ( ) 3 able to stand independently and complete 8 steps >20 seconds ( ) 2 able to complete 4 steps without aid with supervision ( ) 1 able to complete >2 steps needs minimal assist ( ) 0 needs assistance to keep from falling/unable to try

13. STANDING UNSUPPORTED ONE FOOT IN FRONT INSTRUCTIONS: (DEMONSTRATE TO SUBJECT)
Place one foot directly in front of the other. If you feel that you cannot place your foot directly in front, try to step far enough ahead that the heel of your forward foot is ahead of the toes of the other foot. (To score 3 points, the length of the step should exceed the length of the other foot and the width of the stance should approximate the subject's normal stride width)
( ) 4 able to place foot tandem independently and hold 30 seconds ( ) 3 able to place foot ahead of other independently and hold 30 seconds ( ) 2 able to take small step independently and hold 30 seconds ( ) 1 needs help to step but can hold 15 seconds ( ) 0 loses balance while stepping or standing 14. STANDING ON ONE LEG INSTRUCTIONS: Stand on one leg as long as you can without holding. ( ) 4 able to lift leg independently and hold >10 seconds ( ) 3 able to lift leg independently and hold 5-10 seconds ( ) 2 able to lift leg independently and hold = or >3 seconds ( ) 1 tries to lift leg unable to hold 3 seconds but remains standing independently ( ) 0 unable to try or needs assist to prevent fall ITEM DESCRIPTION SCORE (0-4) 1. Sitting to standing _____ 2. Standing unsupported _____ 3. Sitting unsupported _____ 4. Standing to sitting _____ 5. Transfers _____ 6. Standing with eyes closed _____ 7. Standing with feet together _____ 8. Reaching forward with outstretched arm _____ 9. Retrieving object from floor _____ 10. Turning to look behind _____ 11. Turning 360 degrees _____ 12. Placing alternate foot on stool _____ 13. Standing with one foot in front _____ 14. Standing on one foot _____ TOTAL (maximum 56) _____
0–20, wheelchair bound 21–40, walking with assistance 41–56, independent

*References Wood-Dauphinee S, Berg K, Bravo G, Williams JI: The Balance Scale: Responding to clinically meaningful changes. Canadian Journal of Rehabilitation 10: 35-50,1997 Berg K, Wood-Dauphinee S, Williams JI: The Balance Scale: Reliability assessment for elderly residents and patients with an acute stroke. Scand J Rehab Med 27:27-36, 1995 Berg K, Maki B, Williams JI, Holliday P, Wood-Dauphinee S: A comparison of clinical and laboratory measures of postural balance in an elderly population. Arch Phys Med Rehabil 73: 1073-1083, 1992 Berg K, Wood-Dauphinee S, Williams JI, Maki, B: Measuring balance in the elderly: validation of an instrument. Can. J. Pub. Health July/August supplement 2:S7-11, 1992 Berg K, Wood-Dauphinee S, Williams JI, Gayton D: Measuring balance in the elderly: preliminary development of an instrument. Physiotherapy Canada 41:304-311, 1989

Test Instructions for administering the Walkie-Talkie Test
Purpose: This test evaluates a person’s ability to divide his/her attention between multiple tasks, in this case the task of talking while walking.
Testing Procedures: As you walk to the location where you plan to start the fifty-foot walk, begin a conversation with the person you are testing. If the person stops walking in order to respond to you that is a sign that they are unable to adequately divide their attention between the tasks of walking while talking. It is important to ask open-ended questions that require more than a “Yes” or “No” response.
Interpreting Test Results: A “positive” score is recorded if the person stops walking in order to respond to your question. Alternatively, if the person is able to continue walking while conversing with you then a “negative” score is recorded. A “positive” score on this test suggests that the person really needs to direct his/her attention to the task of balancing while walking and will therefore not be ready to perform multiple tasks in the class until he/she has developed better overall balance abilities. Scoring Form
Positive Score (Stops to Respond)
Negative Score (Does not stop to respond)

Short Physical Performance Battery
Side-by-Side StandFeet together side-by-side for 10 sec
Semi-Tandem StandHeel of one foot against side of big toe of the
other for 10 sec
Tandem StandFeet aligned heel to toe for 10 sec
Measures the time required to walk 4 meters at a normal pace (use best of 2 times)
5 repeatsMeasures the time required to perform five risesfrom a chair to an upright position as fast as
possible without the use of the arms
<4.82 sec 4 pt4.82-6.20 sec 3 pt6.21-8.70 sec 2 pt>8.7 sec 1 ptUnable 0 pt
≤11.19 sec 4 pt11.20-13.69 sec 3 pt13.70-16.69 sec 2 pt>16.7 sec 1 pt>60 sec or unable 0 pt
1. Balance Tests< 10 sec (0 pt)
< 10 sec (+0 pt)
10 sec (1 pt)
10 sec (+1 pt)
1m 2m 3m 4m
10 sec (+2 pt)3-9.99 sec (+1 pt)<3 sec (+0 pt)
Go to 4-MeterGait Speed Test
Go to 4-MeterGait Speed Test
3. Chair Stand Test
2. Gait Speed Test
Pre-testParticipants fold their arms across their chest
and try to stand up once from a chairStop (0 pt)
able
unable

Study ID Date Tester Initials
SHORT PHYSICAL PERFORMANCE BATTERY PROTOCOL AND SCORE SHEET
All of the tests should be performed in the same order as they are presented in this protocol. Instructions tothe participants are shown in bold italic and should be given exactly as they are written in this script.
1. BALANCE TESTSThe participant must be able to stand unassisted without the use of a cane or walker. You may help the participant to get up.
Now let’s begin the evaluation. I would now like you to try to move your body in different movements. I will first describe and show each movement to you. Then I’d like you to try to do it. If you cannot do a particular movement, or if you feel it would be unsafe to try to do it, tell me and we’ll move on to the next one. Let me emphasize that I do not want you to try to do any exercise that you feel might be unsafe.
Do you have any questions before we begin?
A. Side-by-Side Stand1. Now I will show you the first movement.
2. (Demonstrate) I want you to try to stand with your feet together, side-by-side, for about 10 seconds.
3. You may use your arms, bend your knees, or move your body to maintain your balance, but try not to move your feet. Try to hold this position until I tell you to stop.
4. Stand next to the participant to help him/her into the side-by-side position.
5. Supply just enough support to the participant’s arm to prevent loss of balance.
6. When the participant has his/her feet together, ask “Are you ready?”
7. Then let go and begin timing as you say, “Ready, begin.”
8. Stop the stopwatch and say “Stop” after 10 seconds or when the participant steps out of position or grabs your arm.
9. If participant is unable to hold the position for 10 seconds, record result and go to the gait speed test.

Study ID Date Tester Initials
B. Semi-Tandem Stand1. Now I will show you the second movement.
2. (Demonstrate) Now I want you to try to stand with the side of the heel of one foot touching the big toe of the other foot for about 10 seconds. You may put either foot in front, whichever is more comfortable for you.
3. You may use your arms, bend your knees, or move your body to maintain your balance, but try notto move your feet. Try to hold this position until I tell you to stop.
4. Stand next to the participant to help him/her into the semi-tandem position
5. Supply just enough support to the participant’s arm to prevent loss of balance.
6. When the participant has his/her feet together, ask “Are you ready?”
7. Then let go and begin timing as you say “Ready, begin.”
8. Stop the stopwatch and say “Stop” after 10 seconds or when the participant steps out of position or grabs your arm.
9. If participant is unable to hold the position for 10 seconds, record result and go to the gait speed test.
C. Tandem Stand 1. Now I will show you the third movement.
2. (Demonstrate) Now I want you to try to stand with the heel of one foot in front of and touching the toes of the other foot for about 10 seconds. You may put either foot in front, whichever is more comfortable for you.
3. You may use your arms, bend your knees, or move your body to maintain your balance, but try notto move your feet. Try to hold this position until I tell you to stop.
4. Stand next to the participant to help him/her into the tandem position.
5. Supply just enough support to the participant’s arm to prevent loss of balance.
6. When the participant has his/her feet together, ask “Are you ready?”
7. Then let go and begin timing as you say, “Ready, begin.”
8. Stop the stopwatch and say “Stop” after 10 seconds or when the participant steps out of position or grabs your arm.

Study ID Date Tester Initials
SCORING:
A. Side-by-side-standHeld for 10 sec ❒ 1 point If participant did not attempt test or failed, circle why:Not held for 10 sec ❒ 0 points Tried but unable 1Not attempted ❒ 0 points Participant could not hold position unassisted 2If 0 points, end Balance Tests Not attempted, you felt unsafe 3
Not attempted, participant felt unsafe 4Participant unable to understand
Number of seconds held if instructions 5less than 10 sec: . sec Other (specify) 6
Participant refused 7
B. Semi-Tandem StandHeld for 10 sec ❒ 1 point Not held for 10 sec ❒ 0 pointsNot attempted ❒ 0 points (circle reason above)If 0 points, end Balance Tests
Number of seconds held if less than 10 sec: . sec
C. Tandem StandHeld for 10 sec ❒ 2 points Held for 3 to 9.99 sec ❒ 1 point Held for < than 3 sec ❒ 0 pointsNot attempted ❒ 0 points (circle reason above)
Number of seconds held if less than 10 sec: . sec
D. Total Balance Tests score (sum points)
Comments:

Study ID Date Tester Initials
2. GAIT SPEED TESTNow I am going to observe how you normally walk. If you use a cane or other walking aid and you feelyou need it to walk a short distance, then you may use it.
A. First Gait Speed Test1. This is our walking course. I want you to walk to the other end of the course at your usual speed,
just as if you were walking down the street to go to the store.
2. Demonstrate the walk for the participant.
3. Walk all the way past the other end of the tape before you stop. I will walk with you. Do you feel this would be safe?
4. Have the participant stand with both feet touching the starting line.
5. When I want you to start, I will say: “Ready, begin.” When the participant acknowledges this instruction say: “Ready, begin.”
6. Press the start/stop button to start the stopwatch as the participant begins walking.
7. Walk behind and to the side of the participant.
8. Stop timing when one of the participant’s feet is completely across the end line.
B. Second Gait Speed Test1. Now I want you to repeat the walk. Remember to walk at your usual pace, and go all the way
past the other end of the course.
2. Have the participant stand with both feet touching the starting line.
3. When I want you to start, I will say: “Ready, begin.” When the participant acknowledges this instruction say: “Ready, begin.”
4. Press the start/stop button to start the stopwatch as the participant begins walking.
5. Walk behind and to the side of the participant.
6. Stop timing when one of the participant’s feet is completely across the end line.

Study ID Date Tester Initials
GAIT SPEED TEST SCORING:
Length of walk test course: Four meters ❒ Three meters ❒
A. Time for First Gait Speed Test (sec)1. Time for 3 or 4 meters . sec2. If participant did not attempt test or failed, circle why:
Tried but unable 1Participant could not walk unassisted 2Not attempted, you felt unsafe 3Not attempted, participant felt unsafe 4Participant unable to understand instructions 5Other (Specify) 6Participant refused 7Complete score sheet and go to chair stand test
3. Aids for first walk……………None ❒ Cane ❒ Other ❒
Comments:
B. Time for Second Gait Speed Test (sec)1. Time for 3 or 4 meters . sec2. If participant did not attempt test or failed, circle why:
Tried but unable 1Participant could not walk unassisted 2Not attempted, you felt unsafe 3Not attempted, participant felt unsafe 4Participant unable to understand instructions 5Other (Specify) 6Participant refused 7
3. Aids for second walk………… None ❒ Cane ❒ Other ❒
What is the time for the faster of the two walks?Record the shorter of the two times . sec[If only 1 walk done, record that time] . sec
If the participant was unable to do the walk: ❒ 0 points
For 4-Meter Walk: For 3-Meter Walk:If time is more than 8.70 sec: ❒ 1 point If time is more than 6.52 sec: ❒ 1 pointIf time is 6.21 to 8.70 sec: ❒ 2 points If time is 4.66 to 6.52 sec: ❒ 2 pointsIf time is 4.82 to 6.20 sec: ❒ 3 points If time is 3.62 to 4.65 sec: ❒ 3 pointsIf time is less than 4.82 sec: ❒ 4 points If time is less than 3.62 sec: ❒ 4 points

Study ID Date Tester Initials
3. CHAIR STAND TESTSingle Chair Stand1. Let’s do the last movement test. Do you think it would be safe for you to try to stand up from a
chair without using your arms?
2. The next test measures the strength in your legs.
3. (Demonstrate and explain the procedure.) First, fold your arms across your chest and sit so that your feet are on the floor; then stand up keeping your arms folded across your chest.
4. Please stand up keeping your arms folded across your chest. (Record result).
5. If participant cannot rise without using arms, say “Okay, try to stand up using your arms.” This is the end of their test. Record result and go to the scoring page.
Repeated Chair Stands1. Do you think it would be safe for you to try to stand up from a chair five times without
using your arms?
2. (Demonstrate and explain the procedure): Please stand up straight as QUICKLY as you can five times, without stopping in between. After standing up each time, sit down and then stand up again. Keep your arms folded across your chest. I’ll be timing you with a stopwatch.
3. When the participant is properly seated, say: “Ready? Stand” and begin timing.
4. Count out loud as the participant arises each time, up to five times.
5. Stop if participant becomes tired or short of breath during repeated chair stands.
6. Stop the stopwatch when he/she has straightened up completely for the fifth time.
7. Also stop:• If participant uses his/her arms• After 1 minute, if participant has not completed rises• At your discretion, if concerned for participant’s safety
8. If the participant stops and appears to be fatigued before completing the five stands, confirm this byasking “Can you continue?”
9. If participant says “Yes,” continue timing. If participant says “No,” stop and reset the stopwatch.

Study ID Date Tester Initials
SCORINGSingle Chair Stand Test
YES NOA. Safe to stand without help ❒ ❒
B. Results:
Participant stood without using arms ❒ → Go to Repeated Chair Stand Test
Participant used arms to stand ❒ → End test; score as 0 points
Test not completed ❒ → End test; score as 0 points
C. If participant did not attempt test or failed, circle why:Tried but unable 1Participant could not stand unassisted 2Not attempted, you felt unsafe 3Not attempted, participant felt unsafe 4Participant unable to understand instructions 5Other (Specify) 6Participant refused 7
Repeated Chair Stand TestYES NO
A. Safe to stand five times ❒ ❒
B. If five stands done successfully, record time in seconds.
Time to complete five stands . sec
C. If participant did not attempt test or failed, circle why:Tried but unable 1Participant could not stand unassisted 2Not attempted, you felt unsafe 3Not attempted, participant felt unsafe 4Participant unable to understand instructions 5Other (Specify) 6Participant refused 7
Scoring the Repeated Chair TestParticipant unable to complete 5 chair stands or completes stands in >60 sec: ❒ 0 pointsIf chair stand time is 16.70 sec or more: ❒ 1 pointsIf chair stand time is 13.70 to 16.69 sec: ❒ 2 pointsIf chair stand time is 11.20 to 13.69 sec: ❒ 3 pointsIf chair stand time is 11.19 sec or less: ❒ 4 points

Study ID Date Tester Initials
Scoring for Complete Short Physical Performance Battery
Test ScoresTotal Balance Test score _____ pointsGait Speed Test score _____ pointsChair Stand Test score _____ points
Total Score _____ points (sum of points above)

INFORMATION FROM THE ONTARIO MINISTRY OF HEALTH AND LONG-TERM CARE FALLS PREVENTION AND MANAGEMENT AND CARE PLANNING
The Ministry of Health and Long-Term Care (MOHLTC) expects care plans to: establish a concern, set a goal in relation to that concern and capture interventions that lead to that goal. For those using Resident Assessment Instrument / Minimum Data Set (RAI-MDS) the concern should reflect information triggered by the Resident Assessment Protocols (RAPs).
Resident Concern, etiology/cause/signs symptoms
Risk for falls related to
Goal Should be Specific,
Measurable Acceptable, Real istic and Time Limited
Interventions Steps staff take to assist the
resident to achieve the identified goal
Example: Mr. Cee is at risk for falls related to wandering and lack of insight about when he should rest
Mr. Cee’s fall risk will be reduced by conditioning him to rest. By the next quarter Mr Cee will rest in the sitting room for at least 15 minutes twice a day – once in the morning and once in the afternoon.
Mr. Cee does not like being alone, RN, RPN and HCA/PSW will work with Mr. Cee to encourage him to sit in the lounge each morning and afternoon. Dietary will provide Mr. Cee’s snack in the lounge, if they find him wandering on the unit they will encourage him to return to the lounge before serving him. Nurse to review in one month to see if intervention is successful in conditioning Mr. Cee to learn to take a short rest.
Triggers for the Falls RAP
The resident assessment protocol (RAP) is one way of assessing a resident’s risk for falls. It has been tested and is valid and reliable. NON RAI-MDS Homes: RAI-MDS automatically generates Resident Assessment Protocols (RAPs), however you can use the triggers in the first column to identify residents at risk.
RAP Trigger Possible Care Planning Considerations
Fell in the past 30 days (J4a checked) Fell in the past 31 – 180 days (J4b checked)
The number one predictor of falls risk is a previous fall.
Wandering (Risk) (E4aA = 1,2,3)
Does the resident have a steady gait when wandering? Do they have adequate footwear? Does the resident use an appropriate ambulatory aid? Do they remember to use it when wandering? Does the resident know their own limits? Do they rest when wandering or do they ambulate until exhausted?
Dizziness (Risk) (J1f= checked)
Investigate cause of dizziness and seek treatment. If dizziness is associated with specific events for example orthostatic hypotension when rising from bed in the morning make sure the care plan reflects that the client needs assistance at this time.

RAP Trigger Possible Care Planning Considerations
Use of Trunk restraint (Risk) (P4c = 1,2)
Review client care to see if trunk restraint is necessary. If it is make sure the care plan reflects the reason for its use and a plan of monitoring its use.
Use of antianxiety drugs (Risk) (O4b= 1-7)
Review the use of anti anxiety drugs. Are they a recent addition to the resident’s medications? Have they been reviewed by a physician? Does the resident need the drug? For example changes in the resident’s health or circumstances may make it worth discussing the continued use of antianxiety drugs with the resident/family and physician
Use of antidepressant drugs (Risk) (O4c= 1-7) See above on the use of antianxiety drugs
Everyone’s fall’s risk increases as they age so if is important to consider modifiable risk factors
when care planning for both groups.
Factors to prevent falls or minimize fall injury Some Care planning considerations
Hearing and/or Vision
Has there been a change in the resident’s hearing or vision this quarter? If so what is causing the change? Do glasses or hearing aids need review? Does the resident need to be reviewed by their family doctor, optometrist or audiologist?
Gait
Is the resident’s footwear appropriate? Does the resident need footcare? Has physiotherapy assessed the resident and are they participating in a physio program?
Mobility Aids Is the mobility aid appropriate and in good repair?
Transfer
Is there appropriate assistance for the resident to transfer/walk? Remember to customize the care plan and focus on the resident’s abilities, for example a person might only need help transferring out of bed in the morning; once they are up they may be able to adequately transfer themselves. The care plan might state they are one person assist for am care, and supervised ambulation for the rest of the day.
Toileting Does the resident require assistance? Is the toileting schedule driven by the resident’s needs?
Environment
Has the resident been orientated to the room and the environment – are there any prompts that would assist with orientation. Is there clutter? Has the resident and family been given information on safety and risks?
Pain
Is the resident’s pain adequately managed? Do they require prophylactic analgesic in order to assist them to be mobile for am care or to participate in an exercise program? Does a PRN order need to become a standing order to ensure consistency in administration?
Dietary Does the resident have adequate dietary intake? Do they require vitamin D supplementation?
Hip Protectors Is there a need for hip protectors? Has this been discussed with the resident and/or family? If using hip protectors is this reflected in the care plan?
Exercise If there are different programs available at the home which program might benefit the resident? Who might need to assist and encourage the resident in participating in exercises

Have you had a fall in the past 6 months? If yes, how many: _____
Have you ever had a fall that resulted in a broken bone?
Are you afraid that you might fall again?
Do you have a problem with your balance?
Do you have a problem with your vision?
Do you get dizzy when you stand up quickly?
Do you have a problem with your memory?
Pre-admission to Residential Care
FALL CHECKLIST
If you or your loved one are waiting to move to a Residential Care Facility, please complete the
following and give this to the admitting nurse.
Completed by person entering care, OR
Completed by family/ caregiver.
Date: ___________________________ (dd/mm/yy)

Reduce Your Risk of
Falling or Being Injured
from a Fall
Be physically active for at least 30 minutes each day.
If you have balance problems, use a mobility aid.
Have your vision checked each year.
Try to drink at least 8 glasses of non-caffeinated beverage each day.
Eat a balanced diet that includes 1200 milligrams of calcium and 800 to 2000 IU of vitamin D daily from food sources and/or supplements.
Wear non-slip footwear with good support.
Have your doctor or pharmacist review your medications and supplements to reduce your fall risk.
Ensure that your home has good lighting, handrails on stairs, grab bars in the bathroom and is free of trip hazards.
Wear hip protectors to reduce the risk of a hip fracture if you fall.
Limit alcohol intake as this impairs your balance and judgment.
1
2
3
4
5
6
7
8
9
10
FOR MORE INFORMATION
www.hiphealth.ca/CEMFIA.htm





























