Embed Size (px)
Citation preview

FACIAL PARALYSIS: MODERATION OF NON-PARALYSED MUSCLES
By JoRGE NIKLISON, M.D.
From the Department of Plastic Surgery, Durand Hospital, Buenos Aires
THE face, considered as a whole, constitutes the most important means whereby human beings give expression to their feelings. It will therefore be appreciated that, when consl~dering the problem of facial paralysis, special attention must be paid to the fact that the face is something dynamic, endowed with functional symmetry.
Obviously, there is no possibility of symmetry in a face with a motionless side while the other has exaggerated movements in the forehead or around the mouth. Thus, in order to counteract these undesirable movements which provoke distortion of the expression so as to obtain a reasonable equilibrium with the paralysed side, the surgeon should aim at regulating or moderating overaction of certain muscles on the non-paralysed half.
In I956 we proposed a plan for the management of the disfigurement brought about by facial paralysis, which plan comprised both a static and dynamic correction, as well as treatment of the opposite or unaffected side of the face. In the present paper we will consider only the last mentioned aspect and instead of referring to " opposite s ide" we prefer speaking of " overactive " areas because the levator palpebra: superioris muscle of the paralysed side should also be submitted to functional moderation.
Functional Asymmetry of the Face in Action.--Contrary to current belief, facial paralysis constitutes a condition which affects both sides of the face.
In many patients--including those operated on with good results--the non-paralysed side shows disfigurement when the patient speaks, smiles, laughs, etc. This is due to the fact that the undamaged opposite muscles, devoid of the restraining action of the corresponding antagonists, behave as unbridled elements and disproportionately at the eyebrows, the lips, and the upper lid.
Generally speaking there is no doubt that the grimaces or contortions originated by this pulling action are even more objectionable than a totally inexpressive facies.
Such is the importance of the uncontrollable muscular action in the production of disfigurement that the moderation referred to has been the only treatment in some of our patients.
In the case of facial paralysis the excessive tonicity of some of the muscles manifests itself in the form of disfigurement of some areas such as : (I) Permanent wrinkling of the sound half of the forehead, accompanied by lifting of the corre- sponding eyebrow ; (2) widening of the palpebral fissure on the paralysed side. This is due to the levator muscle (third cranial nerve) acting without the restraint of its antagonist (orbicularis muscle); (3) a certain degree of abnormal pulling of the upper or lower lip when pronouncing labial consonants, due to exaggerated contraction of the corresponding quadratus muscle ; (4) shrinking of the lips
397

398 BRITISH JOURNAL OF PLASTIC SURGERY
through abnormal contraction of the sound orbicularis muscle ; (5) marked distortion of the smile which turns wry owing to exaggerated action of the zygomatic muscle. It is incumbent upon the surgeon to determine exactly which of the above-mentioned muscles gives rise to disturbance in order to remedy the situation.
Frontal Area . - - In some of the patients the skin of the paralysed side becomes smooth and motionless while the eyebrow descends in an appreciable manner. At times there is blepharochalasis as well. On the opposite side exaggerated contraction sets in, accompanied by steady wrinkling and elevation of the super- ciliary region. Most patients are able to counteract this contraction at will but it reappears as soon as their attention is distracted.
Taking into account that the absence of wrinkles in the forehead is not rare in many persons who are not in the habit of knitting the eyebrows, a practical
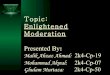
A B FIG. I
A, Permanent and evident contraction of the sound frontalis muscle, in marked contrast with the opposite side which has a smooth skin and a placid expression. B, Practically normal appearance after nerve resection.
solution for the deformities provoked by facial paralysis in the frontal region consists, precisely, in creating a smooth area with an expression of tranquiUity which is undoubtedly less conspicuous than the usual asymmetry prevailing in these patients (Fig. I).
Ramisection of the frontal branch of the facial nerve has given us excellent results in these cases. (It should be recalled that this paper does not touch upon correction of the paralysed side.)
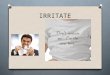
I f surgery is done under general anaesthesia the nerve can be located accurately by faradic stimulation. However, if the operation is to be performed under local anaesthesia, the nervous pathway should be identified by tracing two divergent lines extending from a point just in front of the ear lobe towards the upper and lower wrinkles of the forehead, as indicated in Figure 2, B.
Within the limits of that area and approximately one fingerbreadth above the zygomatic arch, the anaesthetic agent (2 per cent. solution of procaine) is injected. After a few minutes the muscle should become motionless and when that happens the needle is left in situ as a guide to subsequent dissection.
The incision is made along the ha i~ne in the temporal area (Fig. 2, B and c) and the nerve should be looked for along the epicranial fascia at the point indicated

FACIAL PARALYSIS 399
by the previously mentioned test. It should be recalled that between the skin and the temporal fascia there is nothing but the epicranial fascia which is a thin fibrous layer containing the nerve and fatty tissue. Since it is not necessary to get the nerve isolated, a selected portion of this layer can be resected with the certainty that the desired ramus will be carried off as well.
A C B
FIG. 2
Fig. 2 . - -A, Anatomical dissection showing distribution of facial nerve. Arrow points to frontal ramus running from the ear lobe to the forehead. B, Incision along hairline, opposite to eyebrow. Dotted area represents zone to be dissected and excised as it contains the ramus. C, Fibrous layer interposed between scalp and
temporal fascia.
Fig. 3.--Lagophthalmos, largely due to un- bridled action of levator palpebr~e superioris muscle. Usual aspect when patient attempts
to close the eyes.
FIG. 3
Palpebral Fissure (Lagophtha lmos) . - -Movemen t of the lids is dependent upon the action of two antagonistic muscles. Closing is effected by the orbicularis oculi muscle activated by the facial nerve, while opening is governed by the levator palpebrm superioris muscle activated by the oculomotor (third cranial) nerve. When facial paralysis sets in, the latter muscle is deprived of its antagonistic restraint and, consequently, the upper lid fails to cover the eyeball, especially during sleep (Fig. 3).

400 BRITISH JOURNAL OF PLASTIC SURGERY
Under such circumstances widening of the palpebral fissure takes place and lagophthalmos sets in. When getting ready to sleep the patient finds himself forced to use one of his fingers to lower the lid, but when the lifting action manifests itself again, part of the eyeball is left uncovered.
Inasmuch as it is impossible to restore normal function of the orbicularis oculi muscle, correction of the lagophthalmos can be achieved only by sectioning the levator muscle. This procedure brings about a partial lowering of the upper lid which thus is able to fulfil its specific role of covering the eyeball.
At first we feared that the operation referred to would result in blepharoptosis ; however, experience has shown us that some action is regained and the lid level finally becomes more or less equalised with respect to that of the other side. Of course, in those cases in which the lagophthalmos is partly due to drooping of the
A
Palpebral fissure.
B C
FIG. 4 Moderation of upper lid elevation was obtained through division of
corresponding levator muscle.
lower lid, this must be raised either during the same operative procedure or at some later date.
Resection of the levator muscle can be effected by cutaneous or mucosal approach. The latter, however, is to be preferred for its directness, as the muscle lies immediately below the conjunctiva; besides, no visible scar remains (Fig. 4, A, 13 and c).
The operation is carried out under local anaesthesia with the same approach as that recommended by Blastovicz for the treatment of blepharoptosis.
Oral Opening. - -The labial ring is regulated by a system comprising approxi- mately ten muscles on each side of the face. One of thesemorbicularis oris muscle--produces constriction while the remaining ones produce distension by pulling in a radiated fashion (Fig. 5).
In the presence of facial paralysis the " bridles " which regulate facial expression lose their state of equilibrium and the uninvolved muscles behave in an uncontrollable manner. The abnormal pulls and grimaces provoked by laughter are quite beyond the patient's restraint and cause him more preoccupation than the paralysed side. It is therefore .imperative to regulate such immoderate function.

FACIAL PARALYSIS 4Ol
There are four muscles which usually take part in this functional disorder: the orbicularis muscle which puckers the lips towards the sound side, and three dilators which exert a pulling action from precise points. These dilators are the
A B C
FIG. 5 Oral opening..A_, Hypertonicity. At rest the face presents a permanent contraction of the muscles around the lips, especially the levator ones. B, Hypercontractility. Under action the excessive degree of contraction can be dearly appreciated about the levator muscles.
C, The lower lip is pulled down when talking or when the mouth is opened.
quadratus labii superioris muscle in the upper lip, the quadratus labii inferioris muscle in the lower lip, and the zygomatic muscle in the labial commissure. Very rarely patients register exaggerated function of all these muscles (Fig. 6); generally speaking, only two or three of them need to be eliminated.
FIG. 6 Most commonly found conditions about the mouth in patients wit h facial paralysis.
It should be mentioned that the smile is the result of an associated action : that of the risorius, which causes lateral retraction, and that of the zygomafic, which acts as a levator. Thus, even though this last-mentioned action should cease, only part of the smile is lost.
The situation may be regulated by reducing hyperfunction in the chosen muscle either through denervation, muscular resection, or a combination of both procedures. The question of choosing between excision of a portion of muscle or resection of the corresponding motor ramus depends upon each case in particular

402 BRITISH JOURNAL OF PLASTIC SURGERY
as well as upon the surgeon's preference. Approach can be obtained via the skin or the mucosa, the former being usually simpler. The incision is made along the nasolabial fold and no scar is visible after a time (Fig. 7). It might be argued
A B C D
FIG. 7 External or skin approach. The nasolabial fold is the line of the incision. The quadratus superioris muscle is to be divided. Careful anatomical dissection allows its identification. If its limits are passed, the branches of the lateral facial nerve are seen as they go to the muscle and as they continue their course towards the ala nasi (A). The muscle is divided (B and C). Only the necessary denervation is carried out. Finally a bundle of vertical branches is found belonging to the infra-
orbital nerve which is left untouched (D).
that this approach is better in the sense that the anatomical elements are found in their normal position, but the mucosal incision, on the other hand, provides a direct access to them.
A B C
Fro. 8
Muscular resection through rear approach.
Originally we employed the external approach but eventually we decided to adopt the posterior one for muscular or nervous resections, in keeping with the following techniques: For the zygomatic musclemvertical incision in the oral mucosa some 2 cm. from the angle of the lips, resection of approximately r cm. of muscle being made at the point where its fibres intermingle with those of the orbicularis muscle (Fig. 8, A). For the quadratus labii superioris muscle--incision some 3 cm. long in the inner side of, the upper lip at the point where abnormal pulling takes place. This incision is made parallel to the lip's margin and the

FACIAL PARALYSIS 403
quadratus muscle fibres are carefully cut through until exposure is obtained of the under surface of the labial skin. By means of scissors this layer is cut away from the vermilion border upwards (Fig. 8, B). The nerve fibres which reach the lateral aspect of the muscle are also eliminated at the same time. For the quadratus labii inferioris muscle--vertical incision in the inner side of the lip extending downwards from the level of the labial commissure. One must find its muscular fibres towards the middle line, excision being carried out with scissors. The nerve branches which reach the muscle transversely lie in the latero-external aspect and should be resected after proper identification (Fig. 8, c).
In some of our first cases ramisection of the ramus marginalis mandibularis of the facial nerve was carried out through an incision made below the mandibular angle (gonion) but in view of the fact that this procedure brought unnecessary paralysis to the triangularis and mentalis muscles, it was subsequently discontinued
A B C
FIG, 9 Muscular and nervous resection through rear approach.
and replaced by a direct approach of the muscle and the nerves inserted in the lateral aspect.
The orbicularis oris muscle is the most difficult to regulate inasmuch as only a partial paralysis is usually required. It is imperative to employ electric stimulation under general anaesthesia in order to determine which branches are responsible for the localised pull or partial deformation of the orbicular ring.
All these procedures can be carried out under local or general anmsthesia, the latter being mandatory if faradic stimulation is to be resorted to. Even so, epinephrine infiltration is useful to obtain vasoconstriction during dissection. As a guide for the subsequent steps of the operation it is also helpful to use marks on the skin showing the position of the muscles, after which two threads are pierced through the whole thickness of the lip at the muscle borders. Pulling from these threads facilitates eversion of the lip with consequent exposure of its inner surface.
It might be mentioned that the zygomatic muscle is the easiest to find and to cut owing to its being a well-defined muscular bundle. On the contrary, neither the superior nor the inferior quadratus muscles are well isolated or defined because they are represented by a layer adherent to the skin from which fleshy fibres must be peeled off.

404 B R I T I S H JOURNAL OF PLASTIC SURGERY
I f ramisection should be decided upon, the fine nerve branches can also be located by cutaneous or mucosal approach (Figs. 7 and 9). Faradic stimulation is recommended for either of these procedures although it can be dispensed with i f one is intimately acquainted with the anatomy of that area.
Figure IO illustrates the most frequent situations.
FIG. IO
A and B, Correction, through resection, of abnormal pulling down action of the quadratus labii inferioris muscle. C and D, Correction, through ramisection, of puckered lips due to contraction of orbicularis muscle. E and F, Correction, through muscle and nerve resection, of distortion due to abnormal pull of orbicularis and quadratus labii superioris muscles. G and H, Correction, through muscular resection, of exaggerated smile due to unbridled action of zygomatic muscle.
DISCUSSION
Facial paralysis poses a complex problem because it affects both sides of the face. From a functional point of view--which is the most important as far as facial expression is concerned--it should be noted that when certain muscles lack the moderating action of the corresponding antagonists, uncontrollable movements are originated which provoke marked distortion of the forehead, the upper lid, and the oral opening.
I f attention is concentrated on treating the paralysed side alone, the problem will have only a partial solution. Thus, treatment of the two sides is indispensable taking into account that both of them participate in the functional asymmetry.
From a functional point of view the so-called " s o u n d " side cannot be classified as normal because of the excess of tone and contraction of some of its muscles, and these must be correctly identified and regulated. This is the only logical way of levelling differences between both sides of the face without losing the necessary degree of expression.

FACIAL PARALYSIS 405
SUMMARY
The need is pointed out of regulating or moderating the hyperfunction of some muscles as the logical solution for distorted expression in cases of facial paralysis.
Clinical identification of these muscles and the corresponding surgical treatment are commented upon.
REFERENCE
NIKLISON, J. (I956). Plast. reconstr. Surg., x7, 276.
Submitted for publication, July I964.
4 E

![Moderation process for dummies [Read-Only] - pdfMachine ... · 1. PLAN FOR MODERATION Before you can start with Moderation, ask the following questions first:-Who asked for moderation?-Why](https://img.pdfslide.us/doc/110x75/5bc5d2c209d3f264788dfdf4/moderation-process-for-dummies-read-only-pdfmachine-1-plan-for-moderation.jpg)