Embed Size (px)
Citation preview
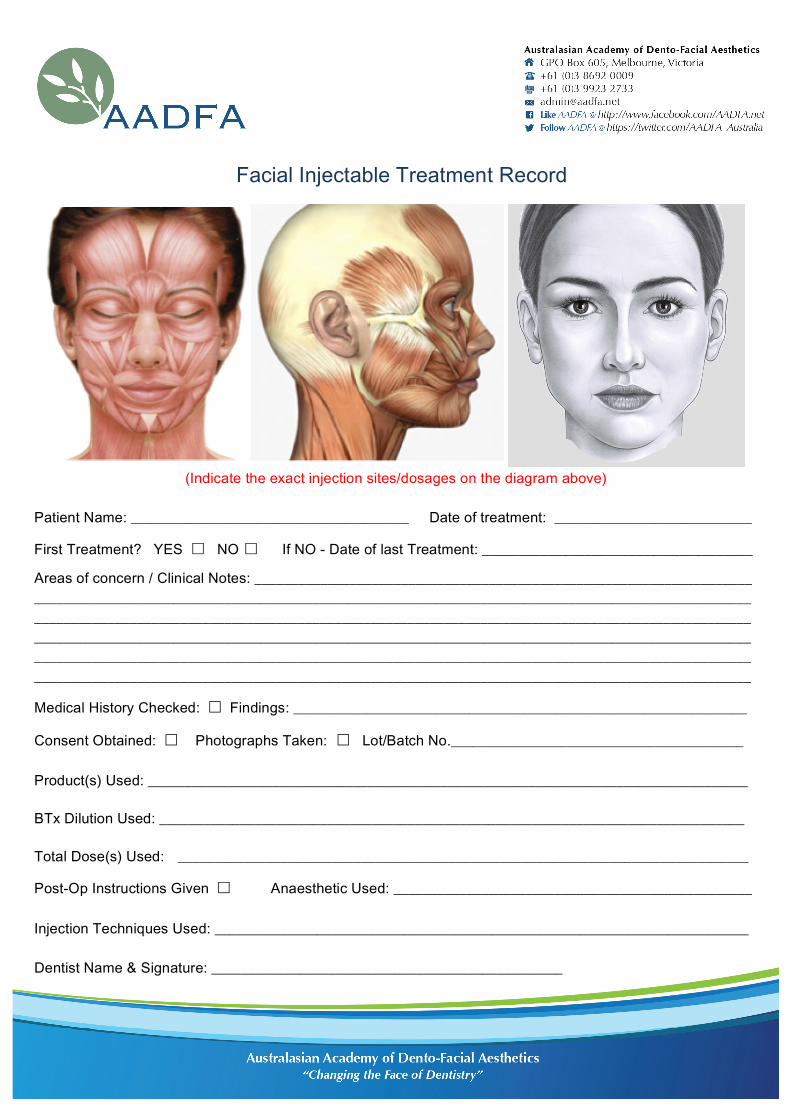
(Indicate the exact injection sites/dosages on the diagram above)
Patient Name: ______________________________________ Date of treatment: ___________________________
First Treatment? YES ☐ NO ☐ If NO - Date of last Treatment: _____________________________________
Areas of concern / Clinical Notes: ____________________________________________________________________ __________________________________________________________________________________________________ __________________________________________________________________________________________________ __________________________________________________________________________________________________ __________________________________________________________________________________________________ __________________________________________________________________________________________________
Medical History Checked: ☐ Findings: ______________________________________________________________
Consent Obtained: ☐ Photographs Taken: ☐ Lot/Batch No.________________________________________
Product(s) Used: __________________________________________________________________________________
BTx Dilution Used: ________________________________________________________________________________
Total Dose(s) Used: ______________________________________________________________________________
Post-Op Instructions Given ☐ Anaesthetic Used: _________________________________________________ Injection Techniques Used: _________________________________________________________________________ Dentist Name & Signature: ________________________________________________
Facial Injectable Treatment Record