Embed Size (px)
Citation preview

Clinical Paper
Congenital Craniofacial Anomalies
Int. J. Oral Maxillofac. Surg. 2010; 39: 1066–1073doi:10.1016/j.ijom.2010.06.020, available online at http://www.sciencedirect.com
Facial animation in patients withMoebius and Moebius-likesyndromesB. Bianchi, C. Copelli, S. Ferrari, A. Ferri, E. Sesenna: Facial animation in patientswith Moebius and Moebius-like syndromes. Int. J. Oral Maxillofac. Surg. 2010; 39:1066–1073. # 2010 International Association of Oral and Maxillofacial Surgeons.Published by Elsevier Ltd. All rights reserved.
Abstract. Moebius syndrome, a rare congenital disorder of varying severity, involvesmultiple cranial nerves and is characterised predominantly by bilateral or unilateralparalysis of the facial and abducens nerves. Facial paralysis causes inability to smileand bilabial incompetence with speech difficulties, oral incompetence, problemswith eating and drinking, including pocketing of food in the cheek and dribbling, aswell as severe drooling. Other relevant clinical findings are incomplete eye closureand convergent strabismus. The authors report on 48 patients with Moebius andMoebius-like syndromes seen from 2003 to September 2007 (23 males and 25females, mean age 13.9 years). In 20 cases a reinnervated gracilis transplant wasperformed to re-animate the impaired sides of the face. In this series, all free-muscletransplantations survived the transfer, and no flap was lost. In 19 patients completereinnervation of the muscle was observed with an excellent or good facial symmetryat rest in all patients and whilst smiling in 87% of cases. In conclusion, according tothe literature, the gracilis muscle free transfer can be considered a safe and reliabletechnique for facial reanimation with good aesthetic and functional results.
0901-5027/1101066 + 08 $36.00/0 # 2010 International Association of Oral and Maxillofacial Surge
B. Bianchi, C. Copelli,S. Ferrari, A. Ferri, E. SesennaMaxillofacial Surgery, Head and NeckDepartment, University of Parma, Italy
Keywords: Moebius syndrome; paralysis; ani-mation; face.
Accepted for publication 14 June 2010Available online 22 July 2010
Moebius syndrome/sequence is a rare con-genital disorder of varying severity char-acterised by bilateral or unilateralparalysis of the facial and abducensnerves1,3,4,7,14,17,19,20. Its aetiology isunknown, but environmental and geneticfactors have been implicated. Recent stu-dies suggest the occurrence of a vasculardisruption causing a hypoxic/ischaemicinsult to the brain stem during the firsttrimester, which could affect some of thecranial nerves4,5,7,14,19,20. The hypoxic/ischaemic insult might result from uterinecontractions due to a variety of causes. Anabortifaciant drug, misoprostol, has been
linked to self-induced but unsuccessfulabortions that result in some subjects withthe clinical findings of Moebiussequence14. Although evidence of agenetic mechanism has been noted in afew subjects, most cases of Moebiussequence appear to be sporadic14.
Paralysis of the VI and VII cranialnerves leads to lack of function in themuscles they supply. Lateral gaze andfacial animation are absent. When theparalysis is bilateral, it can be asymmetric,and facial movement, when present, isalways located in the lower face withplatysmal activity or depressor anguli oris
activity. Effective lower-lip support,lower-lip elevation for bilabial speechproduction and commissure movementand upper-lip elevation for smiling andemotional expression are absent, and theinability of these patients to smile oftenleads to the mistaken impression that theyare dull and disinterested. Speech difficul-ties are complex and multifaceted, andfacial paralysis often leads to bilabialincompetence, which causes the charac-teristic speech pattern of flaccid dysarthriaconsisting of substitution, distortion oromission of the bilabial phonemes/p/,/b/and/m/and the alveolar phonemes/t/,/d/
ons. Published by Elsevier Ltd. All rights reserved.

Facial animation in patients with Moebius and Moebius-like syndromes 1067
Table 1. Patient classification.
n %
Moebius 19 39.6Moebius incomplete 8 16.7Moebius-like 21 43.7
Total 48 100
Table 2. Associated findings in patients withMoebius syndrome.
n
Poland syndrome 2GERD 2Cleft palate 3Syndactyly 2Bifid uvula 1Clubfeet 3Micrognathia 3Testicle anomalies 2Pituitary dysfunction 1Angel wing 1Mental retardation 2Persistent ductus arteriosus 1Hearing reduction 1Epicanthic fold 2
and/n/1,4,17,19. Paralysis of the lower faceoften causes problems with eating anddrinking, including pocketing of food inthe cheek, dribbling and severe drool-ing1,6,12. Other relevant clinical findingsare incomplete eye closure and convergentstrabismus. In addition to the abducensand facial nerves, the hypoglossal nerveis the most commonly involved cranialnerve, being affected in 25% of cases1,6.This manifests with further problems ofarticulation, primarily with vowels. Velo-pharyngeal incompetence is present inabout 11% of patients because of glosso-pharyngeal nerve palsy, which results in ahypernasal voice, glottal substitutions andincreased nasal air emission6. Mental dis-ability is overdiagnosed and is only pre-sent in 14% of patients6. This mistake isoften due to the frequent inability of peo-ple to understand what these patients aresaying or feeling. When these patientsbegin school, they are often teased byother children, which can cause them tobecome withdrawn and reluctant to speak,despite normal intelligence. The inabilityto show happiness, sadness or anger fre-quently results in severe introversion and areclusive personality with low self-esteem17. Impairments of the II, V, Xand XI cranial nerves have also beenobserved in rare instances1,6,17,20.
Patients with Moebius syndrome havebeen associated with additional deformi-ties that include limb malformation (club-feet and agenesis, rudimentary fingers ortoes and syndactyly or brachydactyly),malformations of the orofacial structures(bifid uvula, micrognathia, cleft palate,small palpebral fissures, epicanthic folds,ocular hypertelorism, microstomia, exter-nal ear deformity with occasional hearingloss and airway problems with aspiration),musculoskeletal malformations (absenceof the sternal head of the pectoralis majormuscle, rib defects and arthrogryposis;cases with dextrocardia have beendescribed) and dysfunction of the cere-brum (mental retardation and epi-lepsy)13,17. Moebius syndrome may alsobe associated with Poland syndrome, Klip-pel–Feil anomaly, Kallmann syndromeand Hanhart syndrome17.
The restoration of even a small degreeof volitional facial movement can berewarding in terms of verbal and nonver-bal communication. In this study, theauthors report on patients with Moebiusand Moebius-like syndromes seen andtreated surgically from 2003 to September2007. The authors evaluate the effective-ness of gracilis transplant to restore facialmovement and indications and results inthe use of the controlateral facial nerve or
of the masseter motor nerve in providingadequate innervation to the muscle trans-fer. The complications and the outcomesof the different techniques, focusing onfunctional and aesthetic issues such as oralcompetence, speech and the degree ofmovement and its impact on thesepatients, is analysed.
Materials and methods
The authors reviewed the records of 48patients with Moebius and Moebius-likesyndromes seen between 2003 and Sep-tember 2007. They comprised 23 malesand 25 females with a mean age, when firstseen, of 13.9 years (range 1–48 years). 27patients had bilateral Moebius syndrome,a monolateral form was present in 21patients with involvement of the right sidein 8 and the left side in 13. The patientswere classified (Table 1), following theclassification proposed by TERZIS etal.16,17,23: Moebius (complete bilateralfacial and abducens nerve paralysis);Moebius incomplete (clinical picture ofMoebius with the exception that someresidual motor function was noted onone side of the face); Moebius-like (uni-lateral facial paralysis, but additional cra-nial nerve palsies present).
In those with the Moebius incompleteform, some facial movements were evi-dent, which were always located in thelower face with platysmal activity ordepressor anguli oris activity. The abdu-cens nerve was involved in 70% of thepatients. In 13 patients, additional cranialnerves were involved, of which the hypo-glossal nerve was impaired in 25% and themotor branches of the fifth cranial nerve in4%.
A standardised neurological and logo-paedic examination was performed in allcases. Facial expression, oral motor func-tion and speech were evaluated clinically,and most patients underwent electromyo-graphic examinations during their firstvisit. Special attention was directedtoward the identification of possible motordonor nerves. Examination of the facialnerve included needle electromyographyof the facial musculature, including theupper, middle and lower facial territories.The temporalis and masseter muscles were
tested clinically. All patients were video-taped and photographed with particularattention to facial expression, oral motorfunction and speech.
The logopaedic evaluation showedalterations of speech patterns with articu-lation difficulties and substitution or dis-tortion of the bilabial phonemes/p/,/b/and/m/in 40% of the patients. Speech wasseverely altered in 10%. The associatedfindings are shown in Table 2.
Patients satisfying the following criteriawere excluded from ‘smile surgery’: ageless than 6 years; low collaboration due tomental retardation; good functional repairof the residual motor units; anomalies inwalking; absence of a collaboratingfamily.
Twenty patients underwent microsurgi-cal reconstruction to re-animate theimpaired sides of the face. A segment ofthe gracilis muscle was transplanted in allcases. The facial artery and vein were usedas recipient vessels in most of the proce-dures. In one patient, the facial vein wasnot found so the transverse facial vein wasused. Ten patients underwent a bilateralfree-muscle transplantation, with a total of30 gracilis free flaps. The contralateralfacial nerve was used as a motor donornerve in 7 procedures, the motor nerve tothe masseter muscle in 13 patients, 10 withbilateral and 3 with monolateral facialparalysis.
Cross-facial nerve graft
On the normal side through a preauricularincision, the branches of the facial nerveare identified as they exit the anteriorportion of the parotid fascia. With theaid of a nerve stimulator, a map of themuscles they innervate can be made, iden-tifying the buccal and zygomaticbranches. Segments of these branchescan be sacrificed as their activity is dupli-

1068 Bianchi et al.[(Fig._1)TD$FIG]
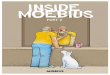
Fig. 1. Sural nerve graft tunnelled across the face with the aid of nasal vestibule incisions.[(Fig._2)TD$FIG]
Fig. 2. Taking off the gracilis muscle. Only a part is used, usually the anterior third.
Fig. 3. Muscle position in the subcutaneous pocket with venous (a) and arterious (b) repair;design of the site of anastomosis with the masseteric nerve (c).
cated. Three to five fascicles are selectedfor division and routed into a sural nervegraft, which is tunnelled across the facewith the aid of nasal vestibule incisions(Fig. 1). On the involved side, the nerve isplaced high on the maxilla and zygoma toease the dissection of this area at the timeof muscle transplantation and to keep thenerve graft from being damaged. Theregeneration of the graft can be followedby Tinel’s sign. After 9–12 months, suffi-cient neural regeneration has occurred inthe graft, and the nerve is capable ofinnervating a muscle transplant. Beforethe second surgical stage, a piece of thepreviously placed cross-facial nerve graftis taken under local anaesthesia and stu-died histologically. This allows better eva-luation of neural regeneration andselection of the best fascicles of the graftto reinnervate the transplant.
Microvascular muscle transfer
The procedure begins with two teamsoperating simultaneously to elevate themuscle and prepare the face. The ispilat-eral gracilis is usually used for transfer.The gracilis is approached through a short
medial thigh incision, posterior to the linejoining the adductor tubercle to the medialcondyle. The vascular pedicle is identifiedon the anterior border of the gracilis at thejunction of the upper-quarter and lower[(Fig._3)TD$FIG]
three-quarters. The nerve to the gracilisfrom the anterior branch of the obturatornerve is traced to the obturator foramen.Only a segment of the muscle is needed;the use of the entire muscle leads to excessbulk. Approximately one-third to half ofthe muscle is needed to produce the appro-priate amount of movement and to avoidexcess bulk. The anterior third of themuscle is usually selected, and the fasciclethat innervates this segment is identifiedand labelled (Fig. 2).
Facial dissection is performed simulta-neously while harvesting the gracilis. Thefacial incision is begun in the scalp nearthe upper pole of the ear, courses down-ward through the preauricular area, andthen, after a small posterior curve, coursesanteriorly in the neck with submandibularextension. The cheek flap is elevatedbelow the fat but above the parotid fascia.The plane of the dissection is carriedanteriorly to the anterior border of themasseter muscle. Superiorly, the dissec-tion extends up onto the body of thezygoma and the temple. The facial vesselsare identified at the level of the anteriorborder of the masseter. Once the vesselsare identified, the dissection continuesanteriorly just above the vessels to thecommissure and upper lip. Three to fivesutures are placed for secure anchorageand careful positioning of the muscle. Thefirst suture is placed in the oral commis-sure, the second is placed in the lower lip,and the third to fifth sutures are placed inthe upper lip. They are positioned so thatthey do not produce eversion or inversion.With traction, they should produce a naso-labial crease that looks as natural as pos-

Facial animation in patients with Moebius and Moebius-like syndromes 1069
Table 3. Clinical results.
Parameters
%
1. Excellent 2. Good 3. Fair 4. Poor
Symmetry at rest 60.0 40.0 0 01. No asymmetry at rest2. Mild asymmetry of oral commissure3. Facial asymmetry of commissures but midline in place4. Marked asymmetry
Symmetry smiling 53.3 33.3 6.7 6.71. No asymmetry2. Minimal asymmetry3. Asymmetry of commissure4. Marked asymmetry
Muscle action 60 26.6 6.7 6.71. Strong contraction2. Good muscle contraction3. Minimal visible muscle contraction4. No muscle contraction
Muscle bulk 53.3 46.7 0 01. No increase in bulk2. Slight increase in bulk3. Moderate increase in bulk4. Marked increase in bulk
Independent action 46.7 33.3 15.3 6.71. Good independent motion of affected side2. Strong contraction requires some movement of normal side3. Partial contraction of muscle requires marked contraction of normal side4. No muscle contraction
Commissure elevation 60 26.6 6.7 6.71. Normal or nearly normal2. Reasonable motion, not level with normal side3. Flicker of movement at commissure4. No movement of commissure
Mouth closure 73.3 6.7 15.3 6.71. Near normal2. Close mouth; asymmetry3. Incomplete closure4. Oral incontinence
Involuntary movement 60 26.6 6.7 6.71. No noticeable2. Minimal, only with strong contraction of other side3. Some involuntary movement of muscle4. Dyskinesias or mass movements of face
Overall final results 60 26.6 6.7 6.7
sible. When the motor nerve to the mass-eter is selected to reinnervate the muscletransplant, it can be identified on theundersurface of the masseter muscle. Itis usually found coursing vertically down-ward at the posterior margin of the musclejust below the zygomatic arch. Occasion-ally it may be seen coursing obliquelydownward and anteriorly or even trans-versely parallel to the arch. A nerve sti-mulator is helpful in identifying the motornerve to the masseter. Once the nerve isidentified, it is cleared of its fibrous con-nections and traced inferiorly, superfi-cially and anteriorly into the muscle.
The gracilis muscle is transferred to theface with the neurovascular pedicle on the
deep surface, enabling subsequent debulk-ing if necessary. The distal end of themuscle is fixed to the lips and oral com-missure through the previously positionedsutures. Anastomoses are carried outbetween the facial vessels and the arteryand the larger of the paired venae comi-tantes of the gracilis. In 20–25% ofpatients, the facial vein cannot be found;in these cases, the transverse facial vein isisolated. Once vascularisation is ensured,a fasicular nerve repair unites the recipientnerve in the face to the selected fascicle ofthe motor nerve in the gracilis (Fig. 3).
After the neurovascular repairs, themuscle origin is secure. It is sutured witha slight degree of tension at the corner of
the mouth and anchored to the temporalfascia and preauricular fascia. Tension atthe insertion may be relieved by a pre-fabricated hook. Reinnervation of themuscle usually appears 3–6 monthspost-transfer.
Study design
To evaluate the results of the techniquedescribed, the authors only consideredpatients with a minimum follow-up of12 months. Through the study of the clin-ical and surgical reports they reviewed thesurgical procedure with attention to: char-acteristics of the flap, fat removed from thecheek, flap survival, early and late com-

1070 Bianchi et al.[(Fig._4)TD$FIG]
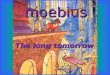
Fig. 4. Nine-year-old female patient with complete Moebius syndrome (a). The clinicalexamination revealed the impairment of the VI cranial nerve bilaterally. In October 2006she underwent transplant of the gracilis muscle on the left side and on June 2007 transplant of thegracilis muscle on the right side. During both the operations 6 g of fat were removed from thecheeks. Postoperative appearance while at rest (b) and while smiling (c).
[(Fig._5)TD$FIG]
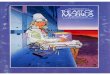
Fig. 5. Twenty-year-old male patient with a Moebius incomplete form. Some facial movementswere observed, which were located in the lower face bilaterally with depressor anguli orisactivity. Clinical examination revealed an impairment of the VI cranial nerve bilaterally and ofthe XII nerve on the left side. Preoperative view at rest (a) and smiling (b). The reconstructionwas achieved by performing two free microneurovascular transfers of gracilis muscle flaps to theright and left cheeks in July 2004 and August 2005, respectively. During both the operations, 2 gof fat were removed from the cheeks. Postoperative appearance while smiling (c) and withindependent bilateral contractions (d and e).
plications and time of reinnervation. Thefunctional and aesthetic results were ana-lysed using patient response, clinicalexamination and preoperative and post-operative videotaping of patients filmedat rest and performing several standardfacial movements to show muscle action,spontaneity, independence and fine facialmovements during speech and smile.
A speech therapist evaluated the speechchanges and the results on the impairedphonemes. The degree of deformity andthe effectiveness of surgery was identifiedby comparing the paralyzed side with thenormal side or the two treated sides inbilateral paralysis.
The smile was evaluated from the func-tional and aesthetic point of view using theevaluation criteria proposed by O’BRIEN
et al.13: symmetry at rest and smiling,muscle action and bulk, independentaction, commissure elevation, mouth clo-sure and presence of involuntary move-ments.
Dynamic (smile movement) measure-ments were performed on each side eval-uating the commissure movements. Asreported by MANKTELOW et al.12 the com-missure movement is considered the dis-tance moved by the commissure from therest position to a maximum smile as mea-sured in the plane of movement of thispoint.
Results
In this series, all free-muscle transplanta-tions survived the transfer, and no flap waslost. The segment of the muscle trans-planted weighed an average of 29 g, witha range of 20–44 g, and had an averagelength of 11.8 cm. During the operation,all patients had fat removed from thecheek area. One seroma was seen at theinner thigh after the gracilis muscle har-vest, which was treated by aspiration andpressure wrapping, and one patient devel-oped a facial abscess that was drained.Three patients developed hypertrophicscars at the site of the neck incision.The mean time for the reinnervation ofthe gracilis muscle was 3.5 months (3–5months). Only in one patient the musclewas well vascularised but did not showsigns of reinnervation despite a new opera-tion to revise the nervous anastomosis. Inone case dyskinesias was observed andone patient required a new surgical opera-tion to improve the muscle position andthe smile direction.
Through direct questioning regardingfunctional problems, all patients with pre-operative difficulties regarding oral com-petence reported a significantimprovement with no spontaneous drool-

Facial animation in patients with Moebius and Moebius-like syndromes 1071
Fig. 6. Twelve-year-old female patient with a Moebius-like form on the left side. Preoperativeappearance at rest (a) and while attempting to smile (b). In November 2005 a microsurgicalreconstruction with the gracilis muscle was performed. The innervation of the muscle transferwas provided by the ipsilateral motor nerve to the masseter muscle. Postoperative appearance atrest (c) and while smiling (d).
ing and with adequate capability to controloral fluid. The seven patients with preo-perative abnormalities in speech had animprovement in articulation and in pro-nunciation of bilabial phonemes reportedby the speech therapist.
Based on the evaluation criteria pre-viously proposed by O’BRIEN et al.13,the results shown in Table 3 wereobtained. Facial symmetry at rest wasexcellent or good in all patients, and87% maintained good symmetry whilstsmiling, although one patient did not haveany muscle movement. Excellent–goodelevation of the commissure was observedin 87% of patients, and the ability to closethe mouth was fair–poor in 20% ofpatients due either to drooping of thelower lip or the presence of micrognathia.Involuntary movements and dyskinesiaswere observed in two patients. The overallfinal results were excellent–good in 87%of patients and fair–poor in 15%. In all,80% of the subjects reported improvementin self-esteem and stated that they wouldundergo the surgery again.
The mean commissural movement mea-sured on the treated sides was 14 mm(range 11–20 mm): 16 mm when the mas-seteric nerve was used and 13 mm inpatients treated with a cross facial nervegraft. The mean difference between thetreated and the healthy side was 3.3 mm inthe masseteric nerve group and – 4.2 mmin the cross facial nerve graft group. Inpatients treated bilaterally, the mean dif-ference between the two sides was 2.5 mm(range 2–3 mm).
Four patients with a Moebius syndromeform treated with facial re-animationthrough a reinnervated gracilis musclefree-flap are presented in Figs. 4–7.
Discussion
The lack of facial animation in patientswith Moebius syndrome poses a majorbarrier to interpersonal communicationand creates severe aesthetic and functionalproblems. Several procedures to restorefacial function have been advocated:neural reconstructions with accessory tofacial nerve transfer, hypoglossal to facialnerve crossover or local muscle transfer17.None of these approaches has producedsatisfactory functional and aestheticresults. Microneurovascular transfer of afree-muscle transplant is the procedure ofchoice for facial paralysis, and the benefitsof using free-functioning muscle trans-plantation for facial paralysis are numer-ous9,15,17,18. Without the restrictions of thepedicle, the muscle can be placed pre-cisely in the desired location and direction
with improved outcomes23. Greater activeexcursion of the oral commissure can beobtained, and the muscle can be sculptedto the desired size and shape, avoiding theearlier drawbacks of excess bulk21,23. Thegracilis muscle represents the first choicefor facial animation, having the advan-tages of easy access, dispensability andappropriate vasculature for free trans-fer9,13 and the authors’ experience con-firms these qualities.
Despite the advances made over the lastfew years with this surgical approach,problems associated with orientation, bulkand excursion remain22,23. It is difficult toobtain accurate symmetry of movementand consistently produce a nasolabialcrease because of the imprecise natureof the muscle excursion, growth and rein-nervation. This can be overcome through acareful preoperative study of the patient,precise selection of the motor nerve, goodpositioning of the muscle and continuouspostoperative smile and speech train-ing22,23.[(Fig._6)TD$FIG]
Preoperative planning is important, anddetailed assessment of the location anddirection of desired movement should bemade22. Before the free-muscle transplant,the authors usually draw lines on thepatient corresponding to the nasolabialcrease and to the vector of the smile fromthe oral commissure toward the tragus.These lines direct the positioning sutureson the oral commissure and lips and aid inorienting the gracilis muscle. With trac-tion, the sutures should produce a nasola-bial crease that looks as natural aspossible. It is important to ensure thatthe direction of contracture of the muscleproduces movement that will simulate anormal smile, or in monolateral forms, thecontralateral side. Lack of accuracy inmuscle positioning will lead to asymme-trical movement, and the most commonfault is placing the muscle too transver-sely.
Excessive bulk at the site of the trans-plant should be avoided. According toZUKER et al.23 during dissection the

1072 Bianchi et al.[(Fig._7)TD$FIG]
Fig. 7. Thirteen-year-old female patient with a Moebius-like form on the left side. Preoperativeappearance at rest (a) and while attempting to smile (b). Clinical examination revealedimpairment of the XII nerve ipsilaterally. The reconstruction was achieved with a cross-facialnerve graft from the right facial nerve in June 2003, and subsequently, a gracilis muscletransplantation in February 2004. Postoperative appearance at rest (c) and while smiling (d).
authors removed 2–6 g of fat from thesubcutaneous tissue of the cheeks andBichat’s fat-pad. They used approximatelyone-third of the width of the normal gra-cilis, and fixed the origin of the muscle onthe inferior surface of the zygomatic archand zygoma, thus avoiding the problem ofmuscle protuberance. If the muscle originis placed on the superficial aspect of thezygomatic arch and zygoma, excess bulkwill be apparent. In some patients, theauthors also spread the proximal end ofthe muscle before anchoring it to thetemporal and preauricular fascia.
The selection of a motor nerve is criticalto the success of the procedure. Sufficientinnervation must be present to power themuscle, and this innervation must be spe-cific to the desired activity to achieve spon-taneity, synchronicity and symmetry. Thecontralateral seventh nerve, by means of across-facial nerve graft, provides the pre-ferred innervation for a muscle transfer inunilateral facial paralysis reconstruc-tion2,8,10,12,18,22,23. When the VII nerve isnot adequate in a person who has a verypowerful smile on their normal side or inpatients with bilateral forms, the authors
used the motor nerve to the masseter mus-cle. As in earlier reports, they noted that inthe cross-facial nerve graft group, theextent of oral commissure movement onthe side that was operated on was much lessthan that of the masseteric group2,12. Thecommissure movements measured weresimilar to those reported by BAE
2. Thecross-facial nerve graft procedure providesa spontaneous movement that cannot beprovided by the motor nerve to the massetermuscle2,10. In children, this spontaneity iscrucial in producing a normal appearingsmile. Nevertheless, the excursion pro-duced by the motor nerve to the masseteris in the normal range and certainly superiorto that provided by a cross-facial graft inputfrom the opposite side2,10,23. Although itdoes not provide true spontaneity of activ-ity, these children can achieve a goodappearance of a smile. In the authors’experience, as in other studies,11,12,21 mostof these patients are able to develop facialmovement independent of jaw motion andno longer have to think about moving theirface whilst laughing.
To achieve a spontaneous and symme-trical smile, postoperative smile training
by a speech–language pathologist usingmirror exercises and biofeedback playsan important role. When reinnervationof the muscle appears 3–6 months post-transfer, an active exercise programmemust be started, so that progress instrength, excursion and most importantly,symmetry, can be achieved. The age of thepatient when undergoing surgery did notinfluence the results from an aesthetic orfunctional point of view. In adults, rein-nervation takes longer (5–6 months) thanin children (3.5 months).
The degree of patient satisfaction andthe functional results in terms of drooling,drinking and speech were similar to thosereported by ZUKER et al.21–23.
Competing interests
None declared
Funding
None.
Ethical approval
Not required.
References
1. Abramson DL, Cohen Jr MM, Mulli-
ken JB. Mobius syndrome: classificationand grading system. Plast Reconstr Surg1998: 102: 961–967.
2. Bae YC, Zuker RM, Manktelow RT,Wade S. A comparison of commissureexcursion following gracilis muscletransplantation for facial paralysis usinga cross-face nerve graft versus the motornerve to the masseter nerve. PlastReconstr Surg 2006: 117: 2407–2413.
3. Bianchi B, Copelli C, Ferrari S, Ferri
A, Sesenna E. Facial animation in chil-dren with Moebius and Moebius-like syn-dromes. J Pediatr Surg 2009: 44: 2236–2242.
4. Cattaneo L, Chierici E, Bianchi B,Sesenna E, Pavesi G. The localization offacial motor impairment in sporadicMobius syndrome. Neurology 2006: 66:1907–1912.
5. Chester CH, Zuker RM. Complexitiesof speech in the Mobius syndromepatient. Plast Surg 1992: II: 241–243.
6. Goldberg C, DeLorie R, Zuker RM,Manktelow RT. The effects of gracilismuscle transplantation on speech in chil-dren with Moebius syndrome. J CraniofacSurg 2003: 14: 687–690.
7. Verzijl HTFM, Padberg GW, Zwarts
MJ. The spectrum of Mobius syndrome:an electrophysiological study. Brain2005: 128: 1728–1736.

Facial animation in patients with Moebius and Moebius-like syndromes 1073
8. Hoffman WY. Reanimation of the paral-yzed face. Otolaryngol Clin North Am1992: 25: 649–667.
9. Johnson PJ, Bajaj-Luthra A, Llull
R, Johnson PC. Quantitative facialmotion analysis after functional free mus-cle reanimation procedures. PlastReconstr Surg 1997: 100: 1710–1719.
10. Lee EI, Hurvitz KA, Evans GR, Wirth
GA. Cross-facial nerve graft: past andpresent. J Plast Reconstr Aesthet Surg2008: 61: 250–256.
11. Lifchez SD, Matloub HS, Gosain
AK. Cortical adaptation to restorationof smiling after free muscle transferinnervated by the nerve to the masseter.Plast Reconstr Surg 2005: 115: 1472–1479.
12. Manktelow RT, Tomat LR, Zuker
RM, Chang M. Smile reconstruction inadults with free muscle transfer inner-vated by the masseter motor nerve: effec-tiveness and cerebral adaptation. PlastReconstr Surg 2006: 118: 885–899.
13. O’Brien BM, Pederson WC, Khazan-
chi RK, Morrison WA, MacLeod AM,Kumar V. Results of management of
facial palsy with microvascular free-mus-cle transfer. Plast Reconstr Surg 1990: 86:12–22.
14. Sjogreen L, Andersson-Norinder J,Jacobsson C. Development of speech,feeding, eating, and facial expression inMobius sequence. Int J Pediatr Otorhino-laryngol 2001: 60: 197–204.
15. Terzis JK, Noah ME. Analysis of 100cases of free-muscle transplantation forfacial paralysis. Plast Reconstr Surg1997: 99: 1905–1921.
16. Terzis JK, Noah EM. Mobius andMobius-like patients: etiology, diagnosis,and treatment options. Clin Plast Surg2002: 29: 497–514.
17. Terzis JK, Noah EM. Dynamic restora-tion in Mobius and Mobius-like patients.Plast Reconstr Surg 2003: 111: 40–55.
18. Ueda K, Harii K, Asato H, Yamada A.Neurovascular free muscle transfer com-bined with cross-face nerve grafting forthe treatment of facial paralysis in chil-dren. Plast Reconstr Surg 1998: 101:1765–1773.
19. Verzijl HT, van der Zwaag B, Cruys-
berg JR, Padberg GW. Mobius syn-
drome redefined: a syndrome ofrhombencephalic maldevelopment. Neu-rology 2003: 61: 327–333.
20. Westin LM, Zuker R. A new classifica-tion system for facial paralysis in theclinical setting. J Craniofac Surg 2003:14: 672–679 [Review].
21. Zuker RM, Manktelow RT. A smilefor the Mobius’ syndrome patient. AnnPlast Surg 1989: 22: 188–194.
22. Zuker RM. Facial paralysis in children.Clin Plast Surg 1990: 17: 95–99.
23. Zuker RM, Goldberg CS, Manktelow
RT. Facial animation in children withMobius syndrome after segmental graci-lis muscle transplant. Plast Reconstr Surg2000: 106: 1–8.
Address:C. CopelliSezione di Chirurgia Maxillo-FaccialeOspedale MaggioreVia Gramsci14-43100 Parma (Pr)ItalyTel.: +39 0521 703107E-mail: [email protected]