Embed Size (px)
Citation preview

F. Schweiger MD
Moncton, May 27, 2007

Celiac sprue - DefinitonCeliac sprue - Definiton
Intolerance to gluten proteins from wheat Intolerance to gluten proteins from wheat and to related proteins from barley or ryeand to related proteins from barley or rye
Presents with Presents with characteristiccharacteristic histopathological changes of the jejeunal histopathological changes of the jejeunal mucosamucosa
Consequences: from asymptomatic to Consequences: from asymptomatic to global malabsorption and an increased global malabsorption and an increased risk to develop GI malignanciesrisk to develop GI malignancies
Manifestation by genetic, Manifestation by genetic, environmental,and immunological factorsenvironmental,and immunological factors

Mortality of celiac sprueMortality of celiac sprue
Before introduction of gluten-free diet:Before introduction of gluten-free diet: 544 children 12 % Hardwick 1939544 children 12 % Hardwick 1939 (malabsorption and infection)(malabsorption and infection)
After introduction of gluten-free diet After introduction of gluten-free diet (Dickie 1951):(Dickie 1951):
485 children 0.4 % Sheldon 1969 485 children 0.4 % Sheldon 1969 653 adults 2 x increased Logan et al 1989 653 adults 2 x increased Logan et al 1989 335 adults on GFD no increase Collin et al 1994 335 adults on GFD no increase Collin et al 1994

Prevalence of Celiac DiseasePrevalence of Celiac Disease
USA / Canada 1 in 100USA / Canada 1 in 100Irish 1 in 152Irish 1 in 152Italians with “dyspepsia” 1 in 103Italians with “dyspepsia” 1 in 103Swedish blood donors 1 in 256Swedish blood donors 1 in 256Brazilians 1 in 680Brazilians 1 in 680Baltimore (USA) 1 in 300Baltimore (USA) 1 in 300
Rare in Afro-Caribbean, Chinese, JapaneseRare in Afro-Caribbean, Chinese, Japanese Mild female preponderance (2:1 at most)Mild female preponderance (2:1 at most)

Triggers of celiac diseaseTriggers of celiac disease
Infectious (viral
bacterial)
Diatetic
(gluten) Genetic
HLA-DQ2
AutoimmunityImmune-maturation
Th2 Th1
Sprue

Family Family GramineaeGramineae
Subfamily Subfamily Festucoideae Panicoideae Festucoideae Panicoideae
Tribe Tribe Triticeae Aveneae Oryzeae Andropogoneae PaniceaeTriticeae Aveneae Oryzeae Andropogoneae Paniceae
Subtribe Subtribe Triticineae Hordeinae Tripsacinae AnthrxoninaeTriticineae Hordeinae Tripsacinae Anthrxoninae
Genus Genus Triticum Secale Hordeum Avena Oryza Zea Sorghum PennisetumTriticum Secale Hordeum Avena Oryza Zea Sorghum Pennisetum
Wheat Rye Barley Oats Rice Corn Sorghum MilletWheat Rye Barley Oats Rice Corn Sorghum Millet
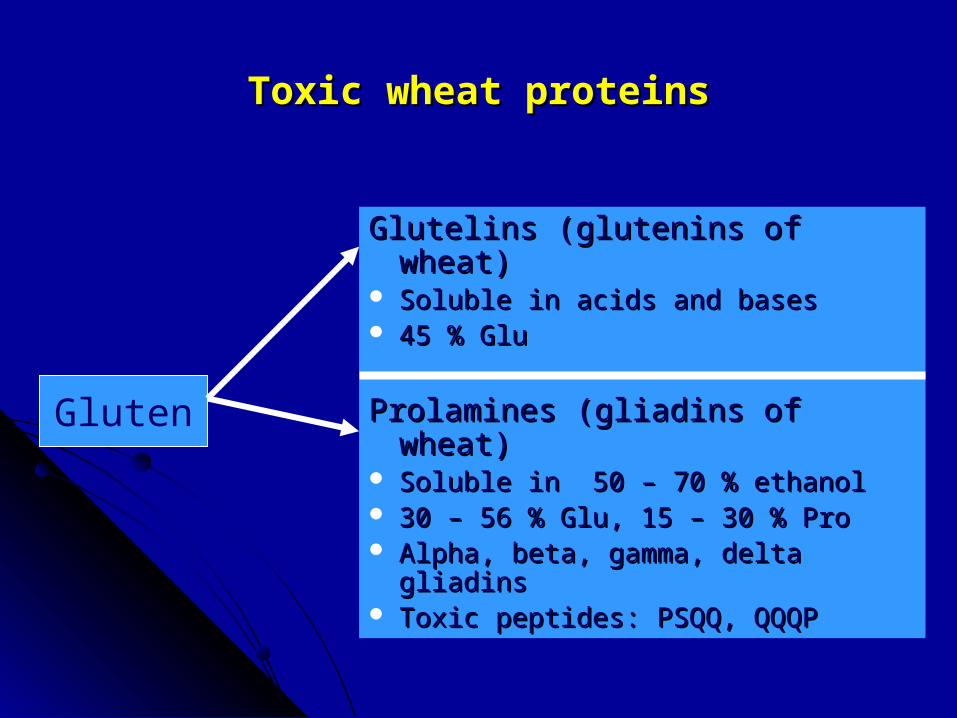
Toxic wheat proteinsToxic wheat proteins
Glutelins (glutenins of wheat)Glutelins (glutenins of wheat) Soluble in acids and basesSoluble in acids and bases 45 % Glu45 % Glu
Prolamines (gliadins of wheat)Prolamines (gliadins of wheat) Soluble in 50 – 70 % ethanolSoluble in 50 – 70 % ethanol 30 – 56 % Glu, 15 – 30 % Pro30 – 56 % Glu, 15 – 30 % Pro Alpha, beta, gamma, delta gliadinsAlpha, beta, gamma, delta gliadins Toxic peptides: PSQQ, QQQPToxic peptides: PSQQ, QQQP
Gluten

Environmental FactorsEnvironmental FactorsOATSOATS
Oats may be tolerated by patientsOats may be tolerated by patients
Oats contain less QQQPF (toxic fraction in wheat Oats contain less QQQPF (toxic fraction in wheat gliadin)gliadin)
Prolamines in oats have less glutamine and prolineProlamines in oats have less glutamine and proline
Tolerance to oats depends on the amount consumed Tolerance to oats depends on the amount consumed (less than 40 gm)(less than 40 gm)

Genetic factorsGenetic factors
Concordance in monozygotic twins : 75 %Concordance in monozygotic twins : 75 % Risk to first degree relatives : 2 – 15 % (10 %)Risk to first degree relatives : 2 – 15 % (10 %) Risk to 2Risk to 2ndnd degree relatives : 3 – 5 % degree relatives : 3 – 5 %

Familial clustering of celiac disease/dermatitis Familial clustering of celiac disease/dermatitis herpetiformisherpetiformis
1.degree relatives number sprue/DH prevalence1.degree relatives number sprue/DH prevalence
Parents 521 22 4.2 %Parents 521 22 4.2 %Sisters/brothers 368 51 13.8 %Sisters/brothers 368 51 13.8 %Offspring 54 7 12.9 %Offspring 54 7 12.9 %2.degree relatives 54 3 5.6 %2.degree relatives 54 3 5.6 %
Total 997 83 8.3 % Total 997 83 8.3 %

Relatives: Who and How to Screen ?Relatives: Who and How to Screen ?
Index case has proven celiac diseaseIndex case has proven celiac disease Relative is interested in being screenedRelative is interested in being screened Relative is willing to undergo diagnostic testingRelative is willing to undergo diagnostic testing Relative is willing to undergo treatmentRelative is willing to undergo treatment Relative will derive benefit from treatmentRelative will derive benefit from treatment If relative is symptomatic, approach is diagnostic not If relative is symptomatic, approach is diagnostic not
screeningscreening
S. Crowe, DDW 2007

Classical presentation of celiac diseaseClassical presentation of celiac disease1960-ies, Helsinki, Finland1960-ies, Helsinki, Finland
Number 53Number 53Age at initial symptoms (months) 7.7Age at initial symptoms (months) 7.7Duration of gluten ingestion (months) 4.3Duration of gluten ingestion (months) 4.3Age at admission (months) 10.2Age at admission (months) 10.2Diarrhea 87 %Diarrhea 87 %Vomiting 74 %Vomiting 74 %Growth retardation 98 %Growth retardation 98 %Weight below 2.5 percentile 70 %Weight below 2.5 percentile 70 %Distended abdomen 64 %Distended abdomen 64 %
Acta Ped Scand 1967

Celiac Disease in AdultsCeliac Disease in Adults
20 % over age 6020 % over age 60 Often mistaken for Irritable Bowel SyndromeOften mistaken for Irritable Bowel Syndrome 50 % do not have diarrhea50 % do not have diarrhea Iron deficiency anemia most common presentationIron deficiency anemia most common presentation Unmasking by gastric surgeryUnmasking by gastric surgery May present as recurrent “canker sores”May present as recurrent “canker sores” Significant fatty stools uncommonSignificant fatty stools uncommon Abdominal pain uncommonAbdominal pain uncommon

Atypical Presentations (1)Atypical Presentations (1)
Nonspecific Nonspecific Weight loss, lethargy, fatigueWeight loss, lethargy, fatigue Hematological Hematological bruising (Vitamin K), anemia bruising (Vitamin K), anemia (iron,folate ,B12) (iron,folate ,B12) hyposplenism (thrombocytosis)hyposplenism (thrombocytosis)
NeurologicalNeurological cerebellar ataxia, peripheral cerebellar ataxia, peripheral neuropathy,post/lateral columnneuropathy,post/lateral column abnormalities, neuromyopathies,abnormalities, neuromyopathies,
epilepsy (+/-cerebral calcifications)epilepsy (+/-cerebral calcifications) demyelinating CNS lesions demyelinating CNS lesions
Atypical Presentations (2)Atypical Presentations (2)
Musculoskeletal Musculoskeletal Osteoporosis, osteomalacia, #sOsteoporosis, osteomalacia, #s
osteoarthropathy,tetany,weaknessosteoarthropathy,tetany,weakness
dental enamel hypoplasia,dental enamel hypoplasia, GynecologicGynecologic primary or secondary amenorrhea primary or secondary amenorrhea
infertility, recurrent abortionsinfertility, recurrent abortions Dermatologic Dermatologic alopecia, follicular keratosisalopecia, follicular keratosis Psychiatric Psychiatric depression, psychosis, depression, psychosis,
schizophreniaschizophrenia

Atypical Presentations (3)Atypical Presentations (3)
Endocrine : Endocrine : pubertal delay, short stature,pubertal delay, short stature,
22ndnd hyperparathyroidism, infertility, hyperparathyroidism, infertility,
impotence, amenorrheaimpotence, amenorrhea

Dietary Response -? DiagnosticDietary Response -? Diagnostic
Placebo response in IBS up to 70 %Placebo response in IBS up to 70 % Gluten (increased prolamines) is hard to digestGluten (increased prolamines) is hard to digest GFD often eliminates other dietary factorsGFD often eliminates other dietary factors
Symptomatic response to GFD, especially a Symptomatic response to GFD, especially a transient response, does not imply the diagnosis transient response, does not imply the diagnosis of celiac diseaseof celiac disease

Laboratory testsLaboratory tests
Protein: Albumin, globulins, Liver testsProtein: Albumin, globulins, Liver tests
Carbs : glucose, Lactose-H breath test, (D-Xylose)Carbs : glucose, Lactose-H breath test, (D-Xylose)
Fats : (stool for fat), lipid profile, caroteneFats : (stool for fat), lipid profile, carotene
Minerals : Ca, Mg, P, Fe, ferritin,zincMinerals : Ca, Mg, P, Fe, ferritin,zinc
Vitamins : RBC folate, B12, Vit A, 25-OH Vitamin D, PTVitamins : RBC folate, B12, Vit A, 25-OH Vitamin D, PT

Serologic Tests for Celiac DiseaseSerologic Tests for Celiac Disease
Serologic Test Sensitivity Specificity PPV NPVSerologic Test Sensitivity Specificity PPV NPV
percentpercent
Anti-EMA (IgA) 85-98 97-100 99 93Anti-EMA (IgA) 85-98 97-100 99 93
IgA antigliadin 75-90 82-95 28-100 65-100IgA antigliadin 75-90 82-95 28-100 65-100
IgG antigliadin 69-85 73-90 20-95 41- 88IgG antigliadin 69-85 73-90 20-95 41- 88
tTg (IgA) 92-98 95-98tTg (IgA) 92-98 95-98

Epidemiology of Celiac DiseaseEpidemiology of Celiac Diseasethe sprue icebergthe sprue iceberg
Healthy individuals
Latent CD
Silent CD
Clinical CD
Normal
mucosa
Abnormal
mucosaEMA present
EMA present
Asymptomatic

The asymptomatic patientThe asymptomatic patient
Advantages of screening:Advantages of screening:
• Reduction in risk of enteropathic T-cell lymphomaReduction in risk of enteropathic T-cell lymphoma• Reversal of unrecognized nutritional deficiencesReversal of unrecognized nutritional deficiences• Resolution of mild or unrecognized symptomsResolution of mild or unrecognized symptoms• Avoidance of other autoimmune disordersAvoidance of other autoimmune disorders• Improvement of general well-beingImprovement of general well-being Disadvantages of screening:Disadvantages of screening:
• Lack of motivation to adhere to GFDLack of motivation to adhere to GFD• Adverse psychological effectsAdverse psychological effects
MMass screening currently not advocatedass screening currently not advocated


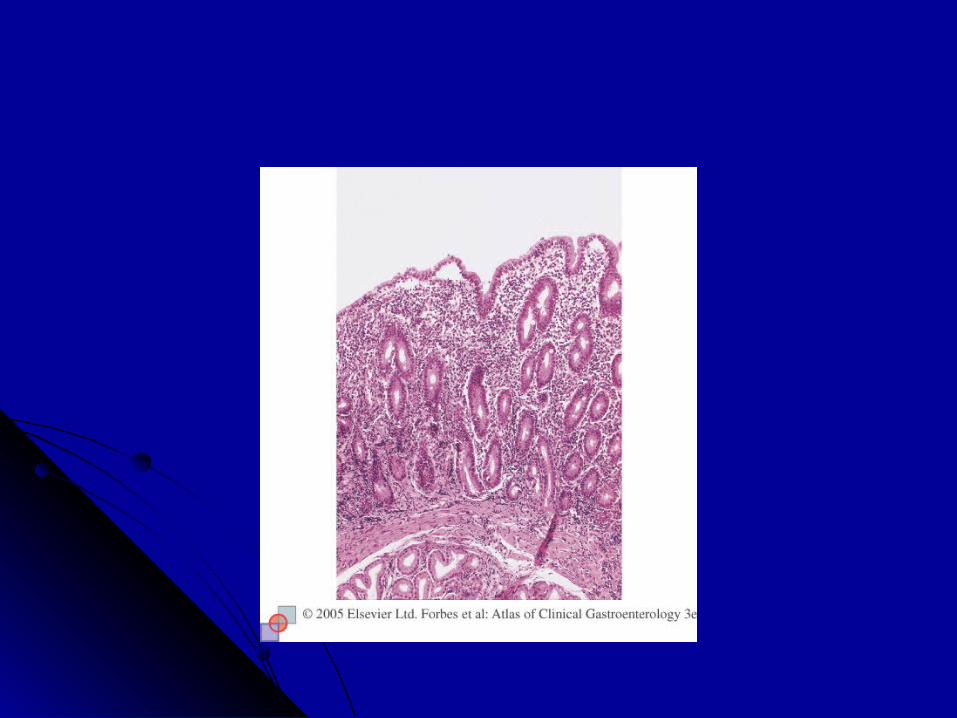
Pathology of celiac diseasePathology of celiac disease
Length of SB involvement correlates with clinical Length of SB involvement correlates with clinical severityseverity
GFD results in marked improvement beginning GFD results in marked improvement beginning distallydistally
Histology is not specific Histology is not specific



Causes of villous atrophyCauses of villous atrophy
Cow’s milk protein intolerance (children)Cow’s milk protein intolerance (children) Post-gastroenteritisPost-gastroenteritis GiardiasisGiardiasis Peptic duodenitis (including ZES)Peptic duodenitis (including ZES) Crohn’s diseaseCrohn’s disease Small intestinal bacterial overgrowthSmall intestinal bacterial overgrowth Eosinophilic enteritisEosinophilic enteritis Radiation or cytotoxic therapyRadiation or cytotoxic therapy Tropical sprueTropical sprue Severe malnutritionSevere malnutrition Diffuse small intestinal lymphomaDiffuse small intestinal lymphoma Graft versus host diseaseGraft versus host disease HypogammaglobulinemiaHypogammaglobulinemia Alpha chain diseaseAlpha chain disease

Prevalence of autoimmune disease in celiac diseasePrevalence of autoimmune disease in celiac disease
0
5
10
15
20
25
30
35
40
<2 2 to 4 4 to 12 12 to 20 > 20
age at diagnosis of celiac sprue (years)
Pre
vale
nce
(%
)

Celiac disease and associated disordersCeliac disease and associated disordersDefinite AssociationDefinite Association
Dermatitis herpetiformisDermatitis herpetiformis Insulin-dependent Diabetes Insulin-dependent Diabetes Thyroid diseaseThyroid disease IgA deficiencyIgA deficiency Epilepsy with cerebral calcificationsEpilepsy with cerebral calcifications Inflammatory bowel diseaseInflammatory bowel disease Microscopic colitidesMicroscopic colitides IgA mesangial nephropathyIgA mesangial nephropathy Chronic autoimmune hepatitisChronic autoimmune hepatitis Sclerosing cholangitisSclerosing cholangitis Primary biliary cirrhosisPrimary biliary cirrhosis Down syndrome (3-12%)Down syndrome (3-12%) Turner syndromeTurner syndrome
Rheumatoid arthritisRheumatoid arthritis SarcoidosisSarcoidosis Bird fancier’s lungBird fancier’s lung Fibrosing alveolitisFibrosing alveolitis Recurrent pericarditisRecurrent pericarditis Idiopathic pulmonary Idiopathic pulmonary
hemosiderosis hemosiderosis

Dermatitis herpetiformisDermatitis herpetiformis
Papulovesicular lesions of extensor surfaces, buttocks, Papulovesicular lesions of extensor surfaces, buttocks, trunk, neck and scalptrunk, neck and scalp
Intensely pruriticIntensely pruritic Early or middle adult life; M = FEarly or middle adult life; M = F 2/3 have patchy enteropathy; tends to be less severe2/3 have patchy enteropathy; tends to be less severe Less than 10 % have intestinal symptomsLess than 10 % have intestinal symptoms 10 – 40 fold increased risk of lymphoma10 – 40 fold increased risk of lymphoma


Dermatitis herpetiformisDermatitis herpetiformis
Frequency of Abs to tTG only about 75 %Frequency of Abs to tTG only about 75 % More than 80 % of pts with DH have sprueMore than 80 % of pts with DH have sprue 10 % of celiacs have DH10 % of celiacs have DH Tx: Dapsone 1 – 2 mg/kg (does not improve SB)Tx: Dapsone 1 – 2 mg/kg (does not improve SB) GFD allows most patients to reduce/stop DapsoneGFD allows most patients to reduce/stop Dapsone

Celiac disease and type 1 DM Celiac disease and type 1 DM
Patients (n) Pos (%)Patients (n) Pos (%)
Finland children (776) 2.4Finland children (776) 2.4Finland adults (195) 4.1Finland adults (195) 4.1Italy children (498) 3.2Italy children (498) 3.2Italy adults (383) 2.6Italy adults (383) 2.6Italy adults (639) 7.8Italy adults (639) 7.8Sweden children (436) 4.6Sweden children (436) 4.6Ireland adults (101) 4.9Ireland adults (101) 4.9UK adults (767) 2.0UK adults (767) 2.0Germ/Switz children (1032) 1.2Germ/Switz children (1032) 1.2Australia children (273) 1.8Australia children (273) 1.8USA children (211) 1.4USA children (211) 1.4

Celiac disease and Osteoporosis Celiac disease and Osteoporosis
Prevalence of CD is increased in osteoporosis (1.5-3%) Prevalence of CD is increased in osteoporosis (1.5-3%) Especially in premature osteoporosis/osteomalaciaEspecially in premature osteoporosis/osteomalacia
Newly diagnosed CD : spine 28 % & hip 15 %Newly diagnosed CD : spine 28 % & hip 15 %
Patients with asymptomatic CD have increased riskPatients with asymptomatic CD have increased risk
Postmenopausal females are at greatest riskPostmenopausal females are at greatest risk

Celiac disease and Osteoporosis Celiac disease and Osteoporosis
Vitamin D deficiency is common in CD Vitamin D deficiency is common in CD
Bone mineral density increases with GFD, especially in Bone mineral density increases with GFD, especially in the first year of treatmentthe first year of treatment
Axial bone mass increases more then appendicular BMDAxial bone mass increases more then appendicular BMD
Celiac disease and Osteoporosis Celiac disease and Osteoporosis
Adequate calcium and vitamin D intakeAdequate calcium and vitamin D intake Regular weight bearing exercisesRegular weight bearing exercises Smoking cessation; avoid alcoholSmoking cessation; avoid alcohol Correction of hypogonadismCorrection of hypogonadism

R epeat D EXA every 12 months
Treat with bisphosphonates
T < -2.5
R epeat D EXA every 12 months
Calcium / Vitam in D ***
-2.5< T < -1.0
R epeat D EXA evey 24 months
Lifestyle m easures alone ***
T > -1.0
Baseline DEXA at dignosis or initial assessm ent
Celiac Disease and OsteoporosisCeliac Disease and Osteoporosis
Celiac disease and associated conditionsCeliac disease and associated conditionsPossible associationPossible association
Congenital heart diseaseCongenital heart disease Lung cavitiesLung cavities Sjogren’s syndromeSjogren’s syndrome Systemic and cutaneous Systemic and cutaneous
vasculitisvasculitis SLESLE PolymyositisPolymyositis Schizophrenia Schizophrenia
Myasthenia gravisMyasthenia gravis Iridocyclitis or choroiditisIridocyclitis or choroiditis Cystic fibrosisCystic fibrosis MacroamylasemiaMacroamylasemia Addison’s diseaseAddison’s disease Autoimmune Autoimmune
thrombocytopenic purpurathrombocytopenic purpura Autoimmune hemolytic Autoimmune hemolytic
anemiaanemia

Celiac Disease and MalignanciesCeliac Disease and Malignancies
44/105 deaths during 13.5 years in 653 (untreated) patients from 44/105 deaths during 13.5 years in 653 (untreated) patients from Edinburgh, ScotlandEdinburgh, Scotland
RiskRisk All malignancies 3 xAll malignancies 3 xLymphoma 30 xLymphoma 30 xIntestinal carcinoma 3 xIntestinal carcinoma 3 xEsophageal carcinoma 8 xEsophageal carcinoma 8 x
Logan et al, Gastroenterology 1989

Cancer and Celiac DiseaseCancer and Celiac Disease
12, 000 celiac patients in Sweden over 30 years:12, 000 celiac patients in Sweden over 30 years:
6-fold increased risk of lymphoma (18% of all Ca)6-fold increased risk of lymphoma (18% of all Ca) Oropharyngeal Ca (SCC)Oropharyngeal Ca (SCC) Esophageal Ca (SCC)Esophageal Ca (SCC) Small bowel CaSmall bowel Ca Colon Ca - confined to subjects older than 60Colon Ca - confined to subjects older than 60 Primary liver CaPrimary liver Ca Reduced occurrence of breast CaReduced occurrence of breast Ca
Askling et al. Gastro 2002Askling et al. Gastro 2002

Celiac Disease and cancerCeliac Disease and cancer
Strict adherence to a GFD probably reduces the risk Strict adherence to a GFD probably reduces the risk of enteropathy-associated T cell lymphoma as well of enteropathy-associated T cell lymphoma as well as the other malignancies as the other malignancies
Treatment of Celiac DiseaseTreatment of Celiac Disease
Dietary counseling and strict avoidance of glutenDietary counseling and strict avoidance of gluten Initial avoidance of dairy products Initial avoidance of dairy products Replacements of micronutrients in case of deficienciesReplacements of micronutrients in case of deficiencies Corticosteroids/azathioprine for celiac crisis or refractory Corticosteroids/azathioprine for celiac crisis or refractory
spruesprue
Treatment of Celiac DiseaseTreatment of Celiac Disease
Non-compliance is an issue - eating out of homeNon-compliance is an issue - eating out of home - peer pressure for children- peer pressure for children - less acceptable taste- less acceptable taste - accidental ingestion of G.- accidental ingestion of G. - cost, availability, labelling- cost, availability, labelling
Use of oats, wheat starch controversialUse of oats, wheat starch controversial GFD reduces risk of malignancyGFD reduces risk of malignancy Unclear how much gluten if any is safeUnclear how much gluten if any is safe - new FDA guidelines up to 10 mg/day safe ? - new FDA guidelines up to 10 mg/day safe ?
S. Crowe, DDW 2007S. Crowe, DDW 2007

Response to TreatmentResponse to Treatment
Clinical improvement in 2 weeks in 70 %, by 6 weeks in Clinical improvement in 2 weeks in 70 %, by 6 weeks in mostmost
Serological improvement by 4 – 6 weeksSerological improvement by 4 – 6 weeks Histological improvement in up to 2 yearsHistological improvement in up to 2 years Gaining weight above ideal BMIGaining weight above ideal BMI ConstipationConstipation Falling off the diet and getting ill againFalling off the diet and getting ill again
S. Crowe, DDW 2007S. Crowe, DDW 2007
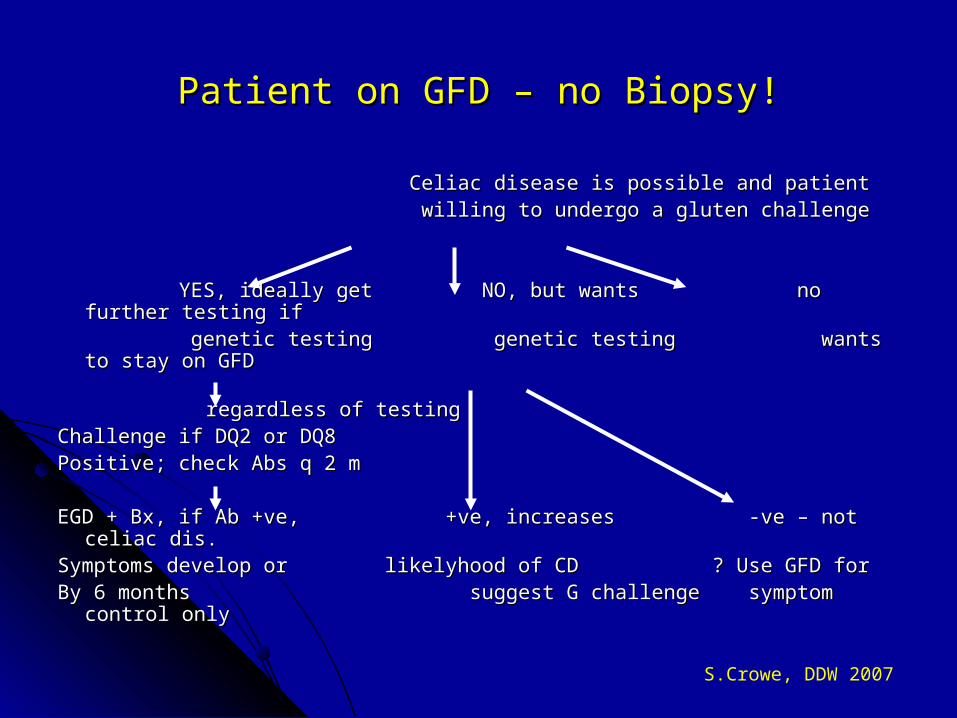
Patient on GFD – no Biopsy!Patient on GFD – no Biopsy!
Celiac disease is possible and patientCeliac disease is possible and patient willing to undergo a gluten challengewilling to undergo a gluten challenge
YES, ideally get NO, but wants no further testing ifYES, ideally get NO, but wants no further testing if genetic testing genetic testing wants to stay on GFDgenetic testing genetic testing wants to stay on GFD regardless of testingregardless of testingChallenge if DQ2 or DQ8Challenge if DQ2 or DQ8Positive; check Abs q 2 mPositive; check Abs q 2 m
EGD + Bx, if Ab +ve, +ve, increases -ve – not celiac dis.EGD + Bx, if Ab +ve, +ve, increases -ve – not celiac dis.Symptoms develop or likelyhood of CD ? Use GFD forSymptoms develop or likelyhood of CD ? Use GFD forBy 6 months suggest G challenge symptom control onlyBy 6 months suggest G challenge symptom control only
S.Crowe, DDW 2007

Gluten ChallengeGluten Challenge
Gradual increase of gluten in diet up to target (typically 4 Gradual increase of gluten in diet up to target (typically 4 slices of bread/day)slices of bread/day)
Check tTG at 4-6 weeks and at intervals thereafter until Check tTG at 4-6 weeks and at intervals thereafter until positivepositive
Biopsy if diarrhea develops and/or become seropositiveBiopsy if diarrhea develops and/or become seropositive Management if sero-negative at 3-6 months needs to be Management if sero-negative at 3-6 months needs to be
individualizedindividualized
S.Crowe, DDW 2007

Treatment of celiac diseaseTreatment of celiac disease
Histology may not recover completely despite clinical Histology may not recover completely despite clinical normalizationnormalization
Negativation of IgA anti-TTG after 4 – 6 months of a Negativation of IgA anti-TTG after 4 – 6 months of a strictly gluten-free diet (GFD)strictly gluten-free diet (GFD)
Diagnosis to be reconsidered when no clinical Diagnosis to be reconsidered when no clinical improvement is reached after 6 – 9 months of a GFDimprovement is reached after 6 – 9 months of a GFD
Risk of malignancy approaches baseline after 5 years of Risk of malignancy approaches baseline after 5 years of a GFDa GFD

Why a Gluten Free Diet ?Why a Gluten Free Diet ?
Benefits overall cancer riskBenefits overall cancer risk Improves unexplained infertilityImproves unexplained infertility Improves osteoporosisImproves osteoporosis Corrects iron deficiencyCorrects iron deficiency Improved QOL even for those detected by screeningImproved QOL even for those detected by screening
GFD is beneficial for preventing, reversing and/or GFD is beneficial for preventing, reversing and/or treating some complicationstreating some complications

SummarySummary
Celiac disease is not rare (1 in 100-300)Celiac disease is not rare (1 in 100-300) It can present in many waysIt can present in many ways iron deficiency anemia, depression, osteoporosis, abnormal liver tests, non-iron deficiency anemia, depression, osteoporosis, abnormal liver tests, non-
specific or IBS-like symptoms, dyspepsia, DH, recurrent miscarriages, specific or IBS-like symptoms, dyspepsia, DH, recurrent miscarriages, microscopic colitismicroscopic colitis
Associated with autoimmune diseasesAssociated with autoimmune diseases Screening with tTG IgA is bestScreening with tTG IgA is best Confirm diagnosis with duodenal biopsyConfirm diagnosis with duodenal biopsy Cornerstone of treatment is avoidance of glutenCornerstone of treatment is avoidance of gluten

?