Embed Size (px)
Citation preview

Ezra W CohenUniversity of California, San Diego
RTP ON DEMAND: Thyroid Cancer

Thyroid CancerNewly Detected 2015 (n = 62,450)
Cancer Facts & Figures 2015.
Papil-lary82%
Fol-licu-lar
10%
5%
Anaplastic1%
Medullary2%
Hürthle

Five- and 10-Year Cumulative Incidences of Death Among Patients with Thyroid Cancer
Yang L et al. J Clin Oncol 2013;31(4):468-74.
Characteristic Cumulative incidence of death resulting from thyroid cancer
5 years (%) 10 years (%) p-value*
All patients 1.9 3.0 —Age at diagnosis, years
<0.001 <45 0.3 0.5 45-64 1.9 3.5 65-74 6.8 10.3 ≥75 12.2 16.0Histologic subtype
<0.001
Papillary 1.3 2.2 Follicular 2.6 4.8 Medullary 9.3 9.3 Anaplastic 77.8 78.9 Other 27.4 29.3
* Gray's test

Five- and 10-Year Cumulative Incidences of Death Among Patients with Thyroid Cancer by Age
Yang L et al. J Clin Oncol 2013;31(4):468-74.
CharacteristicCumulative incidence of death resulting
from thyroid cancer
5 years (%) 10 years (%) p-value*
All patients 1.9 3.0 —
Age at diagnosis, years
<0.001
<45 0.3 0.5
45-64 1.9 3.5
65-74 6.8 10.3
≥75 12.2 16.0
Other 27.4 29.3 <0.001

Radioactive Iodine-Refractory Differentiated Thyroid Cancer: Molecular Pathways and Drug Targets
Adapted from Dadu R, Cabanillas ME. Minerva Endocrinol 2012;37(4):335-56.

Selected Agents in Thyroid Cancer and Some of Their Kinase Targets — Are These “Actionable”?
Colevas AD et al. Proc ASCO 2014;Discussant.
Agent FGFR VEGFR PDGFR BRAF CKIT FLT3 CMET TIE2 EGFR RET
Sorafenib X X X X X
Sunitinib X X X X X
Cabozantinib X X X X X X
Vandetanib X X X
Lenvatinib X X X X X
Lenalidomide X
Axitinib X X
Motesanib X X X X
Pazopanib X X X
Vemurafenib X

Agent ORR (RECIST) mPFS
Axitinib1,2 30%-35% 16.1-18.1 months
Lenvatinib3 50% 12.6 months
Motesanib4 14% 40 weeks
Pazopanib5 49% 11.7 months
Sorafenib6,7,8 15%-23% 16 months – not reached
Sunitinib9,10 18%-31% 12.8 months – not reached
VEGFRi in Thyroid Cancer — Phase II Trials
1 Cohen EE et al. J Clin Oncol 2008;26(29):4708-13; 2 Locati LD et al. Cancer 2014;120(17):2694-703; 3 Sherman SI et al. ASCO 2011;Abstract 5503; 4 Sherman SI et al. N Engl J Med 2008;359(1):31-42; 5 Bible KC et al. Lancet Oncol 2010;11(10):962-72; 6 Gupta-Abramson V et al. J Clin Oncol 2008;26(29):4714-9; 7 Kloos RT et al. J Clin Oncol 2009;27(10):1675-84; 8 Ahmed M et al. Eur J Endocrinol 2011;165(2):315-22; 9 Carr LL et al. Clin Cancer Res 2010;16(21):5260-8; 10 Cohen EE et al. WCTC 2011.

Cohen EE et al. J Clin Oncol 2008;26(29):4708-13.
Investigator-Assessed Response to Treatment in a Phase II Study of Axitinib
Response (n = 60) No. %
Complete response 0 0
Partial response 18 30
Stable disease 23 38
Progressive disease 4 7
Indeterminate* 8 13
Missing 7 12
Objective response rate 18 30
95% CI 18.9 to 43.2
CI = confidence interval
* Includes 8 patients who did not meet any response criteria and 7 patients without postbaseline scans

Efficacy of Pazopanib in a Phase II Study in Progressive, Radioiodine-Refractory, Metastatic Differentiated Thyroid Cancer
Bible KC et al. Lancet Oncol 2010;11(10):962-72.
Response (n = 37 evaluable patients) No. (%)
Complete response 0 (0)
Partial response 18 (49)
Follicular (n = 11) 8 (73)
Hürthle cell (n = 11) 5 (45)
Papillary (n = 15) 5 (33)

Vandetanib in Locally Advanced or Metastatic Differentiated Thyroid Cancer: Progression-Free Survival in a Randomised, Double-Blind, Phase II Trial
Leboulleux S et al. Lancet Oncol 2012;13(9):897-905.
Vandetanib
(n = 72)Placebo(n = 73)
Hazard ratio(95% CI) p-value
Median progression-free survival
11.1 mo 5.9 mo 0.63(0.54-0.74) 0.008
CI = confidence interval

Phase III Trials of Lenvatinib and Sorafenib in Radioiodine-Refractory Differentiated Thyroid Cancer
SELECT1 DECISION2
EndpointLenvatinib(n = 261)
Placebo(n = 131)
Sorafenib(n = 207)
Placebo(n = 210)
Response rate 64.8% 1.5% 12.2% 0.5%
Median PFS 18.3 mo 3.6 mo 10.8 mo 5.8 mo
1 Schlumberger M et al. N Engl J Med 2015;372(7):621-30; 2 Brose MS et al. Lancet 2014;384(9940):319-28.

Phase III DECISION Study Design
Brose MS et al. BMC Cancer 2011;11:349; www.clinicaltrials.gov, NCT00984282.
R
417 patients • Locally advanced or
metastatic RAI-refractory DTC
• Progression (RECIST) within the previous 14 months
• No prior chemotherapy, targeted therapy or thalidomide
Sorafenib 400 mg orally
twice daily
Placebo Orally twice daily
Randomization 1:1
Primary endpointProgression-free
survival
• Stratified by• Geographical region (North America or
Europe or Asia)• Age (<60 or 60 years)
• Progression assessed every 8 weeks (independent central review)
• Patients were allowed to receive open-label sorafenib after progression
Secondary endpoints:Overall survival Response rateSafetyTime to progressionDisease control rateDuration of responseSorafenib exposure (AUC 0-12 hours)

DECISION Study: Response, Survival and AEs
EndpointSorafenib(n = 207)
Placebo(n = 210)
Hazard ratio p-value
Median PFS 10.8 mo 5.8 mo 0.59 <0.0001
Median TTP 11.1 mo 5.7 mo 0.56 <0.0001
Median OS* NR NR 0.80 0.14
Median OS corrected for crossover† — — 0.69 —
ORR 12.2% 0.5% — <0.0001
Disease control rate 54.1% 33.8% — <0.0001
* 71.4% of patients receiving placebo crossed over at progression
• Most AEs were Grade 1 or 2• Most frequent sorafenib-associated AEs
• Hand-foot skin reaction: 76.3%• Diarrhea: 68.6%• Alopecia: 67.1%• Rash or desquamation: 50.2%
Brose MS et al. Lancet 2014;384(9940):319-28; † Brose MS et al. Proc ASCO 2014;Abstract 6060.

SELECT: Phase III Trial of Lenvatinib versus Placebo in Radioiodine-Refractory Thyroid Cancer
Schlumberger M et al. N Engl J Med 2015;372(7):621-30.
Stratification• Geographic
region (Europe, North America, other)
• Prior VEGF/VEGFR-targeted therapy (0, 1)
• Age (≤65 years, >65 years) 2:1
Patients with DTC (N = 392)• IRR evidence of
progression within previous 13 months
• 131I-refractory disease
• Measurable disease
• Up to 1 prior VEGF- or VEGFR-targeted therapy
R
Lenvatinib (n = 261)24 mg daily PO
Primary endpoint• PFS
Secondary endpoints• ORR• OS• Safety
Lenvatinib
(optional, open label)
Treatment until disease
progression confirmed
by IRR (RECIST v1.1)
Placebo (n = 131)24 mg daily PO

SELECT: Patient Characteristics
Schlumberger M et al. N Engl J Med 2015;372(7):621-30.
Variable Lenvatinib (N = 261) Placebo (N = 131)
Median age — y 64 61
Male sex — no. (%) 125 (47.9) 75 (57.3)
Region — no. (%) Europe North America Other
131 (50.2)77 (29.5) 53 (20.3)
64 (48.9)39 (29.8)
28 (21.4)
ECOG performance status — no. (%) 0 or 1 2 or 3
248 (95.0) 13 (5.0)
129 (98.5) 2 (1.5)
One prior treatment regimen with a tyrosine kinase inhibitor — no. (%) 66 (25.3) 27 (20.6)
Histologic subtype of differentiated thyroid cancer — no. (%) Papillary Poorly differentiated Follicular, not Hürthle cell Hürthle cell
132 (50.6) 28 (10.7) 53 (20.3) 48 (18.4)
68 (51.9) 19 (14.5) 22 (16.8) 22 (16.8)
Metastatic lesions — no. (%) With bony metastases With pulmonary metastases
104 (39.8) 226 (86.6)
48 (36.6)124 (94.7)

SELECT: Kaplan-Meier Estimate of PFS
From The New England Journal of Medicine, Martin Schlumberger, Makoto Tahara, Lori J Wirth, et al, Lenvatinib versus Placebo in Radioiodine-Refractory Thyroid Cancer, 372, 621-30. Copyright © 2015 Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society.

SELECT: Progression-Free Survival by Previous VEGF-Targeted Therapy
Schlumberger M et al. N Engl J Med 2015;372(7):621-30.
Median progression-free survival Lenvatinib Placebo
Hazard ratio(95% CI) p-value
TKI naïve (n = 299) 18.7 mo 3.6 mo 0.20
(0.14-0.27)
<0.0001
One prior TKI regimen (n = 93)
15.1 mo 3.6 mo0.22
(0.12-0.41)<0.0001
CI = confidence interval

Schlumberger M et al. N Engl J Med 2015;372(7):621-30.
Events/N Median (months)
Lenvatinib Placebo HR (95% CI) Lenvatinib Placebo
Target tumor size at baseline (mm)
≤35 14/65 21/28 0.14 (0.06, 0.33) NE 5.6
35-60 31/72 31/32 0.19 (0.10, 0.36) 16.4 3.7
61-92 31/63 31/34 0.24 (0.13, 0.43) 14.8 3.6
>92 31/61 30/37 0.21 (0.11, 0.42) 13.9 2.4
Histology
Papillary 58/132 58/68 0.30 (0.20, 0.44) 16.4 3.5
Poorly differentiated 14/28 18/19 0.21 (0.08, 0.56) 14.8 2.1
Follicular 20/53 20/22 0.07 (0.03, 0.21) 18.8 2.4
Hürthle cell 15/48 17/22 0.22 (0.10, 0.51) NE 5.3
Bone metastasis
No 60/157 74/83 0.18 (0.12, 0.27) 20.2 3.7
Yes 47/104 39/48 0.26 (0.16, 0.42) 14.8 2.1
Lung metastasis
No 17/35 7/7 0.24 (0.08, 0.77) 14.8 2.4
Yes 90/226 106/124 0.21 (0.15, 0.29) 18.7 3.6
SELECT: Progression-Free Survival Subgroup Analysis
NE = not evaluable/estimable (not reached)

SELECT: Response Rates
Schlumberger M et al. N Engl J Med 2015;372(7):621-30.
Lenvatinib (N = 261)
Placebo(N = 131)
Odds ratio (95% CI)
Response rate — no. (%)* 169 (64.8) 2 (1.5) 28.87
(12.46–66.86)†
Complete response 4 (1.5) 0
Partial response 165 (63.2) 2 (1.5)
Stable disease 60 (23.0) 71 (54.2)
Durable stable disease ≥23 wk 40 (15.3) 39 (29.8)
Progressive disease 18 (6.9) 52 (39.7)
Could not be evaluated 14 (5.4) 6 (4.6)
Median time to first objective response — mo (95% CI)
2.0 (1.9–3.5)
5.6 (1.8–9.4)
* Tumor responses were assessed with the use of Response Criteria in Solid Tumors (RECIST), version 1.1, and were confirmed by independent centralized radiologic review.† p < 0.001 for the comparison between the two groups

SELECT: Best Tumor Response
From The New England Journal of Medicine, Martin Schlumberger, Makoto Tahara, Lori J Wirth, et al, Lenvatinib versus Placebo in Radioiodine-Refractory Thyroid Cancer, 372, 621-30. Copyright © 2015 Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society.
Best Overall Response (n = 245)CR (n = 4) PR (n = 165)SD (n = 60)PD (n = 16)
Best Overall Response (n = 126)PR (n = 2)SD (n = 71)PD (n = 51)NE (n = 2)
Treatment group: Placebo
Treatment group: Lenvatinib
Per
cen
t C
han
ge
Fro
m B
asel
ine
at N
adir
Per
cen
t C
han
ge
Fro
m B
asel
ine
at N
adir
CR = complete response; NE = not evaluable/estimable (ie, not reached); PD = progressive disease; PR = partial response; SD = stable disease

Schlumberger M et al. N Engl J Med 2015;372(7):621-30.
SELECT: Overall Survival, ITT Population
Lenvatinib(n = 261)
Placebo(n = 131)
Hazard ratio(95% CI) p-value
Median overall survival
NR NR0.73
(0.50-1.07)0.1032
No significant difference was observed in RPSFT-adjusted overall survival (p = 0.051), which was used to correct for a potential crossover effect in the placebo arm.

SELECT: Effect of Age and Lenvatinib Treatment on Overall Survival
Brose MS et al. Proc ASCO 2015;Abstract 6048.
• Patients stratified by:– Age: Younger (≤ 65 y) vs Older (>65 y)– Region– Prior VEGF-targeted therapy
• Median OS was not reached in any subgroup except for older patients in placebo group.
• Older patients in the placebo group had worse OS than younger patients
• The impact of age was mitigated by lenvatinib treatment– No difference in OS between younger and older
patients in lenvatinib group

SELECT: Treatment-Related Adverse Events of Special Interest
Schlumberger M et al. N Engl J Med 2015;372(7):621-30.
Effect (%)
Lenvatinib (N = 261) Placebo (N = 131)
All grades Grade ≥3 All grades Grade ≥3
Hypertension 67.8 41.8 9.2 2.3
Diarrhea 59.4 8.0 8.4 0
Fatigue or asthenia 59.0 9.2 27.5 2.3
Decreased appetite 50.2 5.4 11.5 0
Decreased weight 46.4 9.6 9.2 0
Nausea 41.0 2.3 13.7 0.8
Stomatitis 35.6 4.2 3.8 0
Palmar–plantar erythrodysesthesia syndrome
31.8 3.4 0.8 0
Proteinuria 31.0 10.0 1.5 0

Phase II Trials of Everolimus Combined with Sorafenib in Refractory Thyroid Cancer
EndpointNCT012639511
(n = 33)NCT011413092
(n = 38)
Complete response (CR) 0% NR
Partial response (PR) 3% 55%
Stable disease (SD) 55% 37%
Clinical benefit (CR + PR + SD ≥6 mo)
58% NR
Disease progression NR 8%
Median PFS 13.7 mo NR
1 Brose MS et al. Proc ASCO 2015;Abstract 6072; 2 Sherman EJ et al. Proc ASCO 2015;Abstract 6069.
NR = not reported

Kim KB et al. Thyroid 2013;23(10):1277-83.
Clinical Responses to Vemurafenib in Patients with Metastatic Papillary Thyroid Cancer Harboring BRAF V600E Mutation
• 3 subjects treated• 1 PR (31% reduction in pulmonary target lesion)• 2 SD• TTP = 11.4 to 13.2 months

Vemurafenib
• Phase I study– 1/3 thyroid cancer with response; other 2 with
stable disease• Phase II study in thyroid cancer completed
• Recurrent, unresectable or metastatic papillary thyroid cancer
• BRAF V600 mutation-positive by cobas
• Radioactive iodine refractory
• Evidence of progressionwithin 14 months
Vemurafenib
Brose MS et al. ECCO/ESMO 2013;Abstract 28.
VEGFR2i naïve(n = 26) Vemurafenib
960 mg BID until disease progression
or unacceptable toxicityVEGFR2i pretreated
(n = 25)

Vemurafenib Response Rate
Brose MS et al. ESMO/ECC 2013;Abstract 28.
VEGFR2i naïveVEGFR2i
pretreated
Complete response 0 0
Partial response 35% 26%
Stable disease 6 mo 23% 10%
Clinical benefit rate 58% 36%
Median PFS 15.6 months 6.8 months

Single-Institution, Single-Arm Pilot Study Investigating the Potential for the BRAF Inhibitor Dabrafenib to Induce Radioiodine Uptake in BRAF-Mutant, Radioiodine-Refractory PTC
• Primary endpoint: Increased radioiodine uptake by 4mCi 131-I whole body scan.
• All 7 patients on study had negative 131-I scans within 14 months of enrollment.
• 6/10 evaluable patients demonstrated new radioiodine uptake on whole body scan after treatment with dabrafenib. – 2 patients had partial responses and 4 patients had
stable disease on standard radiographic restaging at 3 months.
– Thyroglobulin decreased in 4 of 6 patients who received treatment.
Rothenberg SM et al. Clin Cancer Res 2015;21(5):1028-35.

Selumetinib Response Rate
All number (%)
Evaluable number (%)
BRAF V600E number (%)
Total number 39 32 12
Complete response 0 (0%) 0 (0%) 0 (0%)
Partial response 1 (3%) 1 (3%) 1 (8%)
Stable disease 21 (54%) 21 (66%) 9 (75%)
Progression 11 (28%) 10 (31%) 2 (17%)
No data on response 6 (15%)
Hayes DN et al. Clin Cancer Res 2012;18(7):2056-65.

Impact of Selumetinib on 124I Incorporation
Ho AL et al. N Engl J Med 2013;368(7):623-32.
N = 20
Patients with new/increased 124I incorporation after selumetinib 12/20
Patients who went on to receive therapeutic RAI 8/20
Tumor genotype
Patients with increased lesional iodine
incorporation after selumetinib
(fraction of total)
Patients who received RAI
(fraction of total)
BRAF 4/9 1/9
NRAS 5/5 5/5
RET/PTC 2/3 1/3
Wild type 1/3 1/3
Total 12/20 8/20

Ho AL et al. N Engl J Med 2013;368(7):623-32.
Response to Iodine-131 Therapy with Selumetinib Treatment
Patient number
Genotype Response Serum thyroglobulin values (ng/mL)
Before
selumetinib (wk 1)
After selumetinib
(wk 5)
1 mo after radioiodine
2 mo after radioiodine
6 mo after radioiodine
1 RET/PTC SD 650 780 240 200 740
2 WT SD 360 880 270 210 194
3 NRAS PR 2,700 3,200 3,700 740 480
4 NRAS PR 510 1,300 NA 31 22
5 NRAS PR 220 530 11.3 0.4 <0.2
6 NRAS SD 840 570 46 31 100
7 NRAS PR 6,500 1,070 170 66 57
8 BRAF PR 82 650 NA 23 14
SD = stable disease; WT = wild type; PR = partial response; NA = not available

A Phase I/II Study of Cediranib (CED) and Lenalidomide (LEN) in Patients with Advanced Differentiated Thyroid Cancers
Brown RL et al. The Endocrine Society’s 94th Annual Meeting and Expo 2012;Abstract SUN-281.
PHASE I
PHASE II
Dose escalation of CED and LEN
Cohort A: CED 30 mg
Cohort B: CED + LEN at MTD
Progression-free survival
Determine maximum tolerated dose (MTD) of combined therapy

RET
• 10q11.2• 3 functional domains• Genotype-phenotype
correlations• Signals through multiple
pathways to regulate survival, cell growth, differentiation
N-terminal signal sequence
Cadherin-like domain
Cysteine-rich domain
Transmembrane domain
Tyrosine kinase domain
MEN 2A/FMTC
FMTC
MEN 2B
Alternative 3 splice sites
COOH

Phase III ZETA Study Design
Vandetanib 300 mg/dayn = 231
Follow for progression Follow for progression
Optional open-label vandetanib 300 mg/day
Follow for survival
Patients with unresectable locally advanced or metastatic hereditary or sporadic MTC (N = 331)
Placebon = 100
2:1 randomization
Discontinue blinded treatment at progression*
*Progression as assessed by the site investigator
www.clinicaltrials.gov, NCT00410761.

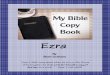
Phase III ZETA Study: PFS by Central Independent Review
0
Vandetanib 300 mg
Placebo
Time (months)
231 196 169 140 40 1 0
100 71 57 45 13 0 0
No. at risk
Vandetanib 300 mg
Placebo
0.6
0.8
Pro
gre
ssio
n-F
ree
Su
rviv
al (
pro
po
rtio
n)
0.9
0
0.1
0.2
0.3
0.4
0.5
0.7
1.0
6 12 18 24 30 36
Wells, SA Jr et al: J Clin Oncol 30 (2), 2012: 134-41. Reprinted with permission. © 2012 American Society of Clinical Oncology. All rights reserved.

ZETA Study: Other Notable Features
• Significantly higher objective response rate– 45% versus 13%; odds ratio = 5.48, 95% CI: 2.99-
10.79, p < 0.001– 12 of 13 responses in the placebo arm were seen
during treatment with open-label vandetanib – Objective responses were durable
• Biochemical response rate– Calcitonin (69% versus 3%; odds ratio = 72.9, 95% CI:
26.2-303.2, p < 0.001)– CEA (52% versus 2%; odds ratio = 52.0, 95% CI: 16.0-
320.3, p < 0.001)• Statistically significant delay in time to worsening of
pain with vandetanib versus placebo (hazard ratio = 0.61; p = 0.006)
• Median overall survival: Not yet reached
Wells SA Jr et al. J Clin Oncol 2012;30(2):134-41.

Cabozantinib
• A potent oral targeted therapy that inhibits MET, VEGFR2 and RET1
• Clinical activity observed in MTC patients in a Phase I study2
– 29% objective response rate per RECIST– 68% disease control rate
• Stable disease for >6 months or confirmed partial response
1 Yakes FM et al. Mol Cancer Ther 2011;10(12):2298-308; 2 Kurzrock R et al. J Clin Oncol 2011;29(19):2660-6.

Trial design Endpoints Study sites
Phase III, randomized, placebo controlled
Primary: PFSSecondary: OS, ORR per RECIST Global
EXAM: Phase III Trial of Cabozantinib in Medullary Thyroid Carcinoma with RECIST Progression at Baseline
2
1
R
• Medullary thyroid carcinoma• Unresectable locally advanced
or metastatic disease• Documented RECIST
progression within 14 mo• No limit to prior therapies
Cabozantinib 140 mg qd
N = 219
Placebo qdN = 111
Progression
No crossover allowed.
Schlumberger M et al. Proc ASCO 2015;Abstract 6012.
Survival follow-
up

EXAM Study: Survival, Response and AEs
Endpoint Cabozantinib PlaceboHazard
ratio p-value
Median PFS 11.2 mo 4.0 mo 0.28 <0.001
ORR (all partial responses)* 28% 0% — <0.001
* ORR for RET mutation-positive and negative subgroups receiving cabozantinib was 32% and 25%, respectively
Ninety-four percent (170 of 180) of patients with measurable disease at baseline and at least one postbaseline assessment who received cabozantinib had a detectable decrease in target lesion size compared to 27% (24 of 89) of patients in the placebo group.
Elisei R et al. J Clin Oncol 2013;31(29):3639-46.
Common Grade ≥3 cabozantinib-related AEsDiarrhea: 15.9%Palmar-plantar erythrodysesthesia: 12.6%Decreased weight: 4.7%Decreased appetite: 4.7%Nausea: 1.4%Fatigue: 9.3%Treatment discontinuation in 16% of cabozantinib and 8% placebo

EXAM: Response and Survival According to RET M918T Status
Endpoint
RET M918T Positive RET M918T Negative
Cabozantinib(n = 81)
Placebo (n = 45)
Cabozantinib(n = 75)
Placebo(n = 32)
ORR 34% 0% 20% 0%
Median OS (mo) 44.3 18.9 20.2 mo 21.5mo
OS HR (95% CI) 0.60 (0.38-0.95) 1.12 (0.70-1.82)
p-value 0.0260 0.6308
Median PFS (mo) 13.9 4.0 5.7 5.4
PFS HR (95% CI) 0.15 (0.08-0.28) 0.67 (0.37-1.23)
p-value <0.0001 0.1875
ORR = objective response rate; OS = overall survival; PFS = progression-free survival; HR = hazard ratio
Schlumberger M et al. Proc ASCO 2015;Abstract 6012.

Genomic Landscape of Anaplastic Thyroid Cancer (ATC)
Capdevila J et al. Proc ASCO 2015;Abstract 6033.
• Exome-seq on 13 cases of ATC including 2 cases of concomitant papillary thyroid cancer (PTC) and ATC in the same patient, showed:– Mutations related with ATC include TP53 (30%); RAS
(29%), PIK3CA (23%), STAT (23%), BRAF (15%) and mutations in genes involved in SWI/SNF (15%), CDK (15%) and hedgehog (15%) pathways
– Significantly different genomic background with few common root mutations between PTC and ATC
– Subclonal oncogenic BRAF and NRAS mutations enriched in PTC but decreased in ATC
– Driver mutations TP53, PI3KCA, STAT and PDGFR detectable only in ATC

Ezra W CohenUniversity of California, San Diego
RTP ON DEMAND: Head and Neck Cancer

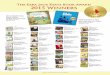
Anatomic Sites of Head and Neck Cancer
• Heterogeneous group of cancers; varying primary sites
• Squamous histology in 95% of cases
• Anatomic sites – Oral cavity
– Nasopharynx/oropharynx/hypopharynx
– Larynx
• Other anatomic sites– Paranasal sinuses
– Lip
– Salivary glands
Adapted from SEER training modules, head & neck cancer. National Institutes of Health, National Cancer Institute.
Oral CavityLipBuccal mucosaAlveolar ridgeRetromolar trigoneFloor of mouthHard palateOral tongue (anterior two thirds)
LarynxSupraglottisGlottisSubglottis
Nasal Cavity
Tongue
Esophagus
Jaw
Nasopharynx
OropharynxBase of tongueSoft palateTonsillar pillar and fossa
Hypopharynx
Pharynx

Two Distinct SCCHN Entities
HPV+ HPV-
Anatomic slide Tonsil/base of tongue All sites
Histology Basaloid Keratinized
Age Younger Older
Gender 3:1 men 3:1 men
Risk factors Sexual behavior Alcohol/tobacco
Incidence Rising Declining
Survival Improved Worse
Molecular PI3K pathway alterations p53, p16, CCDN1, FAT1
• Population-level incidence of HPV-positive oropharyngeal cancers increased by 225% (95% CI, 208% to 242%) from 1988 to 2004 (from 0.8 per 100,000 to 2.6 per 100,000), and incidence for HPV-negative cancers declined by 50% (95% CI, 47% to 53%; from 2.0 per 100,000 to 1.0 per 100,000).1
1 Chaturvedi AK et al. J Clin Oncol 2011;29(32):4294-301.

Subtype Proportion Key characteristics
Basal 31%Expression patterns in basal layer of human airway epithelium; low levels
of SOX2 relative to TP63
Mesenchymal 27%
Expression markers of epithelial to mesenchymal transformation including VIM, DES, TWIST1,
PDGFRA/B
Atypical 24%Includes all HPV+; little evidence for
chromosome 7 amplification
Classical 18%Heaviest smoking histories; elevation expression levels of oxidative stress response genes, including NFE2L2
Gene Expression Subtypes of SCCHN
The Cancer Genome Atlas Network. Nature 2015;517:576-82

ObservationBest supportive care
Treatment Algorithm for Recurrent or Metastatic Head and Neck Squamous Cell Carcinoma
Fit with aggressivesymptomatic disease
Good performance status with active
disease
Frail or indolentasymptomatic disease
• Cisplatin/carboplatin+ 5-FU + cetuximab
• Platinum doublet*• Cisplatin/paclitaxel• Carboplatin/paclitaxel• Cisplatin/docetaxel+/- cetuximab
Single-agent therapy:
• Paclitaxel/docetaxel• Cetuximab*• Capecitabine• Vinorelbine• Methotrexate
R/M HNSCC Locally recurrent or distant metastases
* Consider if platinum resistant
Price KA, Cohen EE. Curr Treat Options Oncol 2012;13(1):35-46.

Single-Agent Response Rates of EGFR-Targeted mAbs and TKIs in SCCHN
-
Drug Phase Reference RRCetuximab II Vermorken et al, 2007 13%
Erlotinib II Soulieres et al, 2004 4%
Gefitinib
II Cohen et al, 2003 11%
II Cohen et al, 2005 2%
III Stewart et al, 2009 8%
Lapatinib II Abidoye et al, 2006 (ASCO) 0%
Zalutumumab III Machiels et al, 2010 (ASCO) 6%
Vermorken JB et al. J Clin Oncol 2007;25(16):2171-7; Soulieres D et al. J Clin Oncol 2004;22(1):77-85; Cohen EE et al. J Clin Oncol 2003;21(10):1980-7; Cohen EE et al. Clin Cancer Res 2005;11(23):8418-24; Kirby AM et al. Br J Cancer 2006;94(5):631-6; Stewart JS et al. J Clin Oncol 2009;27(11):1864-71; Abidoye OO et al. Proc ASCO 2006;Abstract 5568; Machiels JH et al. Proc ASCO 2010;Abstract LBA5506; Seiwert TY et al. ESMO 2010;Abstract 1010PD.

EXTREME Study Design
R
Group ACetuximab 400 mg/m2 initial dose
then 250 mg/m2 weekly + EITHER carboplatin (AUC 5, d1) OR cisplatin (100 mg/m2 IV, d1)+ 5-FU (1,000 mg/m2 IV, d1-4):
3-week cycles
Group BEITHER carboplatin (AUC 5, d1) OR cisplatin (100 mg/m2 IV, d1) + 5-FU (1,000 mg/m2 IV, d1-4):
3-week cycles
Cetuximab No treatment
Progressive disease or unacceptable toxicity
6 chemotherapy cycles maximum
Vermorken JB et al. N Engl J Med 2008;359(11):1116-27.

EXTREME Study: Overall Survival
Vermorken JB et al. N Engl J Med 2008;359(11):1116-27.
Cetuximab + platinum/fluo
rouracil(n = 222)
Platinum/fluorouracil
alone (n = 220)
Hazard ratio(95% CI) p-value
Median overall survival 10.1 mo 7.4 mo 0.80(0.64-0.99) 0.04


Phase II Trial of Dacomitinib: Response, Survival and Grade 3/4 AEs
Response (n = 63) n (%)
Complete response (CR) 0 (0)
Partial response (PR) 8 (12.7)
Stable disease (SD) ≥24 weeks <24 weeks
36 (57.1)9 (14.3)
27 (42.9)
Progressive disease 17 (27)
Indeterminate 2 (3.2)
Objective response rate (CR + PR) 8 (12.7)
Clinical benefit rate (CR + PR + SD ≥24 weeks) 17 (27.0)
Abdul Razak AR et al. Ann Oncol 2013;24(3):761-9.
Most common Grade ≥3 AEsDiarrhea: 15.9%Acneiform dermatitis: 8.7%Fatigue: 8.7%
Survival (n = 69) Median progression-free survival 12.1 weeks
Median overall survival 34.6 weeks

Eligibility criteria:• Locoregionally
recurrent or metastatic SCCHN
• PS 0 or 1
Primary endpoint: Progression-free survival
PD
Trial ID: NCT01836029Estimated enrollment: 175 (open)
www.clinicaltrials.gov; Accessed April 2015.
ACTIVE8: Phase II Trial of Chemotherapy and Cetuximab in Combination with VTX-2337 in Recurrent or Metastatic SCCHN
1:1
R
Chemotherapy + cetuximab + VTX-2337
Up to 6 cycles
Chemotherapy + cetuximab + placebo
Up to 6 cycles
Cetuximab
Cetuximab

Vermorken JB et al. Lancet Oncol 2013;14(8):697-710.
SPECTRUM: Cisplatin + 5-FU ± Panitumumab in Recurrent/Metastatic SCCHN
• Open-label, randomized Phase III trial
Patients with distant metastatic and/or locally
recurrent SCCHN, ECOG PS ≤1
(N = 657)
Stratified by previous treatment, primary tumor
site, ECOG PS
Optional panitumumab maintenance q3wk
Panitumumab 9 mg/kg day 1Cisplatin 100 mg/m2 day 15-FU 1,000 mg/m2 days 1-4
(n = 327)
Cisplatin 100 mg/m2 day 15-FU 1,000 mg/m2 days 1-4
(n = 330)
Max six 3-wk cycles
• Primary endpoint: OS• Secondary endpoints: PFS, ORR, DOR, TTR, safety

SPECTRUM Study: Overall Survival
Vermorken JB et al. Lancet Oncol 2013;14(8):697-710.
Cisplatin/5-FU + panitumumab
(n = 327)Cisplatin/5-FU
(n = 330)Hazard ratio
(95% CI) p-value
Median overall survival 11.1 mo 9.0 mo 0.873(0.729-1.046) 0.1403

Chen LF et al. Clin Cancer Res 2010;16:2489-2495
Mechanisms of Resistance to EGFRi

HNSCC = head and neck squamous cell carcinoma; IV = intravenous; PD = progressive disease; CT = computed tomography scan; MRI = magnetic resonance imaging; R/M = recurrent/metastatic
Stage 1 Stage 2
CT/MRI q8wk
Phase II Study of Afatinib versus Cetuximab
Metastatic recurrent HNSCC
N = 124 (62 per arm)
R
Afatinib50 mg po daily
Cetuximab400/250 mg/m2 IV weekly
Continue until PD or undue AEs
Continue until PD or undue AEs
Cetuximab400/250 mg/m2 IV weekly
Afatinib50 mg po daily
Stratum: No. prior chemotherapies for R/M
disease (0 or ≥1)
Seiwert TY et al. Ann Oncol 2014;25(9):1813-20.

Phase II Study of Afatinib versus Cetuximab: Maximum Tumor Shrinkage in Target Lesions
Seiwert TY et al. Ann Oncol 2014;25(9):1813-20.
Investigator review Independent central review
Afatinib Cetuximab Afatinib Cetuximab
Total randomized, n 62 62 62 62
ORR (CR, PR), n (%) 95% CI
10 (16.1)8.0-27.7
4 (6.5)1.8-15.7
5 (8.1)2.7-17.8
6 (9.7)3.6-19.9
p-value 0.09 0.78

Phase II Study of Afatinib versus Cetuximab: Progression-Free and Overall Survival
Seiwert TY et al. Ann Oncol 2014;25(9):1813-20.
Stage 1
Afatinib(n = 62)
Cetuximab (n = 62)
Hazard ratio(95% CI) p-value
Median progression-free survival 13.0 wk 15.0 wk 0.93
(0.62-1.38) 0.71
Stage 2
Afatinib(n = 36)
Cetuximab (n = 32)
Hazard ratio (95% CI) p-value
Median progression-free survival 9.3 wk 5.7 wk 0.64
(0.38-1.05) 0.08
Stage 1 and Stage 2
Afatinib (n = 62)
Cetuximab (n = 62)
Hazard ratio (95% CI) p-value
Median overall survival 35.9 wk 47.1 wk 1.06 (0.70-1.62) 0.78

Phase II Study of Afatinib versus Cetuximab: Tumor Shrinkage in Stage 2
Seiwert TY et al. Ann Oncol 2014;25(9):1813-20.
Afatinib after prior
cetuximab in Stage 1, nCetuximab after prior afatinib in Stage 1, n
Maximum % tumor shrinkage
≥20% 6 11
≥0% and <20% 12 7
>-30% and <0% 11 7
≤30% 1 1

Phase II Study of Afatinib versus Cetuximab: Treatment-Related Adverse Events in ≥10% of Patients (Stage 1)
Afatinib (n = 61) Cetuximab (n = 60)
All grades Grade 3-4 All grades Grade 3-4
Total, n (%) 59 (96.7) 32 (52.5) 51 (85.0) 11 (18.4)
Rash/acne 48 (78.7) 11 (18.0) 46 (76.7) 5 (8.3)
Diarrhea 48 (78.7) 9 (14.8) 12 (20.0) 0
Stomatitis 21 (34.4) 7 (11.5) 14 (23.3) 0
Fatigue 20 (32.8) 3 (4.9) 13 (21.7) 1 (1.7)
Nausea 17 (27.9) 1 (1.6) 12 (20.0) 1 (1.7)
Vomiting 10 (16.4) 1 (1.6) 8 (13.3) 0
Dry skin 9 (14.8) 0 15 (25.0) 0
Dehydration 8 (13.1) 5 (8.2) 1 (1.7) 0
Decreased appetite 5 (8.2) 3 (4.9) 8 (13.3) 0
Nail effects 4 (6.6) 0 6 (10.0) 1 (1.7)
Ocular effects 4 (6.6) 0 6 (10.0) 1 (1.7)
Constipation 2 (3.3) 0 7 (11.7) 0
Seiwert TY et al. Ann Oncol 2014;25(9):1813-20.

Trial design Endpoints Study sites
Phase III, randomized, open-label
Primary: PFS Key secondary: OS Global
2
1
LUX-Head & Neck 1: Second-Line Afatinib versus Methotrexate in Recurrent and/or Metastatic Squamous Cell Carcinoma of the Head and Neck Progressing After Platinum-Based Therapy
R
Relapsed/metastatic squamous cell carcinoma• Failure of platinum-based
chemotherapy for relapsed/metastatic disease
• Documented PD• PS 0-1• Maximum of 1
chemotherapy regimen for relapsed/metastatic disease
• No prior EGFR TKIs
Afatinib 40 mg qdN = 316
Methotrexate 40 mg/m2 qwk
N = 158
Treatment until PD
Machiels J et al. ESMO 2014;Abstract LBA29_PR.
PFS = progression-free survival; OS = overall survival; PD = progressive disease

LUX-Head & Neck 1: Efficacy
EndpointAfatinib(n = 322)
Methotrexate (n = 161)
Hazard ratio p-value
Progression-free survival 2.6 mo 1.7 mo 0.80 0.03
Overall survival 6.8 mo 6.0 mo 0.96 NS
Disease control rate 49.1% 38.5% — 0.04
Overall response rate 10.2% 5.6% — 0.10
Machiels J et al. ESMO 2014;Abstract LBA29_PR.
• Afatinib delayed deterioration of global health status, pain and swallowing (all p ≤0.03) and provided improvement in pain (p = 0.03)
• Most frequent Grade 3/4 drug-related AEs
• Afatinib: Rash/acne (9.7%), diarrhea (9.4%)
• Methotrexate: Leukopenia (15.6%), stomatitis (8.1%)
• Fewer treatment-related dose reductions, discontinuations and fatal events with afatinib

LUX-Head & Neck 1: Select Drug-Related Adverse Events
Machiels J et al. ESMO 2014;Abstract LBA29_PR.
Afatinib (n = 320) Methotrexate (n = 160)
All grades Grade 3 Grade 4 All grades Grade 3 Grade 4
More frequent with afatinib
Rash/acne 74 10 0 8 0 0
Diarrhea 72 9 1 12 2 0
Paronychia 14 1 0 0 0 0
Decreased appetite 13 3 0 13 1 0
Vomiting 13 1 <1 9 0 0
Dry skin 11 0 0 0 0 0
More frequent with methotrexate
Stomatitis 39 6 <1 43 8 0
Fatigue 25 6 0 32 3 0
Nausea 20 2 0 23 1 0
Neutropenia <1 <1 0 19 6 1
Anemia 7 1 0 19 5 1

Trial design Endpoints Study sites
Phase III, randomized, placebo controlled
Primary: DFSSecondary: 2-year DFS rate, OS, safety Global
LUX-Head & Neck 2: Adjuvant Afatinib in Locally Advanced Squamous Cell Carcinoma of the Head and Neck
NED = no evidence of disease
2
1
R
• Locally advanced squamous cell carcinoma of the head and neck
• Unresected• Stage III–IVb• Previous chemoradiation therapy• Excludes nonsmokers with
oropharyngeal cancer• PS 0-1• NED after chemoradiation
therapy
Afatinib 40 mg qdN = 446
Placebo qdN = 223
Treatment for 18 months/
until recurrence

Basis for Immunotherapy — Immune Escape
Adapted from Seiwert TY et al. Proc ASCO 2014;Abstract 6011; Melero I et al. Clin Cancer Res 2013;19(5):997-1008.
• Expression of PD-L1 on tumor cells and macrophages can suppress immune surveillance.
• In mouse models antibodies blocking PD-1/PD-L1 interaction lead to tumor rejection.
• Clinical prognosis correlates with presence of TILs and PD-L1 expression in multiple cancers.

KEYNOTE-012: Multicenter, Nonrandomized, Phase Ib Squamous Cell Carcinoma of the Head and Neck Expansion Cohort
Seiwert TY et al. Proc ASCO 2014;Abstract 6011.
Recurrent or metastatic head and neck cancer• PD-L1-positive• Investigator-
assessed HPV status
HPV-negative cohort
HPV-positivecohort
Treat until PD*
* Treatment beyond initial PD allowed; radiation therapy to progressive lesion allowed
PD = progressive disease
Pembrolizumab10 mg/kg q2wk
Pembrolizumab10 mg/kg q2wk

KEYNOTE-012: Best Overall Response
Seiwert TY et al. Proc ASCO 2014;Abstract 6011.
Total head/neck
N = 56HPV (+)N = 20
HPV (-)N = 36*
Response evaluation n (%) 95% CI n (%) 95% CI n (%) 95% CI
Complete response (CR) 1 (1.8) 0.0, 9.6 1 (5.0)
0.1, 24.9 0 (0.0) 0.0, 9.7
Partial response (PR) 10 (17.9) 8.9, 30.4 3 (15.0) 3.2, 37.9 7 (19.4) 8.2, 36.0
Best overall response (CR + PR)†
11 (19.6)
10.2, 32.4
4 (20.0)
5.7, 43.7 7 (19.4) 8.2, 36.0
Stable disease 16 (28.6) 17.3, 42.2 8 (40.0)
19.1, 63.9 8 (22.2) 10.1, 39.2
Progressive disease 25 (44.6) 31.3, 58.5 7 (35.0) 15.4, 59.2 18 (50.0) 32.9, 67.1
No assessment 4 (7.1) 2.0, 17.3 1 (5.0) 0.1, 24.9 3 (8.3) 1.8, 22.5
• PD-L1 expression correlates with response• Using a Youden-Index derived, preliminary PD-L1 cut point:
- Above cut point: 45.5% (5/11) RR- Below cut point: 11.4% (5/44) RR
Based on RECIST 1.1 per site assessment; includes confirmed and unconfirmed responses* Includes 2 patients for whom HPV data were unavailable.† A single patient with PD followed by PR on treatment was classified as PR.

KEYNOTE-012: PD-L1 Screening Results
104 patients screened:
PD-L1 staining in tumors of screened patients (N = 104)
Staining (%) 0 1-10 11-20 21-30 31-40 41-50 51-60 61-70 71-80 81-90 91-100
n 26* 24 8 9 3 2 2 4 3 2 21
* Three patients with tumor (-) but stroma (+) by IHC
PD-L1-positive: 78% (81)• Study eligible n = 61*
- HPV (-) n = 36- HPV (+) n = 23- HPV (na) n = 2
PD-L1-negative: 22% (23)
Seiwert TY et al. Proc ASCO 2014;Abstract 6011.

Clinical endpointOverall
(n = 117)HPV (+)(n = 34)
HPV (-)(n = 81)
ORR, n (%) 29 (24.8) 7 (20.6) 22 (27.2)
Complete response 1 (0.9) 1 (2.9) 0 (0)
Partial response 28 (23.9) 6 (17.6) 22 (27.2)
KEYNOTE-012: Efficacy by HPV Status
Seiwert TY et al. Proc ASCO 2015;Abstract LBA6008.

KEYNOTE-012: Select Drug-Related Adverse Events
Seiwert TY et al. Proc ASCO 2014;Abstract 6011.
All grades Grades 3-5
n % n %
Any drug-related event 35 58.3 10 16.7
Fatigue
10
16.7
0
0.0
Pruritus
6
10.0
0
0.0
Rash
5
8.3
2
3.3
Nausea
4
6.7
0
0.0
Decreased appetite
3
5.0
0
0.0
Myalgia
3
5.0
0
0.0

Phase I Study of MEDI4736 in Recurrent/Metastatic SCCHN: Results Summary
• Efficacy outcomes– 29 SCCHN patients evaluable– 7 patients had radiographic shrinkage of target tumor lesions
ranging from 7% to 76%– 5 of 7 have been followed for at least 12 weeks
• 4 patients have partial responses• 0 patients have evidence of objective progression
• Safety outcomes– 50 patients evaluable– 39% had treatment-related AEs (TRAEs)
• Most frequent were nausea, diarrhea, rash and dizziness• No pneumonitis observed
– No TRAE led to treatment discontinuation
Fury M et al. Proc ESMO 2014;Abstract 988PD.

Role for Induction Chemotherapy (IC) in Locally Advanced Head and Neck Cancer Prior to Concomitant Chemoradiation Therapy (CCRT)
– Meta-analysis of randomized controlled trials showed with IC:• No significant effect on OS or PFS• Advantage in complete response and disease
control • Trend to improved overall survival
– Selected patients may benefit from the addition of IC to CCRT
– Future studies are warranted to evaluate role of IC in subpopulations of patients with locally advanced head and neck cancer
Popovtzer A et al. ASCO 2015;Abstract 6068.

NCT00193765: Phase III Trial of Elective Neck Dissection versus Watch and Wait Policy (Therapeutic Neck Dissection)
Elective Neck Dissection
(n=243)
Watch & Wait/Therapeutic Neck
Dissection (n=253)
D’Cruz AK et al. Proc ASCO 2015;Abstract LBA3.
Treatment
Physical Exam
Physical Exam + Ultrasonography
Follow-Up
R1 R2
• Histologically proven SCC cT1/T2N0 oral cavity squamous cell cancers
• Amenable to per-oral excision
• Treatment naive

Survival: Elective versus Therapeutic Neck Dissection
Endpoint
Elective neck dissection
(n = 243)
Therapeutic neck dissection
(n = 253)Hazard
ratio p-value
Three-year overall survival
80% 67.5% 0.64 0.014
Three-year disease-free survival
69.5% 45.9% 0.45 <0.001
D’Cruz AK et al. Proc ASCO 2015;Abstract LBA3.

Oropharyngeal, laryngeal, oral, hypopharyngeal or occult HNSCC
Nodal metastases Stage N2 (a, b, or c) or N3 on CT/MRI
Indication for curative radical concurrent CRT
Suitable for ND1:1
R
PET-CT & assessment*
C
R
T
PET-NECK: A Phase III Trial Comparing PET-CT Guided Active Surveillance to Planned Neck Dissection (ND) for Locally Advanced Nodal Metastases in Patients with HNSCC Treated with Primary Radical Chemoradiation Therapy (CRT)
PET-CT guided “active surveillance”
(n = 282 )
Standard treatment “planned ND”
(n = 282)
Mehanna H et al. ASCO 2015;Abstract 6009.
CT & assessment** 9-13 wk after CRT completion
ND before or after CRT

PET-NECK Trial Conclusions
• PET-CT guided surveillance resulted in equivalent OS to standard treatment of planned ND:– Only 20% of patients received neck dissections– Fewer neck dissection complications– Fewer serious adverse events– Similar quality of life
• Surveillance arm was more cost-effective
Mehanna H et al. ASCO 2015;Abstract 6009.
























![[MS-RTP]: Real-time Transport Protocol (RTP) …...Release: July 24, 2018 [MS-RTP]: Real-time Transport Protocol (RTP) Extensions Intellectual Property Rights Notice for Open Specifications](https://img.pdfslide.us/doc/110x75/5ecb4ebafdd0d04e1c3c1812/ms-rtp-real-time-transport-protocol-rtp-release-july-24-2018-ms-rtp.jpg)