Embed Size (px)
Citation preview
![Page 1: Eyes ambulatory chief 2.pptx [Read-Only] - Santa … · Lids/lashes: Stye (hordeolum) • Chronic or acute infection of eyelash follicle ... Microsoft PowerPoint - Eyes ambulatory](https://reader042.pdfslide.us/reader042/viewer/2022031000/5b81bf1a7f8b9ae87c8cfd1f/html5/page/1.jpg)
2/11/2013
1
Ambulatory Chief Talk: Differential Diagnosis & Treatment of non‐Cannabis Induced Red Eye
Dr. Cathryn Christensen, R3
AKA: “something related to eyes...maybe red eyes. I just learned we just have eye kits in clinic. I might figure out what's in them. Honestly, I'm not quite
sure....”
Objectives
• Review basics of eye exam and anatomy
• Review common causes of red eye
• Know when to refer
• Review treatment of most common diagnoses
• Cases (if time)
• Teaser…..ocular ultrasound
• “Doc, my eye is red….”
• Ddx ?• Ddx…?
Ddx…• Conjunctivitis (bacterial, viral, allergic)• Dry eye syndrome• Contact lens overwear• Corneal abrasion• Corneal foreign body• Corneal foreign body• Subconjunctival hemorrhage• Episcleritis• Eyelid pathology:
– Stye (hordeoleum)– Chalazion (Meibomian gland granuloma)– Blepharitis
Ddx (scary)…
• Angle closure glaucoma• Hyphema• Hypopyon• Iritis• Iritis• Scleritis• Infectious keratitis
– Bacterial– Viral
Anatomy…..
![Page 2: Eyes ambulatory chief 2.pptx [Read-Only] - Santa … · Lids/lashes: Stye (hordeolum) • Chronic or acute infection of eyelash follicle ... Microsoft PowerPoint - Eyes ambulatory](https://reader042.pdfslide.us/reader042/viewer/2022031000/5b81bf1a7f8b9ae87c8cfd1f/html5/page/2.jpg)
2/11/2013
2
History? Ask…
• Vision affected?
• Foreign body sensation? – Objective (unable to open eye) = corneal process
– Subjective (gritty scratchy) = conjunctivitis drySubjective (gritty, scratchy) conjunctivitis, dry
• Photophobia? (+ FB = corneal, ‐FB, think iritis)
• Trauma? Blunt or sharp?
• Contact lens wearer? (r/o keratitis)
• Discharge? If opaque think bacterial conjunctivitis or keratitis
Exam…
• General– Hat, sunglasses, hand blocking out light?– Other signs of trauma, illness?
• Ophtho:– Visual acuity
• If reduced, r/o keratitis, iritis, angle‐closure glaucoma• If wnl and likely lid, conjunctiva or corneal d/o, reassuring
– Penlight• If P not ERL, and mid‐range (4‐5mm), consider glaucoma• If pinpoint, consider corneal abrasion, keratitis, iritis
– Fluorescein exam• Corneal abrasion, keratitis
Exam (continued)…• Purulent d/c?
– Bacterial keratitis (fluorescein defects) v. conjunctivitis• Pattern of redness
– Diffuse (palpebral and bulbar conjunctiva) v focal– Ciliary flush (mosty at limbus where cornea meets sclera): think keratitis, iritis, glaucoma
– Hemorrhagic v. dilated blood vessels?h ?• White spot or opacity on cornea?
– Think infectious keratitis (bacterial or HSV)• Hypopyon or hyphema? (layer of white or red cells in ant chamber) – White: infectious keratitis‐‐‐needs ophtho in hours– Red: trauma, needs eval for penetrating injury, reitnaldetachment, glaucoma
• +/‐ Fundus exam
![Page 3: Eyes ambulatory chief 2.pptx [Read-Only] - Santa … · Lids/lashes: Stye (hordeolum) • Chronic or acute infection of eyelash follicle ... Microsoft PowerPoint - Eyes ambulatory](https://reader042.pdfslide.us/reader042/viewer/2022031000/5b81bf1a7f8b9ae87c8cfd1f/html5/page/3.jpg)
2/11/2013
3
A photographic tour….Emergent referrals…• Angle closure glaucoma:
• HA, malaise, n/v, reduced acuity
Emergent referrals… Emergent referrals…• Hyphema:
• RBCs layered out in anterior chamber
• May reflect trauma, inflammation, neovascularization
![Page 4: Eyes ambulatory chief 2.pptx [Read-Only] - Santa … · Lids/lashes: Stye (hordeolum) • Chronic or acute infection of eyelash follicle ... Microsoft PowerPoint - Eyes ambulatory](https://reader042.pdfslide.us/reader042/viewer/2022031000/5b81bf1a7f8b9ae87c8cfd1f/html5/page/4.jpg)
2/11/2013
4
Emergent referrals… Emergent referrals…• Hypopyon:
• WBCs layered out in ant chamber
• May be associated with
• Infectious keratitis, rheum,
Emergent referrals… Emergent referrals…• Iritis = anterior uveitis:
• Inflammation of anterior uveal tract
• May present similar to corneal process ‐FB
• Ciliary flush: red ring around iris, irr. iris
• Infx, inflam, infiltrative (TB, , , ( ,
Sarcoid, syphilis, Reiters)
Emergent referrals… Emergent referrals…• Infectious keratitis (bacterial, viral, fungi, parasite):
• FB sensation, hard to keep eye open
• White spot (corneal ulcer)
• S. aureus, P. aeruginosa, S. pneumo, others
• Associated with ON contact lensAssociated with ON contact lens
• Dry eyes, topical steroids,
immunosuppression
![Page 5: Eyes ambulatory chief 2.pptx [Read-Only] - Santa … · Lids/lashes: Stye (hordeolum) • Chronic or acute infection of eyelash follicle ... Microsoft PowerPoint - Eyes ambulatory](https://reader042.pdfslide.us/reader042/viewer/2022031000/5b81bf1a7f8b9ae87c8cfd1f/html5/page/5.jpg)
2/11/2013
5
Urgent referrals… Urgent referrals…• Viral keratitis: HSV, occasionally adeno
• Red eye, photophobia, FB sensation, watery d/c
• Faint branching grey opacity on penlight exam
• Clearer dendritic ulcer with fluorescein
• Topical or antiviral agents ophtho in a few daysTopical or antiviral agents, ophtho in a few days
Emergent Referrals… Emergent Referrals… • Scleritis:
• Diffuse redness, reduced vision, photophobia, severe orbital pain which increases with eye movements
• Systemic illness: RA, SLE, polyarteritis nodosa
• Tx: steroid eye drops +/‐ systemic steroids
Review:If…..
• vision is unaffected
• Pupil reacts
• No objective FB sensationj
• No photophobia
• No mucopurulent d/c
• No corneal opacity, hypopyon or hyphema...
Then PCP can make initial dx and start tx
![Page 6: Eyes ambulatory chief 2.pptx [Read-Only] - Santa … · Lids/lashes: Stye (hordeolum) • Chronic or acute infection of eyelash follicle ... Microsoft PowerPoint - Eyes ambulatory](https://reader042.pdfslide.us/reader042/viewer/2022031000/5b81bf1a7f8b9ae87c8cfd1f/html5/page/6.jpg)
2/11/2013
6
Viral conjunctivitis• Discharge is mucoserous
• May have other URI sx
• Often starts in one, then spreads to other
• Tx: antihistamine drops (naphcon A) for no more than 2 weeks
Allergic Conjunctivitis
• Discharge is mucoserous, papillae under eyelid
• Itchy eyes
• Tx: naphcon to calm down (no more than a couple weeks,
• Then: Mast cell stabilizers if longer term txneeded: patanol, zaditor, or alomide
B
![Page 7: Eyes ambulatory chief 2.pptx [Read-Only] - Santa … · Lids/lashes: Stye (hordeolum) • Chronic or acute infection of eyelash follicle ... Microsoft PowerPoint - Eyes ambulatory](https://reader042.pdfslide.us/reader042/viewer/2022031000/5b81bf1a7f8b9ae87c8cfd1f/html5/page/7.jpg)
2/11/2013
7
Bacterial conjuncitivitis• Stinging pain, purulent d/c, “glued eyes” upon waking
• No corneal involvement, PERRL, preserved vision• S. aureus (adults), S. pneumo (children)• Tx: Fluoroquinolones (ofloxacin or cipro), or q ( p ),gentamicin or sulfacetamide (bleph‐10)
• Adults don’t tolerate ointments
Corneal abrasion• Trauma may or may not be recalled (finger, paper, makeup applicator, lenses, metal)
• Eye pain, watery eyes, FB sensation
• +/‐ pain control (consider topical c fluorescein)
• +/‐ Abx: no proof they help, avoid gentamycinp y p g y
• Patching does not improve comfort or healing
• Refer if no improvement
Corneal foreign body• Try to remove by irrigation or dabbing cotton swab
• Per Schneider: beware of using q‐tip abrasion
• Consider topical anesthetic
• Consider calling/sending downstairs to opto
• Metallic foreign bodies can form rust ring, requiring g g, q gmicro‐debridement
• Tetanus?
![Page 8: Eyes ambulatory chief 2.pptx [Read-Only] - Santa … · Lids/lashes: Stye (hordeolum) • Chronic or acute infection of eyelash follicle ... Microsoft PowerPoint - Eyes ambulatory](https://reader042.pdfslide.us/reader042/viewer/2022031000/5b81bf1a7f8b9ae87c8cfd1f/html5/page/8.jpg)
2/11/2013
8
Contact lens overwear
• Take them out at night
Dry eye syndrome(keratoconjunctivitis sicca)
• Bilateral red, itchy eyes with gritty, sandy sensation, mild pain, intermittent watering. No moist tear film
• Review meds (anticholinergics, antihistamines, OCPs), Sjogren’s
• Rx: artificial tears (methylcellulose, hydroxycelloluse)
Episcleritis
• Limited, isolated patches of erythema, often wedge pattern often medial or lateral
• Mild to no pain
• Rheumatologic, idiopathic
• Tx: usually self‐limiting, artificial tears
Subconjunctival hemorrhage
• Trauma, coughing, s/p NSVD passenger
• Painless, “paintbrush”
• Counsel that resolution can take 2‐4 weeks
• If pain is present look for a cause (corneal?)• If pain is present, look for a cause (corneal?)
• If recurrent, w/u bleeding d/o, check INR
![Page 9: Eyes ambulatory chief 2.pptx [Read-Only] - Santa … · Lids/lashes: Stye (hordeolum) • Chronic or acute infection of eyelash follicle ... Microsoft PowerPoint - Eyes ambulatory](https://reader042.pdfslide.us/reader042/viewer/2022031000/5b81bf1a7f8b9ae87c8cfd1f/html5/page/9.jpg)
2/11/2013
9
Lids/lashes: Stye (hordeolum)• Chronic or acute infection of eyelash follicle
• Consider testing for DM if recurrent
• Tx: warm compresses, pull eyelash, +/‐ abx
Lids/lashes: Chalazion(Meibomian “cyst”)
• Painless lump, increasing in size over weeks
• Granulation tissue—trapped sebum
• Tx: spontaneous v. I+C by ophtho
![Page 10: Eyes ambulatory chief 2.pptx [Read-Only] - Santa … · Lids/lashes: Stye (hordeolum) • Chronic or acute infection of eyelash follicle ... Microsoft PowerPoint - Eyes ambulatory](https://reader042.pdfslide.us/reader042/viewer/2022031000/5b81bf1a7f8b9ae87c8cfd1f/html5/page/10.jpg)
2/11/2013
10
Lids/lashes: Blepharitis• Chronic or acute inflammation of eyelid margins, crusting, red swollen
• Look for seb derm, rosacea
• Tx: diluted baby shampoo soap• Tx: diluted baby shampoo, soap
• Abx: erythro or bacitracin
• Not necessarily red, but….
Pinguecula• Yellowish nodules (hyaline and lipid) on nasal or temporal conjunctiva
• Common after middle‐age
• Harmless, sometimes a cosmetic issueissue
Pterygium• Thickening and ingrowth of conjunctiva on to the cornea
• Hot, dry, dusty conditions predispose
• If impinging on iris refer:If impinging on iris, refer: may warrant surgical excision
![Page 11: Eyes ambulatory chief 2.pptx [Read-Only] - Santa … · Lids/lashes: Stye (hordeolum) • Chronic or acute infection of eyelash follicle ... Microsoft PowerPoint - Eyes ambulatory](https://reader042.pdfslide.us/reader042/viewer/2022031000/5b81bf1a7f8b9ae87c8cfd1f/html5/page/11.jpg)
2/11/2013
11
Cases…. Case 1: Painful Red Eye
• A 46‐year‐old man presented to the emergency department with unilateral pain in his left eye that began one day earlier. He had redness and a foreign body sensation. There were no vision changes, discharge, trauma, or recent upper respiratory tract g , , pp p ysymptoms.
• On examination, his pupils were reactive to light with normal ocular motor function. He had consensual photophobia. Slit lamp examination showed ciliaryflush and cell flaring, but no conjunctival injection. The patient was further evaluated with fluorescein staining
QuestionBased on the patient's history, physical examination, and microscopy findings, which one of the following is the most likely diagnosis?A. Foreign body.B. Fungal keratitis.C. Herpes keratitis.D. Sarcoidosis.
• The answer is C: herpes keratitis. Herpes simplex virus is one of the leading causes of infectious keratitis resulting in blindness. Herpes keratitis is the most common ocular form of herpes infection and usually presents as an infection of the superficial epithelium with dendritic lesions in this layer.1 Symptoms of herpes keratitis vary but may include pain, blurred vision, sensitivity to light, red eye, watery discharge, or foreign body sensation Recurrent episodes areforeign body sensation. Recurrent episodes are common.
• The diagnosis is made based on history and slit lamp examination.1 This patient's examination with f luorescein staining revealed a dendritic lesion (Figure 2). Laboratory testing is generally not indicated. Herpes keratitis is treated with antiviral therapy.2
• Patients with a foreign body may have excruciating pain, tearing, and a scratchy sensation with blinking. Slit lamp examination may reveal a foreign body in the anterior or posterior chamber. However, if the object is not present, fluorescein staining may demonstrate a corneal epithelial injury or defect.1
• Patients with fungal keratitis may have a history of trauma with vegetative matter, or long‐term steroid use.1,3Common symptoms include pain, red eye, foreign body sensation and discharge Typical slit light examinationsensation, and discharge. Typical slit light examination findings include a dry, gray, elevated infiltrate and satellite lesions. Diagnosis requires laboratory confirmation using a fungal culture.
• Ocular sarcoidosis can manifest before the presentation of systemic sarcoidosis. Uveitis is a common ocular manifestation of sarcoidosis.4 Examination shows redness in the corneal area. Patients present with bilateral ocular pain, photophobia, and decreased vision, and granuloma formation can be seen in the conjunctiva and uvea.
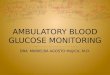
• Case 2: Acute Red Eye:
• A 28‐year‐old woman presented with a five‐day history of redness (see accompanyingfigure) and mild pain in her left eye. She hadnot experienced discharge, blurry vision, orphotophobia. The patient denied any historyp p p y yof trauma to the eye or participation in anoccupation or hobby that put her at risk of a foreign body injury. She did not wear contactlenses. On examination, her uncorrectedvision was 20/20 in both eyes.
![Page 12: Eyes ambulatory chief 2.pptx [Read-Only] - Santa … · Lids/lashes: Stye (hordeolum) • Chronic or acute infection of eyelash follicle ... Microsoft PowerPoint - Eyes ambulatory](https://reader042.pdfslide.us/reader042/viewer/2022031000/5b81bf1a7f8b9ae87c8cfd1f/html5/page/12.jpg)
2/11/2013
12
Based on the patient's history and physical examination, which one of the following is the most likely diagnosis?A. Perilimbal nevus.B. Pingueculitis.C. Pterygium.D. Subconjunctival foreign body.E. Viral conjunctivitis.
• The answer is B: pingueculitis. A pinguecula is a common eye lesion. The lesion is a small, yellowish‐white, elevated mass on the bulbar conjunctiva located on either side of the cornea, typically at the 3 and 9 o'clock positions. Sometimes the lesion becomes inflamed (pingueculitis).
• Pingueculae are more common on the nasal side than the temporal side. The lesions may gradually enlarge over time but do not grow onto the cornea. The prevalence increases with age, and pingueculae occur in almost all persons older than 80 years.1
• Pingueculae are likely actinic in origin, caused by damage from exposure to ultraviolet (UV) rays.
• The treatment of pingueculitis involves the use of artificial tears and/or mild topical steroids; topical nonsteroidal anti‐inflammatory ophthalmic solutions (e.g., ketorolac [Acular], diclofenac [Voltaren], flurbiprofen [Ocufen]) are also effective.
Ocular Ultrasound…. Ocular Ultrasound….
• Retinal detachment
• Increased ICP?
• Vitreous hemorrhage
• Foreign body
• PERRL?
Thank you! References:
• www.AAFP.org: Photo Quiz: Acute Red Eye nad Painful Red Eye
• Bankes, J. Clinical Ophthalmology: A Color Text and Atlas. 1994
• Cronau, Holly, Kankanala, R, et al. Diagnosis and Management of Red Eye in Primary Care Am Famof Red Eye in Primary Care, Am FamPhysician. 2010 Jan 15;81(2):137‐144.
• Jacobs, D, Trobe, J, et al. Evaluation of the red eye. UptoDate, last updated 11/30/12
• Schneider, D.
![Page 13: Eyes ambulatory chief 2.pptx [Read-Only] - Santa … · Lids/lashes: Stye (hordeolum) • Chronic or acute infection of eyelash follicle ... Microsoft PowerPoint - Eyes ambulatory](https://reader042.pdfslide.us/reader042/viewer/2022031000/5b81bf1a7f8b9ae87c8cfd1f/html5/page/13.jpg)
2/11/2013
13