Embed Size (px)
Citation preview

Eyelid, Periorbital, and Ocular Surface
Temperature Differences Between
Sjögren’s Eyes and Asymptomatic Controls
Holly B. Hindman1,2, Christine Callan1,2, Ranjini Kottaiyan1,2, Kerstin Abreau3, Aizhong Zhang4,5, James Aquavella1,2, James Zavislan4,5
1Flaum Eye Institute, 2University of Rochester, 3Juniata College, 4Center for Visual Science, 5Institute of Optics
Background
Sjögren’s Syndrome (SS) is an autoimmune mediated inflammatory disorder characterized by dry eyes and mouth. Infrared (IR) thermography is promising technology for ocular surface investigations as it is non-invasive and has high accuracy. IR imaging has been previously used to differentiate dry and normal eyes on the basis of ocular surface temperatures.1, 2 Prior work in our laboratory has demonstrated that subjects with Sjögren’s Syndrome experience increased cooling of their ocular surfaces over an interblink interval. 3 The current study also compared eyelid and periorbital skin temperatures between SS and healthy control subjects to determine if the temperatures of the surrounding tissues are also relevant in understanding ocular surface temperature differences between these groups.4
Purpose
To compare the ocular surface, eyelid, and periorbital skin temperatures in
subjects affected by dry eye resulting from Sjögren’s Syndrome with healthy
controls within a controlled environmental chamber.
Methods
Subjects:
Data were collected from 10 subjects (20 eyes) with SS, and 10 age-matched,
asymptomatic, control subjects (20 eyes). All patients included in the SS group
fulfilled the AECG criteria for classification of SS.5 The control group was
comprised of patients that reported no subjective dry eye symptoms, and had no
previous diagnosis of SS.
Methods:Measurements were taken in a climate controlled chamber, with standardized conditions set to 75º F and 40% RH. Images were taken over 5-second blink intervals using an infrared thermal camera (Thermovision SC325, FLIR System). Post-image processing was completed utilizing custom written Matlab code (Mathworks, Inc.).
Methods (continued)
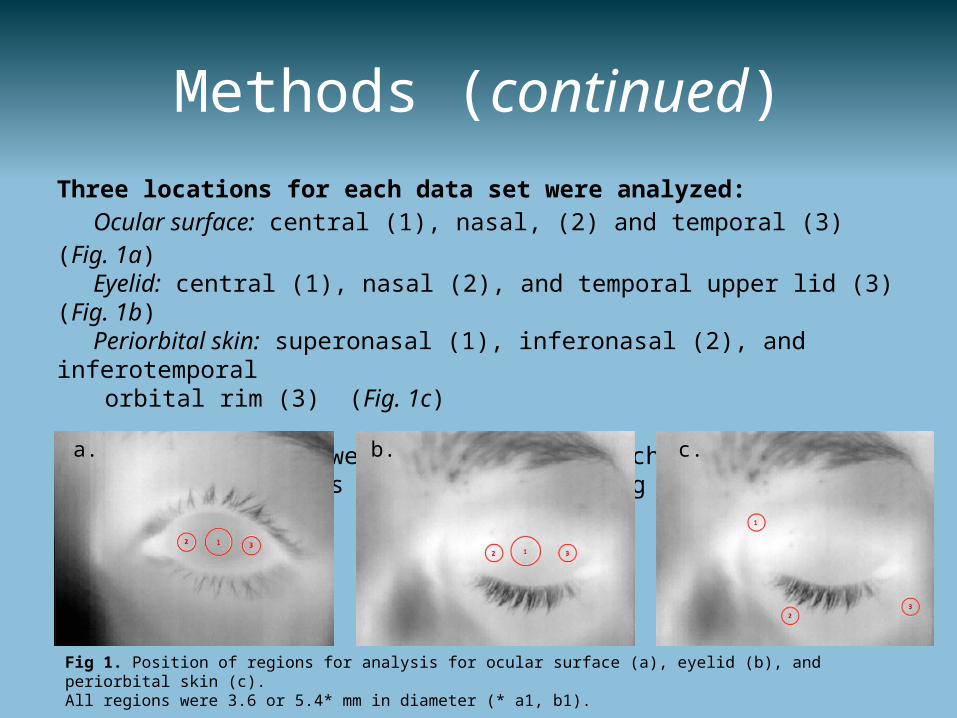
Three locations for each data set were analyzed:Ocular surface: central (1), nasal, (2) and temporal (3) (Fig. 1a)Eyelid: central (1), nasal (2), and temporal upper lid (3) (Fig. 1b)Periorbital skin: superonasal (1), inferonasal (2), and inferotemporal
orbital rim (3) (Fig. 1c)
Temperature values were averaged over each region. Statistical analyses were performed using t-tests.
Fig 1. Position of regions for analysis for ocular surface (a), eyelid (b), and periorbital skin (c). All regions were 3.6 or 5.4* mm in diameter (* a1, b1).
a. b. c.
Results
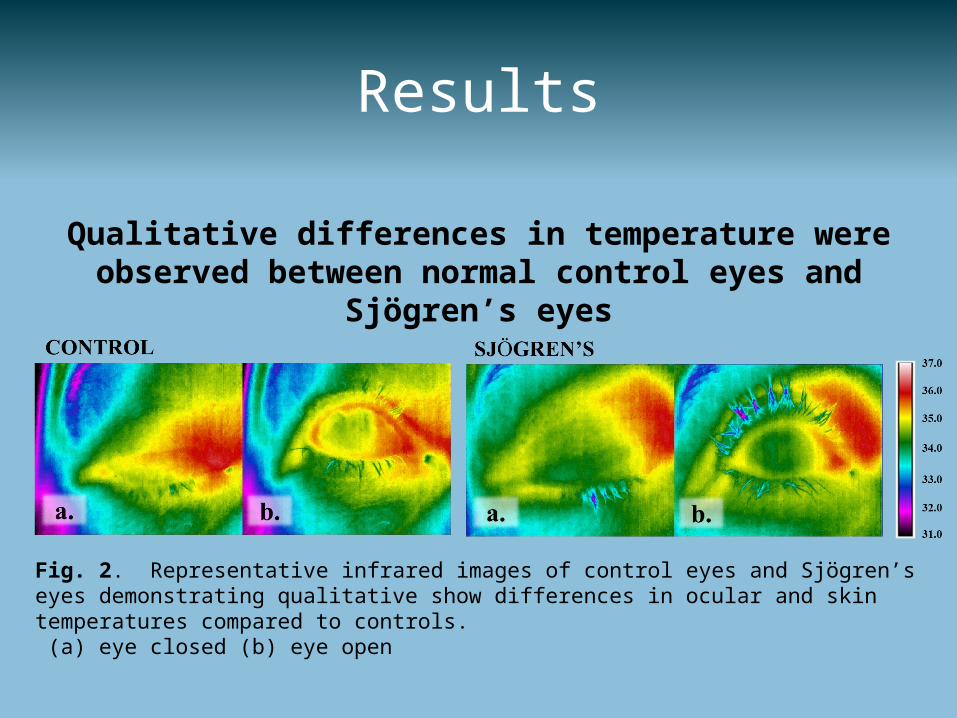
Qualitative differences in temperature were observed between normal control eyes and Sjögren’s eyes
Fig. 2. Representative infrared images of control eyes and Sjögren’s eyes demonstrating qualitative show differences in ocular and skin temperatures compared to controls. (a) eye closed (b) eye open
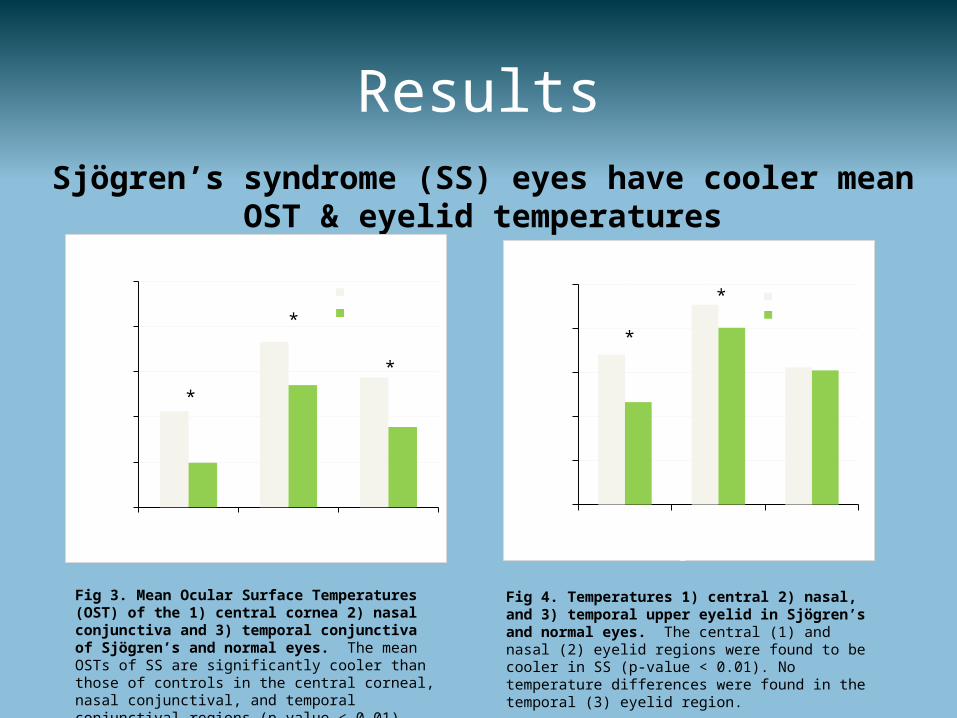
ResultsSjögren’s syndrome (SS) eyes have cooler mean OST & eyelid
temperatures
Fig 3. Mean Ocular Surface Temperatures (OST) of the 1) central cornea 2) nasal conjunctiva and 3) temporal conjunctiva of Sjögren’s and normal eyes. The mean OSTs of SS are significantly cooler than those of controls in the central corneal, nasal conjunctival, and temporal conjunctival regions (p-value < 0.01).
Fig 4. Temperatures 1) central 2) nasal, and 3) temporal upper eyelid in Sjögren’s and normal eyes. The central (1) and nasal (2) eyelid regions were found to be cooler in SS (p-value < 0.01). No temperature differences were found in the temporal (3) eyelid region.
Central Nasal Temporal34
34.4
34.8
35.2
35.6
36Upper Eyelid
Normal Sjögren's
Region of interest
Tem
pera
ture
(°C) *
*
Central Nasal Temporal34
34.4
34.8
35.2
35.6
36Ocular Surface
Normal Sjögren's
Region of Interest
Tem
pera
ture
(°C
)
*
*
*
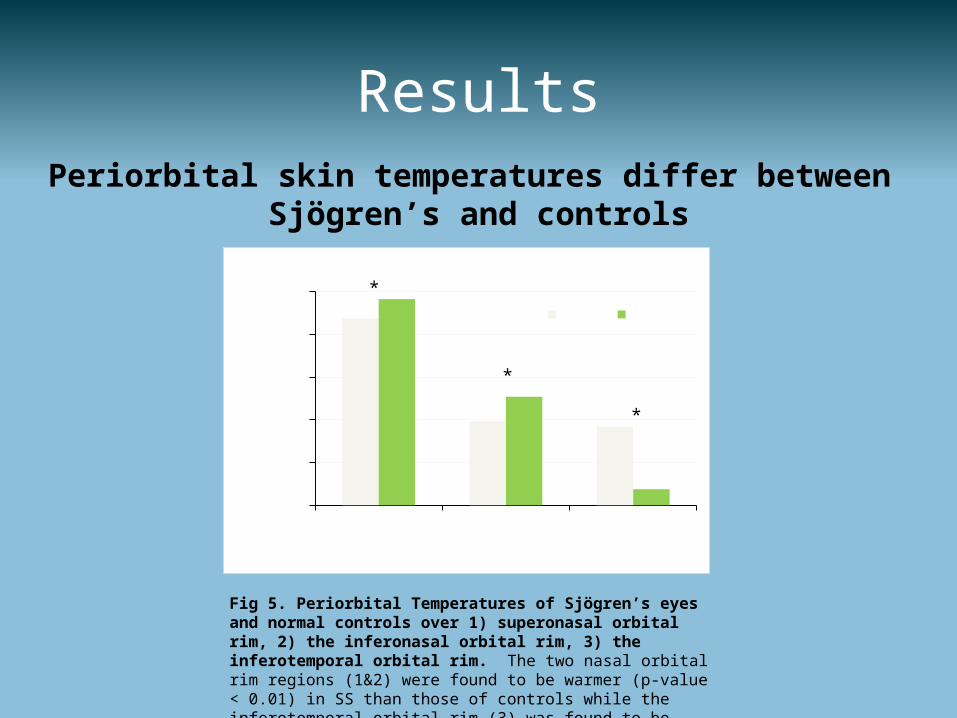
ResultsPeriorbital skin temperatures differ between
Sjögren’s and controls
Fig 5. Periorbital Temperatures of Sjögren’s eyes and normal controls over 1) superonasal orbital rim, 2) the inferonasal orbital rim, 3) the inferotemporal orbital rim. The two nasal orbital rim regions (1&2) were found to be warmer (p-value < 0.01) in SS than those of controls while the inferotemporal orbital rim (3) was found to be cooler in SS (p-value < 0.01).
Supero- nasal
Infero- nasal
Infero- temporal
34
34.4
34.8
35.2
35.6
36Periorbital Skin
Normal Sjögren's
Region of interest
Tem
pera
ture
(°C)
*
*
*
Supplemental Graphs
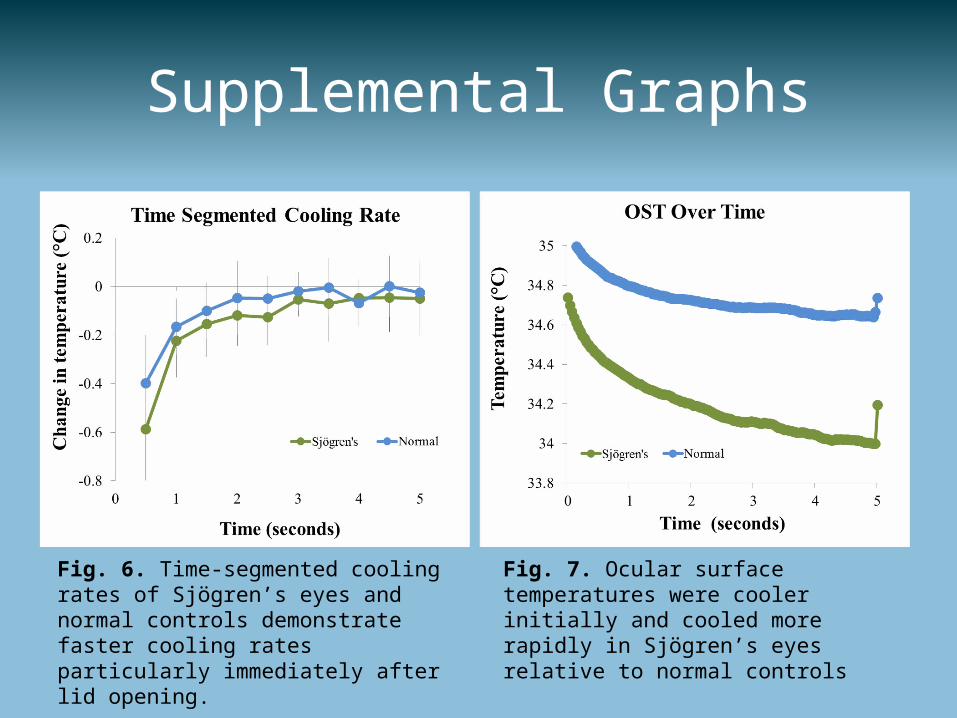
Fig. 6. Time-segmented cooling rates of Sjögren’s eyes and normal controls demonstrate faster cooling rates particularly immediately after lid opening.
Fig. 7. Ocular surface temperatures were cooler initially and cooled more rapidly in Sjögren’s eyes relative to normal controls
Discussion
• Our results are consistent with other reports in that Sjögren’s eyes hadcooler ocular surface temperatures and faster cooling rates relative to normal eyes.
• Our study also measured for the first time, the temperatures of the surrounding tissues and found that Sjögren’s eyes have cooler eyelids and other periorbital temperature differences from normals.
• Temperatures of the surrounding structures likely impact the ocular surface temperature (e.g. cooler eyelid temperatures provide a cooler “thermal pulse”6 with each blink to the ocular surface which may account for the cooler OST upon eyelid opening of SS patients).
• Lid temperature may impact initial ocular surface temperature whereas the change in OST observed during the interblink period may be more affected by tear film evaporation.
• Additional research is needed to better understand the identified differences in temperature and their potential pathophysiologic underpinnings.
Conclusion
In this study we have demonstrated significant differences in lid and periorbital temperatures between Sjögren’s syndrome eyes and age-matched normal controls. Given the transfer of heat by conduction and proximity of these tissues to the ocular surface, the temperature differences in the lids and periorbital likely play an important role in the initial ocular surface temperature differences identified.
Acknowledgements: Funding was provided by: RPB, CVS training grant T32 EY 007125
No Financial Disclosures
References:1 Azharuddin M, et al. Thermal fluctuation based study of aqueous deficient dry eyes by non-invasive thermal imaging.
Exp Eye Res. 2014;120:97-102.2 Kottaiyan R, et al. Integrated Multimodal Metrology for Objective and Noninvasive Tear Evaluation. Ocul Surf. 2012;
10:43-50.3 Kottaiyan R, et al. Tear Dynamic Measurements in the Differentiation of Sjogren’s Dry Eye from Non-Sjogren’s Dry
Eye. ARVO 2011.4 Chang, Hsiao, & Liao. Application of digital infrared thermal imaging in determining inflammatory state and follow-up
effect of methyprednisolone pulse therapy in patients with Grave’s opthalmopathy. Graefes Arch Clin Opthalmol 2007;246:45-49.
5 Goules AV, et al. Classification criteria of Sjögren's syndrome. J Autoimmun. 2014; 48-49; 42-45.6 Zhang, Aizhong. Thermal analysis of dry eye subjects and the thermal impulse perturbation model of ocular surface.
Manuscript submitted for publication. 2014.