Embed Size (px)
DESCRIPTION
Eye Care Benefits Center What we do and why it is critical to Optometrists’ success. Colorado Optometric Association Coding & Billing Seminar October 23, 2005. ECBC: What we do for you. Managed Care Marketing Initiative Coding education, initiatives and support - PowerPoint PPT Presentation
Citation preview
1
Eye Care Benefits CenterWhat we do and why it is critical to
Optometrists’ success
Colorado Optometric AssociationCoding & Billing Seminar
October 23, 2005

2
ECBC: What we do for youManaged Care Marketing InitiativeCoding education, initiatives and supportMonitoring trends in health care and
third party payment systemsImprove exchange of information with
statesPosition Optometry with healthcare
stakeholders

3
Managed Care Marketing Initiative: What it is.
Expanding the presence of Optometry in medical plans administered by managed care organizations (MCOs) and employers
Convert MCOs who exclude or underutilize Optometrists to full inclusion in their networks
Persuade ERISA plans managed by large employers to reimburse for medical services provided by Optometrists
4
Managed Care Marketing Initiative: How we do it.
Target identificationResearch and validation
Confirm the issue/exclusion ERISA v. MCO v. payment
Determine scope of impact Local v. regional v. national Small v. large
Identify contacts
5
Managed Care Marketing Initiative: How we do it.
Secure Meeting Leverage Aon contacts Utilize local contacts where available
Prepare for meeting Research organization and background Identify and prepare team
Aon, ECBC representative and local Optometrist
Customize presentation and prepare proof documents

6
Well PreparedSeek to establish partnership
Understand MCO goals Demonstrate how Optometrists help meet
goalsThoroughly researchedVetted and proven documents
Power Point Presentation Emergency Room and cost studies Facts and relevant stories
Follow up
Managed Care Marketing Initiative: Style and Approach

7
Managed Care Marketing Initiative: Who does it
Eye Care Benefit Center volunteersTom Weaver DMD (AOA staff)Aon ConsultingLocal Optometrists from the
impacted State

8
Managed Care Marketing Initiative: Who does it
ECBC Dr. Mark Hennen, Chair Dr. Randy Fincher Dr. Kathleen Goff Dr. Greg Kraupa Dr. Mark Lee Dr. Doug Morrow Dr. Bill Rivard Dr. Joe Studebaker Dr. Mike Todd Dr. Rebecca Wartman
9
Managed Care Marketing Initiative: Aon Consulting
One of the largest employee benefit consulting firms
We know the managed care organizations
We understand the dynamics of health care benefits
MCOs are usually willing to meet with us We understand the needs of large
employers and MCOs

10
Managed Care Marketing Initiative: Targets
National, regional or large local PPOs
Large, multi-state employers (ERISA)
Medicare Advantage plans (newly added category)
Federal plans (cooperating with Federal Relations Committee-FRC)

11
Managed Care Marketing Initiative: SuccessesOptometrists now have access to reimbursed
medical care for 29.4 million additional patientsNotable Colorado Successes

12
Managed Care Marketing Initiative: Reasons for Exclusion
MCOs/Employers typically have excluded Optometrists due to: They do not understand what we do They think it will increase claims costs They do not want to spend resources
on credentialing “They always have done it this way”

13
Managed Care Marketing Initiative: Critical Success Factors
Liaison Program to identify targets ECBC representative maintains
contact with state appointed liaison Primary communication method
regarding managed care issues Ensures best effort by Optometry to
promote inclusion Liaison program needs full ED/state
leadership support and commitment

14
State Liaison Roles and Responsibilities
Knowledgeable of state managed care issues affecting all parts of the state
Familiar with coding issuesResponsive to/from ECBC and StateConnected to state leadershipWilling to attend national meetingsLongevity of service

15
Trends in Third Party PaymentContinued consolidation of payorsPay for performance
Driving quality to reduce cost increasesConsumer Directed Health Care
HSAs and HRAs Empowered consumer
Medicare Reform Prescription drug Advantage: HMOs and PPOs

16
What is driving change in health care?
COST!!!!

17
The Widening Gap
8.5%
5.3%
13.9%
12.0%
0.8%
10.9% 11.2%
0%
2%
4%
6%
8%
10%
12%
14%
16%
1988 1993 1996 1999 2001 2003 2004
Premiums Workers' Earnings Inflation
Increases in Premiums vs. Other Indicators
Source: Kaiser/HRET and KPMG
18
The Widening GapAt current trend rates of 12% and
household income growth rate of 4.6%, health benefits as a percent of total compensation will increase from 19% in 2003 to 63% in 2021
Household healthcare expenditures will increase to 17% of income from 5%
Source: Kaiser/HRET and KPMG
19
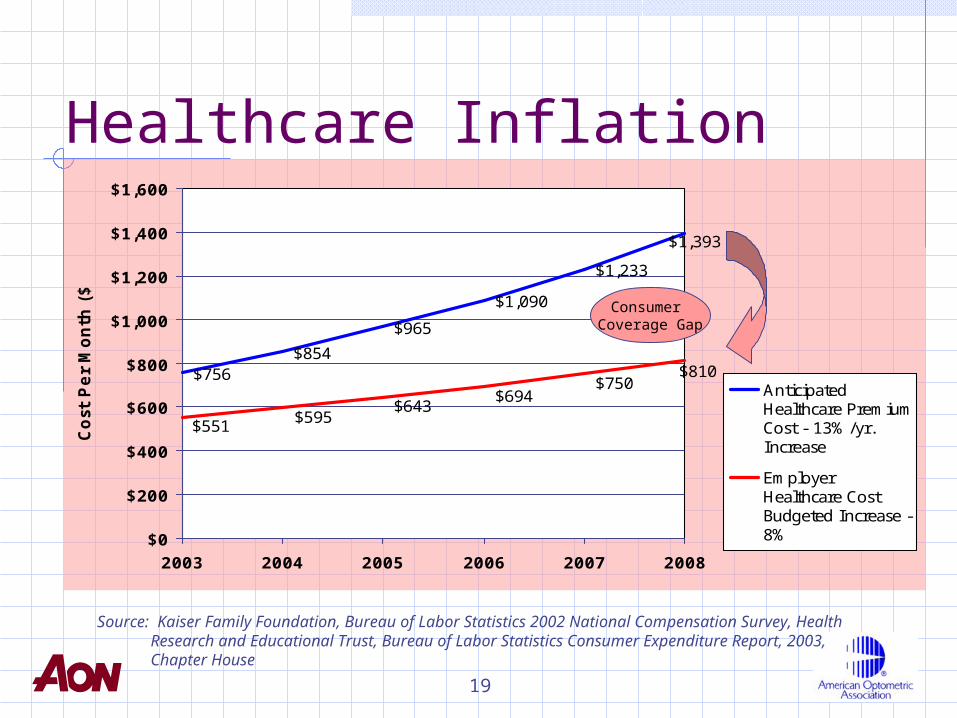
Healthcare Inflation
$756$854
$965
$1,090
$1,233
$1,393
$810$750
$694$643
$595$551
$0
$200
$400
$600
$800
$1,000
$1,200
$1,400
$1,600
2003 2004 2005 2006 2007 2008
Cost
Per
Month
($)
AnticipatedHealthcare PremiumCost - 13%/yr.Increase
EmployerHealthcare CostBudgeted Increase -8%
Consumer Coverage Gap
Source: Kaiser Family Foundation, Bureau of Labor Statistics 2002 National Compensation Survey, Health Research and Educational Trust, Bureau of Labor Statistics Consumer Expenditure Report, 2003, Chapter House

20
Driving Health Care QualityPay for performance
“Premier” physicians at UHC Network within a network More than 35 health plans utilizing
Electronic health records Implemented effectively at Veterans
Affairs Intended to eliminate errors VISTA is now available to any practice

21
Growth of HRAs and HSAsHSAs were legislated December 2003
Jan. 2005: over 600,000 participants Mid 2005: over 1 million participants
HRA available around 2001 Jan. 2005:2.6 million participants Mid 2005: over 3 million participants
Combined CDHP membership anticipated by January 2006: 6 million
Source: American Association of Health Plans, Inside Consumer Directed Healthcare

22
Expansion of Consumer Directed Health Care and HSAsMCOs now committed to marketplace
UHC purchased Definity UHC only offering HSA/CDHC to own staff Anthem purchased Lumenos
Federal Government offering HDHP/HSAs
Much of HSA growth coming from small employers
23
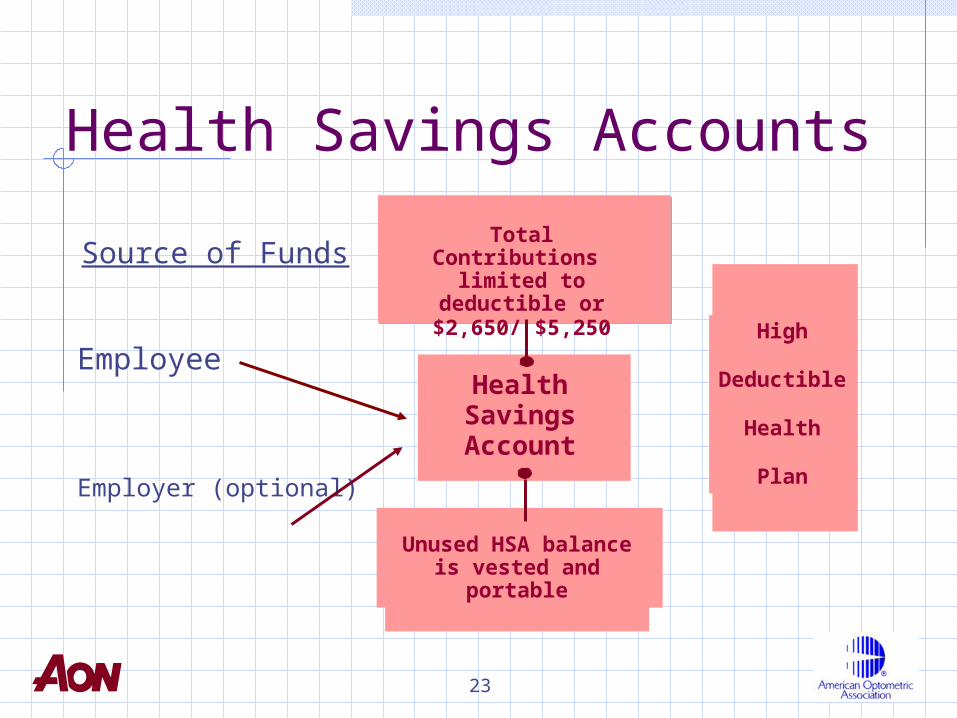
Health Savings Accounts
Source of Funds
HealthSavingsAccount
High
Deductible
Health
Plan
Employee
Employer (optional)
Total Contributions limited to deductible or
$2,650/ $5,250
Unused HSA balance is vested and portable

24
Empowered Consumer with Consumer Driven PlansAetna will provide actual allowed
office visit charge amountUHC is identifying “Premier”
physiciansParticipants have ready access to
peer reviewed health care informationMCOs and employers are driving
hospitals to measure outcomes and reduce errors
25
Impact on OptometryMore self-pay by patients. Patients may:
still use network doctors for discounts rely more on coupons for savings be willing to pay full cost for outstanding
value/service insist on negotiating fees
Direct-to-consumer marketing may become even more critical
More billing challenges

26
Impact on OptometryCompete on basis of cost, outcomes
and serviceCollect and monitor dataDevelop performance and quality
standards and strive to meet them
Source: Chapter House
27
Medicare Advantage
ECBC and FRC monitoring Medicare Advantage development
Aggressively pursuing plans that exclude ODs
Adopting successful Managed Care Marketing Initiative for discriminating Medicare Advantage plans

28
Impact on OptometryConsider joining Medicare Advantage
networks to provide medical and/or vision services Some networks may resist including
Optometrists
Fewer Traditional Medicare patientsDifferent rules than original MedicareBe aware, this may only be temporary
29
A Closer Look at Colorado

30
Trends in ColoradoHealthcare
Consolidation & ChangeUHC purchases PacifiCareWellPoint CA purchases AnthemGreat West HealthCare wins State of
CO contract and selects AvisisCigna drops Opticare for routine
vision in favor of VSP
31
Trends in ColoradoHealthcare – LegislativeHouse Bill 04-1354 - Uniform
Credentialing New 28 page credentialing application
Senate Bill 37 – 2nd Level Appeals Mandatory to Carriers –Voluntary to
Members
House Bill 05-1165 Insurance Benefit Assignment
Carriers are required to pay Claims directly to a Provider who holds assignment regardless of being In or Out-of-Network.
32
Trends in ColoradoVision Care
Voluntary Vision PlansColorado Vision Care Direct
Discount Plans are popping upeverywhere
Wal-Mart Vision InsurancePlans covering routine vision and
Safety Programs are being introduced

33





























