Embed Size (px)
Citation preview

Extracranial Head and NeckInfections
Denise Jaworsky, MDa, Steven Reynolds, MD, FRCPCb,c,d,Anthony W. Chow, MD, FACP, FRCPCe,*
KEYWORDS
� Submandibular space infection � Lateral pharyngeal space infection� Retropharyngeal space infection � Danger space infection� Prevertebral space infection � Mediastinitis � Sinusitis � Ludwig angina
KEY POINTS
� Management of extracranial head and neck infections is often 2-pronged, involving appro-priate antibiotic therapy and source control such as surgical drainage.
� Most extracranial head and neck infections are either odontogenic or rhinogenic, and usu-ally polymicrobial; initial therapy should include agents active against oral aerobes and an-aerobes (both b-lactamase-producing anaerobic and facultative gram-negative bacilli.
� Methicillin-resistant Staphylococcus aureus and fungal causes should also be considered,
INTRODUCTION
The head and neck contain several potential spaces that can become infected and canresult in life-threatening complications, including airway compromise, neurologicsequelae, and dissemination of infection. Many early presentations are subtle andmay be missed even by an astute clinician. This article outlines infections in the sub-mandibular, lateral pharyngeal, retropharyngeal, danger, and prevertebral spaces, inconjunction with infections of the sinuses and mediastinum. By understanding theanatomy and pathophysiology, the reader will gain insight into the rationale for varioustherapeutic options.
depending on local epidemiology and patients’ risk factors.
Funding Sources: None.Conflicts of Interest: None.a Department of Medicine, University of British Columbia, 2775 Laurel Street, 10th Floor,Vancouver, British Columbia V5Z 1M9, Canada; b Division of Critical Care, Department ofMedicine, University of British Columbia, British Columbia, Canada; c Division of InfectiousDiseases, Department of Medicine, University of British Columbia, British Columbia, Canada;d Intensive Care Unit, Department of Critical Care, Royal Columbian Hospital, 330 ColumbiaStreet, New Westminster, British Columbia V3L 3W7, Canada; e Division of Infectious Diseases,Department of Medicine, Vancouver Hospital, University of British Columbia, 2773 HeatherStreet, Vancouver, British Columbia V5Z 3J5, Canada* Corresponding author.E-mail address: [email protected]
Crit Care Clin 29 (2013) 443–463http://dx.doi.org/10.1016/j.ccc.2013.03.003 criticalcare.theclinics.com0749-0704/13/$ – see front matter � 2013 Elsevier Inc. All rights reserved.
Jaworsky et al444
INFECTIONS OF THE SUBMANDIBULAR SPACEAnatomy and Pathophysiology
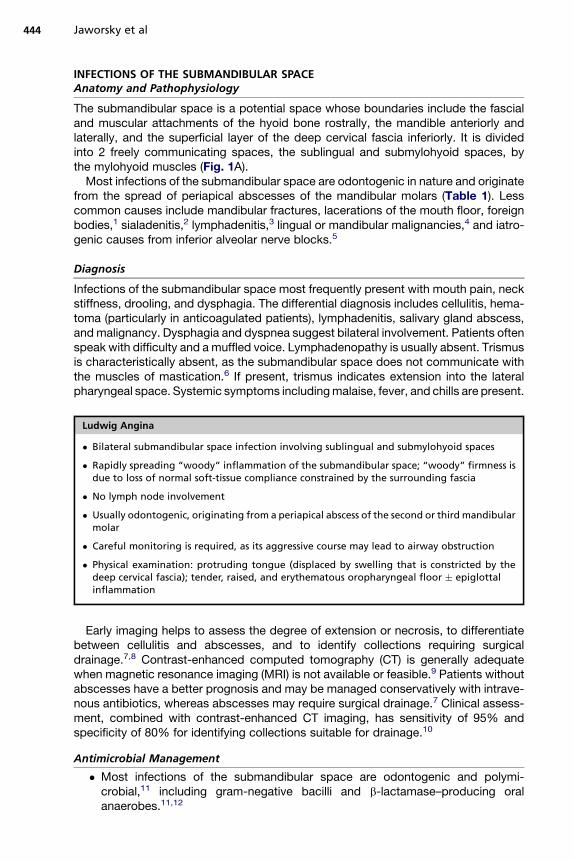
The submandibular space is a potential space whose boundaries include the fascialand muscular attachments of the hyoid bone rostrally, the mandible anteriorly andlaterally, and the superficial layer of the deep cervical fascia inferiorly. It is dividedinto 2 freely communicating spaces, the sublingual and submylohyoid spaces, bythe mylohyoid muscles (Fig. 1A).Most infections of the submandibular space are odontogenic in nature and originate
from the spread of periapical abscesses of the mandibular molars (Table 1). Lesscommon causes include mandibular fractures, lacerations of the mouth floor, foreignbodies,1 sialadenitis,2 lymphadenitis,3 lingual or mandibular malignancies,4 and iatro-genic causes from inferior alveolar nerve blocks.5
Diagnosis
Infections of the submandibular space most frequently present with mouth pain, neckstiffness, drooling, and dysphagia. The differential diagnosis includes cellulitis, hema-toma (particularly in anticoagulated patients), lymphadenitis, salivary gland abscess,and malignancy. Dysphagia and dyspnea suggest bilateral involvement. Patients oftenspeak with difficulty and a muffled voice. Lymphadenopathy is usually absent. Trismusis characteristically absent, as the submandibular space does not communicate withthe muscles of mastication.6 If present, trismus indicates extension into the lateralpharyngeal space. Systemic symptoms includingmalaise, fever, and chills are present.
Ludwig Angina
� Bilateral submandibular space infection involving sublingual and submylohyoid spaces
� Rapidly spreading “woody” inflammation of the submandibular space; “woody” firmness isdue to loss of normal soft-tissue compliance constrained by the surrounding fascia
� No lymph node involvement
� Usually odontogenic, originating from a periapical abscess of the second or third mandibularmolar
� Careful monitoring is required, as its aggressive course may lead to airway obstruction
� Physical examination: protruding tongue (displaced by swelling that is constricted by thedeep cervical fascia); tender, raised, and erythematous oropharyngeal floor � epiglottalinflammation
Early imaging helps to assess the degree of extension or necrosis, to differentiatebetween cellulitis and abscesses, and to identify collections requiring surgicaldrainage.7,8 Contrast-enhanced computed tomography (CT) is generally adequatewhen magnetic resonance imaging (MRI) is not available or feasible.9 Patients withoutabscesses have a better prognosis and may be managed conservatively with intrave-nous antibiotics, whereas abscesses may require surgical drainage.7 Clinical assess-ment, combined with contrast-enhanced CT imaging, has sensitivity of 95% andspecificity of 80% for identifying collections suitable for drainage.10
Antimicrobial Management
� Most infections of the submandibular space are odontogenic and polymi-crobial,11 including gram-negative bacilli and b-lactamase–producing oralanaerobes.11,12
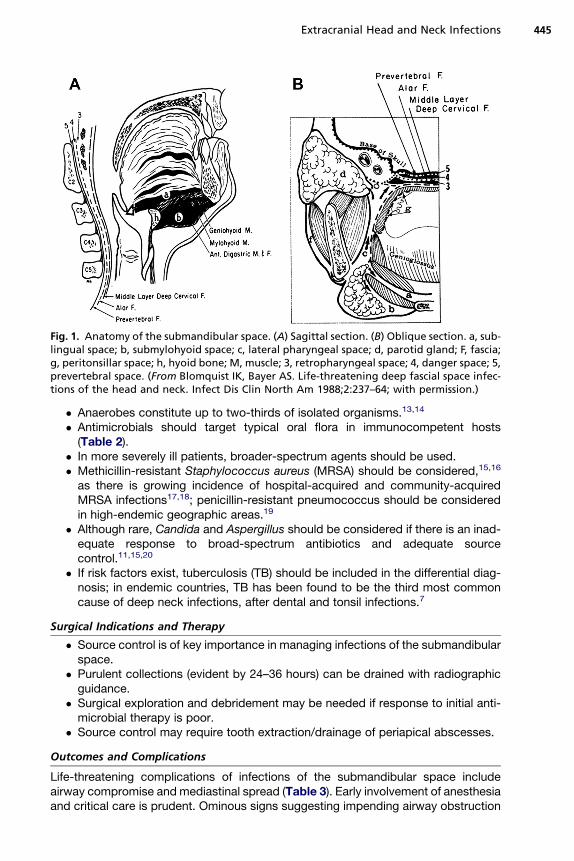
Fig. 1. Anatomy of the submandibular space. (A) Sagittal section. (B) Oblique section. a, sub-lingual space; b, submylohyoid space; c, lateral pharyngeal space; d, parotid gland; F, fascia;g, peritonsillar space; h, hyoid bone; M, muscle; 3, retropharyngeal space; 4, danger space; 5,prevertebral space. (From Blomquist IK, Bayer AS. Life-threatening deep fascial space infec-tions of the head and neck. Infect Dis Clin North Am 1988;2:237–64; with permission.)
Extracranial Head and Neck Infections 445
� Anaerobes constitute up to two-thirds of isolated organisms.13,14
� Antimicrobials should target typical oral flora in immunocompetent hosts(Table 2).
� In more severely ill patients, broader-spectrum agents should be used.� Methicillin-resistant Staphylococcus aureus (MRSA) should be considered,15,16
as there is growing incidence of hospital-acquired and community-acquiredMRSA infections17,18; penicillin-resistant pneumococcus should be consideredin high-endemic geographic areas.19
� Although rare, Candida and Aspergillus should be considered if there is an inad-equate response to broad-spectrum antibiotics and adequate sourcecontrol.11,15,20
� If risk factors exist, tuberculosis (TB) should be included in the differential diag-nosis; in endemic countries, TB has been found to be the third most commoncause of deep neck infections, after dental and tonsil infections.7
Surgical Indications and Therapy
� Source control is of key importance in managing infections of the submandibularspace.
� Purulent collections (evident by 24–36 hours) can be drained with radiographicguidance.
� Surgical exploration and debridement may be needed if response to initial anti-microbial therapy is poor.
� Source control may require tooth extraction/drainage of periapical abscesses.
Outcomes and Complications
Life-threatening complications of infections of the submandibular space includeairway compromise and mediastinal spread (Table 3). Early involvement of anesthesiaand critical care is prudent. Ominous signs suggesting impending airway obstruction
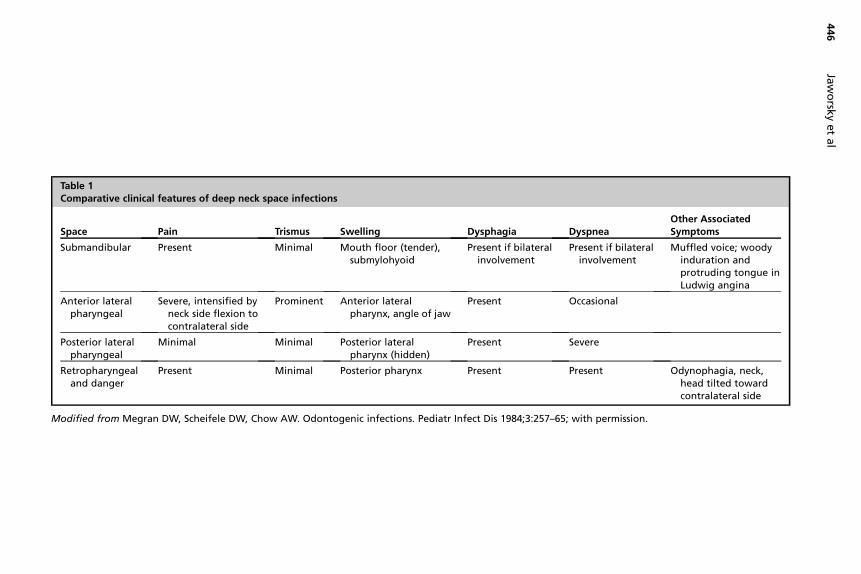
Table 1Comparative clinical features of deep neck space infections
Space Pain Trismus Swelling Dysphagia DyspneaOther AssociatedSymptoms
Submandibular Present Minimal Mouth floor (tender),submylohyoid
Present if bilateralinvolvement
Present if bilateralinvolvement
Muffled voice; woodyinduration andprotruding tongue inLudwig angina
Anterior lateralpharyngeal
Severe, intensified byneck side flexion tocontralateral side
Prominent Anterior lateralpharynx, angle of jaw
Present Occasional
Posterior lateralpharyngeal
Minimal Minimal Posterior lateralpharynx (hidden)
Present Severe
Retropharyngealand danger
Present Minimal Posterior pharynx Present Present Odynophagia, neck,head tilted towardcontralateral side
Modified from Megran DW, Scheifele DW, Chow AW. Odontogenic infections. Pediatr Infect Dis 1984;3:257–65; with permission.
Jaworsk
yetal
446
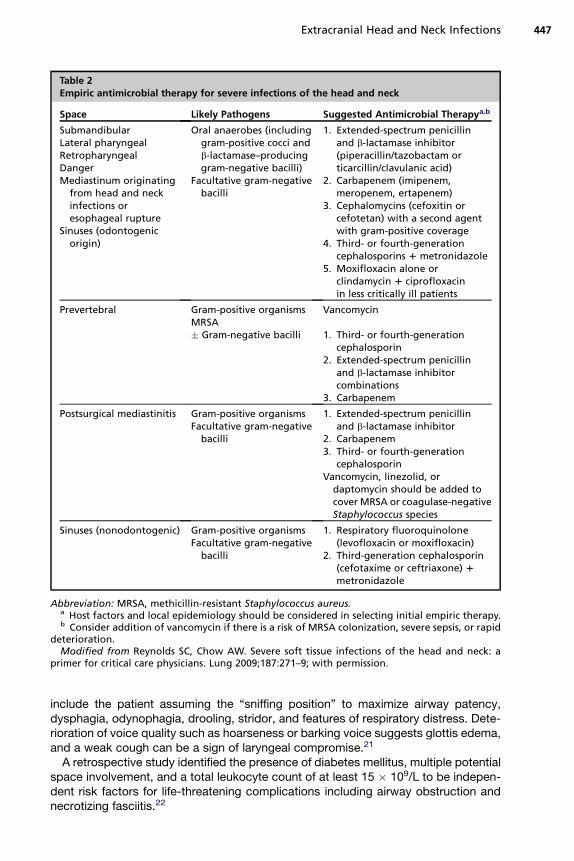
Table 2Empiric antimicrobial therapy for severe infections of the head and neck
Space Likely Pathogens Suggested Antimicrobial Therapya,b
SubmandibularLateral pharyngealRetropharyngealDangerMediastinum originating
from head and neckinfections oresophageal rupture
Sinuses (odontogenicorigin)
Oral anaerobes (includinggram-positive cocci andb-lactamase–producinggram-negative bacilli)
Facultative gram-negativebacilli
1. Extended-spectrum penicillinand b-lactamase inhibitor(piperacillin/tazobactam orticarcillin/clavulanic acid)
2. Carbapenem (imipenem,meropenem, ertapenem)
3. Cephalomycins (cefoxitin orcefotetan) with a second agentwith gram-positive coverage
4. Third- or fourth-generationcephalosporins 1 metronidazole
5. Moxifloxacin alone orclindamycin 1 ciprofloxacinin less critically ill patients
Prevertebral Gram-positive organismsMRSA
Vancomycin
� Gram-negative bacilli 1. Third- or fourth-generationcephalosporin
2. Extended-spectrum penicillinand b-lactamase inhibitorcombinations
3. Carbapenem
Postsurgical mediastinitis Gram-positive organismsFacultative gram-negative
bacilli
1. Extended-spectrum penicillinand b-lactamase inhibitor
2. Carbapenem3. Third- or fourth-generation
cephalosporinVancomycin, linezolid, or
daptomycin should be added tocover MRSA or coagulase-negativeStaphylococcus species
Sinuses (nonodontogenic) Gram-positive organismsFacultative gram-negative
bacilli
1. Respiratory fluoroquinolone(levofloxacin or moxifloxacin)
2. Third-generation cephalosporin(cefotaxime or ceftriaxone) 1metronidazole
Abbreviation: MRSA, methicillin-resistant Staphylococcus aureus.a Host factors and local epidemiology should be considered in selecting initial empiric therapy.b Consider addition of vancomycin if there is a risk of MRSA colonization, severe sepsis, or rapid
deterioration.Modified from Reynolds SC, Chow AW. Severe soft tissue infections of the head and neck: a
primer for critical care physicians. Lung 2009;187:271–9; with permission.
Extracranial Head and Neck Infections 447
include the patient assuming the “sniffing position” to maximize airway patency,dysphagia, odynophagia, drooling, stridor, and features of respiratory distress. Dete-rioration of voice quality such as hoarseness or barking voice suggests glottis edema,and a weak cough can be a sign of laryngeal compromise.21
A retrospective study identified the presence of diabetes mellitus, multiple potentialspace involvement, and a total leukocyte count of at least 15 � 109/L to be indepen-dent risk factors for life-threatening complications including airway obstruction andnecrotizing fasciitis.22
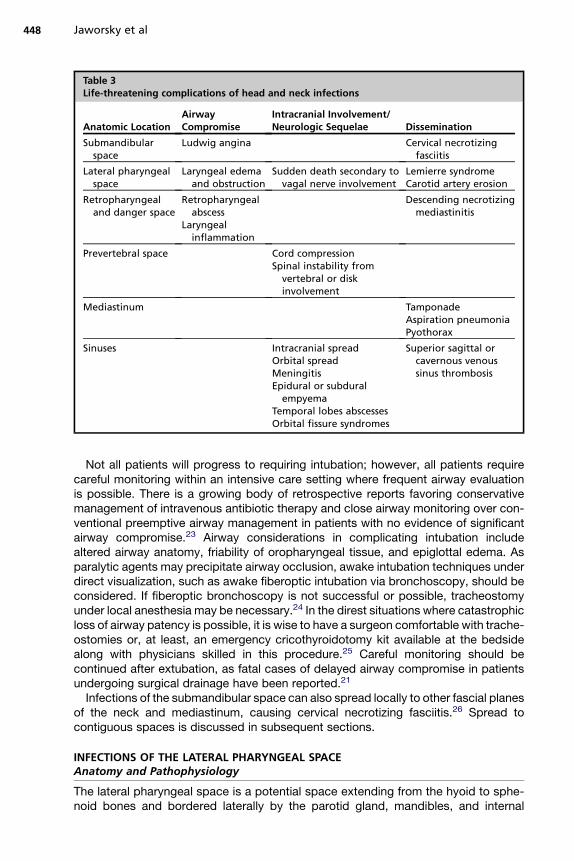
Table 3Life-threatening complications of head and neck infections
Anatomic LocationAirwayCompromise
Intracranial Involvement/Neurologic Sequelae Dissemination
Submandibularspace
Ludwig angina Cervical necrotizingfasciitis
Lateral pharyngealspace
Laryngeal edemaand obstruction
Sudden death secondary tovagal nerve involvement
Lemierre syndromeCarotid artery erosion
Retropharyngealand danger space
Retropharyngealabscess
Laryngealinflammation
Descending necrotizingmediastinitis
Prevertebral space Cord compressionSpinal instability from
vertebral or diskinvolvement
Mediastinum TamponadeAspiration pneumoniaPyothorax
Sinuses Intracranial spreadOrbital spreadMeningitisEpidural or subdural
empyemaTemporal lobes abscessesOrbital fissure syndromes
Superior sagittal orcavernous venoussinus thrombosis
Jaworsky et al448
Not all patients will progress to requiring intubation; however, all patients requirecareful monitoring within an intensive care setting where frequent airway evaluationis possible. There is a growing body of retrospective reports favoring conservativemanagement of intravenous antibiotic therapy and close airway monitoring over con-ventional preemptive airway management in patients with no evidence of significantairway compromise.23 Airway considerations in complicating intubation includealtered airway anatomy, friability of oropharyngeal tissue, and epiglottal edema. Asparalytic agents may precipitate airway occlusion, awake intubation techniques underdirect visualization, such as awake fiberoptic intubation via bronchoscopy, should beconsidered. If fiberoptic bronchoscopy is not successful or possible, tracheostomyunder local anesthesia may be necessary.24 In the direst situations where catastrophicloss of airway patency is possible, it is wise to have a surgeon comfortable with trache-ostomies or, at least, an emergency cricothyroidotomy kit available at the bedsidealong with physicians skilled in this procedure.25 Careful monitoring should becontinued after extubation, as fatal cases of delayed airway compromise in patientsundergoing surgical drainage have been reported.21
Infections of the submandibular space can also spread locally to other fascial planesof the neck and mediastinum, causing cervical necrotizing fasciitis.26 Spread tocontiguous spaces is discussed in subsequent sections.
INFECTIONS OF THE LATERAL PHARYNGEAL SPACEAnatomy and Pathophysiology
The lateral pharyngeal space is a potential space extending from the hyoid to sphe-noid bones and bordered laterally by the parotid gland, mandibles, and internal
Extracranial Head and Neck Infections 449
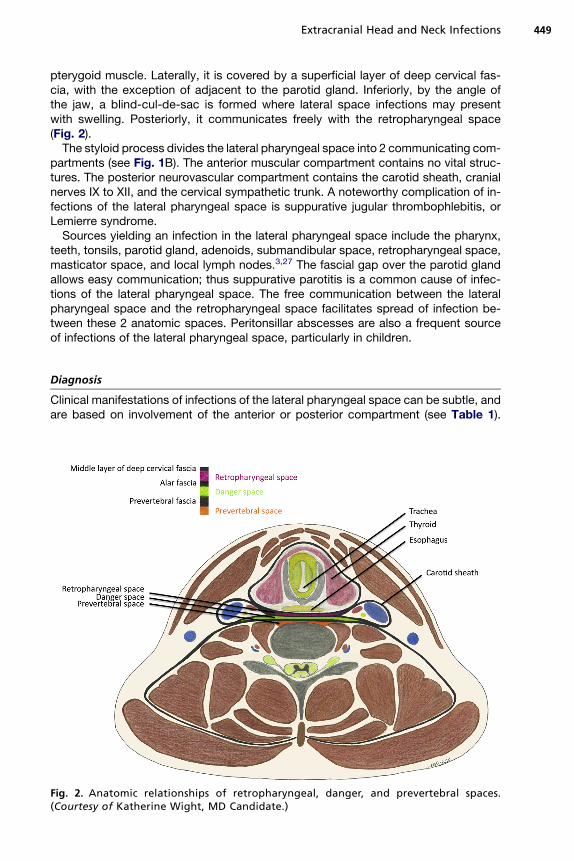
pterygoid muscle. Laterally, it is covered by a superficial layer of deep cervical fas-cia, with the exception of adjacent to the parotid gland. Inferiorly, by the angle ofthe jaw, a blind-cul-de-sac is formed where lateral space infections may presentwith swelling. Posteriorly, it communicates freely with the retropharyngeal space(Fig. 2).The styloid process divides the lateral pharyngeal space into 2 communicating com-
partments (see Fig. 1B). The anterior muscular compartment contains no vital struc-tures. The posterior neurovascular compartment contains the carotid sheath, cranialnerves IX to XII, and the cervical sympathetic trunk. A noteworthy complication of in-fections of the lateral pharyngeal space is suppurative jugular thrombophlebitis, orLemierre syndrome.Sources yielding an infection in the lateral pharyngeal space include the pharynx,
teeth, tonsils, parotid gland, adenoids, submandibular space, retropharyngeal space,masticator space, and local lymph nodes.3,27 The fascial gap over the parotid glandallows easy communication; thus suppurative parotitis is a common cause of infec-tions of the lateral pharyngeal space. The free communication between the lateralpharyngeal space and the retropharyngeal space facilitates spread of infection be-tween these 2 anatomic spaces. Peritonsillar abscesses are also a frequent sourceof infections of the lateral pharyngeal space, particularly in children.
Diagnosis
Clinical manifestations of infections of the lateral pharyngeal space can be subtle, andare based on involvement of the anterior or posterior compartment (see Table 1).
Fig. 2. Anatomic relationships of retropharyngeal, danger, and prevertebral spaces.(Courtesy of Katherine Wight, MD Candidate.)

Jaworsky et al450
Systemic symptoms such as fevers, chills, rigors, and malaise can be present. Signsor symptoms of the precipitating infection, such as pharyngitis or tonsillitis, may haveresolved, and are often mild on history.28 However, signs and symptoms of suppura-tive parotitis include tender erythematous swelling of the preauricular and postauric-ular regions with extension to the angle of the mandible and associated trismus,dysphagia, and evidence of systemic toxicity. Peritonsillar abscesses may manifestas fever, muffled voice, unilateral sore throat with possible ipsilateral ear pain, trismus,and drooling. In some cases, patients may experience only a minor upper respiratorytract infection or malaise several weeks before presentation with an infection of thelateral pharyngeal space.Classic signs of anterior compartment infection include dysphagia, trismus, and
ipsilateral neck and jaw pain with possible referral to the ipsilateral ear. This paincan be intensified by side flexion of the neck to the contralateral side, which com-presses the lateral pharyngeal space and sternocleidomastoid muscles. Examinationmay reveal swelling and induration at the ipsilateral angle of the jaw. Trismus suggestsinflammation of the internal pterygoid muscle, which lies close to the lateral pharyn-geal space. On pharyngeal examination, the lateral pharyngeal wall is often distortedmedially, but the overlying mucosa appears normal. However, thorough examinationmay be limited by pain and trismus.Posterior compartment infections in isolation lack trismus. Patients may not have
localizing signs because the infection is deep-seated, but may first present with sepsisof unknown origin. The diagnosis may only become evident after the development ofneurologic or vascular complications, or when appropriate imaging is performed.Swelling of the parotid space may be present, with parotid involvement. Epiglottaland laryngeal edema can cause significant dyspnea; however, edema of the pharyn-geal wall may be difficult to detect on oropharyngeal examination because it may behidden by the palatopharyngeal arch.An ipsilateral Horner syndrome or palsies of cranial nerves IX to XII are sugges-
tive of carotid-sheath involvement. A devastating potential complication is erosionand rupture of the carotid artery, which is often preceded by smaller “heraldbleeds.”29
Lemierre Syndrome (Suppurative Jugular Thrombophlebitis)
� Rare condition, but most common vascular complication of infections of the lateralpharyngeal space30
� Induration and swelling behind the sternocleidomastoid muscle
� Occlusive anaerobic septic thrombus of the internal jugular vein, often associated withbacteremia and metastatic foci of infection, most commonly in the lung and large joints
� For a more detailed discussion, the reader is directed to the review by Kuppalli andcolleagues31
Contrast-enhanced CT or duplex ultrasonographic imaging of the neck can helpidentify complications of infections of the lateral pharyngeal space such as Lemierresyndrome. Ultrasonography can reveal occlusive and nonocclusive thrombus of largeveins, although contrast-enhanced CT is superior in defining the extent of the under-lying infection such as a peritonsillar abscess. MRI provides comparable imaging, butavailability limits its utility in urgent management.32
Extracranial Head and Neck Infections 451
Antimicrobial Management
� Antimicrobial coverage is similar to that for infections of the submandibularspace (see Table 2).
� If there is no airway compromise, limited data suggest that posterior compart-ment infections (lower tendency to spread) can be treated with antibioticsalone.33–36
� Suppurative jugular thrombophlebitis can usually be treated with 4 to 6 weeks ofantibiotics (duration supported by case reports and series).
� Fusobacterium necrophorum (pathognomonic organism of Lemierre syndrome)is usually penicillin sensitive.
� Anticoagulation in Lemierre syndrome is controversial, with limited data; someexperts suggest consideration, particularly with poor initial response toantibiotics.37,38
Surgical Indications and Therapy
� Adequate, early drainage of pus (if present), in addition to appropriate antibiotictherapy, can prevent spread of infection to contiguous anatomic spaces.
� Contrast CT can identify lateral pharyngeal infections amenable to surgicaldrainage.
� Impending rupture of the carotid artery requires emergent surgical managementand is historically associated with very high morbidity and mortality, even withintervention.27,39
� Lemierre syndrome with ongoing septic embolic events/thrombus propagationmay require surgical ligation of the internal jugular vein.
� Poor surgical candidates may benefit from percutaneous mechanical thrombec-tomy plus thrombolytic therapy.40
Outcomes and Complications
The anatomy of the lateral pharyngeal space makes it a hub for deep space infectionsof the head and neck (see Table 3). Anterior infections of the lateral pharyngeal spacehave a tendency to liquefy the fat of the anterior compartment, creating pus andnecrotic debris that can easily spread to other compartments. Life-threatening com-plications of posterior compartment infection include laryngeal edema and obstruc-tion, sudden death secondary to vagal nerve involvement, Lemierre syndrome, andcarotid artery erosion.
INFECTIONS OF THE RETROPHARYNGEAL AND DANGER SPACESAnatomy and Pathophysiology
Layers of the deep cervical fascia between the pharynx and esophagus create 3 sepa-rate spaces (see Fig. 2). From anterior to posterior, these are the retropharyngeal,danger, and prevertebral spaces.The retropharyngeal space extends from the base of the skull to approximately the
C7/T1 level. The extension of the fascial planes allows for infection to easily spread tothe superior anterior and posterior mediastinum. The middle layer of the deep cervicalfascia extends anteriorly, and fuses with the parietal pericardium and adventitia of thegreat vessels. Risk factors for retropharyngeal abscess include foreign bodies, esoph-ageal instrumentation (endoscopy, nasogastric tubes, frequent suctioning, intubationattempts), suppurative adenitis in children, and spread from contiguous spaces.41 Inadults, infections of the retropharyngeal space often result from contiguous spreadof a coexisting infection of the lateral pharyngeal space. In children, infections of
Jaworsky et al452
the retropharyngeal space may exist in isolation, owing to hematogenous seeding ofthe retropharyngeal lymph nodes from a distant source.Between the alar fascia and the prevertebral fascia lies the danger space, which ex-
tends from the base of the skull to the diaphragm, passing through the posterior medi-astinum. Infections of the danger space often originate from contiguous spread fromneighboring anatomic locations. The third andmost posterior space is the prevertebralspace, which is discussed in a subsequent section as it does not share the samemicrobiology and pathophysiology.
Diagnosis
Infections of the danger space and retropharyngeal space, including retropharyngealabscesses, can present with a wide spectrum of clinical signs and symptoms rangingfrom mild retropharyngeal pain and malaise to respiratory distress and sepsis (seeTable 1). Patients may present with odynophagia, dysphagia, and dyspnea. The pa-tient may also have a stiff neck and may tilt the head up and backwards to maximizeair intake. The pharyngeal wall and supraglottic structures may be displaced, leadingto respiratory distress and noisy breathing. Pleuritic chest pain suggests mediastinalinvolvement. Examination of the oropharynx may reveal bulging of the posteriororopharynx, and a pharyngeal mass may be observed or palpated. Clinicians mustbe aware that palpation of the mass may result in abscess rupture with subsequentaspiration or asphyxiation.In children, a radiograph of the lateral soft tissue of the neck can help to identify a
retropharyngeal collection; however, this is less sensitive than a contrast-enhancedCT scan.42 Imaging is not able to adequately differentiate between infections of theretropharyngeal and danger spaces; however, extension below the T4 level suggestsinvolvement of the danger space.8 Infections in these spacesmay be evident as phleg-mon, suppurative lymphadenitis, or abscesses. Retropharyngeal abscesses second-ary to suppurative lymphadenitis will reveal large paramedian lymph nodes that have alow central density and are ring-enhancing on contrast-enhanced CT.43
Antimicrobial Management
� Antibiotic therapy is similar to that of infections of the submandibular space (seeTable 2).
� Empiric therapy should include coverage for oral anaerobes, including b-lacta-mase–producing organisms.
Surgical Indications and Therapy
� Early antibiotics, before abscess formation, may prevent the need for surgicaldrainage.44–46
� However, there is disagreement regarding the optimal timing for surgicaldrainage.47
� If drainage is needed, minimally invasive drainage in addition to washout tech-niques may be used.48
Outcomes and Complications
Complications of infections of the retropharyngeal and danger spaces include spreadto neighboring spaces and structures, as well as direct local effects (see Table 3).The fascial extension of the pretracheal or anterior visceral fascia allows for spread
of infections of the retropharyngeal space to the visceral space containing the esoph-agus and trachea, and to the superior anterior mediastinum, which can progress to
Extracranial Head and Neck Infections 453
purulent pericardial and pleural infections.49 Infections of the danger space canspread to the posterior mediastinum, pericardium, and, occasionally, the retroperito-neal space.Infections of the retropharyngeal and danger spaces with severe laryngeal inflam-
mation can result in life-threatening airway occlusion. A retropharyngeal abscesscan rupture into the posterior oropharynx, causing aspiration of purulent contents,which can lead to pneumonia or asphyxiation. A potentially lethal complication of in-fections of the retropharyngeal and danger spaces is descending necrotizing media-stinitis. A retrospective review of deep neck infections requiring surgical drainage andadmission to the intensive care unit (ICU) found retropharyngeal abscesses to be morelikely to result in septic shock, severe sepsis, mediastinitis, empyema, or necrotizingfasciitis than deep neck abscesses in other locations.50
INFECTIONS OF THE PREVERTEBRAL SPACEBackground and Epidemiology
The prevertebral space is bounded anteriorly by the prevertebral fascia and poste-riorly by the vertebral bodies. The fascial planes are as described earlier. The prever-tebral space extends from the base of the skull to the coccyx and is contiguous withthe psoas muscle sheath. Infections of the prevertebral space generally originatefrom the cervical or thoracic spine, including vertebral osteomyelitis and discitis,which are usually hematogenous in origin.51 Risk factors for hematogenous spreadinclude injection drug use, diabetes mellitus, immune suppression, and alcoholabuse.52,53
Diagnosis
The presentation of infections of the prevertebral space depends on the degree of spi-nal cord compression and neurologic dysfunction (see Table 1), and the diagnosis ofprevertebral abscesses is often difficult. Nearly half of cases are initially misdiag-nosed.54 Roughly 75% of patients experience back or neck pain, 50% present withfever, and 33% have neurologic deficits, ranging in severity from nerve root pain to pa-ralysis.55 Sixty percent of patients with epidural abscesses are bacteremic on presen-tation.56 The prevertebral space is contiguous with the psoas muscle sheath, so apsoas abscess raises suspicion of an underlying infection of the prevertebral space.57
As infections of the prevertebral space often arise from discitis or spinal osteomyelitis,a thorough assessment should also look for signs for spinal involvement andinstability.MRI is the imaging modality of choice for infections of the prevertebral space, to
assess involvement of the epidural space or spinal cord.43,58
Antimicrobial Management
� The most common organism identified in infections of the prevertebral space isS aureus (see Table 2).
� Other organisms, including oral anaerobes, enteric gram-negative rods, bru-cella,59 nocardia, mycobacteria,60 fungi, and, rarely, parasites,55 have alsobeen found.
� Empiric antimicrobial therapy should be broad, including coverage for MRSA andfacultative gram-negative bacilli, and guided by local antimicrobial resistancepatterns.
� Coverage of gram-negative rods is important, particularly if risk factors (eg, injec-tion drug use, urinary tract infection) are present.53,55
Jaworsky et al454
Surgical Indications and Therapy
� Surgical drainage is required for source control and to minimize neurologicsequelae.
� There is controversy regarding combined surgical-medical management versusmedical management alone:
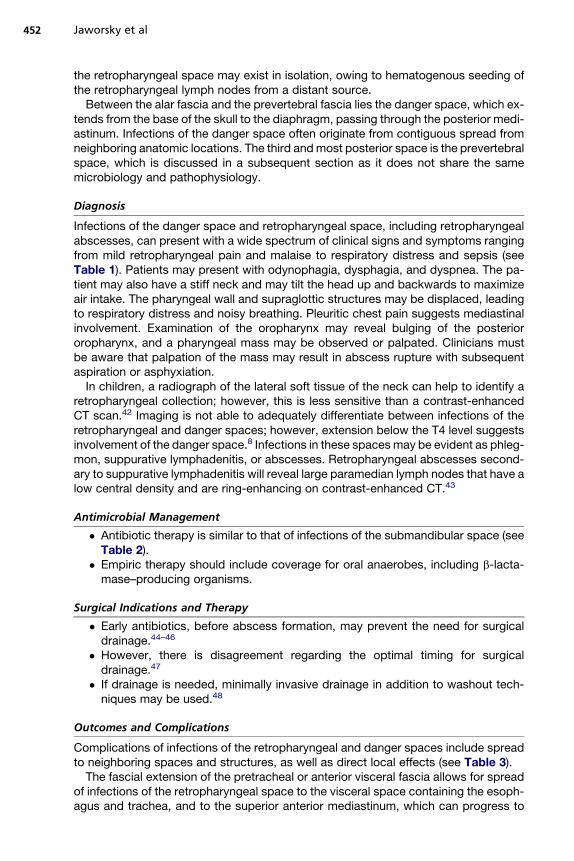
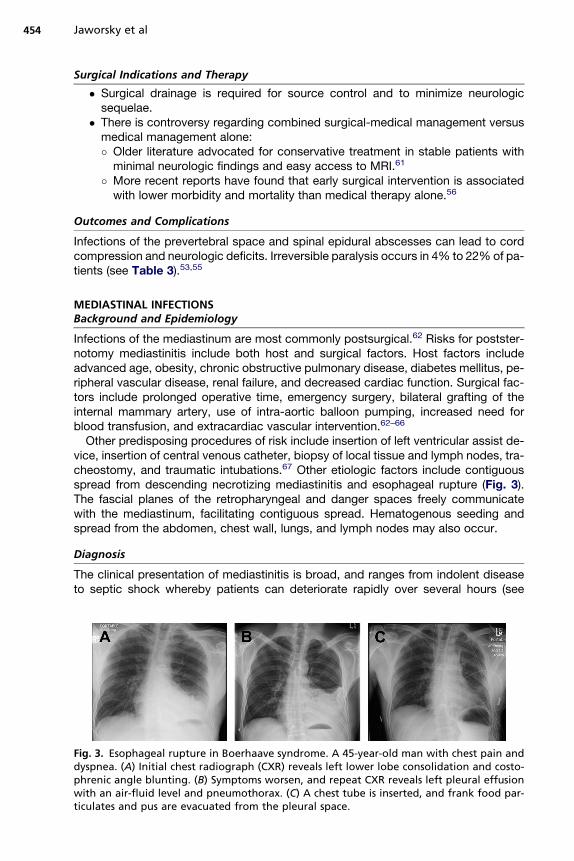
Fig. 3dyspnphrenwithticula
� Older literature advocated for conservative treatment in stable patients withminimal neurologic findings and easy access to MRI.61
� More recent reports have found that early surgical intervention is associatedwith lower morbidity and mortality than medical therapy alone.56
Outcomes and Complications
Infections of the prevertebral space and spinal epidural abscesses can lead to cordcompression and neurologic deficits. Irreversible paralysis occurs in 4% to 22% of pa-tients (see Table 3).53,55
MEDIASTINAL INFECTIONSBackground and Epidemiology
Infections of the mediastinum are most commonly postsurgical.62 Risks for postster-notomy mediastinitis include both host and surgical factors. Host factors includeadvanced age, obesity, chronic obstructive pulmonary disease, diabetes mellitus, pe-ripheral vascular disease, renal failure, and decreased cardiac function. Surgical fac-tors include prolonged operative time, emergency surgery, bilateral grafting of theinternal mammary artery, use of intra-aortic balloon pumping, increased need forblood transfusion, and extracardiac vascular intervention.62–66
Other predisposing procedures of risk include insertion of left ventricular assist de-vice, insertion of central venous catheter, biopsy of local tissue and lymph nodes, tra-cheostomy, and traumatic intubations.67 Other etiologic factors include contiguousspread from descending necrotizing mediastinitis and esophageal rupture (Fig. 3).The fascial planes of the retropharyngeal and danger spaces freely communicatewith the mediastinum, facilitating contiguous spread. Hematogenous seeding andspread from the abdomen, chest wall, lungs, and lymph nodes may also occur.
Diagnosis
The clinical presentation of mediastinitis is broad, and ranges from indolent diseaseto septic shock whereby patients can deteriorate rapidly over several hours (see
. Esophageal rupture in Boerhaave syndrome. A 45-year-old man with chest pain andea. (A) Initial chest radiograph (CXR) reveals left lower lobe consolidation and costo-ic angle blunting. (B) Symptoms worsen, and repeat CXR reveals left pleural effusionan air-fluid level and pneumothorax. (C) A chest tube is inserted, and frank food par-tes and pus are evacuated from the pleural space.
Extracranial Head and Neck Infections 455
Table 1). Historical features such as recent surgery or instrumentation, head and neckinfections, caustic ingestions, emesis, and dysphagia may help to identify an underly-ing cause. Patients may experience chest pain, dysphagia, odynophagia, dyspnea,nausea, and, occasionally, abdominal pain. Physical examination often reveals a feverand tachycardia, and possible septic shock. Chest-wall crepitus may be palpated anda Hamman crunch may be auscultated. Hamman crunch, a sign of pneumomediasti-num, is a systolic crunching or clicking sound best heard over the cardiac apex. Inesophageal rupture a history of emesis, chest pain, and subcutaneous emphysemamay be present. Poststernotomy mediastinitis is commonly associated with sternalosteomyelitis and associated failure of sternal closure wires. Poststernotomy patientsmay or may not have incision-site infections, chest pain, wound dehiscence, sternalinstability, or sepsis with no alternative source.Chest radiography may show subcutaneous, mediastinal, or pericardial air, a
widened mediastinum, or pleural effusions with or without air-fluid levels. Contrast-enhanced CT of the chest is imperative in the diagnostic workup, and can identifylocalized infection and complications. Within 2 weeks of a sternotomy, MRI may berequired owing to extensive postoperative edema. CT of the neck and lower skullmay identify a source of descending necrotizing mediastinitis.
Antimicrobial Management
� The cornerstone of treatment is early broad-spectrum antibiotics (see Table 2)plus consideration of surgical debridement.
� Microbiology is largely determined by the source of infection:
� Head and neck origin: polymicrobial, oropharyngeal organisms� Esophageal perforation: similar, but more gram-negative bacilli� Postsurgical: more likely to be caused by Staphylococcus aureus, althoughEnterococcus spp and facultative gram-negative bacilli should be considered� Indolent infections may be caused by coagulase-negative staphylococci.� Anaerobic organisms are less common.� If there is poor response to broad-spectrum antibacterial agents, other patho-gens such as Candida and Aspergillus should be considered.68
Surgical Indications and Therapy
� Historically, surgical drainage and debridement has been a mainstay oftreatment.
� Appropriate surgical services (thoracic, oromaxillofacial, cardiac, or otolaryn-gology) may be consulted.
� Thoracotomy with cervicotomy has been the technique of choice for mediastinaldrainage and debridement.69,70
� Some evidence indicates that aggressive surgical debridement leads to betteroutcomes in necrotizing mediastinitis.71–73
� Recent literature supports more conservative measures, including percutaneouscatheter drainage and drainage via video-assisted thoracoscopic surgery.74,75
� Recurrent abscesses may require subsequent drainage, percutaneous orotherwise.76
Outcomes and Complications
Complications of mediastinitis include pericardial spread causing pericardial effusionand possible tamponade, aspiration pneumonia, and rupture into the pleural cavitywith subsequent pyothorax and pleural effusions (see Table 3).77 Acute mediastinitisis associated with mortality rates ranging from 12% to 50%.63,78–81
Jaworsky et al456
Factors associated with mortality due to poststernotomy mediastinitis include ageolder than 70 years, surgical procedures other than coronary artery bypass graft alone,McCabe class 2/3, APACHE II score, persistent bacteremia, and failure to wean frommechanical ventilation by postoperative day 3.80
SINUSITISBackground and Epidemiology
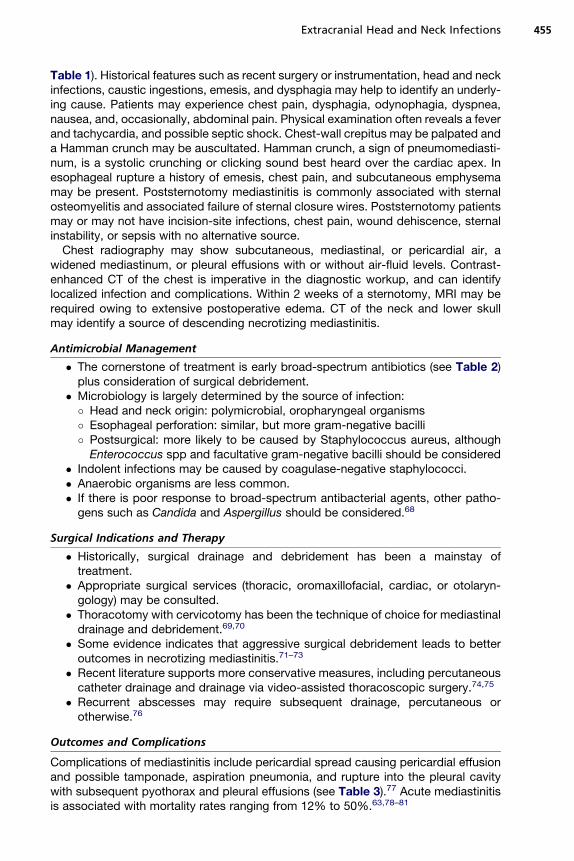
The maxillary, ethmoid, frontal, and sphenoid sinuses make up the paranasal sinuses(Fig. 4, Table 4). These air-filled cavities are connected via sinus ostia, which drain intothe nasal cavity. The posterior ethmoid and sphenoid sinuses drain into the superiormeatus of the nasal cavity. The frontal, anterior ethmoid, and maxillary sinuses draininto the middle meatus. Drainage from the paranasal sinuses converges in the osteo-meatal complex, which lies between the middle and inferior nasal turbinates.Though generally sterile, the paranasal sinuses can be transiently colonized by flora
from the upper respiratory tract. The most common sinus infection occurs in the maxil-lary sinuses. The apices of the first, second, and thirdmaxillarymolars rest just beneaththe inferior aspect of the maxillary sinus. As a result, odontogenic infection can lead tomaxillary sinusitis. Traumatic head injury is also a risk factor for maxillary sinusitis.82
Fig. 4. Anatomic relationships of the paranasal sinuses. (Netter illustration from www.netterimages.com. � Elsevier Inc. All rights reserved.)
Table 4Comparative clinical features of sinusitis
Sinus Symptoms
Maxillary Toothache
Frontal Headache
Ethmoid Eyelid edema, excess lacrimation, proptosis andretro-orbital pain if orbit involvement
Sphenoid Headache; orbital pain, exophthalmos andophthalmoplegia in superior orbital fissure syndrome
Extracranial Head and Neck Infections 457
The frontal sinus is a less common site of sinusitis, but because of its anatomic loca-tion, subsequent spread to the intracranial space or orbit can occur. The ethmoid si-nuses lie adjacent to the orbit, with only a thin orbital plate separating the 2compartments. The sphenoid sinus is bordered superiorly by the pituitary gland,rostrally by the optic nerve and optic chiasm, and laterally by the internal carotid ar-teries, cavernous sinuses, and temporal lobes of the brain.In critically ill patients, nasal foreign bodies and irritation contribute to nosocomial
sinusitis. Risk factors for ICU-associated sinusitis include nasal colonization withgram-negative bacilli, nasoenteric-tube feeding, sedation, and Glasgow Coma Scalescore of 7 or less.83 Prevalence of rhinosinusitis in the ICU varies broadly and rangesfrom 7.7% to 58%, making this a significant source of ICU-associated infection.83–85
Diagnosis
Sinusitis in critically ill patients can range in presentation from an indolent chronicsinusitis to rare instances of severe and complicated infection (see Table 1). Sinusitissecondary to nasotracheal or nasogastric intubation may be difficult to detect clini-cally. Signs may include purulent rhinorrhea or a middle-ear effusion. In critically illintubated patients, sinusitis can manifest as only an unexplained fever.86,87 Signs ofethmoid sinusitis include eyelid edema and excess lacrimation. Proptosis and retro-orbital pain suggest involvement of the orbit. In sphenoid sinusitis, severe headachecan resemble trigeminal neuralgia or an ophthalmic migraine.Endoscopy can identify purulent discharge from themiddle meatus and edematous,
hyperemic nasal turbinates, and endoscopically directed middle meatal cultures havea high yield for detecting causative organisms.88 In ICU patients, visualization of puru-lence in the middle meatus has been found to be more sensitive than CT for predictingpositive cultures on antral lavage.89
Imaging studies are required if there is a concern for orbital or intracranial extensionand in cases that fail initial empiric therapy. Plain sinus radiographs may reveal signs ofacute sinusitis; however, CT imaging allows for better visualization of the sinuses andtheir contents, particularly the ethmoid and sphenoid sinuses. Orbital or intracranialcomplications are best visualized with contrast-enhanced CT. Air-fluid levels are themost sensitive CT sign of sinusitis.89 Although CT is very sensitive for detecting evi-dence of sinusitis, its specificity is poor and findings must be interpreted within thegiven clinical context. MRI is limited in evaluating cortical bone, but is valuable forinvestigating intracranial suppurative and intraorbital complications. B-mode ultraso-nography can be used to diagnose maxillary sinusitis, although it is not a useful mo-dality for imaging the other sinuses.82 Bedside A-mode ultrasonography can also beused to detect maxillary sinusitis, although its sensitivity is low.90
Mucormycosis sinusitis, commonly caused by fungi in the order Mucorales (eg,Mucor, Rhizopus), can also be caused by other molds such as Aspergillus spp.
Jaworsky et al458
Mucormycosis is most common in immunocompromised and diabetic patients, andis characterized by a rapidly progressive and invasive infection that can often becomplicated by intracranial and intraorbital spread. Presenting signs and symptomsmay include headache, fever, facial swelling, and unilateral orbital apex syndromewith involvement of cranial nerves III to VI, caused by invasion of the apex of theorbit. If there is intracranial involvement, patients may experience seizures,decreased level of consciousness, stroke, and coma. CT findings of sinonasalmucormycosis include hyperdense opacification of the soft tissue, nodular mucosalthickening, and an absence of fluid levels in the paranasal sinuses. Bony change anddestruction with focal masses can also be seen. Orbital invasion from the ethmoidsinus is characterized by thickening and lateral displacement of the medial rectusmuscle.91
Antimicrobial Management
� In patients admitted to the ICU, the most commonly isolated pathogens aregram-negative organisms, although gram-positive organisms are also frequentlyisolated.
� Anaerobic and fungal isolates are less common.82,83,87,92
� Cultures (sinus puncture 1 aspiration) can help guide antimicrobial therapy (seeTable 2).92
� Antifungals should be considered in severely immunocompromised patients withinvasive disease.
� Noninvasive fungal sinusitis may respond to surgical debridement.� In immunocompromised hosts, high-dose intravenous amphotericin B plus sur-gical debridement is often needed.
� Once the fungal pathogen is known, alternatives to amphotericin (toxicity) can beused.
� Careful consideration needs to be given to the antimicrobial susceptibility to andintracranial penetration of the antifungal chosen.
Surgical Indications and Therapy
� Invasive fungal infections (eg, mucormycosis), orbital involvement, intracranialcomplications, and refractory sinusitis secondary to osteomeatal obstructionwarrant surgical intervention.
� Functional endoscopic sinus surgery can be used to relieve ostial obstructionand to access ethmoid and sphenoid sinuses.
� Initial management for patients diagnosed with sinusitis in a critical care settingconsists of antibiotics, saline nasal irrigation, aspiration of secretions, andremoval of nasal catheters.
� If conservative therapy fails, sinus puncture with drainage, irrigation, andpossible temporary drain insertion is indicated, although rarely done.
� Most of the literature is restricted to the use of sinus puncture for maxillary sinus-itis; however, emerging evidence suggests a role for sphenoid sinus puncture.92
Outcomes and Complications
Although rare in the postantibiotic era, suppurative complications of sinusitis canoccur (see Table 3).Frontal sinusitis can lead to intracranial or orbital spread, frontal bone osteomyelitis
(Pott puffy tumor), or superior sagittal sinus thrombosis. Compromise of the plate be-tween the ethmoid sinus and the orbital space can facilitate spread of infection to theretro-orbital space. In addition, ethmoid sinusitis can be complicated by cavernous
Extracranial Head and Neck Infections 459
venous or superior sagittal sinus thrombosis and intracranial spread. Maxillary orethmoid sinusitis can result in osteomyelitis of the facial bones and subsequent pro-lapse of the orbital antral wall. Maxillary sinusitis rarely leads to intracranial spread,except in rhinocerebral mucormycosis. Because of its anatomic location and prox-imity to essential structures, sphenoid sinusitis can result in meningitis, epidural orsubdural empyema, temporal lobe abscesses, orbital fissure syndromes, andcavernous sinus thrombosis.
REFERENCES
1. Meyers BR, Lawson W, Hirschman SZ. Ludwig’s angina. Case report, with re-view of bacteriology and current therapy. Am J Med 1972;53:257–60.
2. Tsuji T, Shimono M, Yamane G, et al. Ludwig’s angina as a complication of ame-loblastoma of the mandible. J Oral Maxillofac Surg 1984;42:815–9.
3. Levitt GW. Cervical fascia and deep neck infections. Laryngoscope 1970;80:409–35.
4. Fischmann GE, Graham BS. Ludwig’s angina resulting from the infection of anoral malignancy. J Oral Maxillofac Surg 1985;43:795–6.
5. Rothwell BR. Odontogenic infections. Emerg Med Clin North Am 1985;3:161–78.6. Megran DW, Scheifele DW, Chow AW. Odontogenic infections. Pediatr Infect Dis
1984;3:257–65.7. Bakir S, Tanriverdi MH, Gun R, et al. Deep neck space infections: a retrospective
review of 173 cases. Am J Otol 2012;33:56–63.8. Rana RS, Moonis G. Head and neck infection and inflammation. Radiol Clin
North Am 2011;49:165–82.9. Smith JL 2nd, Hsu JM, Chang J. Predicting deep neck space abscess using
computed tomography. Am J Otol 2006;27:244–7.10. Miller WD, Furst IM, Sandor GK, et al. A prospective, blinded comparison of clin-
ical examination and computed tomography in deep neck infections. Laryngo-scope 1999;109:1873–9.
11. Brook I. Microbiology and management of peritonsillar, retropharyngeal, andparapharyngeal abscesses. J Oral Maxillofac Surg 2004;62:1545–50.
12. Coulthard M, Isaacs D. Retropharyngeal abscess. Arch Dis Child 1991;66:1227–30.
13. Har-El G, Aroesty JH, Shaha A, et al. Changing trends in deep neck abscess. Aretrospective study of 110 patients. Oral Surg Oral Med Oral Pathol 1994;77:446–50.
14. Huang TT, Tseng FY, Yeh TH, et al. Factors affecting the bacteriology of deepneck infection: a retrospective study of 128 patients. Acta Otolaryngol 2006;126:396–401.
15. Rega AJ, Aziz SR, Ziccardi VB. Microbiology and antibiotic sensitivities of headand neck space infections of odontogenic origin. J Oral Maxillofac Surg 2006;64:1377–80.
16. Sato K, Izumi T, Toshima M, et al. Retropharyngeal abscess due to methicillin-resistant Staphylococcus aureus in a case of acute myeloid leukemia. InternMed 2005;44:346–9.
17. Wertheim HF, Melles DC, Vos MC, et al. The role of nasal carriage in Staphylo-coccus aureus infections. Lancet Infect Dis 2005;5:751–62.
18. Frazee BW, Lynn J, Charlebois ED, et al. High prevalence of methicillin-resistantStaphylococcus aureus in emergency department skin and soft tissue infec-tions. Ann Emerg Med 2005;45:311–20.
Jaworsky et al460
19. Kobayashi KI, Haruta T, Kubota M, et al. A case of retropharyngeal abscesscaused by penicillin-resistant Streptococcus pneumoniae. J Infect 2002;44:267–9.
20. Kuriyama T, Karasawa T, Nakagawa K, et al. Antimicrobial susceptibility of majorpathogens of orofacial odontogenic infections to 11 beta-lactam antibiotics. OralMicrobiol Immunol 2002;17:285–9.
21. Greenland KB, Acott C, Segal R, et al. Delayed airway compromise following ex-tubation of adult patients who required surgical drainage of Ludwig’s angina:comment on three coronial cases. Anaesth Intensive Care 2011;39:506–8.
22. Mathew GC, Ranganathan LK, Gandhi S, et al. Odontogenic maxillofacial spaceinfections at a tertiary care center in North India: a five-year retrospective study.Int J Infect Dis 2012;16:e296–302.
23. Hasan W, Leonard D, Russell J. Ludwig’s Angina-A controversial surgical emer-gency: how we do it. Int J Otolaryngol 2011;2011:231816.
24. Ovassapian A, Tuncbilek M, Weitzel EK, et al. Airway management in adult pa-tients with deep neck infections: a case series and review of the literature.Anesth Analg 2005;100:585–9.
25. Wolfe MM, Davis JW, Parks SN. Is surgical airway necessary for airway manage-ment in deep neck infections and Ludwig angina? J Crit Care 2011;26:11–4.
26. Ustin JS, Malangoni MA. Necrotizing soft-tissue infections. Crit Care Med 2011;39:2156–62.
27. Blomquist IK, Bayer AS. Life-threatening deep fascial space infections of thehead and neck. Infect Dis Clin North Am 1988;2:237–64.
28. Scully RE, Galdabini JJ, McNeely BU. Case records of the Massachusetts Gen-eral Hospital. Weekly clinicopathological exercises. Case 33-1975. N Engl JMed 1975;293:394–9.
29. Knouse MC, Madeira RG, Celani VJ. Pseudomonas aeruginosa causing a rightcarotid artery mycotic aneurysm after a dental extraction procedure. Mayo ClinProc 2002;77:1125–30.
30. Brazier JS. Human infections with Fusobacterium necrophorum. Anaerobe2006;12:165–72.
31. Kuppalli K, Livorsi D, Talati NJ, et al. Lemierre’s syndrome due to Fusobacteriumnecrophorum. Lancet Infect Dis 2012;12:808–15.
32. Weeks DF, Katz DS, Saxon P, et al. Lemierre syndrome: report of five new casesand literature review. Emerg Radiol 2010;17:323–8.
33. Sichel JY, Dano I, Hocwald E, et al. Nonsurgical management of parapharyng-eal space infections: a prospective study. Laryngoscope 2002;112:906–10.
34. Sakaguchi M, Sato S, Ishiyama T, et al. Characterization and management ofdeep neck infections. Int J Oral Maxillofac Surg 1997;26:131–4.
35. McClay JE, Murray AD, Booth T. Intravenous antibiotic therapy for deep neckabscesses defined by computed tomography. Arch Otolaryngol Head NeckSurg 2003;129:1207–12.
36. Boscolo-Rizzo P, Marchiori C, Zanetti F, et al. Conservative management of deepneck abscesses in adults: the importance of CECT findings. Otolaryngol HeadNeck Surg 2006;135:894–9.
37. Bondy P, Grant T. Lemierre’s syndrome: what are the roles for anticoagulationand long-term antibiotic therapy? Ann Otol Rhinol Laryngol 2008;117:679–83.
38. Phan T, So TY. Use of anticoagulation therapy for jugular vein thrombus in pedi-atric patients with Lemierre’s syndrome. Int J Clin Pharm 2012;34(6):818–21.
39. Blum DJ, McCaffrey TV. Septic necrosis of the internal carotid artery: a compli-cation of peritonsillar abscess. Otolaryngol Head Neck Surg 1983;91:114–8.
Extracranial Head and Neck Infections 461
40. Kar S, Webel R. Septic thrombophlebitis: percutaneous mechanical thrombec-tomy and thrombolytic therapies. Am J Ther 2011. [Epub ahead of print].
41. Barratt GE, Koopmann CF Jr, Coulthard SW. Retropharyngeal abscess—a ten-year experience. Laryngoscope 1984;94:455–63.
42. Uzomefuna V, Glynn F, Mackle T, et al. Atypical locations of retropharyngeal ab-scess: beware of the normal lateral soft tissue neck X-ray. Int J Pediatr Otorhi-nolaryngol 2010;74:1445–8.
43. Maroldi R, Farina D, Ravanelli M, et al. Emergency imaging assessment of deepneck space infections. Semin Ultrasound CT MR 2012;33:432–42.
44. Chow AW. Life-threatening infections of the head, neck and upper respiratorytract. In: Hall JB, Schmidt GA, Wood LD, editors. Principles of critical care.3rd edition. New York: McGraw-Hill; 2005. p. 881–96.
45. Plaza Mayor G, Martinez-San Millan J, Martinez-Vidal A. Is conservativetreatment of deep neck space infections appropriate? Head Neck 2001;23:126–33.
46. Ungkanont K, Yellon RF, Weissman JL, et al. Head and neck space infections ininfants and children. Otolaryngol Head Neck Surg 1995;112:375–82.
47. Shanti RM, Aziz SR. Should we wait for development of an abscess before weperform incision and drainage? Oral Maxillofac Surg Clin North Am 2011;23:513–8, v.
48. Adelson RT, Murray AD. Minimally invasive transoral catheter-assisted drainageof a danger-space infection. Ear Nose Throat J 2005;84:785–6.
49. Endo S, Tsubochi H, Nakano T, et al. Descending necrotizing mediastinitis sec-ondary to retropharyngeal abscess without cervical spread. Gen Thorac Cardi-ovasc Surg 2008;56:25–7.
50. Garcia T, Rios M, Paiva JA. Predictors of severity in deep neck infectionsadmitted to the intensive care unit. Anaesth Intensive Care 2012;40:832–7.
51. Grewal S, Hocking G, Wildsmith JA. Epidural abscesses. Br J Anaesth 2006;96:292–302.
52. Gordon RJ, Lowy FD. Bacterial infections in drug users. N Engl J Med 2005;353:1945–54.
53. Darouiche RO. Spinal epidural abscess. N Engl J Med 2006;355:2012–20.54. Davis DP, Wold RM, Patel RJ, et al. The clinical presentation and impact of diag-
nostic delays on emergency department patients with spinal epidural abscess.J Emerg Med 2004;26:285–91.
55. Reihsaus E, Waldbaur H, Seeling W. Spinal epidural abscess: a meta-analysis of915 patients. Neurosurg Rev 2000;23:175–204 [discussion: 205].
56. Curry WT Jr, Hoh BL, Amin-Hanjani S, et al. Spinal epidural abscess: clinicalpresentation, management, and outcome. Surg Neurol 2005;63:364–71 [discus-sion: 371].
57. Muckley T, Schutz T, Kirschner M, et al. Psoas abscess: the spine as a primarysource of infection. Spine 2003;28:E106–13.
58. Stabler A, Reiser MF. Imaging of spinal infection. Radiol Clin North Am 2001;39:115–35.
59. Pina MA, Modrego PJ, Uroz JJ, et al. Brucellar spinal epidural abscess of cer-vical location: report of four cases. Eur Neurol 2001;45:249–53.
60. Krishnan A, Patkar D, Patankar T, et al. Craniovertebral junction tuberculosis: areview of 29 cases. J Comput Assist Tomogr 2001;25:171–6.
61. Hanigan WC, Asner NG, Elwood PW. Magnetic resonance imaging and thenonoperative treatment of spinal epidural abscess. Surg Neurol 1990;34:408–13.
Jaworsky et al462
62. Gummert JF, Barten MJ, Hans C, et al. Mediastinitis and cardiac surgery—anupdated risk factor analysis in 10,373 consecutive adult patients. Thorac Cardi-ovasc Surg 2002;50:87–91.
63. Upton A, Roberts SA, Milsom P, et al. Staphylococcal post-sternotomy mediasti-nitis: five year audit. ANZ J Surg 2005;75:198–203.
64. Diez C, Koch D, Kuss O, et al. Risk factors for mediastinitis after cardiac sur-gery—a retrospective analysis of 1700 patients. J Cardiothorac Surg 2007;2:23.
65. Risnes I, Abdelnoor M, Almdahl SM, et al. Mediastinitis after coronary arterybypass grafting risk factors and long-term survival. Ann Thorac Surg 2010;89:1502–9.
66. Tiveron MG, Fiorelli AI, Mota EM, et al. Preoperative risk factors for mediastinitisafter cardiac surgery: analysis of 2768 patients. Rev Bras Cir Cardiovasc 2012;27:203–10.
67. Khan AZ, Strauss D, Mason RC. Boerhaave’s syndrome: diagnosis and surgicalmanagement. Surgeon 2007;5:39–44.
68. Reynolds S, Ahmad O. Mediastinal infections. In: Vincent J, Hall JB, editors.Encyclopedia of intensive care medicine. Berlin/Heidelberg: Springer Science;2012. p. 1371–7.
69. Makeieff M, Gresillon N, Berthet JP, et al. Management of descending necro-tizing mediastinitis. Laryngoscope 2004;114:772–5.
70. Mihos P, Potaris K, Gakidis I, et al. Management of descending necrotizing me-diastinitis. J Oral Maxillofac Surg 2004;62:966–72.
71. Misthos P, Katsaragakis S, Kakaris S, et al. Descending necrotizing anterior me-diastinitis: analysis of survival and surgical treatment modalities. J Oral Maxillo-fac Surg 2007;65:635–9.
72. Sandner A, Borgermann J, Kosling S, et al. Descending necrotizing mediastini-tis: early detection and radical surgery are crucial. J Oral Maxillofac Surg 2007;65:794–800.
73. De Feo M, Vicchio M, Sante P, et al. Evolution in the treatment of mediastinitis:single-center experience. Asian Cardiovasc Thorac Ann 2011;19:39–43.
74. Min HK, Choi YS, Shim YM, et al. Descending necrotizing mediastinitis: a mini-mally invasive approach using video-assisted thoracoscopic surgery. AnnThorac Surg 2004;77:306–10.
75. Nakamori Y, Fujimi S, Ogura H, et al. Conventional open surgery versus percu-taneous catheter drainage in the treatment of cervical necrotizing fasciitis anddescending necrotizing mediastinitis. AJR Am J Roentgenol 2004;182:1443–9.
76. Singhal P, Kejriwal N, Lin Z, et al. Optimal surgical management of descendingnecrotising mediastinitis: our experience and review of literature. Heart LungCirc 2008;17:124–8.
77. Bulut M, Balci V, Akkose S, et al. Fatal descending necrotising mediastinitis.Emerg Med J 2004;21:122–3.
78. Milano CA, Kesler K, Archibald N, et al. Mediastinitis after coronary artery bypassgraft surgery. Risk factors and long-term survival. Circulation 1995;92:2245–51.
79. Braxton JH, Marrin CA, McGrath PD, et al. Mediastinitis and long-term survivalafter coronary artery bypass graft surgery. Ann Thorac Surg 2000;70:2004–7.
80. Trouillet JL, Vuagnat A, Combes A, et al. Acute poststernotomy mediastinitismanaged with debridement and closed-drainage aspiration: factors associatedwith death in the intensive care unit. J Thorac Cardiovasc Surg 2005;129:518–24.
81. Jablonski S, Brocki M, Kordiak J, et al. Acute mediastinitis: evaluation of clinicalrisk factors for death in surgically treated patients. ANZ J Surg 2012. [Epubahead of print].
Extracranial Head and Neck Infections 463
82. Cengiz M, Celikbilek G, Andic C, et al. Maxillary sinusitis in patients ventilatedfor a severe head injury and with nostrils free of any foreign body. Injury 2011;42:33–7.
83. George DL, Falk PS, Umberto Meduri G, et al. Nosocomial sinusitis in patients inthe medical intensive care unit: a prospective epidemiological study. Clin InfectDis 1998;27:463–70.
84. Holzapfel L, Chastang C, Demingeon G, et al. A randomized study assessingthe systematic search for maxillary sinusitis in nasotracheally mechanicallyventilated patients. Influence of nosocomial maxillary sinusitis on the occurrenceof ventilator-associated pneumonia. Am J Respir Crit Care Med 1999;159:695–701.
85. Ylipalosaari P, Ala-Kokko TI, Laurila J, et al. Epidemiology of intensive care unit(ICU)-acquired infections in a 14-month prospective cohort study in a singlemixed Scandinavian university hospital ICU. Acta Anaesthesiol Scand 2006;50:1192–7.
86. van Zanten AR, Dixon JM, Nipshagen MD, et al. Hospital-acquired sinusitis is acommon cause of fever of unknown origin in orotracheally intubated critically illpatients. Crit Care 2005;9:R583–90.
87. Padua FG, Bezerra TF, Voegels RL, et al. The efficacy of functional endoscopicsinus surgery in the evolution of fever of unknown origin in ICU patients. ActaOtolaryngol 2011;131:166–72.
88. Elwany S, Helmy SA, El-Reweny EM, et al. Endoscopically directed middle mea-tal cultures vs computed tomographic scans in the diagnosis of bacterial sinus-itis in intensive care units. J Crit Care 2012;27:315.e1–5.
89. Skoulas IG, Helidonis E, Kountakis SE. Evaluation of sinusitis in the intensivecare unit patient. Otolaryngol Head Neck Surg 2003;128:503–9.
90. Boet S, Guene B, Jusserand D, et al. A-mode ultrasound in the diagnosis ofmaxillary sinusitis in ventilated patients. B-ENT 2010;6:177–82.
91. Bae MS, Kim EJ, Lee KM, et al. Rapidly progressive rhino-orbito-cerebralmucormycosis complicated with unilateral internal carotid artery occlusion: acase report. Neurointervention 2012;7:45–9.
92. Jardim Vieira FM, Nunes da Silva R, Stefanini R, et al. Safety of sphenoid aspi-ration for diagnosis and treatment of intensive care unit rhinosinusitis. Am JRhinol Allergy 2010;24:389–91.





























