Embed Size (px)
Citation preview

CASE REPORT
Extra-hepatic bile duct hamartoma in a 10-month-oldwith a morgagni hernia and multiple anatomical anomalies:a rare and incidental finding
Adil A. Shah • Michael Karass • Andrew J. Page •
Bahig M. Shehata • Megan M. Durham
Accepted: 16 January 2013
� Springer-Verlag Berlin Heidelberg 2013
Abstract Von Meyenburg complexes (VMCs), also
known as bile duct hamartomas, are a part of a group of
ductal plate malformations. They are typically present in-
trahepatically. In this case, we present to our knowledge
the first report of an extra-hepatic VMC in the pediatric
population. The patient presented as a 10-month-old infant
with a weeklong history of progressive breathing difficulty.
A chest radiograph was obtained, showing intestinal loops
in the thoracic cavity consistent with a Morgagni’s hernia,
unrelated to his breathing difficulty. The patient then
underwent an elective repair of his congenital diaphrag-
matic defect. During the operation, the bile duct hamar-
toma was found adherent to the accessory lobe of the liver,
present to the left of the ligamentum teres.
Introduction
Bile duct hamartomas, also known as VMCs, are uncom-
mon, often noted as incidental findings during abdominal
procedures [1]. They are part of a group of defects and
conditions caused by ductal plate malformations including
choledochal cyst, adult autosomal dominant polycystic
liver disease, Caroli’s disease, and Caroli’s syndrome [1].
They are infrequent anomalies in adults (5.6 %) and even
rarer in children (0.9 %) [2]. However, the incidence from
radiological studies is different from the above reported
figures [1, 5, 8]. Believed to sporadically occur as a con-
sequence of ductal plate dysgenesis, these lesions are
considered anatomical anomalies rather than neoplastic
transformations. Histopathologically, they consist of dis-
ordered aggregates of dilated bile ductules embedded in a
fibrocollagenous stroma [3]. Radiological diagnosis may be
difficult for small nodules. Multiple lesions are often
mistaken for metastasis [4, 5].
We report a case of a 10-month-old boy, initially diag-
nosed with a Morgagni hernia at the age of 5 months.
Intraoperatively, in addition to the diaphragmatic hernia, he
had an intra-abdominal mass, that was histopathologically
an extra-hepatic bile duct hamartoma.
Case presentation
A 5-month-old male infant presented to our institution with
a weeklong history of progressive difficulty in breathing
and nasal congestion, for which he had received nebulized
inhalation therapy at an outside facility. He was brought to
our ED when symptoms failed to improve. His oral intake
had decreased significantly with increased work of
breathing. Clinically, the child appeared dehydrated, tach-
ycardic and tachypneic with noticeable wheezing, grunting
and chest retractions. Pulse oximetry, however, revealed
his saturations to be in the 90 % range. Suctioning of the
airway and intermittent nebulizations with albuterol and
ipratropium bromide failed to produce significant
improvement.
A chest radiograph (Fig. 1) showed intestinal loops in
the thoracic cavity consistent with a Morgagni’s hernia.
A. A. Shah
Medical College, Aga Khan University, Karachi, Pakistan
M. Karass � B. M. Shehata (&)
Department of Pediatric Pathology, Children’s Health Care
of Atlanta, Emory University School of Medicine, Atlanta,
Georgia, USA
e-mail: [email protected]
A. J. Page � M. M. Durham
Department of Pediatric Surgery, Children’s Health Care
of Atlanta and Emory University, Atlanta, Georgia, USA
123
Pediatr Surg Int
DOI 10.1007/s00383-013-3271-2
Surgery was consulted and it was determined that his
respiratory condition was unrelated to the congenital dia-
phragmatic hernia. The patient was admitted to the pedi-
atrics service for management of his respiratory symptoms.
He was found to be respiratory syncytial virus (RSV)
positive which was expectantly managed with supple-
mental oxygen and nebulizers with the diagnosis of acute
bronchiolitis.
Elective repair of the congenital diaphragmatic defect
(CDH) was scheduled once his respiratory symptoms
resolved. He had no significant past medical or surgical
history. He was born at term with no complications and
was developmentally appropriate. The child’s CDH had
been completely asymptomatic and had no history of dif-
ficulties in feeding or stooling.
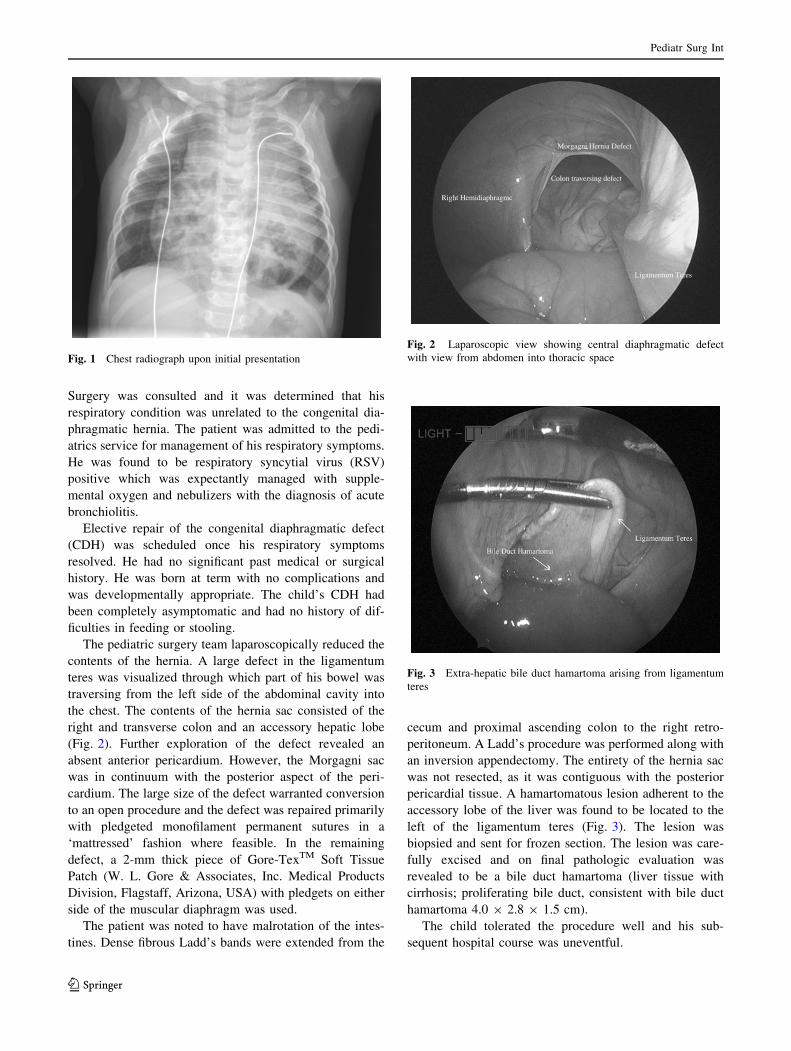
The pediatric surgery team laparoscopically reduced the
contents of the hernia. A large defect in the ligamentum
teres was visualized through which part of his bowel was
traversing from the left side of the abdominal cavity into
the chest. The contents of the hernia sac consisted of the
right and transverse colon and an accessory hepatic lobe
(Fig. 2). Further exploration of the defect revealed an
absent anterior pericardium. However, the Morgagni sac
was in continuum with the posterior aspect of the peri-
cardium. The large size of the defect warranted conversion
to an open procedure and the defect was repaired primarily
with pledgeted monofilament permanent sutures in a
‘mattressed’ fashion where feasible. In the remaining
defect, a 2-mm thick piece of Gore-TexTM Soft Tissue
Patch (W. L. Gore & Associates, Inc. Medical Products
Division, Flagstaff, Arizona, USA) with pledgets on either
side of the muscular diaphragm was used.
The patient was noted to have malrotation of the intes-
tines. Dense fibrous Ladd’s bands were extended from the
cecum and proximal ascending colon to the right retro-
peritoneum. A Ladd’s procedure was performed along with
an inversion appendectomy. The entirety of the hernia sac
was not resected, as it was contiguous with the posterior
pericardial tissue. A hamartomatous lesion adherent to the
accessory lobe of the liver was found to be located to the
left of the ligamentum teres (Fig. 3). The lesion was
biopsied and sent for frozen section. The lesion was care-
fully excised and on final pathologic evaluation was
revealed to be a bile duct hamartoma (liver tissue with
cirrhosis; proliferating bile duct, consistent with bile duct
hamartoma 4.0 9 2.8 9 1.5 cm).
The child tolerated the procedure well and his sub-
sequent hospital course was uneventful.
Fig. 1 Chest radiograph upon initial presentation
Right Hemidiaphragmc
Colon traversing defect
Ligamentum Teres
Morgagni Hernia Defect
Fig. 2 Laparoscopic view showing central diaphragmatic defect
with view from abdomen into thoracic space
Fig. 3 Extra-hepatic bile duct hamartoma arising from ligamentum
teres
Pediatr Surg Int
123

Discussion
First described in 1918 by von Meyenberg, VMCs can only
be diagnosed histopathologically. Biliary hamartomas are
usually benign malformations of the hepato-biliary system,
are largely asymptomatic, and usually found during lapa-
rotomies or in 0.5 to 5.6 % of autopsies [2, 5]. To the best
of our knowledge, this is the first report of an extra-hepatic
VMC in the pediatric literature.
The most common variant of hepatobiliary fibrocystic
disease occurring as a result of ductal plate malformation is
the von Meyenberg complex. Persistence of the double-
layered ductal plate, that is a normal constituent of fetal
livers, post-natally is called ductal plate malformation. It is
postulated that interruption of hepatic ductal plate recon-
stitution and remodeling during the late phase of embryo-
logical biliary differentiation may lead to its occurrence [2,
6–8].
VMCs are diagnosed using imaging as well as through
biopsies. Typical imaging findings include multiple comet-
tail echoes on US, small hypodense lesions on CT dis-
persed throughout the liver, and a cystic appearance on
MRI [5, 8]. On ultrasound, hypoechoic and hyperechoic
foci are seen distributed uniformly among the liver, while
on the MRI, they appear as hypointense lesions on T1 and
hyperintense lesions on T2. Needle biopsies are also used
to diagnose VMCs and are especially useful due to the
possibility of mixing biliary hamartomas with liver
metastases, microabscesses, lymphoma, and simple liver
cysts. Biliary hamartomas are usually uniform in size and
distribution, while liver metastases are larger and have a
variable size and distribution [5, 8].
Bile duct hamartomas are gray to white lesions that are
normally small, measuring anywhere from 1 mm to 1.5 cm
and are multifocal and irregular in appearance. On micro-
scopic evaluation they consist of multiple, small to mod-
erate sized ductules. These ductules are cystically dilated
and are typically separated by dense collagenous bands of
stroma. Bile duct hamartomas are commonly situated
peripherally around the portal tracts and consist of irregu-
larly shaped cystic spaces containing eosinophilic frag-
ments and inspissated bile that help differentiate these
lesions from normal ducts. The cells lining the ductules are
flattened, cuboidal cells that are distinguished by their
well-circumscribed, round to oval nuclei [8–10]. They are
typically composed of multiple lesions that are less than
1.5 cm each and are generally dispersed throughout the
liver, especially in the subcapsular region [8]. However,
solitary lesions have been discovered [5].
It is pertinent to note here that the VMC in our patient
had an extra-hepatic location. The lesion was found on top
of the accessory lobe of the liver, located to the left of the
ligamentum teres. This may have been brought about as a
result of ectopic hepatic tissue adherent to the ligamentum
teres.
Literature on the nature and natural history of this
seemingly benign lesion remains scarce. Some cases were
associated with polycystic liver and kidney disease, pan-
creatic cysts, and simple liver cysts [8]. Ductal plate mal-
formations (DPM), which include VMCs, are associated
with an increased incidence of hepatic malignancy
including cholangiocarcinoma, hepatocellular carcinoma,
adenosquamous carcinoma, squamous cell carcinoma, and
papilloma [6]. There is also a positive correlation between
bile stasis and the development of malignancy in DPMs
[6]. Thus far, only a few cases have been reported in the
literature of neoplastic transformation of VMCs [6]. Fur-
thermore, VMCs that progress to a neoplasm have a low
metastatic potential [6].
Some studies suggest that patients with VMCs have a
greater chance of developing hepatic carcinoma. However,
the rate of occurrence of hepatic carcinoma is thought to be
proportional to the size of the lesion. Bile duct hamartomas
or VMCs can also rarely undergo malignant transformation
to cholangiocarcinoma [6, 11, 12]. However, some of the
literature suggests that the association of cholangiocarci-
noma with VMCs is likely an under recognized phenom-
enon due to the obtainment of small sample sizes from
patients and misdiagnosis of cholangiocarcinoma as HCC
[6].
The nature of his disease and the consequent interven-
tion brought this interesting lesion to medical attention,
which may have gone unnoticed otherwise.
References
1. Thommesen N (1978) Biliary hamartomas (von Meyenburg
complexes) in liver needle biopsies. Acta Pathol Microbiol Scand
A 86(2):93–99
2. Redston MS, Wanless IR (1996) The hepatic von Meyenburg
complex: prevalence and association with hepatic and renal cysts
among 2843 autopsies [corrected]. Mod Pathol 9(3):233–237
3. Terada T, Moriki T (2010) Monolobar ductal plate malformation
disease of the liver. Pathol Int 60(5):407–412
4. Nagano Y et al (2006) Bile duct hamartomas (von Mayenburg
complexes) mimicking liver metastases from bile duct cancer:
MRC findings. World J Gastroenterol 12(8):1321–1323
5. Venkatanarasimha N et al (2011) Imaging features of ductal plate
malformations in adults. Clin Radiol 66(11):1086–1093
6. Jain D et al (2000) Evidence for the neoplastic transformation of
von-Meyenburg complexes. Am J Surg Pathol 24(8):1131–1139
7. Rocken C et al (2000) Cholangiocarcinoma occurring in a liver
with multiple bile duct hamartomas (von Meyenburg complexes).
Arch Pathol Lab Med 124(11):1704–1706
8. Zheng RQ et al (2005) Imaging findings of biliary hamartomas.
World J Gastroenterol 11(40):6354–6359
9. Wei SC et al (1997) Bile duct hamartomas. A report of two cases.
J Clin Gastroenterol 25(4):608–611
Pediatr Surg Int
123

10. Zen Y et al (2006) Multicystic biliary hamartoma: a hitherto
undescribed lesion. Hum Pathol 37(3):339–344
11. Kim YW et al (1999) A case with intrahepatic double cancer:
hepatocellular carcinoma and cholangiocarcinoma associated
with multiple von Meyenburg complexes. Yonsei Med J
40(5):506–509
12. Song JS et al (2008) Cholangiocarcinoma arising in von Mey-
enburg complexes: report of four cases. Pathol Int 58(8):503–512
Pediatr Surg Int
123





























