Embed Size (px)
Citation preview

Extern ConferenceOphthalmia Neonatorum

A 17-day-old female term newborn
• CC: purulent discharge from Rt eye for 3 days
• PI:
• 7 d PTA, Rt eye showed whitish-grey watery discharge and tear but no eyelid swelling was detected.
• 3 d PTA, Rt eyelids were red and swelled with occasional bloody-purulent discharge.
• She was treated by topical ATB and eye irrigation with sterile water but these symptoms did not improve.
• She had no fever, no drowsiness, no URI symptoms. She was breast-fed well.
Case presentation
• Birth history: G1P0A0, GA 38 wks, NL, Apgar 10,10 BW 3,090 g, length 50 cm, HC 33 cm
• There was no complication after delivery.
• History of pregnancy: • serology : neg • no maternal history of STD• amniotic membrane ruptured 7 hr before
delivery• mother had no fever or vaginal discharge.
• Family history: no genetic or contagious disease
• No history of drug allergy
• Vaccine: BCG, HBV1
History

Physical examination
BW 3,700 g (P50-75), length 54 cm (P75-90). HC 35 cm (P50)
V/S: T 36.8°C, P 168/min, R 40/min
GA: active and non-toxic child, not irritable, not pale, no jx, no dyspnea, no signs of dehydration
HEENT: pharynx and tonsils are not injected Rt eye: red and mildly swollen eyelid,
marked conjunctival injection with purulent and bloody discharge, clear cornea, EOM and VA cannot be evaluated Lt eye : normal
Physical examination
CVS: normal S1, S2, no murmur
RS: normal breath sound, no adventitious sound
Abd: soft, not tender, no hepatosplenomegaly
NS: normal movement, Brudzinski’s sign negative
Problem list
1. Unilateral purulent discharge (Rt eye)2. Mild eyelid swelling with marked conjunctival injection (Rt eye)

Differential Diagnosis
• Ophthalmia neonatorum (neonatal conjunctivitis)
• Neonatal dacryocystitis• Periorbital cellulitis

Ophthalmia neonatorum: in this patient
Pros• Age of onset• Clinical symptoms• Most common cause in newborn
Cons• No history of maternal infection or vaginal discharge
Differential Diagnosis
-Schachter, J, Grossman, M. Chlamydia. In: Infectious Diseases of the Fetus and Newborn, 5th ed, Remington, JS, Klein, JO (Eds), WB Saunders, Philadelphia 2001. p.769. -de Toledo AR, Chandler JW: Conjunctivitis of the newborn. Infect Dis Clin North Am1992 Dec; 6:807-13

Neonatal Dacryocystitis• onset 2-4 wk • Tenderness & swelling in medial canthal region• Epiphora most prominent • ± purulent D/C from puncta, cellulitis, conjunctivitis,
Differential Diagnosis
• Epiphora was not eminent• No tenderness & swelling in medial canthal region
In this patient
Lang, Gerhard K., Ophthalmology: a short textbook, 2000 Georg Thieme Verlag, Germany

Periorbital cellulitis• Local spread (preceded with URI) • Acute eyelid erythema and edema• Pain, epiphora• ± fever, conjunctivitis,
Differential Diagnosis
In this patient
• Mild eyelid edema• No Hx of URI, hordeolum, bug bite, trauma• Discharge more prominent than swelling
Malinow I, Powell KR: Periorbital cellulitis. Pediatr Ann 1993 Apr; 22:241-6
, leukocytosis

Causes Clinical symptoms
Associated findings
Neonatal conjunctivitis
Maternal infection
Discharge, conjunctivitis
Maternal STD
Neonatal dacryocystitis
Obstruction of lacrimal system
Epiphora, tenderness at epicanthal region
Nasal diseases
Periorbital cellulitis
Local spread Marked eyelid edema
URI
Differential Diagnosis
Approaching pediatric conjunctivitis
History
• Maternal/paternal infection during pregnancy
esp. STD
• Onset, severity, characters of discharge
• Associated symptoms, preceding illness
• Possible causes of illness (trauma, bug bites)
Physical examination• eyelid eversion: hyperemia, follicles, papillae, membranes• Characters and amount of discharge (purulent, mucoid, watery, bloody) • Detailed eye exam if possible (EOM, VA, pupillary reaction, proptosis)• Preauricular lymphadenopathy• Systemic manifestation (fever, pneumonia, sinusitis, meningitis, arthritis)
Approaching pediatric conjunctivitis

Ophthalmia neonatorum

Ophthalmia neonatorum
• Neonatal conjunctivitis – during the first mo• Aseptic – chemical: silver nitrate• Septic – bacteria, chlamydia, virus
• Septic neonatal conjunctivitis• Neisseria gonorrhoeae (GC) – most serious• Chlamydia trachomatis – most common• Non-gonococcal, non-chlamydial
• Acquire during passing through the birth canal
Incidence
• One of the most common eye disease
in neonate • Incidence ranging from 1.6-12.0%
Weiss AH. Conjunctivitis in neonatal period. In Long S, Pickening LK, Prober CG (eds): Principle and practice of pediatric infectious disease, 2003, pp 486-89.

Clinical presentation
• Common findings:erythema and edema of the eyelidsconjunctival injectionchemosiswatery to purulent eye discharge
• More specific findings for different causative agents

Clinical presentationSilver nitrate
GC Chlamydia Herpes
Onset Day 1 Day 3-5 Day 5-14 Day 6-14
Character Transient, disappear in 2-4 days
Hyperacute, purulent
Acute, varying in severity
Corneal epith defects
Affected eye Bilat Bilat Uni or bilat Uni or bilat
Corneal involvement
No Edema, ulcer, perforation
No
(eyelid scarring, pannus)
Geographic ulcers
Extraocular No Maybe Maybe (pharyngeal colonization, pneumonitis, otitis)
Vesicles on the skin or lid margin, others
Adapted from: Weiss AH. Conjunctivitis in neonatal period. In Long S, Pickening LK, Prober CG (eds): Principle and practice of pediatric infectious disease, 2003, pp 486-89.
Investigation• When to perform?
• Look more severe• Persist than 2-3 days or progress• First appear after the first day of life
Cited from: Weiss AH. Conjunctivitis in neonatal period. In Long S, Pickening LK, Prober CG (eds): Principle and practice of pediatric infectious disease, 2003, pp 486-89.
Gram stainconjunctival exudate

Histologic study
Ophthalmia neonatorum
Chemical conjunctivitis
Bacterial conjunctivitis
Chlamydial conjunctivitis
Gram stain
neutrophils, lymphocytes
neutrophils, bacteria
neutrophils, lymphocytes, plasma cells
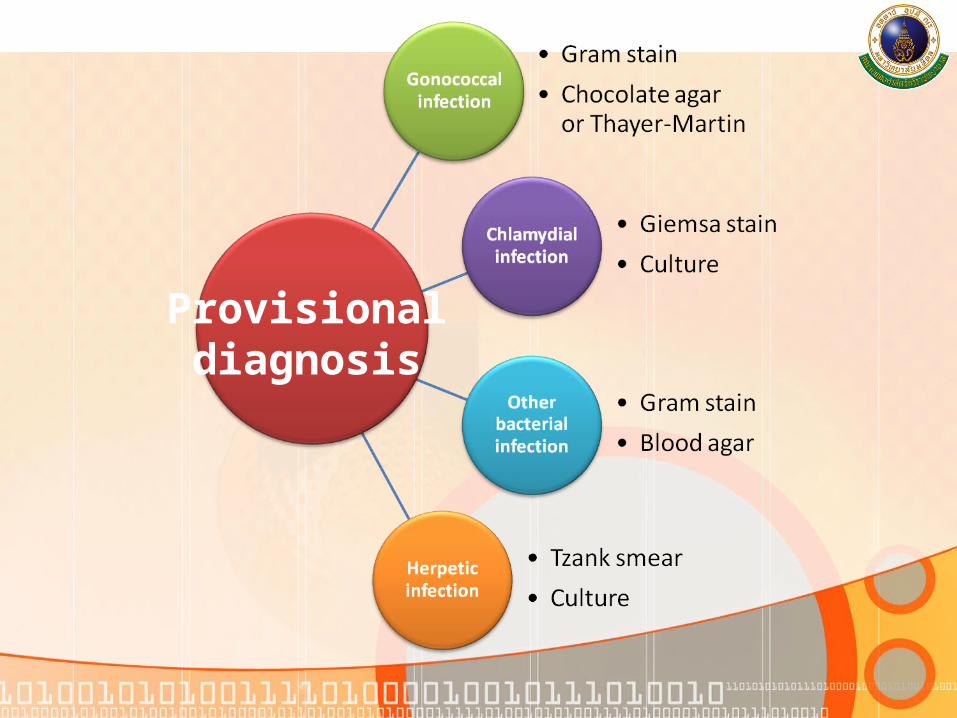
Provisionaldiagnosis

Gonococcal infection

Investigation for Chlamydial infection
• Conjunctival scraping for chlamydia• Giemsa stains from lower conjunctiva
• intracytoplasmic inclusion bodies• Do not collect from ocular discharge alone
• Culture• Non-culture method
• Direct immunofluorescent antibody assay• Nucleic acid amplification tests (PCR)
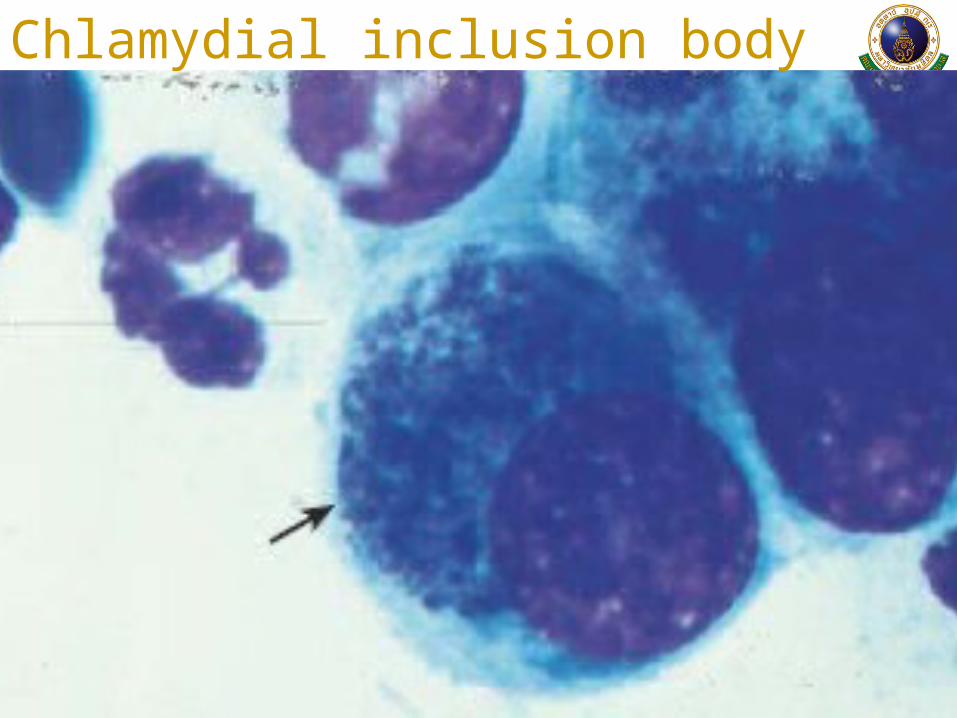
Chlamydial inclusion body
Management
1. If there are systemic symptoms, admit the patient for specific treatments and further investigation
2. Laboratory investigations include discharge G/S, cultures
3. IV or IM third-generation cephalosporin should be given before laboratory results
4. Topical ATB is not necessary5. Consult ophthalmologist
Specific treatment
1. Gonorrhea conjunctivitis (non-disseminated)
• Admit and separate patient from other babies
• Ceftriaxone 25-50 mg/kg/day IM single dose not to exceed 125 mg.
• Irrigated with NSS frequently until discharges disappear
• Treat parents
2. Chlamydia conjunctivitis
• Erythromycin oral 50 mg/kg/day qid for 14 days
• 0.5% erythromycin ointment tid/qid for 3 wks (unnecessary but may be adjunctive)
• Irrigated with NSS frequently until discharge disappear
• Treat parents
Red Book: 2006 Report of the Committee on Infectious Diseases. 27th ed.
Prophylaxis
• Baby that born from Gonorrhea-infected
mother
• Ceftriaxone 25-50 mg/kg/day (max 125 mg)
IM single dose stat or aqueous pen-G
100,000 U IV single dose
• The American Academy of Pediatrics and
the U.S. Centers for Disease Control(CDC)
1% silver nitrate solution
0.5% erythromycin ointment
1% tetracycline ointmentRed Book: 2006 Report of the Committee on Infectious Diseases. 27th ed.

16/4/50 (Day 1)
• Admit (consult ophthalmologist: r/o orbital
cellulitis)
• Observe clinical signs: sepsis
• RE: mild lid swelling, not tensed, erythema;
conjunctival injection with chemosis; purulent
bloody discharge wih pseudomembrane, full
EOM
Progression
16/4/50 (cont.)
• Investigation
• G/S of discharge: numerous PMN, no organism
• Giemsa staining of conjunctival scraping: pending
• Discharge culture for GC, bacteria, Chlamydia trachomatis: pending
• CBC: Hb 12.7 g/dL Hct 38.1% WBC 11640/mm3 N30.5% L 49.7% M16.2% E3.4% B0.2% plt 343000/mm3
Progression
16/4/50 (cont.)• Imp: Ophthalmia neonatorum,
suspected C. trachomatis conjunctivitis
• Start ATB covering GC and Chlamydia• Ceftriaxone 50 mg/kg/day iv over 30 min, single
dose
• Erythromycin Syr 50 mg/kg/day for 14 days
• Topical ATB : erythromycin ed. (Tobrex ed. instead)
• Evaluate and treat mother OPD Gynae
Progression

17/4/50 (Day 2)S: active child, afebrileO: RE: eyelid swelling, soft;
conjunctival injection with chemosis; purulent bloody discharge; normal cornea
A: not worseP: continue treatment18/4/50 (Day 3)• Giemsa stain (16/4/50): not appropriate specimen• Repeated conjunctival scaping for Giemsa• Zymar (Gatifloxacin) ed to RE q 2 hr (12.5 MKdose)
Progression
19/4/50 (Day 4)
• Afebrile
• RE: eyelid not swelling, conjunctiva-mildly injected, small amount of discharge, clear cornea
• Plan F/U OPD eye 1 week, with Giemsa stain result
Progression

• NB with conjunctivitis are at risk of systemic infection
• Hx of mother (ANC, STD, perinatal Hx) and child
• Complete PE
• Treat for GC if it cannot be ruled out and admit if there is evidence of systemic infection.
• Presumptive treatment is based on the clinical picture, G/S and Giemsa
• Systemic ATB, not just ATB eye drop, is recommended. (Chlamydia, GC, HSV)
• Evaluate and treat the parents.
Take home message

References1. American Academy of Pediatrics. Red Book: 2006 Report of the
Committee on Infectious Diseases. 27th ed. Elk Grove Village, IL:
American Academy of Pediatrics; 2006:401–411
2. de Toledo AR, Chandler JW: Conjunctivitis of the newborn. Infect
Dis Clin North Am1992 Dec; 6:807-13
3. Lang, Gerhard K., Ophthalmology: a short textbook, 2000 Georg
Thieme Verlag, Germany
4. Malinow I, Powell KR: Periorbital cellulitis. Pediatr Ann 1993
Apr; 22:241-6
5. Weiss AH. Conjunctivitis in neonatal period. In Long S,
Pickening LK, Prober CG (eds): Principle and practice of
pediatric infectious disease, 2003, pp 486-89.
6. Schachter, J, Grossman, M. Chlamydia. In: Infectious Diseases of
the Fetus and Newborn, 5th ed, Remington, JS, Klein, JO (Eds),
WB Saunders, Philadelphia 2001. p.769

Thank you for your attention