Embed Size (px)
Citation preview

(CANCER RESEARCH 52. 3460-3466. June 15, 19921
Expression of Class II Major Histocompatibility Complex Molecules Correlateswith Human Colon Tumor Vaccine EfficacyJanet H. Ransom,1 Barbara Pelle, and Michael G. Hanna, Jr.
Organati Teknika, Biotechnology Research Institute, Rockrille, Maryland 20850
ABSTRACT
Vaccination of colon cancer patients with \-irradiated autologoustumor cells and Bacillus Calmette-Guerin results in a significant reduc
tion in tumor recurrence. A study was undertaken to determine whetherthe expression of tumor-associated antigens, expression of major histo-
compatibility complex molecules, or the cellular composition of thevaccine cells correlates with vaccine efficacy. A significant increase inthe percentage of histocompatibility leukocyte antigen (HLA) class IImolecule-expressing tumor cells was the only marker with a positive
correlation. Because HLA class II molecule expression is not a prognosticmarker in control patients, it was hypothesized that HLA class IImolecules are involved in the induction of tumor immunity in patientstreated with the autologous colon tumor vaccine. Enhancement of HLAclass II molecule-expressing cells could be induced in \-irradiated colon
tumor cells injected into the skin of mice when the cells were mixed with•¿�v-interferon.Therefore, addition of -y-interferon to the colon tumor
vaccine, resulting in increased numbers of HLA class II molecule-
expressing cells, could potentiate the generation of tumor immunity.
INTRODUCTION
Active specific immunotherapy of colon cancer has beenachieved by administering a vaccine composed of enzymaticallydissociated, X-irradiated, autologous tumor cells admixed withBCG2 to patients (1, 2). In a 65-month median follow-up of a
prospectively randomized phase II clinical trial designed toevaluate the autologous colon tumor vaccine. Hoover andHanna (3) reported a significant increase in time to tumorrecurrence. They observed a 21% rate of recurrence in theimmunotherapy group versus 52% in the surgery-only controls.Although not statistically significant, they reported 12.5% mortality after immunotherapy and 30% after surgery alone. Tumorimmunity developed, as demonstrated by the delayed cutaneoushypersensitivity response to autologous tumor cells (4), whichappeared to correlate with clinical outcome (3). In this paper,an immunohistochemical analysis of the vaccine cells was performed to determine whether any cell-associated markers correlate with vaccine efficacy, such that the possible reasons whynot all immunized patients were cured can be elucidated.
Expression of three different classes of markers was considered for evaluation: (a) phenotypic markers indicative of thevaccine's cellular composition, (b) tumor-associated antigens,
and (c) major histocompatibility complex molecules. It washypothesized that vaccine efficacy could result simply from thetotal cellular composition of the vaccine, i.e., vaccines that wereineffective could have contained more normal cells and leukocytes than immunizing tumor cells. To discriminate among thecolon tumor cells, normal fibroblasts, and leukocytes in the
Received 9/3/91; accepted 3/30/92.The costs of publication of this article were defrayed in part by the payment
of page charges. This article must therefore be hereby marked advertisement inaccordance with 18 U.S.C. Section 1734 solely to indicate this fact.
' To whom requests for reprints should be addressed, at Organen Teknika/Biotechnology Research Institute. 1330-A Piccard Drive. Rockville. MD 208SO.
2The abbreviations used are: BCG. Bacillus Calmette-Guérin;HLA, humanleukocyte antigen; HBSS, Hanks' balanced salt solution; MHC. major histocompatibility complex; PBS. phosphate-buffered saline; SCID. severe combinedimmunodeficient.
dissociated tumor cell suspension, two sets of phenotypic markers were chosen. Because colon carcinomas are of epithelialorigin, the malignant cells present in the vaccine should expresscytokeratin 18. The normal fibroblasts of mesenchymal originexpress the intermediate filament protein vimentin. Leukocytesalso express vimentin. However, because leukocytes are morphologically distinguishable from the tumor cells and normalfibroblasts, vimentin-positive leukocytes were not enumeratedwhen the presence of normal mesenchymal and malignantepithelial cells in the vaccines was quantitated. It is possiblethat, although irradiated, these metabolically active leukocytesmay play a role in host immune recognition, by secretingbioactive lymphokines.
A number of colon tumor-associated antigens have beenidentified and characterized using human and mouse monoclonal antibodies. If the expression of one or more of these antigenson the vaccine cells correlates with a positive clinical outcome,this antigen could possibly be used as the primary vaccine or asan adjuvant to the cellular vaccination. Haspel et al. (5, 6) haveimmortalized and cloned cells producing colon tumor-reactivehuman monoclonal antibodies, from patients undergoing activespecific immunotherapy. These antibodies were selected because they have specificity for tumor-associated antigens, theyrecognize cell surface and cytoplasmic determinants, and somehave been shown to localize to tumor in human colon carcinomapatients (7-11). Moreover, because these antibodies are theproducts of the human immune response to an autologoustumor, our supposition is that their respective antigens wouldbe more relevant to tumor immunity than those isolated afterimmunization of mice. Carcinoembryonic antigen and tumorassociated antigen-72 (TAG-72) are well characterized antigensassociated with colon carcinoma and recognized by murinemonoclonal antibodies, which have also been used successfullyfor imaging of colon tumors (12,13). HER2 is a proto-oncogenethat has been reported to have prognostic significance in breastcancer (14) and also has been shown to be expressed by coloncarcinomas (15), but whose prognostic significance for coloncarcinoma is not known. Monoclonal antibodies to mono-morphic determinants of HLA-ABC (class I) and HLA-DR,-DP, and -DQ (class II) molecules were also used to characterizethe vaccine tumor cells. HLA class I and class II molecules ofthe MHC are the cell surface molecular structures that presentantigens to cytotoxic T lymphocytes and T helper/inducerlymphocytes, respectively (16-18). MHC molecules are expressed on a variety of neoplasms, with apparent wide variationin expression and differences in prognostic implication, depending upon the type of malignancy (19-22). However, reportshave indicated that the MHC has a role in tumor resistance(23, 24). We sought to determine whether MHC moleculeexpression played a role in conferring tumor immunity.
MATERIALS AND METHODS
Colon Tumor Vaccines. Tumors were obtained at the time of surgeryand, with the assistance of a surgical pathologist, non-necrotic tumortissue was dissected, minced with a scalpel, and dissociated into a
3460
on May 17, 2020. © 1992 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

HUMAN COLON TUMOR VACCINE CHARACTERIZATION
TABLE 1 Characteristics of monoclonal antibodies used for colon carcinoma vaccine characterization
Antibody characteristics Antigen characteristics
Antibody Species Isotype Identification Character
Tissue markers
Leukocyte markersSK3/SK4SKI
L27S-HCL-3
Tumor antigens81AV7879AV829104MV14888BV5979AV101781AV117B72.3mAbl
SC20
HLA antigens
Mouse
Mouse
MouseMouse
MouseMouse
HumanHumanHumanHumanHumanHumanMouseMouse
Mouse
IgG
IgG
IgGIgG
IgGIgG
IgMIgMIgMIgGIgAIgAIgGIgG
IgG
Cytokcratin 18
Vimentin
CD4CDS
CD20CDI1C
CTAA81AV78CTAA 79AV829CTAA 104MV148CTAA 1688CTAA79AV1017CTAA81AV117TAG-72HER-2/neu
CEA
Intermediate filament ofepithelial cells
Intermediate filament ofmesenchymal cells
Helper T cellsCytotoxic/suppressor T
cellsB cellsMacrophages
Cell surface phospholipidCell surface proteinCell surface proteinAltered cytokeratinsCell surface proteinCytoplasmic proteinCell surface mucinProto-oncogene epider
mal growth factor receptor-like
Carcinoembryonic antigen
M736
M704
B7/21
SK10Mouse
Mouse
Mouse
MouseIgG
IgG
IgG
IgGHLA-ABC
HLA-DR
HLA-DP
HLA-DQClass
I molecules; cyto-toxic T cell recognition
Class 11molecules; Thelper cell induction
Class II molecules; Thelper cell induction
Class II molecules; Thelper cell induction
single-cell suspension with collagenase and DNase (25). Cells werecryopreserved and maintained in the vapor phase of a liquid nitrogencylinder until prepared for either patient vaccination or marker characterization. Cells used for characterization were surplus dissociatedcells obtained from the tumors of patients in the reported phase II trial(1, 2). Due to the limited clinical material, marker analysis was performed once for each patient.
Monoclonal Antibodies. The monoclonal antibodies described in Table 1 were used to quantitate expression of the three classes of markersused for vaccine characterization. All of the human monoclonal antibodies were provided by M. V. Haspel (Organon Teknika/Biotechnol-ogy Research Institute, Rockville, MD). The specificity and biochemicalcharacteristics of their cognate antigens have been described (7-11).SC20 was provided by B. T. Butman (Organon Teknika/BiotechnologyResearch Institute). B72.3 was a gift from J. Schlom (National CancerInstitute, Bethesda, MD). M736 and M704 were from DAKO (SantaBarbara, CA). mABl was from Triton Biosciences (Alameda, CA). Theantibodies to intermediate filament proteins were from Behring Diagnostics (Somerville, NJ). The remaining antibodies were from BectonDickinson Corp. (Hialeah, FL). The concentrations of monoclonalantibodies ranged from 1 to 10 Mg/ml and were selected based onoptimal reactivity, with no nonspecific binding. Appropriate class-matched control antibodies were used, and no background reactivitywas observed.
Immunohistochemical Analysis. Twenty thousand cells from colla-genase/DNase-dissociated, cryopreserved, colon tumors were thawedin HBSS with 10% fetal bovine serum, cytocentrifuged onto slides, airdried, and frozen at —¿�70°C.The cells were stained by incubating the
slide in 25 /nlof an appropriate concentration of monoclonal antibodyfor 2 h at room temperature, washing with PBS, incubating for l hwith 25 fil of an appropriate concentration of peroxidase-conjugatedgoat anti-human IgM or goat anti-mouse IgG (KPL Laboratories,Gaithersburg, MD), washing with PBS, incubating for 40 min with 3-amino-9-ethylcarbazole substrate (Sigma, St. Louis, MO), washing withPBS, and counterstaining for 5 min with hematoxylin. The exceptions
Table 2 Comparison of cell marker expression with clinical course in patientsvaccinated with the autologous colon tumor vaccine
Percentage of positive cells"
Marker
Tissue markersCytokeratin 18Vimentin
Leukocyte markersCD4CDSCD20CD11C
Tumor markers81AV7879AV829104MV14888BV5979AV101781AV117TAG-72HER-2CEA
HLA moleculesHLA-ABCHLA-DRHLA-DPHLA-DQ
No. of patients
NED REC
55 ±1841 ±13
23 ±1411 ±721 ±1040 ±9
38 ±1842 ±1822 ±2027 ±123±6
11 ±18I4±1224 ±1557 ±28
87 ±2148 ±2445 ±2227 ±15
10
55 ±1837 ±16
23 ±1710±16I4±1532 ±15
37 ±1642 ±1712±1429 ±II8±II
14 ±13II ±1024 ±2367 ±19
95 ±824 ±1223 ±2118±16
NSC
NS
NSNSNSNS
NSNSNSNSNSNSNSNSNS
NS0.020.04NS
" NED, no evidence of disease; REC, tumor recurrence. Values are mean ±
SD.* Probability by Student's / test (two-tailed), performed on the transformed
percentages using the arcsin of the square root of the percentage (32), that astatistically significant difference exists between the groups with no evidence ofdisease and those with tumor recurrence. The P values reported are not correctedfor bctween-group comparisons.
NS, not significant at P = 0.05.
3461
on May 17, 2020. © 1992 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

HUMAN COLON TUMOR VACCINE CHARACTERIZATION
to this were that the human IgG and IgA monoclonal antibodies usedwere conjugated directly to biotin, to minimize background staining,and binding was visualized with an avidin-biotin-peroxidase complex(Vector Laboratories, Burlingame, CA), using 3-amino-9-ethylcarba-zole as the substrate.
In a blind coded fashion, at least 200 cells were enumerated forpositive or negative reactivity, by microscopic examination. Counting200 cells was found to yield a difference in enumeration of identicallystained slides of <7%. The intensity of a positive staining reaction wasdramatic with all of the antibodies used in this study and, therefore,discrimination between positive and negative staining was clear. Onlynonleukocytic cells were enumerated for expression of tumor-associatedantigens, intermediate filament proteins, and major histocompatibilitycomplex molecules. The leukocyte antigen expression represents thepercentage of positive cells in the leukocyte population alone.
Up-regulation of MHC Molecules. 7-Interferon was used to determine whether MHC molecule expression could be up-regulated in anin vivo model of the colon carcinoma vaccine. 7-Interferon dose-response studies were initially performed in vitro. One million tumorcells were plated in 10 ml of RPMI 1640, 10% fetal bovine serum, 50Mg/ml Gentamicin, in 100-mm tissue culture dishes. Of the four tumorcell lines used, two were the established colon tumor lines HT-29 andWiDr (obtained from the American Type Culture Collection, Rockville,MD), and the other two were early-passage colon tumor cell lines, CWand HAR (obtained after 10 population doublings), established in ourlaboratory from dissociated primary colon tumors. After a 24 h incubation at 37*C in a 95% air-5% CO2 incubator, 7-interferon, in increas
ing concentrations from 0 to 0.7 ¿ig/ml,was added and an additional48-h incubation was performed. 7-Interferon (specific activity, 1.5 xIO7units/mg) was obtained from Genentech, Inc. (South San Francisco,CA). The cells were harvested after brief trypsinization, and 5 x IO5
cells were incubated with 100 p\ of 1 Mg/ml anti-HLA-ABC, anti-HLA-DR, or IgG control monoclonal antibodies (as described in Table 1),for l h on ice. After washing with HBSS, 0.01% sodium azide, 1%bovine serum albumin, the cells were incubated for l h with fluoresceinisothiocyanate-conjugated goat anti-mouse IgG (diluted 1:50; KPL,Gaithersburg, MD), on ice. After washing, the cells were subjected toflow cytometric analysis, using an Epics C flow cytometer (Coulter,Inc., Hialeah, FL). The results are expressed as percentage of fluorescent cells and, when increases in marker expression were analyzed, asincrease in mean positive channel number (determined by subtractingthe mean channel number of positively staining cells of the untreatedcontrol from the mean positive channel number of the treated cells).
In the i/i vivo MHC up-regulation experiments, cells were preparedsimilarly to preparation of the autologous human colon tumor vaccine(1). The same four cell lines described above were harvested fromculture. The cells were suspended in 10 ml of HBSS and X-irradiated,for a total dose of 20,000 rad, in a Nordion Gamma-cell Elite irradiator(Ontario, Canada). After centrifugation, IO7cells were resuspended in0.1 ml of HBSS containing IO7 colony-forming units of BCG andgraded doses of 7-interferon and were injected intradermally into theskins of SCID mice. SCID mice were chosen to eliminate participationof host immunological factors. After 2 days, the injection site wasexcised and immediately frozen in optimal cutting temperature compound (OCT) suspended in liquid nitrogen. Serial sections were cut ona cryostat, and immunohistochemical staining for expression of MHCmolecules was performed as described above. At least four microscopicfields (x400 magnification) were enumerated for positively stainingcells (approximately 1000 cells).
RESULTS AND DISCUSSION
Immunohistochemical analysis of marker expression was performed on vaccine cell cytospins from patients who had under-
100
wua
coOBUHZuUoÃ
.0007 .007 .07UG GAMMA-INTERFERON/ML
.7
ILICO
OÃUZ
JwZ•¿�z.<Xuz<w
.0007 .007 .07UG GAMMA-INTERFERON/ML
.7
UUfu
coOo.H
tau«wCU
.0007 .007 .07UG GAMMA-INTERFERON/ML
.7 .0007 .007 .07UG GAMMA-INTERFERON/ML
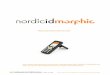
Fig. 1. In vitro dose-response studies of 7-interferon up-regulation of MHC molecules. Cells, CW (*), HAR (•).WIDR (A), and HT-29 (•),were exposed tovarying concentrations of 7-interferon for 2 days and analyzed by flow cytometry for percentages of HLA-DR- (A) or HLA-ABC-positive (C) cells or increases inmean positive channel number for HLA-DR (fi) and HLA-ABC (D).
3462
on May 17, 2020. © 1992 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

HUMAN COLON TUMOR VACCINE CHARACTERIZATION
gone active specific immunotherapy. The data were sorted intotwo groups. The first group contained data from patients whoremained disease free after at least a 5-year follow-up from thetime of vaccination. The second group was from patients whosetumor recurred after vaccination. We were looking for a difference in markers among the two groups that would be indicativeof a possible role in the induction of tumor immunity. As canbe seen in Table 2, the colon tumor vaccines were composed ofcolon carcinoma cells, fibroblasts, and leukocytes that hadinfiltrated the tumor. About one half of the nonleukocytic cellsin the vaccine expressed the intermediate filament cytokeratin18. This suggests that only half of the nonleukocytic cells inthe vaccine are carcinoma cells that are of epithelial origin. Thenumber of infiltrating leukocytes ranged from 36 to 67% of thetotal cells in the vaccine (data not shown). The vaccine contained macrophages, CD4+ and CD8+ T cells, and B cells.
There were no significant differences in the cellular compositionof the vaccine in the two groups of vaccinated patients, regardless of their clinical outcome. This suggests that the differencein vaccine efficacy was not due simply to the total numbers oftumor and other cell types.
There were also no significant differences in the expressionof any of the tumor-associated antigens between the two groups(Table 2). Therefore, no indication of the importance of a tumorantigen for induction of tumor immunity was evident. Therewere, however, significant differences in expression of HLAmolecules between the two groups (Table 2). Vaccine tumorcells from both groups had high levels of expression of H LA-ABC markers. Vaccine tumor cells in patients with no evidenceof disease had statistically significantly higher levels of expression of both the HLA-DR and HLA-DP molecules than foundon the tumor cells from patients whose tumors recurred aftervaccination. There was a somewhat lesser expression of HLA-DQ molecules on the tumor cells, with no significant differencesbetween the two groups. HLA class II molecules (HLA-DR andDP) present antigen to T helper cells. Even though the studygroups were not large, because the differences were statisticallysignificant it is compelling to speculate that increased expression of these two HLA class II molecules in the vaccines ofpatients who were rendered disease free suggests that the HLAclass II molecules on the tumor cells in the vaccine may playan active role in the development of tumor immunity. Hannaet al. (26) have reported that an inadequate number of tumorcells in the vaccine renders the vaccine ineffective. Therefore,having the appropriate numbers of tumor cells expressing HLA-DR and -DP molecules in the vaccines of patients who had noevidence of disease may be sufficient to drive the tumor immuneresponse adequately. Once T cell immunity is established, theresidual tumor, which has nearly 100% of cells expressing HLAclass I molecules, as demonstrated by the data in Table 2,possesses the appropriate target structures for recognition andelimination by cytotoxic T cells.
We next asked the question: do increased numbers of HLA-DR and -DP molecule-expressing cells correlate with vaccineefficacy, or are these markers just generally prognostic? Thesame set of HLA molecules, tumor markers, and tissue markerswere compared on dissociated cells from colon tumors of control patients who received surgery without vaccination and hadappropriate clinical follow-up. There were no statistically significant differences in MHC molecule expression in the twogroups of control patients, who either had no evidence of diseaseafter surgery or had recurring tumors (data not shown). This isconsistent with the findings of Möller et al. (27, 28), who
reported a lack of correlation between expression of HLA classI and class II molecules and survival of colon cancer patientstreated by surgical resection. Although HLA class II moleculeexpression has also not been prognostic in other tumors, anumber of investigators have reported correlations betweenmolecule expression on tumor cells and the effectiveness ofimmunotherapy. Cohen et al. (29) reported an association ofHLA-DR expression and response to interleukin 2 immunotherapy of melanoma. In follow-up studies, Rubin et al. (23)also found that pretreatment HLA-DR antigen expression wasnot predictive of clinical response but that regressing métastaseshad increased HLA-DR expression, compared with lesions thatdid not respond. Mitchell (30) has also reported that certainHLA subclass-specific antigens on an allogenic melanoma vaccine correlate with response rates. Furthermore, Prescott et al.(24) reported that HLA-DR molecules were expressed on regressing bladder tumors only after immunotherapy with BCG.In our study, there is no prognostic correlation with expressionof HLA class II molecules by colon tumors, but there is anassociation showing elevated numbers of tumor cells expressingHLA class II molecules in the vaccines of patients who werecured; this suggests that expression of these molecules is important to confer tumor immunity.
Another interesting observation found when comparingmarker expression with clinical course in control patients isthat the expression of the tumor marker recognized by the
auu
ViO2-
H"ZPJuOÃcucu
100
0.02 0.2 2.0 20.0UG GAMMA-INTERFERON INJECTED
_mU-
coOCUH
UUoÃ03CU
100
80
60
40
20
B
0.02 0.2 2.0UG GAMMA-INTERFERON INJECTED
20.0
Fig. 2. ¡nvivo dose-response studies of -y-interferon up-regulation of MHCmolecules. Cells, CW (»),HAR (•),WIDR (A), and HT-29 (•).were X-irradiatedwith 20.000 rads, mixed with 10' colony-forming units of BCG and varying dosesof -y-interferon, and injected intradermally into the skins of SCID mice. After 2days, the injection site was excised, frozen, sectioned, and stained for HLA-ABC(A) and HLA-DR (A) expression.
3463
on May 17, 2020. © 1992 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

HUMAN COLON TUMOR VACCINE CHARACTERIZATION
UNTREATEDCONTROL
UNTREATEDIgG CONTROL
IFN-y TREATED ,'HLA-ABC
IFN-y TREATEDHLA DR
IFN-, TREATEDIgG CONTROL
Sfèì
W¿IFN .TREATED
•¿�•IIgG CONTROL
Fig. 3. Photomicrographs of the stained frozen sections of the intradermal inoculation site of human tumor cells treated with -y-interferon, demonstration the up-regulation of HLA-DR expression in vivo. CW colon tumor cells (IO7) were X-irradiated with 20,000 rads, admixed with IO7 colony-forming units of BCG, andsuspended in either HBSS (top 4 panels) or HBSS with 0.3 jig of 7-interferon (lower 4 panels), aand injected intradermally in 0.1 ml into the dorsal flank of SCIDmice. After 2 days, the inoculation site was excised, frozen, sectioned, and stained indirectly for expression of HLA-ABC or directly with a biotinylated antibody toHLA-DR or with the appropriate IgG control antibodies, as described in Table 1. The appearance of the red 3-amino-9-ethylcarbazole substrate in a section isindicative of positive expression of a particular marker.
3464
on May 17, 2020. © 1992 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

HUMAN COLON TUMOR VACCINE CHARACTERIZATION
81AV78 human monoclonal antibody was elevated in controlpatient's tumors that did not recur after surgery (61 ±19%
positive for patients with no evidence of disease, compared to43 ±16% positive for patients whose tumors recurred; P =0.046). This human monoclonal antibody recognizes a lipidantigen, and these data suggest that this may have some prognostic implications. This warrants further study. There was noassociation with elevated 81AV78 antigen expression in thevaccinated patients, suggesting that this antigen is not criticalfor induction of tumor immunity in the vaccine setting.
If critical numbers of cells expressing HLA class II moleculesare required for effective vaccination, then we may be able toimprove the vaccine by augmenting the proportion of HLA-DR-expressing cells. The next set of experiments were designedto determine whether we could up-regulate the expression ofthe HLA molecules on a colon tumor vaccine after inoculationinto the skin of SCID mice. 7-Interferon has the ability to up-
regulate HLA class I and class II molecules on a variety of celltypes. In preliminary dose-response experiments performed invitro, four cell lines were selected. As can be seen in Fig. \A,none of the four cell lines expressed HLA-DR before 7-inter-feron treatment, but both the percentage of positive cells andthe fluorescent intensity per cell were maximally increased afterexposure to as little as 0.007 jig/ml 7-interferon (Fig. I, A andB). These four cell lines had relatively high percentages ofHLA-ABC-positive cells. 7-Interferon did not augment thepercentage of HLA-ABC-positive cells but did increase thefluorescent intensity per cell (Fig. 1, C and D). The data inFigs. 2 and 3 demonstrate that coinjection of irradiated colontumor cells with 7-interferon results in the up-regulation ofHLA-DR molecules in vivo. As was seen in vitro, the cells didnot express HLA-DR when 7-interferon was not included inthe inoculum (Figs. 2H and 3). The maximal expression in allfour cell lines was achieved at a dose of 2.0 ^g. All four celllines were induced to the same extent in vitro; however, theirin vivo responses and minimal dose-response varied (Fig. 2B).The percentages of HLA-ABC-positive cells (used as a positivecontrol for staining) were not as high as those in vitro and werenot as greatly affected by 7-interferon. Although these cellswere lethally irradiated, they were still sufficiently metabolicallyactive to respond to 7-interferon, via a mechanism believed toinvolve the induction of proteins that bind to the promoterregion of the MHC gene. Because the number of tumor cells ina vaccine is critical to confer tumor immunity (26, 31), theincrease in percentages of HLA-DR-expressing tumor cells inthe vaccine, which are capable of presenting tumor-associatedantigens to the immune system, may potentiate the development of tumor immunity.
In summary, enhanced expression of HLA class II moleculeson the tumor vaccine cells of colon carcinoma patients correlates with therapeutic effectiveness. This marker, however, isnot indicative of a good prognosis in patients not receivingimmunotherapy. No other tumor-associated antigen showedthis correlation and, therefore, could be identified as critical forvaccination. Augmentation of HLA class II molecule expressioncan be achieved by coadministration of the vaccine with 7-interferon, thereby possibly providing a means of enhancing theeffectiveness of colon cancer active specific immunotherapy.
ACKNOWLEDGMENTS
The authors would like to acknowledge Dr. James Murray forassisting in the establishment of the immunohistochemistry technology,
Suzie Longava for preparing the cryosections, and Leona Peters andJane Brandhorst for preparing and collecting the dissociated humancolon tumors.
REFERENCES
1. Hoover, H. C, Jr., Surdyke, M. G., Dangel, R. B., Peters, L. C, and Hanna.M. G., Jr. Prospectively randomized trial of adjuvant active specific immu-notherapy for human colorectal cancer. Cancer (Phila.), 55: 1236-1243,1985.
2. Hanna. M. G., Jr.. and Hoover, H. C.. Jr. Basic and applied principles ofactive specific immunotherapy in the treatment of metastatic solid tumors.In: R. Herberman, R. Wiltrout, and E. Gorlik (eds.). Immune Responses toMétastases,Vol. 2, pp. 95-115. Boca Raton, FL: CRC Press, Inc., 1987.
3. Hoover, H. C., Jr.. and Hanna, M. G., Jr. Immunotherapy by active specificimmunization: clinical applications, in: V. T. DeVita, S. Hellman, and S. R.Rosenberg (eds.), Biologic Therapy of Cancer, pp. 670-682. Philadelphia: J.P. Lippincott Co., 1991.
4. Hoover, H. C., Jr., Surdyke, M.. Dangel, R. B., Peters, L. C., and Hanna,M. G., Jr. Delayed cutaneous hypersensitivity to autologous tumor cells incolorectal cancer patients immunized with an autologous tumor cell: BacillusCalmette-GuérÃnvaccine. Cancer Res., 44: 1671-1676, 1984.
5. Haspel, M. V., McCabe, R. P., Pomato, N., Janesch, N. J., Knowlton, J. V.,Peters, L. C., Hoover, H. C., Jr., and Hanna, M. G., Jr. Generation of tumorcell reactive human monoclonal antibodies using peripheral blood lymphocytes from actively immunized colorectal carcinoma patients. Cancer Res.,45: 3951-3961, 1985.
6. Haspel, M. V., McCabe, R. P., Pomato, N., Hoover, H. C., Jr., and Hanna,M. G., Jr. Human monoclonal antibodies: generation of tumor cell reactivemonoclonal antibodies using peripheral blood lymphocytes from activelyimmunized colorectal carcinoma patients. In: R. A. Reisfeld and S. Sell(eds.), Monoclonal Antibodies and Cancer Therapy, pp. 505-522. New York:Alan R. Liss, Inc., 1985.
7. Steis, R. G., Carrasquillo. J. A., McCabe, R. P., Bookman, M. A., Reynolds,J. C, Larson, S. M., Smith, J. W., II, Clark, J. W., Dailey, V., Del Vecchio,S., Surdyke, N., Pinsky, C. M., Urba, W. J., Haspel, M. V., Perentesis, P.,Paris, B., Longo, D., and Hanna, M. G., Jr. Toxicity, immunogenicity, andtumor radioimmunodetecting ability of two human monoclonal antibodiesin patients with metastatic colorectal carcinoma. J. Clin. Oncol., 8:476-490,1990.
8. Murray, J. H., Longava, S., Haspel, M. V., McCabe, R. P., and Hanna, M.G., Jr. Tumor cell surface reactive human monoclonal antibodies generatedfrom peripheral blood lymphocytes of patients immunized with autologoustumor cells. Proc. Am. Assoc. Cancer Res., 31: 1682, 1990.
9. Pomato, N., Murray, J. H., Bos, E., Haspel. M. V., McCabe, R. P., andHanna, M. G., Jr. Identification and characterization of a human colontumor-associated antigen, CTAA 16-88, recognized by a human monoclonalantibody. In: R. S. Metzger and M. S. Mitchell (eds.). Human TumorAntigens and Specific Tumor Therapy, pp. 127-136. New York: Alan R.Liss, Inc., 1989.
10. McCabe, R. P., Haspel, M. V., Pomato, N., Steis, R. G., Carrasquillo, J. A.,and Hanna, M. G., Jr. Human monoclonal antibodies: concepts in development and application to colon cancer. In: M. P. Mover and G. N. Poste(eds.). Colon Cancer Cells, pp. 497-578. New York: Academic Press, 1990.
11. Haspel. M. V., McCabe, R. P., Pomato, N., Hoover, H. C. and Hanna, M.G., Jr. Coming full circle in the immunotherapy of colorectal cancer: vaccination with autologous tumor cells —¿�to human monoclonal antibodies —¿�to development and application of a generic tumor vaccine. In: R. S. Metzgerand M. S. Mitchell (eds.). Human Tumor Antigens and Specific TumorTherapy, pp. 335-344. New York: Alan R. Liss, 1989.
12. Kuroki, M., Fernstein, P. D., Wunderlich, D., Colcher, D., Simpson, J. F.,Poole, D. J., and Schlom, J. Serological mapping of the TAG-72 tumor-associated antigen using 19 distinct monoclonal antibodies. Cancer Res., 50:4872-4879, 1990.
13. Patt, Y. /... Lamki, L. M., Shanken, J., and Jessup, J. M. Imaging withindium-111-labeled anticarcinoembryonic antigen monoclonal antibodyZCE-.025 of recurrent colorectal or carcinoembryonic antigen-producingcancer in patients with rising serum carcinoembryonic antigen levels andoccult métastases.J. Clin. Oncol., «:1246-1254, 1990.
14. Slamon, D. J., Godolphin, W., Jones, L. A., Holt, J. A, Wong, S. G., Keith,D. E., Levin, W. J., Stuart, S. G., Vdove, J., Ulrich, A., and Press, M. E.Studies of the HER-2/nc« proto-oncogene in human breast and ovariancancer. Science (Washington DC), 244: 707-712. 1989.
15. Tal, M., Wetzler, M., Josefberg, Z., Deutch, A., Gulman, M., Assaf, D.,Kris, R., Shiloh, Y., Givrol, D., and Schlessinger, J. Sporadic amplificationof the HER2/nfu protooncogene in adenocarcinomas of various tissues.Cancer Res., 48: 1517-1520, 1988.
16. Ploegh, H. L., Orr, H. T., and Strominger, J. L. Major histocompatibilityantigens: the human (HLA-A, -B, -C) and murine (H-2K, H-2D) class IImolecules. Cell, 24: 287-299, 1981.
17. Giles, R. C., and Capra, D. Structure, function, and genetics of human classII molecules. Adv. Immunol., 37: 1-71, 1985.
18. Zinkernagel, R. M., and Doherty, P. C. MHC-restricted cytotoxic T cells:studies on the biological role of polymorphic major transplantation antigens
3465
on May 17, 2020. © 1992 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

HUMAN COLON TUMOR VACCINE CHARACTERIZATION
determining T-cell restriction-specificity, function, and responsiveness. Adv.Immunol.. 27:51-177, 1979.
19. Brunner, C. A., Gokel, J. M.. Riethmiller, G.. and Johnson. J. P. Expressionof HLA-D subloci DR and DQ by breast carcinomas is correlated withdistinct parameters of favorable prognosis. Eur. J. Cancer, 27: 411-416,1991.
20. Hilton. D. A., and West, K. P. An evaluation of the prognostic significanceof HLA-DR expression in gastric carcinoma. Cancer (Phila.), 66: 1154-1157, 1990.
21. Ghosh, A. K., Moore, M., Street, A. J., Howat, J. M. T., and Schofield. P.J. Expression of HLA-D sub-region products on human colorectal carcinoma.Int. J. Cancer, 38:459-464, 1986.
22. Conor O'Keane. J., Mack. C., Lynch, E.. Harrington, D., and Neiman, R. S.Prognostic correlation of HLA-DR expression in large cell lymphoma asdetermined by LN3 antibody staining. Cancer (Phila.), 66:1147-1153. 1990.
23. Rubin. J. T., Elwood, L. J., Rosenberg, S. A., and Lotze, M. T. Immunohis-tochemical correlates of interleukin-2-based response to recombinant immunotherapy in humans. Cancer Res.. 49: 7086-7092. 1989.
24. Prescott, S., James, K., Hargreve, T. B., Chisholm, G. D., and Smyth, J. F.Immunopathological effects of intravesical BCG therapy. Prog. Clin. Biol.Res., 310: 93-105. 1989.
25. Hanna. M. G.. Jr., and Peters, L. C. Immunotherapy of established micro-metastases with Bacillus Calmette-dtierin tumor cell vaccine. Cancer Res.,38: 204-211, 1978.
26. Hanna, M. G., Jr.. Brandhorst. J. S.. and Peters, L. C. Active specific
immunotherapy of residual micrometastases: an evaluation of sources, dosesand ratios of BCG with tumor cells. Cancer Immunol. Immunother., 7: 165-173, 1979.
27. Möller,P., Momburg, F.. Loretz, K., Moldenhaver, G., Herfarth, C., Otto,H. F., Hà mmerling, G. J., and Schlag, P. Influence of major histocompati-bility complex class I and II antigens on survival in colorectal carcinoma.Cancer Res., 51: 729-736, 1991.
28. Möller,P., Koretz, K., Schlag, P.. and Momburg, F. Frequency of abnormalexpression of HLA-A, B, C and HLA-DR molecules, invariant chain, andLFA-3 (CD58) in colorectal carcinoma and its impact on tumor recurrence.Int. J. Cancer Suppl.. 6: 155-162, 1991.
29. Cohen, P. J., Lotze, M. T., Roberts. J. R.. Rosenberg, S. A., and Jaffe, E. S.The immunopathology of sequential biopsies in patients treated with inter-leukin-2: correlation of response with T cell infiltration and HLA-DR expression. Am. J. Pathol., 129: 208-216, 1987.
30. Mitchell, M. S. Active specific immunotherapy with allogeneic melanomalysates and the adjuvant DETOX. In: P. Hersey (ed.), Biological Agents inthe Therapy of Melanoma and Other Cancers, pp. 121-130. Sydney, Australia: New South Wales Government Printing Service, 1990.
31. Jessup. J. M., McBride, C. M., Ames, F. C., Guarda, L., Ota, D. M.,Romsdahle. M. M.. and Martin, R. G. Active specific immunotherapy ofDuke's B2 and C colorectal carcinoma: comparison of two doses of the
vaccine. Cancer Immunol. Immunother., 21: 233-239, 1986.32. Sokal. R. R., and Kohlt. F. J. Introduction to Biostatistics, pp. 215-216. San
Francisco: W. H. Freeman and Co., 1973.
3466
on May 17, 2020. © 1992 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

1992;52:3460-3466. Cancer Res Janet H. Ransom, Barbara Pelle and Michael G. Hanna, Jr. EfficacyMolecules Correlates with Human Colon Tumor Vaccine Expression of Class II Major Histocompatibility Complex
Updated version
http://cancerres.aacrjournals.org/content/52/12/3460
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/52/12/3460To request permission to re-use all or part of this article, use this link
on May 17, 2020. © 1992 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
















![Reduced Expression of HLA Class I and II Antigens in Colon Cancer1 · [CANCER RESEARCH 50, 8023-8027, December 15, 1990] Reduced Expression of HLA Class I and II Antigens in Colon](https://img.pdfslide.us/doc/110x75/5f5945785c4df2481d781bbc/reduced-expression-of-hla-class-i-and-ii-antigens-in-colon-cancer1-cancer-research.jpg)