Embed Size (px)
Citation preview

Exploring the Relationship Between Miscarriage and Depression
.
Results DiscussionBackground: Miscarriages are a common outcome of pregnancies, with approximately 15–20% of clinically recognized pregnancies resulting in miscarriages. While the physical complaints associated with a miscarriage are routinely and easily addressed, the psychological impact of a miscarriage is often overlooked. Previous research has demonstrated poor psychological outcomes in women who have miscarried. Objective: This review aims to explore the relationship between miscarriage and depression. Methods: A structured literature review was conducted to understand the association between miscarriage and depression. Articles were retrieved by searching the databases SCOPUS and PubMed with the following key terms: depression, miscarriage, psychological consequences, and spontaneous abortion. Articles published in North America between 1990 and 2015 were included. The search was limited to articles published in the English language. Results: The literature search resulted in fifty-five articles. Eight articles of the fifty-five articles met the inclusion criteria. Of the eight articles, three were literature reviews and five were cohort studies. Conclusion: The literature suggests that depressive symptoms frequently occur in women who have miscarried. Further research is required as there is a lack of high quality study designed research on this topic.
Introduction
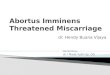
Methods
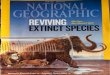
Searched PubMed and SCOPUS for: (((depression) AND miscarriage) AND psychological consequences) AND
spontaneous abortion n=55
Records after duplicates removed: n=42
Records limited to English Studies:n=41
Records limited to studies published since 1990: n=37
Records excluded based on screening abstracts for
relevance:n=17
Records limited to studies published in North America:
n=9
Records used for structured literature review: n=8
Records excluded due to unavailability of full text:
n=1
Conclusion
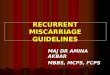
ReferencesLiterature Review:
Carter et al. (2007), Geller et al. (2010), Lok & Neugebauer (2007)
Cohort Study:Neugebauer (2003), Klier et al. (2000), Neugebauer et al. (1997), Robinson et al. (1994), Neugebauer et al. (1992)
Figure 3. Pyramid of Evidence
Findings of Structured Literature
The search yielded 5 cohort studies and 3 literature reviews. The literature confirms an association between miscarriage and depression. It suggests
that women who experience a miscarriage are likely to display higher levels of depressive symptoms compared to women who do not miscarry. 30-50% of women who miscarried were found to have developed depressive symptoms within 6 months of the loss (Carter et al., 2007). Robinson et al. (1994) used the Centre for Epidemiological Study Depression Scale (CES-D), and found women at 3 months following miscarriage had depression levels significantly higher than the population standard. Additionally, women who miscarried were found to have a 6.6% higher absolute risk of experiencing a major depressive disorder than the community women (Neugebauer et al., 1997).
Limitations
Only articles written and published in the English language were accessed, articles published prior to 1990 were not reviewed, and databases were not searched individually. One article was excluded due to unavailability of the full text.
Many studies selected for the review use convenience sampling as their method for enrolling participants, for example, support groups and hospitals. This is a type of selection bias as the sample is unlikely to be representative of the population.
The definition of miscarriage used between studies varies. Miscarriage is frequently defined in the research studies as loss prior to 28 weeks, whereas other studies in the literature review refer to miscarriage as a loss of pregnancy prior to 20 weeks. A varying definition makes it difficult to compare studies. This results in information bias, specifically, detection bias.
Implications
Most studies revealed that depression was most prevalent in the early months following miscarriage. With an understanding of the possibility for depression to result from miscarriage, health care professionals (HCPs) can employ interventions to target the prevention of depression in women who miscarry. Women who miscarry often criticize the follow-up care they received on the basis that the care did not encompass emotional well being. Intervention plans should focus on placing effective support groups that are geared towards reducing the stress and discomfort associated with experiencing a miscarriage.
Future considerations
Generate an effective standardized screening tool for detecting depression after miscarriage. This would allow for HCPs to detect women who are likely to develop depression and identify those in need of further intervention.
Few studies in the literature examine the possible psychological impact on the spouse after a miscarriage and thus, more research should be conducted in this area as well.
Figure 1. Methodology
Miscarriage, the spontaneous termination of pregnancy prior to the 28th week of gestation, is a complex biological process resulting in significant loss (Klier, Geller, and Neugebauer, 2000). For many women who experience a miscarriage, the loss of a desired child and the physical pain of miscarriage can elicit negative psychological reactions (Neugebauer, 2003). The physical complaints that are associated with miscarriage are usually resolved rapidly, however, the psychological outcomes that can result are often overlooked (Lok and Neugebauer, 2007). Previous research suggests depression as a psychological outcome of miscarriage (Lok and Neugebauer, 2007).
Research Question:Do women who experience a miscarriage display higher levels of depressive symptoms compared to women who do not miscarry?
There is evidence that suggests women who experience miscarriage are more likely to develop depressive symptoms, and most often in the first month following miscarriage. Factors of age, previous history of pregnancy loss, and having other children do not appear to be correlated with risk of depression after miscarriage. Further research utilizing high quality study designs is required on this topic.
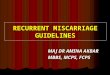
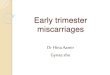
Article Research Design Population Measurements/ Statistical Analyses Findings
Lok & Neugebauer (2007)
Literature Review •Included a total of 1243 meeting the inclusion criteria, distributed across a span of 8 studies. Studies included case-control, prospective cohort, and longitudinal observational designs.
•Psychiatric interviews: Present State Examination (PSE) protocol•Diagnostic criteria: Diagnostic and Statistical Manual of Mental Disorders (DSM-IV)
•A summary of all studies revealed that 10-50% of patients were diagnosed as having major depressive disorders (MDD) following miscarriage.•Depressive symptoms persisted at an elevated state 6 months after miscarriage, and only returned to normal after 1 year.
Neugebauer et al. (1992)
Cohort Study •Case group consisting of miscarrying women (n=382), and control group consisting of pregnant women (n=283) and community women not recently pregnant (n=318).
•Fully structured interviews•Psychiatric diagnostic assessment tool: Center for Epidemiologic Studies Depression Scale (CES-D)
•Proportion of highly symptomatic women (according to CES-D) were 3.4 times higher (95% confidence interval, 2.0 – 5.0) in the miscarrying group than in the pregnant women group, and 4.3 times higher (95% confidence interval, 3.0-5.8) than in the community women group.•Women reinterviewed at 6 weeks and 6 months did not show elevated symptom levels.
Robinson et al. (1994)
Cohort Study •39 women completed the full length of the study.•Mean age was 32.9 years (SD 4.4).
•Longitudinal assessments at 3, 6 and 12 months following miscarriage•CES-D scale, Spanner Dyadic Adjustment Scale, Rosenberg Self-Esteem Scale, Impact of Pregnancy Loss Questionnaire•ANOVA analysis was used to determine relationship between time, age, and presence of children
•Findings confirm that miscarriage significantly impacts most women’s for 1 year following the loss.•At 3 months following miscarriage, depression levels were significantly higher than the population standard, dipped back to normal at 6 months, and returned to elevated levels at 1 year.•Age or having other children was not correlated with risk for depression.
Neugebauer et al. (1997)
Cohort Study •Hospital-based miscarriage cohort (n=229) and cohort of non-pregnant women drawn from the community (n=230).•50% of women were aged between 25-34.
•Structured Interview: Diagnostic Interview Schedule (DIS)
•10.9 % of miscarrying women experienced an episode of major depressive disorder (MDD), compared to 4.3% of community women.•72% of cases of MDD began in the first month following loss.•The overall relative risk for an episode of minor depression for miscarrying women was 2.5 (95% confidence interval, 1.2-23.6).•Relative risk did not vary by history of prior reproductive loss, maternal age, time of gestation or attitude towards pregnancy.
Klier et al. (2000)
Cohort Study •Hospital-based miscarriage cohort (n=229) and cohort of non-pregnant women drawn from the community (n=230).•50% of women were aged between 25-34.*analyzed same sample as above study, in the context of minor depressive disorder.
•Diagnostic criteria: DSM-IV•Structured Interview: Diagnostic Interview Schedule (DIS)•CES-D Scale•Statistical Analysis: Unadjusted relative risk (RR)
•5.4% of miscarrying women experienced an episode of minor depression, compared to 1.0% of community women.•Relative risk of minor depression for miscarrying women was 5.2 (95% confidence interval, 1.2-23.6).•Risk did not vary based on gestation length, or attitude towards pregnancy.•The majority of episodes began within one month following loss.
Geller et al. (2010)
Literature Review •Included a total of 1389 participants meeting the inclusion criteria, distributed across a span of 17 quantitative and qualitative studies, with cross-sectional, longitudinal, retrospective, and interview based research designs.
•Likert Scale questionnaires•Semi-structured/structured interviews•Impact of Events Scale•Profile of Mood States•General Health Questionnaire
•No correlation found between satisfaction with miscarriage aftercare and development of depression.
Carter et al. (2007)
Literature Review •Reviewed a total of 11 articles pertaining to depression and/or depressive symptomatology.
•Diagnostic criteria: DSM-IV •30-50% of women who miscarry experience some degree of depressive symptoms within 6 months of lost; majority within the first month.•One analyzed study found an significantly increased suicide rate amongst miscarrying women 1 year post-loss.•Another study found that 54% of women who have had previous history of depression relapse after miscarriage.
Neugebauer (2003)
Cohort Study •Miscarrying women cohort (n=114) and community women cohort (n=318)
•CES-D Scale •Substantial elevation of depressive symptoms in the miscarriage cohort compared to community cohort with an adjusted difference in means between cohorts of 4.9 (95% confidence interval, 2.3 -7.4).•20.2% of miscarrying women were highly symptomatic (CES-D score = 30+), compared to 10.1% in community women (adjusted odds ratio 2.8, 95% confidence interval, 1.4 - 5.6).•Impact on depressive symptoms significantly greater at 6-8 weeks following miscarriage, than at 2 weeks following miscarriage.•No correlation between depressive symptoms and number of living children, marital status, ethnicity or educational level.
Figure 2. Summary of Literature Review
1. Neugebauer, R. (2003). Depressive symptoms at two months after miscarriage: interpreting study findings from an epidemiological versus clinical perspective.Depression and anxiety, 17(3), 152-161.
2. Neugebauer, R., Kline, J., O’Connor, P., Shrout, P., Johnson, J., Skodol, A., ... & Susser, M. (1992). Depressive symptoms in women in the six months after miscarriage. American journal of obstetrics and gynecology, 166(1), 104-109.
3. Neugebauer, R., Kline, J., Shrout, P., Skodol, A., O'Connor, P., Geller, P. A., ... & Susser, M. (1997). Major depressive disorder in the 6 months after miscarriage. JAMA, 277(5), 383-388.
4. Klier, C. M., Geller, P. A., & Neugebauer, R. (2000). Minor depressive disorder in the context of miscarriage. Journal of affective disorders, 59(1), 13-21.
5. Carter, D., Misri, S., & Tomfohr, L. (2007). Psychologic aspects of early pregnancy loss. Clinical obstetrics and gynecology, 50(1), 154-165.
6. Lok, I. H., & Neugebauer, R. (2007). Psychological morbidity following miscarriage. Best Practice & Research Clinical Obstetrics & Gynaecology,21(2), 229-247.
7. Robinson, G. E., Stirtzinger, R., Stewart, D. E., & Ralevski, E. (1994). Psychological reactions in women followed for 1 year after miscarriage. Journal of Reproductive and Infant Psychology, 12(1), 31-36.
8. Geller, P. A., Psaros, C., & Kornfield, S. L. (2010). Satisfaction with pregnancy loss aftercare: are women getting what they want?. Archives of women's mental health, 13(2), 111-124.
Interdisciplinary School of Health Sciences, University of Ottawa
Faraz Ahmad Abdul Hadi Djokhdem Laura Danielle Pozzobon Sadad Rahman `
Abstract