Embed Size (px)
Citation preview

Psycho-OncologyPsycho-Oncology 19: 150–159 (2010)Published online 2 March 2009 in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/pon.1517
Exploring the association between functional strain andemotional well-being among a population-based sampleof breast cancer survivors
Kimlin T. Ashing-Giwa1,2* and Jung-Won Lim1
1Center of Community Alliance for Research and Education (CCARE), Division of Population Sciences, City of Hope National Medical Center,
Duarte, CA, USA2UCLA School of Medicine, Los Angeles, CA, USA
Abstract
Objective: Breast cancer survival and survivorship outcomes have improved dramatically; yet,
there are still considerable morbidities associated with this illness. Functional strain is
conceptualized as the unfavorable outcome of the functional well-being domain of health-
related quality of life. This study intends to (1) examine the adequacy of the functional strain
concept; (2) describe the level of functional strain and emotional well-being by ethnicity and job
types; and (3) investigate the salient functional strain components influencing emotional well-
being for breast cancer survivors (BCS) after controlling for ethnicity and job types.
Methods: A cross-sectional design with mixed sampling methods was used. BCS were
recruited from the California Cancer Surveillance Program, hospital registries and community
agencies in Southern California. Functional strain was measured by assessing family and work
burdens.
Results: Confirmatory factor analysis established the adequacy of the two factors (family
and work burdens) defining the functional strain. Findings demonstrated significant differences
in functional strain by ethnicity and job types. Latina-Americans and homemakers/housewives
showed the worst scores in functional strain variables. The final model examining the impact of
functional strain components on emotional well-being explained 34% of the variance of
emotional well-being.
Conclusion: Findings suggest the impact of cancer on family and work life varies by ethnic
and demographic characteristics, such that Latino ethnicity and homemaker/housewife status
may be risk factors for functional strain. Our findings imply that functional strain provides a
reasonable concept that can be used to deepen our understanding and examination of the
impact of functional status on emotional well-being.
Copyright r 2009 John Wiley & Sons, Ltd.
Keywords: breast cancer; functional strain; cancer and work; emotional well-being; health-related
quality of life; survivorship; ethnic minority survivorship
Introduction
Owing to earlier detection and more effectivetreatment regimens, the survival rate for breastcancer has increased significantly [1]. Accordingly,overall health-related outcomes among breastcancer survivors (BCS) have been improved [2,3].However, breast cancer is still accompanied byconsiderable challenging late effects that becomeapparent after treatment has ended such aslymphedema, fatigue, memory problem, and de-pression [4]. One common area of concern amongBCS is the functional domain such as familyobligations and work ability and/or performance.The functional well-being domain of health-relatedquality of life (HRQOL) refers to one’s ability to
perform the activities related to one’s societal/familial role including household and employmenttasks [5]. The functional domain, although im-portant to survivorship outcomes and overallHRQOL is understudied. Our qualitative researchsuggests that functional domain is related toemotional well-being specifically [4,6–8]. Therefore,this study will investigate the association betweenfunctional and emotional well-being among apopulation-based multiethnic sample of BCS.
Definition of functional strain
BCS endure physical, psychological, and socialsequelae, as well as greater functional concernsincluding work capacity, lack of job security,
* Correspondence to: Centerof Community Alliance forResearch and Education, Cityof Hope, 1500 East DuarteRoad, Duarte, CA 91010-3000, USA. E-mail:[email protected]
Received: 27 August 2008
Revised: 6 November 2008
Accepted: 12 November 2008
Copyright r 2009 John Wiley & Sons, Ltd.

restricted career advancements, and lack of supportat the workplace [4,9–12]. Particularly, ethnicminority BCS reported that they earned lessincome, had fewer weeks off from work thanrequested, and were not paid time off during theirbreast cancer treatments [9]. This situation wasworse for survivors who were in labor or domestictype jobs. Additionally, about 20% of BCSindicated that they experienced some job discrimi-nation and 15% stated that they were laid off, andethnic minority BCS were more likely to reportthese negative employment experiences [13].Such employment and financial problems are
related to family burden among BCS [8]. Anotherstudy found that ethnic minority BCS reported agreater number of familial challenges or daily livingconcerns compared with European-Americans [14].For example, Asian women were particularlytroubled about the financial burden placed on thefamily due to the cancer and its treatments [4].African-American women reported low energy anddifficulties focusing on family obligations, as well asconcerns about their job stability [15]. Latinas wereespecially worried about being unable to financiallysupport their families, and felt that cancer had asignificant effect on their employability [8].In an effort to better understand the impact of
functional well-being on emotional well-being, thecurrent study conceptualizes ‘functional strain’ asthe poor or unfavorable outcome of the functionalwell-being domain of HRQOL. In general, thedictionary explains ‘functional’ as ‘capable ofperforming’; and ‘strain’ as ‘a great or excessivepressure, demand, or stress on one’s body, mind, orresources’ [16]. The word strain has also beenfrequently used for the internal force in a body orstress. Functional strain, therefore, measures thesummative demands of daily living, and familialand work burdens (Figure 1). Functional strainmay provide a more proximal and survivor
sensitive assessment of a survivor’s familial andwork burdens.
Functional strain and emotional well-being
Emotional well-being is described as the mostimportant contributor to overall HRQOL forBCS [17–20]. Both Quigley [21] and Pedro [22]in their studies of the emotional well-being of BCS,found uncertainty, psychological distress, de-creased self-esteem, and body image to be keyconcerns. Other emotional effects include fearof recurrence and distress related to physicalcompromise [23]. Naturally, the literature onemotional well-being focuses on its psychologicalcomponents.The preliminary findings drawn from evaluating
the Contextual Model of HRQOL [24], aswell as the results from qualitative investigations[8,25] suggest that familial- and work-relatedburdens may negatively influence emotional well-being [26,27]. A study reported that job strain(high demands and stress, low self-control) wasassociated with poorer mental health and emo-tional well-being, and lower health status [28].These findings may be exacerbated for BCS.Indeed, BCS perceived greater strains due torole demands related to family and workafter their illness [29–32]. Therefore, functionalstrain may be important to emotional well-being,particularly because many families, especiallyethnic minority families, are highly dependent onsurvivors’ care-giving, job productivity and in-come; these obligations can emotionally taxing forBCS. However, research examining family or workburden after cancer, as well as its impact onemotional well-being is lacking among cancersurvivors, in general, and among BCS specifically.Therefore, further investigation of the associationbetween functional strain and emotional well-beingis necessary.
Functional Strain
Emotional
Well-being
Family burden
1. Family stress 2. Living situation 3. Change in martial status 4. Financial responsibilities
Work burden
1. Functional role limitation due to physical problem 2. Functional stress 3. The impact of cancer on work life 4. Work capabilities
Neighborhood stress
Ethnicity
Medical Information
Job Types
Figure 1. The conceptual model: the impact of functional strain on emotional well-being
Copyright r 2009 John Wiley & Sons, Ltd. Psycho-Oncology 19: 150–159 (2010)
DOI: 10.1002/pon
Functional strain and emotional well-being 151

The purpose of study
This study aims (1) to examine the adequacy of thefunctional strain concept that links family burdenplus work burden; (2) to describe the level of thefunctional strain and emotional well-being byethnicity and job types; and (3) to investigate thesalient functional strain components influencingemotional well-being for a multiethnic sample ofBCS after controlling for ethnicity and job types.The following hypotheses were formulated:
1. The functional strain concept will be com-prising family and work burdens.
2.1. Latina Americans will report greater functionalstrain and lower emotional well-being com-pared with other ethnic groups.
2.2. Homemakers/housewife will report greaterfunctional strain and lower emotional well-being compared with BCS employed in otherjobs.
3. Functional strain including family and workburdens will negatively influence emotionalwell-being after controlling for ethnicity andjob types.
Methods
Details regarding sampling, recruitment proce-dures, instrument development, and reliabilityand validity employed for the study have beenreported elsewhere [9]. A brief overview of themethodologies used follows.
Study design and participants
Secondary data derived from 626 multiethnic(European-, African-, Latina-, and Asian-Amer-ican) BCS, who had participated in a projectexamining HRQOL [9], were used for this study.BCS in this study were included if they werebetween 18- and 69-years old and were disease freefrom 1 to 5 years post diagnosis. Specifically, thecurrent study considered BCS of working age, onlyto examine family- and work-related obligationsthat may vary according to age.This study used a cross-sectional, mixed sam-
pling design with a population-based ethnicallyand socio-economically diverse sample drawn fromthe California Cancer Surveillance Program, areahospital registries, and community agencies. Basedon the culturally responsive model [33], ethnicallyand linguistically diverse staffs were included toenhance cultural sensitivity with the targetedpopulations. All potential participants were as-signed alternately to receive either a telephonesurvey or a mailed survey. After mailing arecruitment packet, initial telephone contact witha potential participant was conducted for eligibilityscreening. Eligible survivors then participated in
the interview or survey questionnaire in theirpreferred language. Signed informed consents wereobtained from all participants. The study protocolwas approved by the UCLA Institutional ReviewBoard.
Measures
A culturally informed survey instrument consistingof standard measures and new scales based onprevious studies [6,15], qualitative data [9], and theresearch literature was developed and validatedthrough a sequence of measurement development.Reliability and validity tests indicate that thestandard and new measures used are appropriatefor a diverse BCS sample (Cronbach’s coefficienta5 0.65–0.92) [9]. The assessment included onestandardized instrument measuring emotional well-being. The functional strain measure comprises twocomponents such as family burden (family stress,living situation, change in marital status, andfinancial responsibilities) and work burden (func-tional role limitation due to physical problem,functional stress, the impact of cancer on work life,and work capabilities). Additionally, neighbor-hood stress (e.g. availability and quality of publicresources), which may provide additional strain forBCS, is included in our study as a control variable(Figure 1).The emotional well-being sub-domain (six item;
a5 0.75) was adapted from the Functional Assess-ment of Cancer Therapy-Breast (FACT-B), whichis a standardized QOL instrument [34]. Items arerated from 0 to 4, with higher scores indicatingbetter QOL. A total emotional well-being score wasobtained in accordance with the instructions in themanual for the FACT measurement system [35].Family, functional, and neighborhood stress
were adapted from the 14 items of Life StressScale developed to examine the level of burdenassociated with various aspects of life [9]. Ourpreliminary factor analysis demonstrated that thisscale comprises three components. Items are ratedfrom 1 to 5, a higher score indicates higher stress.For assessing family stress, four items (death andinjury/illness of family members, raising children,marriage/romantic relationships) were adaptedfrom this scale, and two items (family careresponsibilities and burden) were developed fromthe principal investigator’s preliminary studies. Allsix items were averaged to obtain a total score(a5 0.65). For functional stress, four relevantitems (money/finances, housing, job situation,education) was averaged to obtain a total scoreof functional stress (a5 0.71). Neighborhood stressincludes six items: neighborhood environment,public services, transportation, crime/violence,relations with police, and relations with ethnic/racial groups. A total score was obtained byaveraging the items (a5 0.66).
152 K. T. Ashing-Giwa and J.-W. Lim
Copyright r 2009 John Wiley & Sons, Ltd. Psycho-Oncology 19: 150–159 (2010)
DOI: 10.1002/pon

Functional role limitations due to physicalproblems (four item; a5 0.90), one of work burdenvariables, were adapted from the Short-Form-36Health Survey (SF–36) [37]. Items are ratedusing Likert-type scales: subscale scores range from0 to 100, with higher scores indicating betterfunctioning.Other family burden variables are as follows:
living situation, change in marital status, andfinancial responsibilities before and after cancer(‘Did/do you have any family members who was/were dependent on your income?’). In terms ofwork burden, this study evaluated the impact ofcancer on work life from the following question:‘Overall, what impact has your experience withbreast cancer had on your career/job?’ Items arerated from 1 (negative impact) to 3 (positiveimpact). Additionally, another item about workcapability was included ‘In the past 12 months,how much has breast cancer affected your ability towork outside the home?’ Items are rated from 1 to4, with higher scores indicating better workcapability.
Data analyses
Descriptive and correlation analyses were con-ducted to examine the characteristics and relation-ships of the variables. First, confirmatory factoranalysis (CFA), using AMOS 7.0, was conductedto determine the validity of the functional strainconcept consisting of family and work burdens(hypothesis 1). Specifically, one-factor and two-factor models were tested to examine the variablesshared by the functional strain components. Forthe two-factor model, ‘family burden’ and ‘workburden’ factors were created. Family burden ismeasured by family stress, change in marital status,financial responsibilities before and after cancer,and living situation. Work burden is measured byfunctional limitations due to physical problems,functional stress, work capability, and the impactof cancer on work life.Second, for hypotheses 2.1 and 2.2, analyses of
covariance and logistic regression were used toassess differences in functional strain and emo-tional well-being by ethnicity and job types aftercontrolling for covariates.Finally, a hierarchical regression analysis was
performed to determine the influence of functionalstrain components on emotional well-being aftercontrolling for covariates (hypothesis 3). Thus,demographic and medical information was enteredinto Step 1, neighborhood stress in Step 2, familyburden in Step 3, and work burden in Step 4,respectively. For these statistical techniques, thedata were analyzed using the SPSS 15.0 computerprogram. All hypotheses were tested with a po0.05criterion of significance for a two-sided test.
Results
Of the 1219 accessible BCS, 134 were ineligible, 382refused (including 139 non-completers), and 703(58%) BCS completed the survey. Of the 703 BCSparticipants, 77 survivors (X70 years) were ex-cluded from this study due to the age criteria. Thefinal sample of BCS included 154 European-, 121African-, 166 Latina-, and 185 Asian-American.The mean age of the sample was 52 years, rangingfrom 29- to 69-years old. The majority ofparticipants (85.5%) had been diagnosed withcancer in stages 1 or 2. The mean time since cancerdiagnosis was about 2.9 years. Details regardingsubjects’ demographic and medical characteristicsare described elsewhere [9,38].
Descriptive analyses for functional strain
In terms of general findings regarding familyburden, 11% of the respondents reported thattheir breast cancer caused a change in their maritalstatus/relationship status. Approximately a third ofthe participants reported having familial financialobligations before and after their breast cancerdiagnosis; specifically, 40% reported having familymembers who were dependent on their income atthe time of their breast cancer diagnosis. Addi-tionally, about 37% reported that they currentlyhad family members who are dependent on theirincome. Of the three types of stress, survivorsreported greater family stress (Mean5 1.42;SD5 0.75) compared with functional (Mean5
0.91; SD5 0.81) and neighborhood stress (Mean5
0.37; SD5 0.46).Regarding work burden, overall, BCS expressed
less functional limitations due to physical problems(Mean5 68.12; SD5 40.54) compared with thenormative score (Mean5 50; SD5 10), indicatingthat their work problems, for the most part, werenot primarily due to physical problems. Of the 416survivors employed in the past or currently, 117(28%) survivors indicated that their boss did notgive them adequate support during their breastcancer treatment, and 22 (5%) did not even informtheir boss about their breast cancer. About 10% ofemployed participants reported that they hadexperienced some form of employment/job discri-mination due to their breast cancer, and 19%indicated that the breast cancer had an overallnegative impact on their career/job. On the otherhand, 23% endorsed that the breast cancerexperience had a positive impact on their career/job, and 58% did not suggest any impactsregarding cancer experiences.
H1: which components explain functional strain?
Two competing models (one factor and two factor)were tested to investigate the structure of the
Functional strain and emotional well-being 153
Copyright r 2009 John Wiley & Sons, Ltd. Psycho-Oncology 19: 150–159 (2010)
DOI: 10.1002/pon
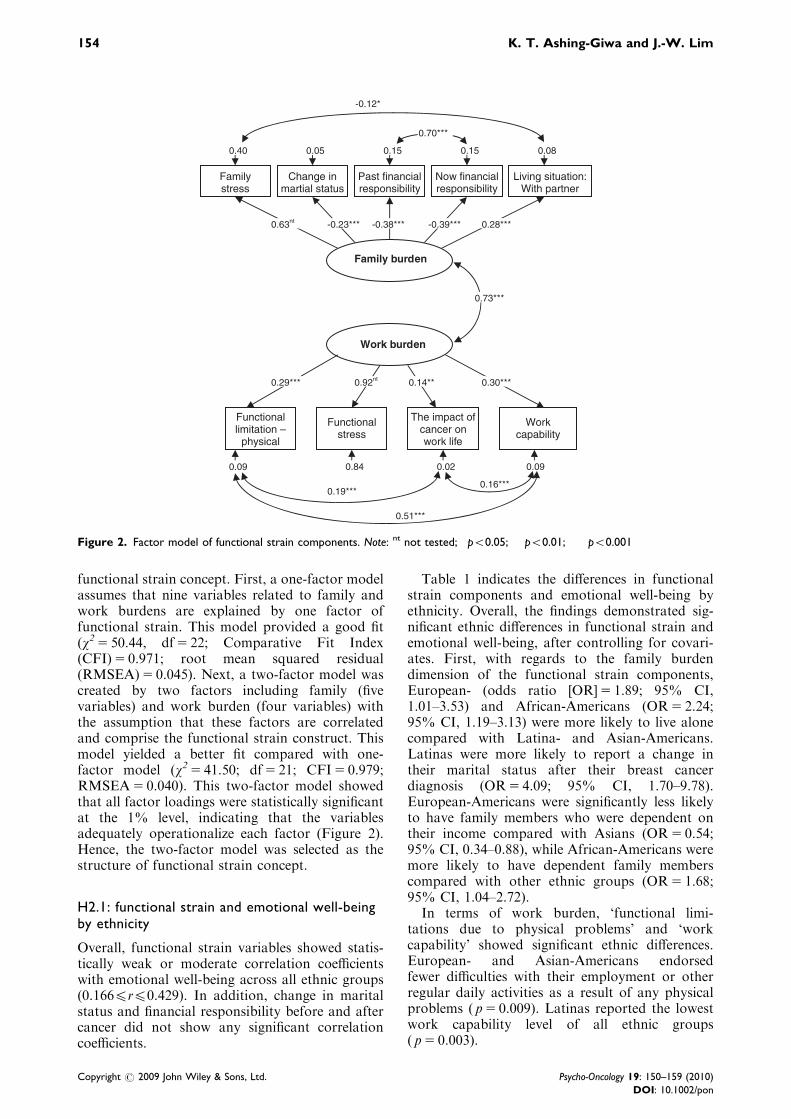
functional strain concept. First, a one-factor modelassumes that nine variables related to family andwork burdens are explained by one factor offunctional strain. This model provided a good fit(w2 5 50.44, df5 22; Comparative Fit Index(CFI)5 0.971; root mean squared residual(RMSEA)5 0.045). Next, a two-factor model wascreated by two factors including family (fivevariables) and work burden (four variables) withthe assumption that these factors are correlatedand comprise the functional strain construct. Thismodel yielded a better fit compared with one-factor model (w2 5 41.50; df5 21; CFI5 0.979;RMSEA5 0.040). This two-factor model showedthat all factor loadings were statistically significantat the 1% level, indicating that the variablesadequately operationalize each factor (Figure 2).Hence, the two-factor model was selected as thestructure of functional strain concept.
H2.1: functional strain and emotional well-beingby ethnicity
Overall, functional strain variables showed statis-tically weak or moderate correlation coefficientswith emotional well-being across all ethnic groups(0.166prp0.429). In addition, change in maritalstatus and financial responsibility before and aftercancer did not show any significant correlationcoefficients.
Table 1 indicates the differences in functionalstrain components and emotional well-being byethnicity. Overall, the findings demonstrated sig-nificant ethnic differences in functional strain andemotional well-being, after controlling for covari-ates. First, with regards to the family burdendimension of the functional strain components,European- (odds ratio [OR]5 1.89; 95% CI,1.01–3.53) and African-Americans (OR5 2.24;95% CI, 1.19–3.13) were more likely to live alonecompared with Latina- and Asian-Americans.Latinas were more likely to report a change intheir marital status after their breast cancerdiagnosis (OR5 4.09; 95% CI, 1.70–9.78).European-Americans were significantly less likelyto have family members who were dependent ontheir income compared with Asians (OR5 0.54;95% CI, 0.34–0.88), while African-Americans weremore likely to have dependent family memberscompared with other ethnic groups (OR5 1.68;95% CI, 1.04–2.72).In terms of work burden, ‘functional limi-
tations due to physical problems’ and ‘workcapability’ showed significant ethnic differences.European- and Asian-Americans endorsedfewer difficulties with their employment or otherregular daily activities as a result of any physicalproblems ( p5 0.009). Latinas reported the lowestwork capability level of all ethnic groups( p5 0.003).
0.19*** 0.16***
Family burden
Work burden
Family stress
Living situation: With partner
Now financial responsibility
Past financial responsibility
Change in martial status
Work capability
The impact of cancer on work life
Functional stress
Functional limitation –
physical
0.63nt -0.23*** -0.38*** -0.39*** 0.28***
0.29*** 0.92nt 0.14** 0.30***
0.40 0.05 0.15 0.15 0.08
0.73***
0.09 0.84 0.02 0.09
0.70***
-0.12*
0.51***
Figure 2. Factor model of functional strain components. Note: nt not tested; �po0.05; ��po0.01; ���po0.001
154 K. T. Ashing-Giwa and J.-W. Lim
Copyright r 2009 John Wiley & Sons, Ltd. Psycho-Oncology 19: 150–159 (2010)
DOI: 10.1002/pon

H2.2: functional strain and emotional well-beingby job types
After controlling for medical information, weexamined the relationships between functionalstrain and emotional well-being by job types(Table 2). Overall, survivors employed in a profes-sional job were more likely to live alone comparedwith homemakers (OR5 3.16; 95% CI, 1.52–6.49).Additionally, survivors employed in a professionaljob were more likely to endorse a greater financialresponsibility before (OR5 2.23; 95% CI,1.39–3.53) and after cancer (OR5 3.56; 95% CI,2.14–5.93) compared with homemakers. In terms ofwork-related burden, homemakers showed thehighest functional strain scores compared withother working survivors ( p5 0.016). For example,homemakers reported greater functional limitationswith maintaining employment or other regular dailyactivities due to physical problems ( p5 0.002).They also exhibited the lowest score in workcapability ( p5 0.026). In addition, BCS employedin service jobs endorsed the highest functional stresslevel of all job types. Meanwhile, survivors who are/were in the professional/technical job type showedbetter scores in emotional well-being; while home-makers expressed the lowest score ( p5 0.015).Additionally, among all the ethnic groupsAfrican-Americans showed the best emotionalwell-being score of all ethnic groups; while,Latina-Americans exhibited the lowest score.
H3: the impact of functional strain on emotionalwell-being
In accordance with our conceptual framework andresults from CFA, a hierarchical multiple regres-sion analysis identified predictors influencing emo-tional well-being among multiethnic BCS. Model 1,including demographic (ethnicity and job typesspecifically) and medical characteristics, explained13% of the variance of emotional well-being.Neighborhood stress when added to the Model 2,explained 4% of the variance in emotional well-being. Next, family-burden-related factors signifi-cantly improved Model 3, explaining an additional7% of the variance in emotional well-being. Lastly,adding work-burden-related factors significantlyimproved the model, accounting for 10% of thevariance in the emotional well-being final model.Thus, the final model accounted for 34% of thevariance in emotional well-being (Table 3).In the final model, family stress, functional
limitations due to physical problems, functionalstress, the impact of cancer on work life, and workcapability are significant predictors. Specifically, allfunctional strain-related factors significantly influ-enced emotional well-being among multiethnicBCS, after controlling for covariates. Overall,survivors who reported less familial and workstress and experienced less functional limitationsdue to physical problems, and endorsed a positiveimpact of breast cancer on job/career and work
Table 1. Emotional well-being and functional strain by ethnicity
Mean (SD)
European (N 5 154) African (N 5 121) Latina (N 5 166) Asian (N 5 185) F
Emotional well-beinga,b,c,d 19.36 (3.6) 20.17 (3.7) 17.79 (4.5) 19.36 (4.4) 8.25���
Family stress 1.35 (0.7) 1.44 (0.7) 1.44 (0.8) 1.45 (0.7) 0.99
Functional limitation—physicalb,e 73.53 (37.3) 66.60 (39.0) 59.82 (45.5) 72.94 (38.0) 3.86��
Functional stress 0.95 (0.7) 1.03 (0.9) 0.92 (0.9) 0.79 (0.7) 1.29
The impact of cancer on work life 2.05 (0.7) 2.08 (0.6) 2.04 (0.6) 2.04 (0.7) 0.32
Work capabilityb,c,e 3.54 (1.0) 3.36 (1.0) 3.18 (1.1) 3.55 (0.7) 4.66��
OR(95% CI)f Wald v2
Living situation (0 5 no/1 5 yes)
Alonea,g 1.89 (1.01–3.53) 2.24 (1.19–3.13) 0.84 (0.42–1.70) 1.0 15.25��
Partner 1.51 (0.94–2.41) 0.57 (0.32–1.01) 0.65 (0.39–1.08) 1.0 15.79��
Partner and childrena,g 0.45 (0.28–0.72) 0.59 (0.36–0.97) 1.28 (0.83–1.97) 1.0 25.99���
Othersc,g 1.14 (0.56–2.29) 2.54 (1.31–4.95) 1.97 (1.04–3.74) 1.0 10.89�
Change in martial status
(0 5 no/1 5 yes)a,c,g 2.53 (1.01–6.36) 3.10 (1.20–8.00) 4.09 (1.70–9.78) 1.0 17.52��
Financial responsibility before
(0 5 no/1 5 yes)a,g 0.54 (0.34–0.88) 1.68 (1.04–2.72) 0.97 (0.63–1.51) 1.0 18.48���
Financial responsibility after
(0 5 no/1 5 yes)d 0.77 (0.48–1.23) 0.61 (1.13–3.00) 0.93 (0.59–1.48) 1.0 10.59�
aSignificant differences between African- and Latina-Americans.bSignificant differences between European- and Latina-Americans.cSignificant differences between Latina- and Asian-Americans.dSignificant differences between African- and Asian-Americans.eSignificant differences between European- and African-Americans.fAsian-American is a reference group.gSignificant differences between European- and Asian-Americans.
Covariates: years since diagnosis, cancer stage, comorbidities. �po0.05, ��po0.01, ���po0.001.
Functional strain and emotional well-being 155
Copyright r 2009 John Wiley & Sons, Ltd. Psycho-Oncology 19: 150–159 (2010)
DOI: 10.1002/pon

capability were likely to report better emotionalwell-being regardless of ethnicity and job types.
Discussion
This study focused on the preliminary evaluationof the functional strain concept and investigatingthe impact of functional strain on emotional well-being among a multiethnic BCS sample. Findingssuggest that the (i) functional strain was character-ized by family and work burden; (ii) relationshipsbetween the functional strain and emotional well-being varied by ethnicity and job types, such thatLatinas and homemakers showed the worst scores;and (iii) functional strain components significantlyand negatively influenced emotional well-being.Thus, our hypotheses were confirmed in the currentstudy.Functional well-being although important to
overall HRQOL outcomes is largely understudied.This study is the first investigation, to our knowl-edge, to try to measure the human side offunctional strain and to describe the differences infunctional strain among a population-based multi-ethnic sample of BCS. The current study concep-tualizes ‘functional strain’ as the poor orunfavorable outcome of the functional well-beingdomain of HRQOL that is assessed by thesummative demands of daily living, and familialand work burdens. Thus, the current study
attempts to characterize the social and ecologicaldimensions of ‘functional strain’. Given our con-ceptualization and measurement ‘functional strain’may provide a comprehensive concept that caninform our appreciation, examination, and inter-vention toward improving functional well-beingspecifically and HRQOL, in general.If gaps between the empirical and analytic parts
of a concept may be in confusion, then a moretheoretical use of factor analysis, which incorpo-rates analytic possibilities as a theory and empiricaltechniques, may be necessary. Based on such rolesof factor analysis, our findings seem to support thereasoning of functional strain including family andwork burden. Specifically, we chose the two-factormodel of the functional strain because it yielded abetter fit compared with one-factor model. Eventhough family burden is highly correlated withwork burden in the two-factor model, it is under-standable in that financial and employment pro-blems are interconnected with family burdenamong BCS [8]. However, it may be relevant todisentangle the links among employment andfinancial problems and family burden. As a result,this model may allow for the gathering of newknowledge regarding the definition and compo-nents of functional strain in the broader socio-ecologic context. In addition, the methodologicaljustification for expanding theoretical concepts canbe an indication for a direction toward deepeningour exploration of the role of functional strain, and
Table 2. Emotional well-being and functional strain by job types
Job types (Mean; SD)
Professional (N 5 232) Tech/sales (N 5 150) Service (N 5 103) Homemaker (N 5 139) F
Emotional well-beinga,b,c 19.38 (3.9) 19.79 (3.8) 18.64 (4.8) 18.15 (4.4) 3.54�
Family stress 1.43 (0.7) 1.51 (0.7) 1.37 (0.8) 1.35 (0.9) 1.44
Functional limitation—physicala,b,c,d 75.11 (36.7) 71.64 (38.5) 60.05 (41.5) 59.89 (45.2) 5.13��
Functional stressb,e 0.88 (0.7) 0.99 (0.9) 1.05 (0.8) 0.77 (0.8) 3.46�
The impact of cancer on work life 2.05 (0.7) 2.09 (0.7) 2.11 (0.6) 1.95 (0.4) 1.21
Work capabilitya,b 3.51 (0.8) 3.47 (0.9) 3.38 (0.9) 3.18 (1.0) 3.11�
OR(95% CI)f Wald v2
Living situation (0 5 no/1 5 yes)
Alonea,b,e 3.16 (1.52–6.49) 2.25 (1.02–4.95) 2.83 (1.25–6.42) 1.0 22.63��
Partner 1.31 (0.80–2.14) 1.11 (0.64–1.90) 1.13 (0.63–2.03) 1.0 3.28
Partner and childrena,b,e 0.38 (0.25–0.60) 0.44 (0.27–0.71) 0.38 (0.22–0.64) 1.0 31.77���
Others 1.21 (0.64–2.29) 1.39 (0.71–2.75) 1.43 (0.69–2.97) 1.0 5.87
Change in martial status
(0 5 no/1 5 yes)e 1.04 (0.50–2.16) 1.55 (0.73–3.32) 1.25 (0.53–2.92) 1.0 25.38���
Financial responsibility before
(0 5 no/1 5 yes)a,b,e 2.23 (1.39–3.53) 1.97 (1.19–3.25) 1.90 (1.09–3.32) 1.0 19.27��
Financial responsibility after
(0 5 no/1 5 yes)a,b,e 3.56 (2.14–5.93) 2.86 (1.65–4.76) 2.72 (1.49–4.95) 1.0 38.57���
aSignificant differences between specific job types: professional and homemaker.bSignificant differences between specific job types: tech/sales and homemaker.cSignificant differences between specific job types: tech/sales and service.dSignificant differences between specific job types: professional and service.eSignificant differences between specific job types: service and homemaker.fHomemaker is a reference group.
Covariates: years since diagnosis, cancer stage, comorbidities. �po0.05, ��po0.01, ���po0.001.
156 K. T. Ashing-Giwa and J.-W. Lim
Copyright r 2009 John Wiley & Sons, Ltd. Psycho-Oncology 19: 150–159 (2010)
DOI: 10.1002/pon

investigating its impact on emotional well-being aswell as other HRQOL domains.In the current study, work burdens including the
impact of cancer on work life, functional limita-tions due to physical problems, and work cap-ability were important factors influencingemotional well-being among multiethnic BCS.However, living situation, change in marital status,and financial responsibilities did not significantlyimpact emotional well-being. This finding suggeststhat the manner in which BCS perceive and dealwith their stress and adjust within the family maybe more important to emotional well-being thantheir family living situation or even changes in thefamily members after the cancer.Additionally, perceptions about the positive
impact of the breast cancer experience on theircareer or job were expressed across all ethnicgroups. However, 116 survivors or 19% reportednegative job outcomes including lack of support,job discrimination, and loss of their job as a resultof missing work or change in job performance dueto the cancer treatment. Consequently, these BCSmay experience distress and worry about beingunable to financially support their family. Thus,there is an urgent need to investigate the changing
patterns in the employment/career status duringand after cancer treatment to further understandemployment issues and functional strain amongBCS.There are several limitations. Our instrument
was based on self-reporting, thus findings may beinfluenced by participant recall biases. The cross-sectional study design does not adequately assessthe dynamic relationships of variables, thus alongitudinal, prospective study will be necessaryto fully understand their nature. Additionally,findings from this sample may not be generalizableto all populations, even though the sampleprimarily is population-based. Howevers, thisstudy provides meaningful new knowledge aboutfunctional strain and emotional well-being forBCS. Several clinical and research implicationsexist.Our data reveal unique ethnic patterns relevant
to family situation and obligations that influencefunctional strain among each ethnic group. Ourfindings suggest that survivors’ living situation andtheir familial obligation may be framed by acultural context including gender roles.In summary, differences in functional strain
suggest the impact of cancer on family and work
Table 3. Effects of independent variables on emotional well-being
Variables Unstandardized b coefficients
Model 1 Model 2 Model 3 Model 4
R2 5 0.13
F 5 6.98���R2 5 0.17
F 5 8.92���R2 5 0.24
F 5 8.21���R2 5 0.34
F 5 10.84���
Demographic and medical information
Age 0.07�� 0.06�� 0.05� 0.04
Job types(ref: homemaker)
Managerial/professional 0.40 0.02 0.26 �0.13
Technical/sales 1.23� 0.94 1.17� 0.87
Service/operator 0.29 0.08 0.05 �0.09
Ethnicity(ref: European-Americans)
African-Americans 0.48 0.64 0.62 0.75
Latina-Americans �1.30� �1.14� �0.88 �0.61
Asian-Americans �0.50 �0.37 �0.19 �0.15
Years since diagnosis 0.32�� 0.28� 0.30�� 0.12
Cancer Stage �0.17 �0.16 �0.18 �0.05
Number of Comorbidities �0.67��� �0.57��� �0.46��� �0.21
Neighborhood stressa �2.08��� �1.13�� �0.53
Family burden
Family stressa �1.48��� �1.27���
Living situation(ref: living alone)
Partner �0.22 �0.77
Partner and children 0.10 �0.46
Others 0.24 �0.01
Change in martial status �0.12 0.05
Financial responsibilities before �0.35 �0.06
Financial responsibilities after 0.36 0.33
Work burden
Functional limitation–physicala 0.02���
Functional stressa �0.63��
The impact of cancer on work lifea 0.70��
Work capabilitya 0.48�
aHigher score refers to better well-being/function and less stress level.�po0.05, ��po0.01, ���po0.001.
Functional strain and emotional well-being 157
Copyright r 2009 John Wiley & Sons, Ltd. Psycho-Oncology 19: 150–159 (2010)
DOI: 10.1002/pon

life vary by ethnic and demographic characteristics.Such that a Latino ethnicity and homemaker/housewife status may be risk factors for functionalstrain. Specifically, the lowest scores in the emo-tional well-being, as well as the functional strainamong homemakers and Latinas, may reflect theirdifficulties and burdens in addressing all thedemands and obligations related to family andhousehold care following breast cancer and itstreatments. In addition, homemakers may havelower social network and social support availabi-lity. Further, our findings suggest that functionalstrain provides a reasonable concept that can beused to deepen our understanding and examinationof the impact of functional status on emotionalwell-being. Thus, intervention strategies designedto improve emotional well-being may have greatersustainable benefits if socio-ecological contexts,including familial and functional parameters, arealso considered.Finally, there is a tremendous need for popula-
tion-based research to assess the impact of thephysical, functional, emotional, socio-ecologicaldimensions on survivorship outcomes. Clinically,this study highlights the need for greater attention tothe functional strain among BCS that considerscultural and familial characteristics. Further, culturaland familial contexts should inform interventions toaddress employment issues for BCS to moreadequately reduce functional strain and ultimatelyimprove their HRQOL. On the research side, thefindings support a broader, more contextuallyinclusive conceptualization of functional and emo-tional well-being. Therefore, investigational andclinical strategies should include cultural and socio-cultural contexts as well as consider the specificcontributions and the interrelationship among theHRQOL dimensions. This contextual approach mayenhance the salience and utility of our interventionto reduce the burden of cancer particularly amongour most underserved populations.
Acknowledgements
A grant from the CDBMRP-DOD (17-99-1-9106).
References
1. American Cancer Society. Cancer Facts and Figures2008. American Cancer Society: Atlanta, GA, 2007.
2. Ganz PA, Desmond KA, Leedham B, Rowland JH,Meyerowitz BE, Belin TR. Quality of life in long-term,disease-free survivors of breast cancer: a follow-upstudy. J Natl Cancer Inst 2002;94:39–49.
3. Institute of Medicine. Cancer Care for the WholePatient: Meeting Psychosocial Health Needs. NationalAcademy Press: Washington, DC, 2007.
4. Ashing-Giwa KT, Padilla G, Tejero J, Kagawa-Singer M.Understanding the breast cancer experience of AsianAmerican women. Psycho-Oncology 2003;12:38–58.
5. Cella DF. Quality of life and decision making. The SixthBiennial Symposium on Minorities and the MedicallyUnderserved and Cancer, Washington, DC, 1997.
6. Ashing-Giwa K. Quality of life and psychologicaloutcomes in long-term breast cancer survivors: a studyof African American women. Psychosoc Oncol2000;17:47–62.
7. Ashing-Giwa K, Padilla G, Bohorquez D, Tejero J,Garcia M. Understanding the breast cancer experienceof Latinas. J Psychosoc Oncol 2006;24:19–52.
8. Ashing-Giwa K, Padilla G, Tejero J et al. Under-standing the breast cancer experience of women: aqualitative study of African American, Asian American,Latina and European American cancer survivors.Psycho-Oncology 2004;13:408–428.
9. Ashing-Giwa K, Padilla G, Tejero J, Kim J. Breast cancersurvivorship in a multiethnic sample: challenges inrecruitment and measurement. Cancer 2004;101:450–465.
10. Abrahamsen AF, Loge JH, Hannisdal E, Holte H,Kvaloy S. Socio-medical situation for long-term survi-vors of Hodgkin’s disease: a survey of 459 patientstreated at one institution. Eur J Cancer 1998;34:1865–1870.
11. Bradley CH, Bednarek HL, Neumark D. Breast cancersurvival, work, and earnings. J Health Econ 2002;21:757–779.
12. Langeveld NE, Ubbink MC, Last BF, Grootenhuis MA,Voute RJ, De Haan RJ. Educational achievement,empoyment, and living situation in long-term youngadult survivors of childhood cancer in the Netherlands.Psycho-Oncology 2003;12:213–225.
13. Eversley R, Estrin D, Dibble S, Wardlaw L, Pedrosa M,Favila-Penney W. Post-treatment symptoms amongethnic minority breast cancer survivors. Oncol NursForum 2005;32:250–256.
14. Kim K, Stein K, Baker F, DeFrank J. The effects ofproblems in daily living and ethnicity on quality of lifeof cancer survivors. Psycho-Oncology 2004;13:S1–S75.
15. Ashing-Giwa K, Ganz PA, Petersen L. Quality of life ofAfrican-American and White long-term breast cancersurvivors. Cancer 1999;85:418–426.
16. Farlex. The Free Dictionary. Farlex Inc., 2008.17. Ersek M, Ferrell BR, Dow KH, Melancon CH. Quality
of life in women with ovarian cancer. West J Nurs Res1997;19:334–350.
18. Ferrell BR, Hassey DK, Grant M. Measurement of thequality of life in cancer survivors. Qual Life Res 1995;4:523–531.
19. Ferrell B, Smith SL, Cullinane CA, Melancon C.Psychological well being and quality of life in ovariancancer survivors. Cancer 2003;98:1061–1071.
20. Dow KH, Ferrell BR, Haberman MR, Eaton L. Themeaning of quality of life in cancer survivorship. OncolNurs Forum 1999;26:519–528.
21. Quigley KH. The adult cancer survivor: psychosocialconsequences of cure. Semin Oncol Nurs 1989;5:63–69.
22. Pedro LW. Quality of life for long-term survivors ofcancer: influencing variables. Cancer Nurs 2001;24:1–11.
23. Corney RH, Everett H, Howells A, Crowther ME.Psychosocial adjustment following major gynaecologi-cal surgery for carcinoma of the cervix and vulva.J Psychosom Res 1992;36:561–568.
24. Ashing-Giwa K. The Contextual Model of HRQOL: aparadigm for expanding the HRQOL framework. QualLife Res 2005;14:297–307.
25. Ashing-Giwa K, Kagawa-Singer M, Padilla GV et al.The impact of cervical cancer and dysplasia: aqualitative, multiethnic study. Psycho-Oncology 2004;13:675–753.
26. Michael YL, Kawachi I, Berkman LF, Holmes MD,Colditz GA. The persistent impact of breast carcinoma
158 K. T. Ashing-Giwa and J.-W. Lim
Copyright r 2009 John Wiley & Sons, Ltd. Psycho-Oncology 19: 150–159 (2010)
DOI: 10.1002/pon

on functional health status: prospective evidence fromthe Nurses’ Health Study. Cancer 2000;89:2176–2186.
27. Vinokur AD, Threatt BA, Caplan RD, Zimmerman BL.Physical and psychosocial functioning and adjustmentto breast cancer: long-term follow-up of a screeningpopulation. Cancer 1989;63:394–405.
28. Amick BCr, Kawachi I, Coakley EH, Lerner D, Levine S,Colditz GA. Relationship of job strain and iso-strain tohealth status in a cohort of women in the United States.Scand J Work Environ Health 1998;24:54–61.
29. Inoue S, Saeki T, Mantani T, Okamura H, Yamawaki S.Factors related to patient’s mental adjustment to breastcancer: patient characteristics and family functioning.Support Care Cancer 2003;11:178–184.
30. Northouse LL. Breast cancer in younger women: effectson interpersonal and family relations. J Natl Cancer InstMonogr 1994;16:183–190.
31. Northouse L. The impact of cancer in women on thefamily. Cancer Pract 1995;3:134–142.
32. Woods NF, Lewis FM. Women with chronic illness:their views of their families’ adaptation. Health CareWomen Int 1995;16:135–148.
33. Ashing-Giwa K. Can a culturally responsive model forresearch design bring us closer to addressing participa-tion disparities? Lessons learnt from Cancer Survivor-ship Studies. Ethn Dis 2005;15:130–137.
34. Cella D, Tulsky D, Gray G et al. The FunctionalAssessment of Cancer Therapy Scale: development andvalidation of the general measure. J Clin Oncol1993;11:570–579.
35. Cella D. FACIT Manual: Manual of the FunctionalAssessment of Chronic Illness Therapy (FACIT) Mea-surement System Version 4. Evanston NorthwesternHealthcare and Northwest University, Evanston, IL,1997.
36. Ware JE, Snow KK, Kosinski M, Gandek B.SF-36 Health Survey: Manual and Interpretation Guide.Health Institute, New England Medical Center: Boston,1993.
37. Ashing-Giwa KT, Tejero JS, Kim J, Padilla GV,Hellemann G. Examining predictive models ofHRQOL in a population-based, multiethnic sample ofwomen with breast carcinoma. Qual Life Res2007;16:413–428.
Functional strain and emotional well-being 159
Copyright r 2009 John Wiley & Sons, Ltd. Psycho-Oncology 19: 150–159 (2010)
DOI: 10.1002/pon