Embed Size (px)
Citation preview
RESEARCH Open Access
Exploring health workforce regulationpractices and gaps in Ethiopia: a nationalcross-sectional studyDaniel Dejene1*, Tegbar Yigzaw1, Samuel Mengistu2, Firew Ayalew1, Manuel Kahsaye1 and Damtew Woldemariam1
Abstract
Background: Health workforce regulation plays key roles in ensuring the availability of competent health workersand improving performance of the health system. In 2010, Ethiopia established a national authority aiming toensure competence and ethics of health professionals. Subsequently, subnational regulators were established andregulatory frameworks were developed. Although there were anecdotal reports of implementation gaps, there waslack of empirical evidence to corroborate the reports. We conducted a national study to explore health professionalregulation practices and gaps focusing on registration, licensing, ethics, scope of practice, and continuingprofessional development.
Methods: We conducted a mixed methods cross-sectional survey using structured interview with a nationalrepresentative sample of health professionals and key informant interviews with health regulators and managers.We used two stage stratified cluster sampling to select health professionals. The quantitative data were subjectedto descriptive and multivariable logistic regression analysis. We conducted thematic analysis of the qualitative data.
Results: We interviewed 554 health professionals in the quantitative survey. And 31 key informants participated inthe qualitative part. Nearly one third of the respondents (32.5%) were not registered. Many of them (72.8%) did notrenew their licenses. About one fifth of them (19.7%) did nothing against ethical breaches encountered during theirclinical practices. Significant of them ever practiced beyond their scope limits (22.0%); and didn’t engage in CPD inthe past 1 year (40.8%). Majority of them (97.8%) never identified their own CPD needs. Health regulators andmanagers stressed that regulatory bodies had shortage of skilled staff, budget and infrastructure to enforceregulation. Regulatory frameworks were not fully implemented.
Conclusions: Health professionals were not regulated well due to limited capacity of regulators. This might haveaffected quality of patient care. To ensure effective implementation of health professional regulation, legislations shouldbe translated into actions. Draft guidelines, directives and tools should be finalized and endorsed. Capacity of theregulators and health facilities needs to be built. Reinstituting health professionals’ council and regulation enforcementstrategies require attention. Future studies are recommended for assessing effects and costs of weak regulation.
Keywords: Health professional regulation, Registration, Licensing, Ethics, CPD, SOP, Ethiopia
© The Author(s). 2019 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, andreproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link tothe Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver(http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
* Correspondence: [email protected], Kirkos Subcity, PO Box 2881, Code 1250 Addis Ababa, EthiopiaFull list of author information is available at the end of the article
Global HealthResearch and Policy
Dejene et al. Global Health Research and Policy (2019) 4:36 https://doi.org/10.1186/s41256-019-0127-x

BackgroundCapacity to advance health services and meet people’shealthcare needs in a country is determined by theavailability of a highly performing health workforce.That is why the health workforce is considered asone of the six essential building blocks of a healthsystem, and; a competent and motivated workforce iscrucial to achieve national and global health develop-ment goals [1–3].Health workforce regulation plays key roles in en-
suring the availability of competent, responsive andproductive human resources for health and improvingperformance of the health system. Through effectiveregulation, arrangements are put in place to protectthe public and ensure that high standards of health-care are maintained [4]. Regulation prevents andmanages harm on patients that might happen becauseof incompetence and malpractice [5, 6]. It builds mu-tual trust in quality of care among health profes-sionals, patients and stakeholders [7]. Market failure,misuse of resources and economic inefficiency arelikely to happen in a healthcare industry where thereis no effective regulation [8].Ethiopia has made impressive progress in improving
health access and outcomes [9]. The recent increment inhealth workforce density and distribution has contrib-uted for these successes [10]. However, unsatisfactoryperformance of health professionals has remained amajor gap [11], partly due to lack of robust healthcareregulation [9]. As the result of this and other factors, as-suring quality of healthcare has remained elusive for thecountry.In 2010, the Government of Ethiopia established the
Food, Medicine, and Healthcare Administration andControl Authority (FMHACA) with the mandate toprotect population health by ensuring the competenceand ethics of health professionals, the standards ofhealth institutions, the safety and quality of food, thesafety, efficacy, quality and proper use of medicines,and hygiene and environmental health protection. TheFMHACA incorporated globally recommended regula-tory frameworks for optimizing performance of thehealth workforce in its policy statements [10, 12, 13].The FMHACA established 11 subnational branch of-fices, and delegated some regulatory duties and pow-ers to the branch offices where it found it necessary.The FMHACA and its branches have been managinghealth professional registration and licensing, scope ofpractice (SOP), ethics and continuing professionaldevelopment (CPD). Health facilities have alsosupported the health professional regulation practicesthrough creating CPD opportunities, supportinghealthcare ethics review system; and applying enforce-ment measures to strengthen regulation. Accreditation
and certification examination are managed by otheragencies.Although Ethiopia adopted various health professional
regulatory frameworks, their implementation has fallenbehind [10, 14]. Ratified proclamations on regulationand the health professional council have not been fullyenacted. Directives and guidelines on registration andlicensing, CPD, SOP and ethics have not been finalized,officially endorsed or implemented. Despite issuing aCPD directive, health professionals are not asked toshow evidence that they meet the requirements whenthey renew their licenses. There are anecdotal reports ofunregistered and unlicensed practitioners, out of scopepractice and ethical breaches. The health professionalregulators in Ethiopia like those in other developingcountries lack the necessary capacity, resources andautonomy to respond to the increasing public pressurefor patient safety and redrawing professional boundaries[15–17].However, there is a dearth of empirical evidence on
gaps of the health professional regulation practices andcapacity of the regulators in Ethiopia which is necessaryto inform the health systems strengthening interven-tions. Such evidence will also expand the global know-ledge base on regulation and inform regulatory practicesin other low and middle income countries having similarchallenges. Hence, we conducted a national study to ex-plore health professional regulation practices and gapsfocusing on registration, licensing, ethics, SOP, andCPD.
MethodsStudy design and sampleWe conducted a mixed methods cross-sectional studyin March 2015. The quantitative survey was donewith a nationally representative sample of health pro-fessionals working in government health facilities. Thestudy targeted seven major clinical cadres; namely,medical doctors (including specialist doctors), healthofficers, nurses, midwives, anesthetists, medical la-boratory professionals, and pharmacy professionals. InEthiopia, health officers are health cadres trained for4 years to provide clinical and public health servicesin rural hospitals and health centers where medicaldoctors are in short supply. Anesthetists are non-physician anesthesia providers with diploma or bache-lor’s degree level training. According to a 2014unpublished report from the Federal Ministry ofHealth (FMOH), there were 73,514 health profes-sionals working in 2782 government health facilities(122 hospitals and 2660 health centers) in Ethiopia.We calculated a sample size of 508 health profes-sionals using a single population proportion formulawith assumptions of 95% level of confidence,
Dejene et al. Global Health Research and Policy (2019) 4:36 Page 2 of 12

proportion of 50% (since there was no prior study toestimate the proportion), design effect of 1.2 (sincethere was no prior study to estimate the design ef-fect), relative error of 10%, and anticipated non-response rate of 10%. According to health facilitystaffing standards, the seven target health professionalcategories were expected to serve in hospitals but fiveof them (health officers, midwives, nurses, pharmacyprofessionals and medical laboratory professionals)were also assigned in health centers. Hence, 102health facilities were required to fulfill the sample sizetaking the minimum five professional categories serv-ing at each facility (508/5 = ~ 102). We used a powerallocation technique to break down the 102 samplefacilities into 22 hospitals and 80 health centers. Wethen proportionally allocated health facilities to theregional states.We used a two stage stratified cluster sampling pro-
cedure to select health facilities and the target healthprofessionals. Lists of the government health facilitiesin each regional state were used as sampling frames.Data collectors applied a lottery method to randomlyselect hospitals and health centers from the lists.Study participants were selected from lists of healthprofessionals at each facility using the lottery methodmaking sure that all the targeted professional categor-ies were represented. Thus, the five professional typesfrom each health center and the seven professionaltypes from each hospital were included.In situations where the selected facility was not func-
tional or did not have the targeted professionals, it wasreplaced by a nearby facility. Health professionals whowere full time employees and had a minimum of 6month work experience were invited for participation.The rationale was that health professionals with fewerthan 6months at the job could not have adequate op-portunity to experience regulation schemes and providevalid judgment about the health professional regulationpractices and gaps.For the qualitative part, the target populations were
health regulators at FMHACA and its regional branches,and health managers at FMOH, regional health bureaus(RHBs), and selected public hospitals. We believed thatthe regulators and managers in these organizations pos-sessed adequate knowledge of the implementation statusand gaps of regulation. Using purposeful samplingmethod, we selected 24 managers and regulators for keyinformant interviews (KII): one from each of the 11RHBs, 11 regional regulatory branches, the FMOH, andthe FMHACA. In addition, we selected directors from11 hospitals, one hospital from each region. The hospi-tals in the regions were selected based on convenience.The inclusion criteria for regulators and managers werebeing full time employees and having a minimum of 6
month work experience. Similarly, we thought that man-agers with less work experience could not give valid as-sessment about the health professional regulatorypractices and gaps.
Data collectionWe developed two data collection tools using relevantnational directives, guidelines and health workforcesurvey instruments [18]. The first tool was a struc-tured questionnaire for the quantitative survey. It had72 variables which were devoted to explore experi-ences and perceptions of health professionals on:registration (a process whereby a health professionaldata are recorded and assigned to a profession withits appropriate nomenclature), licensing (a processwhereby a health professional data are recorded andassigned to a profession to its appropriate nomencla-ture, and a license to practice were provided to healthprofessionals in his/her domain for 5 years), CPD (anyeducational activity to enhance knowledge and skillsof health professionals), SOP (a list of procedures, ac-tions and processes an individual is permitted to per-form based on specific education, experiences anddemonstrated competences), and ethics review system(system to protect the safety, rights, and well-being ofpatients and to promote ethical health care). The sec-ond tool was a key informant interview guideintended to understand process, performance andcapability of the regulatory system. Four regulationexperts from the FMHACA validated the tools. Wepilot tested and improved the tools. Data collectionwas carried out by a research consultancy firm. Thefirm deployed 12 data collectors, each with a master’sdegree and relevant work experiences. Prior to de-ployment, we trained the data collectors on the datacollection procedures, tools and ethics. The data col-lectors conducted interviews with study participantsin a private room. Aiming to ensure confidentiality,data on study participants’ names and their facilitieswere not collected. The key informant interviews wereaudio-recorded after getting consent from each inter-viewee. The data collectors were closely supported by12 supervisors. Errors and omissions found during thedata collection were corrected timely.
Data management and analysisFor the quantitative data, questionnaires were checkedfor completeness and consistency of responses. The datawere entered into Epi Info version 3.5.1 and exported toSTATA Version 13 [19, 20]. Data cleaning was per-formed using both the Epi Info and STATA. Weconducted data analysis using descriptive statistics andlogistic regression. The logistic regression analysis wasperformed to look into the association between socio-
Dejene et al. Global Health Research and Policy (2019) 4:36 Page 3 of 12
demographic variables (sex, age, facility type, type ofprofession, level of education and work experience) andthe two main outcome variables (practice beyond scopelimits and participation in CPD). Multivariable logisticregression analysis was done only for variables with p-value less than or equal to 0.25 during binary logisticregression. We calculated 95% confidence intervals andused a p-value of less than 0.05 to determine statisticalsignificance. Regarding qualitative data analysis, inter-views were transcribed verbatim into local language(Amharic) and translated into English. The field noteswere included in the transcripts. Transcription andtranslation of the interviews were conducted on thesame day to avoid the loss of details. All transcripts werecross-checked with the audio files and the translationsfor consistency, correctness and completeness. Errors inthe translation were corrected by referring to the Am-haric versions and the audio files. We then conductedthematic analysis for the purpose of classification,summarization, and tabulation. Open Code 3.6 softwarewas used to analyze qualitative data [21].
Ethical ConsiderationWe obtained ethical clearance from the InstitutionalReview Board of Johns Hopkins University (JHU)Bloomberg School of Public Health. Since this re-search was supported by Jhpiego; an affiliate of JHU,it was a requirement for Jhpiego to obtain IRB clear-ance from the University. The Federal Ministry ofHealth and regional health bureaus also approved thestudy protocol and provided support letters to con-duct the study. The study team members met withmanagers of target institutions to explain the purposeof the study and processes of data collection. Datacollectors obtained informed oral consent from eachstudy participant before data collection.
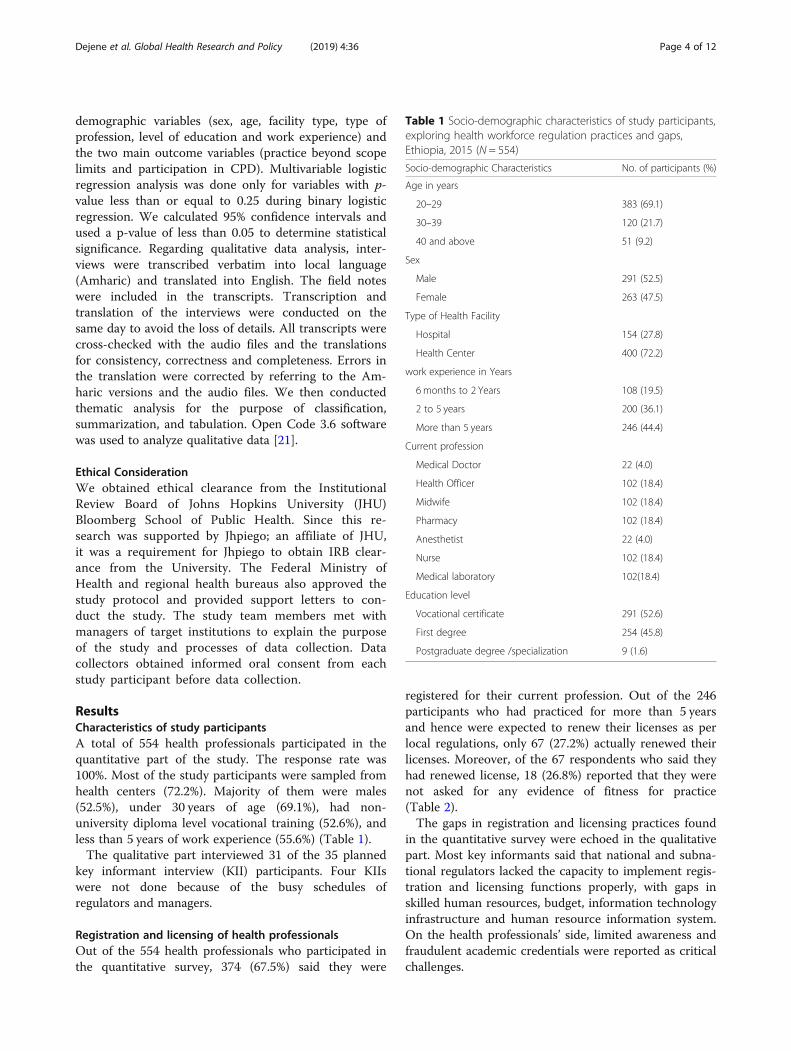
ResultsCharacteristics of study participantsA total of 554 health professionals participated in thequantitative part of the study. The response rate was100%. Most of the study participants were sampled fromhealth centers (72.2%). Majority of them were males(52.5%), under 30 years of age (69.1%), had non-university diploma level vocational training (52.6%), andless than 5 years of work experience (55.6%) (Table 1).The qualitative part interviewed 31 of the 35 planned
key informant interview (KII) participants. Four KIIswere not done because of the busy schedules ofregulators and managers.
Registration and licensing of health professionalsOut of the 554 health professionals who participated inthe quantitative survey, 374 (67.5%) said they were
registered for their current profession. Out of the 246participants who had practiced for more than 5 yearsand hence were expected to renew their licenses as perlocal regulations, only 67 (27.2%) actually renewed theirlicenses. Moreover, of the 67 respondents who said theyhad renewed license, 18 (26.8%) reported that they werenot asked for any evidence of fitness for practice(Table 2).The gaps in registration and licensing practices found
in the quantitative survey were echoed in the qualitativepart. Most key informants said that national and subna-tional regulators lacked the capacity to implement regis-tration and licensing functions properly, with gaps inskilled human resources, budget, information technologyinfrastructure and human resource information system.On the health professionals’ side, limited awareness andfraudulent academic credentials were reported as criticalchallenges.
Table 1 Socio-demographic characteristics of study participants,exploring health workforce regulation practices and gaps,Ethiopia, 2015 (N = 554)
Socio-demographic Characteristics No. of participants (%)
Age in years
20–29 383 (69.1)
30–39 120 (21.7)
40 and above 51 (9.2)
Sex
Male 291 (52.5)
Female 263 (47.5)
Type of Health Facility
Hospital 154 (27.8)
Health Center 400 (72.2)
work experience in Years
6 months to 2 Years 108 (19.5)
2 to 5 years 200 (36.1)
More than 5 years 246 (44.4)
Current profession
Medical Doctor 22 (4.0)
Health Officer 102 (18.4)
Midwife 102 (18.4)
Pharmacy 102 (18.4)
Anesthetist 22 (4.0)
Nurse 102 (18.4)
Medical laboratory 102(18.4)
Education level
Vocational certificate 291 (52.6)
First degree 254 (45.8)
Postgraduate degree /specialization 9 (1.6)
Dejene et al. Global Health Research and Policy (2019) 4:36 Page 4 of 12
A manager in a regional health bureau said, “Trainingof regulators and facility managers, and strengtheningregulatory functions is needed. It is necessary to createawareness among health professionals on theimportance, processes and expectations of registration,licensing and other regulations.” (HM2)
A respondent at a subnational regulatory body said,“The health workforce data are not completely enteredinto a database yet. [The] networking process [betweennational and subnational regulatory bodies] is notcompleted yet.” (HR4)
A respondent from another subnational regulatorybody stated, “On average, we find seven cases offalse certificate of competency examination duringregistration per month. It is very shocking.” (HR9)
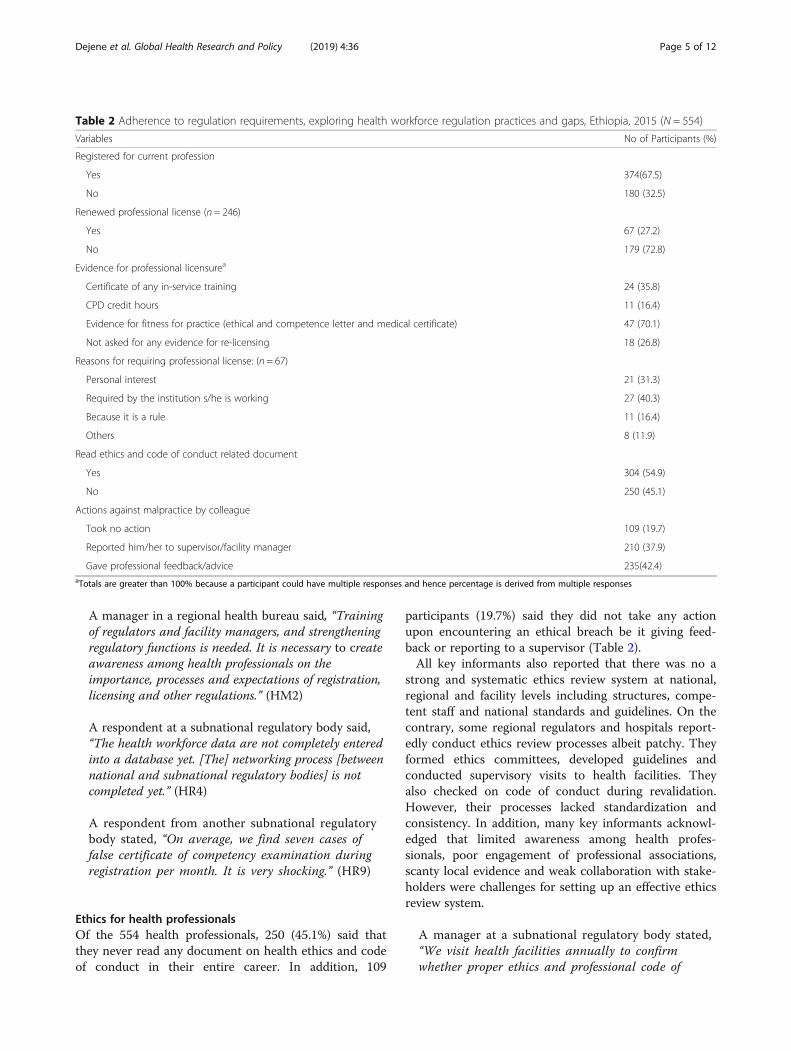
Ethics for health professionalsOf the 554 health professionals, 250 (45.1%) said thatthey never read any document on health ethics and codeof conduct in their entire career. In addition, 109
participants (19.7%) said they did not take any actionupon encountering an ethical breach be it giving feed-back or reporting to a supervisor (Table 2).All key informants also reported that there was no a
strong and systematic ethics review system at national,regional and facility levels including structures, compe-tent staff and national standards and guidelines. On thecontrary, some regional regulators and hospitals report-edly conduct ethics review processes albeit patchy. Theyformed ethics committees, developed guidelines andconducted supervisory visits to health facilities. Theyalso checked on code of conduct during revalidation.However, their processes lacked standardization andconsistency. In addition, many key informants acknowl-edged that limited awareness among health profes-sionals, poor engagement of professional associations,scanty local evidence and weak collaboration with stake-holders were challenges for setting up an effective ethicsreview system.
A manager at a subnational regulatory body stated,“We visit health facilities annually to confirmwhether proper ethics and professional code of
Table 2 Adherence to regulation requirements, exploring health workforce regulation practices and gaps, Ethiopia, 2015 (N = 554)
Variables No of Participants (%)
Registered for current profession
Yes 374(67.5)
No 180 (32.5)
Renewed professional license (n = 246)
Yes 67 (27.2)
No 179 (72.8)
Evidence for professional licensurea
Certificate of any in-service training 24 (35.8)
CPD credit hours 11 (16.4)
Evidence for fitness for practice (ethical and competence letter and medical certificate) 47 (70.1)
Not asked for any evidence for re-licensing 18 (26.8)
Reasons for requiring professional license: (n = 67)
Personal interest 21 (31.3)
Required by the institution s/he is working 27 (40.3)
Because it is a rule 11 (16.4)
Others 8 (11.9)
Read ethics and code of conduct related document
Yes 304 (54.9)
No 250 (45.1)
Actions against malpractice by colleague
Took no action 109 (19.7)
Reported him/her to supervisor/facility manager 210 (37.9)
Gave professional feedback/advice 235(42.4)aTotals are greater than 100% because a participant could have multiple responses and hence percentage is derived from multiple responses
Dejene et al. Global Health Research and Policy (2019) 4:36 Page 5 of 12

conduct are applied by health professionals.During renewing license, our body [the subnationalregulator] ensures that professionals are fitfor practice through requesting support lettersstating ethical behaviors from their work place.”(HR10)
A key informant in another subnational regulatorybody said, “We monitor whether professionals areworking up to the level of their scope. We have ourown ethics guideline at regional level but there is noendorsed national document to ensure uniformityacross regions.” (HR2)
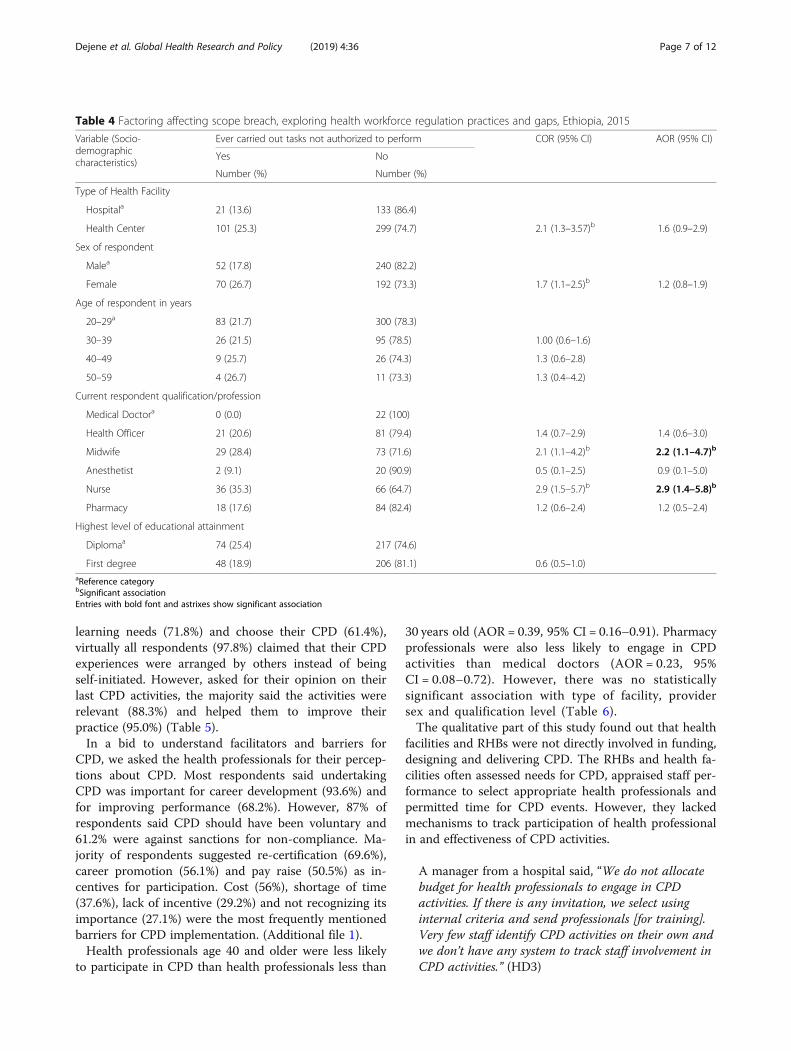
Scope of Practice (SOP)Out of the surveyed health professionals, about one-fifth of them (22%) did not have adequate knowledgeabout their own job descriptions. More than half ofthem (57.9%) were not aware of their SOPs asdirected by the regulatory body. Moreover, 122respondents (22%) admitted that they conductedunauthorized tasks (tasks beyond their scope) as somepoint in their career while nearly twice that number(43.3%) reported knowledge of scope breach by theircolleagues. The frequently mentioned reasons forpracticing beyond one’s scope were shortage of quali-fied staff and the need to respond to life-threateninghealth emergencies (Table 3).Nurses and midwives, respectively, were thrice and
twice more likely than medical doctors to perform tasksbeyond their scope (AOR = 2.9; 95% CI = 1.4–5.8); and(AOR = 2.2; 95% CI = 1.1–4.7). However, scope breachwas not significantly associated with type of facility, andprovider age, sex, and qualification level (Table 4).The qualitative part also showed that practicing be-
yond the limits of one’s scope was more common amongnon-physician health professionals like nurses, midwivesand health officers. According to the key informants, theroot cause of non-adherence to scope was scarcity ofphysicians. Sometimes, the health professionals areinstructed by managers to complete tasks outside oftheir scope.
One facility manager said, “Some professionals areassigned to work beyond their scope of practice. Thishappens because of lack of qualified staff and toprovide care to patients with emergency.” (HD10)
Most key informants from regional regulator bodies saidthat they did not have any mechanism to ensure thathealth professionals complied with their scope-of-practice,as the national directive and policy have not yet been en-dorsed. Many of them also said they often encountered
conflicts between different professional groups because oflack of a scope-of-practice directive to govern professions.
A manager from a regional health bureau said, “Thereis a conflict between nurses and doctors on scope ofpractice. Druggists have had conflicts withpharmacists. We usually face conflict betweenemergency surgical officers and surgeons. This happensbecause of lack of legally endorsed scope of practicedirective.” (HM8)
Continuing professional development (CPD)Nearly six out of ten health professionals (59.2%) whoparticipated in this study reported that they were en-gaged in CPD activities in the last 12 months. Non-governmental organizations (NGOs) were the main CPDproviders and financiers, mentioned by 71.3 and 63.7%of respondents, respectively. Although most respondentssaid health professionals themselves should define their
Table 3 Experiences regarding Scope of Practice, exploringhealth workforce regulation practices and gaps, Ethiopia, 2015
Variables No of Participants (%)
Adequate Knowledge on JD
Yes 434 (78%)
No 120 (22%)
Adequate knowledge on legal SOP (n = 554)
Yes 233 (42.1)
No 321 (57.9)
Ever seen a colleague practice beyond his/her scope(n = 554)
Yes 240 (43.3)
No 314 (56.7)
Measures taken against practice beyond scope (n = 240)
Congratulated him/her 50 (20.8)
Told him/her not to do it again 89 (37.1)
Reported to supervisor 15 (6.2)
Reported to regulatory body 4 (1.7)
Kept quite 79 (32.9)
Others 3 (1.3)
Ever carried tasks one is not authorized to do (n = 554)
Yes 122 (22.0)
No 432 (78.0)
Reasons for carrying out tasks beyond scope (122)a
Absence of qualified staff 80 (72.1)
Included in the job description 2 (1.7)
Official delegation 4 (3.3)
In case of life threating emergencies 66 (54.1)apercentage is larger than 100% since one participant could havemultiple responses
Dejene et al. Global Health Research and Policy (2019) 4:36 Page 6 of 12
learning needs (71.8%) and choose their CPD (61.4%),virtually all respondents (97.8%) claimed that their CPDexperiences were arranged by others instead of beingself-initiated. However, asked for their opinion on theirlast CPD activities, the majority said the activities wererelevant (88.3%) and helped them to improve theirpractice (95.0%) (Table 5).In a bid to understand facilitators and barriers for
CPD, we asked the health professionals for their percep-tions about CPD. Most respondents said undertakingCPD was important for career development (93.6%) andfor improving performance (68.2%). However, 87% ofrespondents said CPD should have been voluntary and61.2% were against sanctions for non-compliance. Ma-jority of respondents suggested re-certification (69.6%),career promotion (56.1%) and pay raise (50.5%) as in-centives for participation. Cost (56%), shortage of time(37.6%), lack of incentive (29.2%) and not recognizing itsimportance (27.1%) were the most frequently mentionedbarriers for CPD implementation. (Additional file 1).Health professionals age 40 and older were less likely
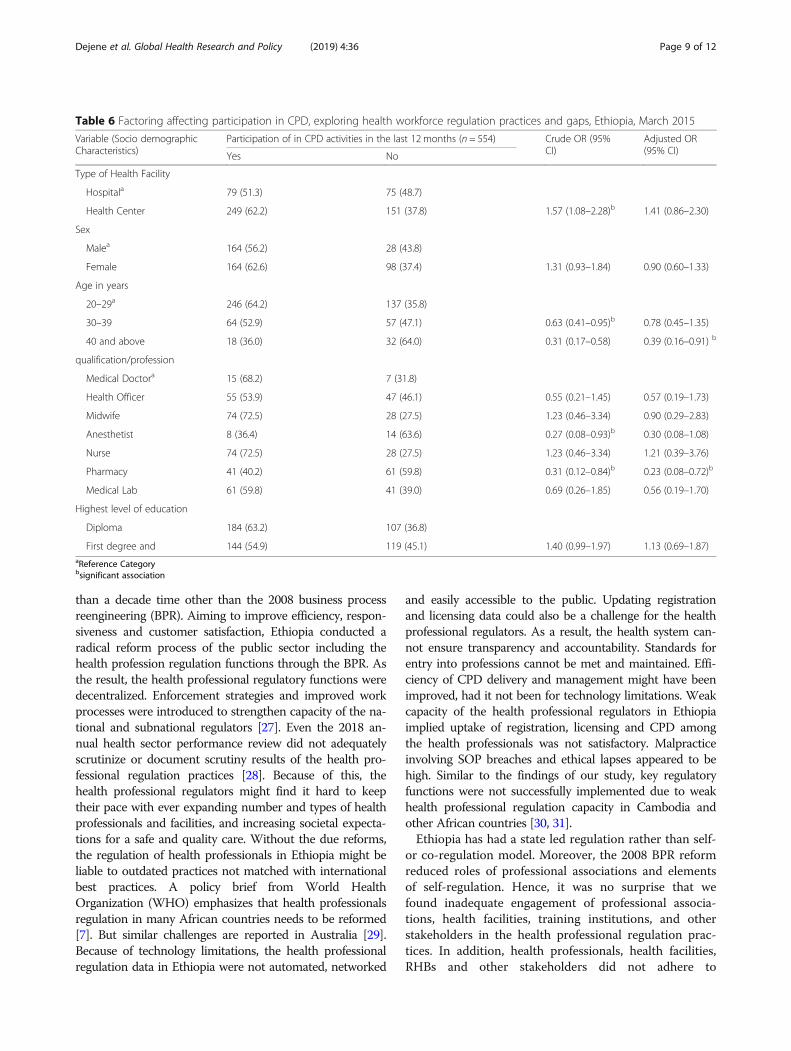
to participate in CPD than health professionals less than
30 years old (AOR = 0.39, 95% CI = 0.16–0.91). Pharmacyprofessionals were also less likely to engage in CPDactivities than medical doctors (AOR = 0.23, 95%CI = 0.08–0.72). However, there was no statisticallysignificant association with type of facility, providersex and qualification level (Table 6).The qualitative part of this study found out that health
facilities and RHBs were not directly involved in funding,designing and delivering CPD. The RHBs and health fa-cilities often assessed needs for CPD, appraised staff per-formance to select appropriate health professionals andpermitted time for CPD events. However, they lackedmechanisms to track participation of health professionalin and effectiveness of CPD activities.
A manager from a hospital said, “We do not allocatebudget for health professionals to engage in CPDactivities. If there is any invitation, we select usinginternal criteria and send professionals [for training].Very few staff identify CPD activities on their own andwe don’t have any system to track staff involvement inCPD activities.” (HD3)
Table 4 Factoring affecting scope breach, exploring health workforce regulation practices and gaps, Ethiopia, 2015
Variable (Socio-demographiccharacteristics)
Ever carried out tasks not authorized to perform COR (95% CI) AOR (95% CI)
Yes No
Number (%) Number (%)
Type of Health Facility
Hospitala 21 (13.6) 133 (86.4)
Health Center 101 (25.3) 299 (74.7) 2.1 (1.3–3.57)b 1.6 (0.9–2.9)
Sex of respondent
Malea 52 (17.8) 240 (82.2)
Female 70 (26.7) 192 (73.3) 1.7 (1.1–2.5)b 1.2 (0.8–1.9)
Age of respondent in years
20–29a 83 (21.7) 300 (78.3)
30–39 26 (21.5) 95 (78.5) 1.00 (0.6–1.6)
40–49 9 (25.7) 26 (74.3) 1.3 (0.6–2.8)
50–59 4 (26.7) 11 (73.3) 1.3 (0.4–4.2)
Current respondent qualification/profession
Medical Doctora 0 (0.0) 22 (100)
Health Officer 21 (20.6) 81 (79.4) 1.4 (0.7–2.9) 1.4 (0.6–3.0)
Midwife 29 (28.4) 73 (71.6) 2.1 (1.1–4.2)b 2.2 (1.1–4.7)b
Anesthetist 2 (9.1) 20 (90.9) 0.5 (0.1–2.5) 0.9 (0.1–5.0)
Nurse 36 (35.3) 66 (64.7) 2.9 (1.5–5.7)b 2.9 (1.4–5.8)b
Pharmacy 18 (17.6) 84 (82.4) 1.2 (0.6–2.4) 1.2 (0.5–2.4)
Highest level of educational attainment
Diplomaa 74 (25.4) 217 (74.6)
First degree 48 (18.9) 206 (81.1) 0.6 (0.5–1.0)aReference categorybSignificant associationEntries with bold font and astrixes show significant association
Dejene et al. Global Health Research and Policy (2019) 4:36 Page 7 of 12
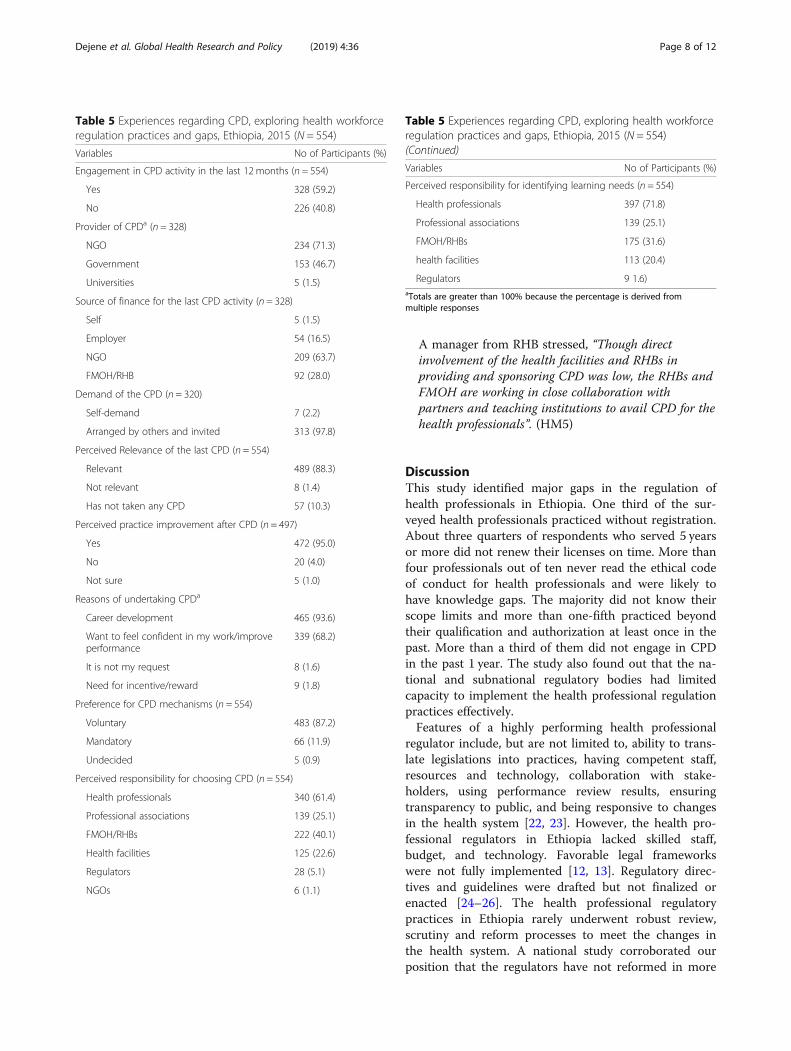
A manager from RHB stressed, “Though directinvolvement of the health facilities and RHBs inproviding and sponsoring CPD was low, the RHBs andFMOH are working in close collaboration withpartners and teaching institutions to avail CPD for thehealth professionals”. (HM5)
DiscussionThis study identified major gaps in the regulation ofhealth professionals in Ethiopia. One third of the sur-veyed health professionals practiced without registration.About three quarters of respondents who served 5 yearsor more did not renew their licenses on time. More thanfour professionals out of ten never read the ethical codeof conduct for health professionals and were likely tohave knowledge gaps. The majority did not know theirscope limits and more than one-fifth practiced beyondtheir qualification and authorization at least once in thepast. More than a third of them did not engage in CPDin the past 1 year. The study also found out that the na-tional and subnational regulatory bodies had limitedcapacity to implement the health professional regulationpractices effectively.Features of a highly performing health professional
regulator include, but are not limited to, ability to trans-late legislations into practices, having competent staff,resources and technology, collaboration with stake-holders, using performance review results, ensuringtransparency to public, and being responsive to changesin the health system [22, 23]. However, the health pro-fessional regulators in Ethiopia lacked skilled staff,budget, and technology. Favorable legal frameworkswere not fully implemented [12, 13]. Regulatory direc-tives and guidelines were drafted but not finalized orenacted [24–26]. The health professional regulatorypractices in Ethiopia rarely underwent robust review,scrutiny and reform processes to meet the changes inthe health system. A national study corroborated ourposition that the regulators have not reformed in more
Table 5 Experiences regarding CPD, exploring health workforceregulation practices and gaps, Ethiopia, 2015 (N = 554)
Variables No of Participants (%)
Engagement in CPD activity in the last 12 months (n = 554)
Yes 328 (59.2)
No 226 (40.8)
Provider of CPDa (n = 328)
NGO 234 (71.3)
Government 153 (46.7)
Universities 5 (1.5)
Source of finance for the last CPD activity (n = 328)
Self 5 (1.5)
Employer 54 (16.5)
NGO 209 (63.7)
FMOH/RHB 92 (28.0)
Demand of the CPD (n = 320)
Self-demand 7 (2.2)
Arranged by others and invited 313 (97.8)
Perceived Relevance of the last CPD (n = 554)
Relevant 489 (88.3)
Not relevant 8 (1.4)
Has not taken any CPD 57 (10.3)
Perceived practice improvement after CPD (n = 497)
Yes 472 (95.0)
No 20 (4.0)
Not sure 5 (1.0)
Reasons of undertaking CPDa
Career development 465 (93.6)
Want to feel confident in my work/improveperformance
339 (68.2)
It is not my request 8 (1.6)
Need for incentive/reward 9 (1.8)
Preference for CPD mechanisms (n = 554)
Voluntary 483 (87.2)
Mandatory 66 (11.9)
Undecided 5 (0.9)
Perceived responsibility for choosing CPD (n = 554)
Health professionals 340 (61.4)
Professional associations 139 (25.1)
FMOH/RHBs 222 (40.1)
Health facilities 125 (22.6)
Regulators 28 (5.1)
NGOs 6 (1.1)
Table 5 Experiences regarding CPD, exploring health workforceregulation practices and gaps, Ethiopia, 2015 (N = 554)(Continued)
Variables No of Participants (%)
Perceived responsibility for identifying learning needs (n = 554)
Health professionals 397 (71.8)
Professional associations 139 (25.1)
FMOH/RHBs 175 (31.6)
health facilities 113 (20.4)
Regulators 9 1.6)aTotals are greater than 100% because the percentage is derived frommultiple responses
Dejene et al. Global Health Research and Policy (2019) 4:36 Page 8 of 12
than a decade time other than the 2008 business processreengineering (BPR). Aiming to improve efficiency, respon-siveness and customer satisfaction, Ethiopia conducted aradical reform process of the public sector including thehealth profession regulation functions through the BPR. Asthe result, the health professional regulatory functions weredecentralized. Enforcement strategies and improved workprocesses were introduced to strengthen capacity of the na-tional and subnational regulators [27]. Even the 2018 an-nual health sector performance review did not adequatelyscrutinize or document scrutiny results of the health pro-fessional regulation practices [28]. Because of this, thehealth professional regulators might find it hard to keeptheir pace with ever expanding number and types of healthprofessionals and facilities, and increasing societal expecta-tions for a safe and quality care. Without the due reforms,the regulation of health professionals in Ethiopia might beliable to outdated practices not matched with internationalbest practices. A policy brief from World HealthOrganization (WHO) emphasizes that health professionalsregulation in many African countries needs to be reformed[7]. But similar challenges are reported in Australia [29].Because of technology limitations, the health professionalregulation data in Ethiopia were not automated, networked
and easily accessible to the public. Updating registrationand licensing data could also be a challenge for the healthprofessional regulators. As a result, the health system can-not ensure transparency and accountability. Standards forentry into professions cannot be met and maintained. Effi-ciency of CPD delivery and management might have beenimproved, had it not been for technology limitations. Weakcapacity of the health professional regulators in Ethiopiaimplied uptake of registration, licensing and CPD amongthe health professionals was not satisfactory. Malpracticeinvolving SOP breaches and ethical lapses appeared to behigh. Similar to the findings of our study, key regulatoryfunctions were not successfully implemented due to weakhealth professional regulation capacity in Cambodia andother African countries [30, 31].Ethiopia has had a state led regulation rather than self-
or co-regulation model. Moreover, the 2008 BPR reformreduced roles of professional associations and elementsof self-regulation. Hence, it was no surprise that wefound inadequate engagement of professional associa-tions, health facilities, training institutions, and otherstakeholders in the health professional regulation prac-tices. In addition, health professionals, health facilities,RHBs and other stakeholders did not adhere to
Table 6 Factoring affecting participation in CPD, exploring health workforce regulation practices and gaps, Ethiopia, March 2015
Variable (Socio demographicCharacteristics)
Participation of in CPD activities in the last 12 months (n = 554) Crude OR (95%CI)
Adjusted OR(95% CI)Yes No
Type of Health Facility
Hospitala 79 (51.3) 75 (48.7)
Health Center 249 (62.2) 151 (37.8) 1.57 (1.08–2.28)b 1.41 (0.86–2.30)
Sex
Malea 164 (56.2) 28 (43.8)
Female 164 (62.6) 98 (37.4) 1.31 (0.93–1.84) 0.90 (0.60–1.33)
Age in years
20–29a 246 (64.2) 137 (35.8)
30–39 64 (52.9) 57 (47.1) 0.63 (0.41–0.95)b 0.78 (0.45–1.35)
40 and above 18 (36.0) 32 (64.0) 0.31 (0.17–0.58) 0.39 (0.16–0.91) b
qualification/profession
Medical Doctora 15 (68.2) 7 (31.8)
Health Officer 55 (53.9) 47 (46.1) 0.55 (0.21–1.45) 0.57 (0.19–1.73)
Midwife 74 (72.5) 28 (27.5) 1.23 (0.46–3.34) 0.90 (0.29–2.83)
Anesthetist 8 (36.4) 14 (63.6) 0.27 (0.08–0.93)b 0.30 (0.08–1.08)
Nurse 74 (72.5) 28 (27.5) 1.23 (0.46–3.34) 1.21 (0.39–3.76)
Pharmacy 41 (40.2) 61 (59.8) 0.31 (0.12–0.84)b 0.23 (0.08–0.72)b
Medical Lab 61 (59.8) 41 (39.0) 0.69 (0.26–1.85) 0.56 (0.19–1.70)
Highest level of education
Diploma 184 (63.2) 107 (36.8)
First degree and 144 (54.9) 119 (45.1) 1.40 (0.99–1.97) 1.13 (0.69–1.87)aReference Categorybsignificant association
Dejene et al. Global Health Research and Policy (2019) 4:36 Page 9 of 12
regulation enforcement strategies developed during theBPR reform process. Hiring unregistered and unlicensedprofessionals, lack of ethics support system and weakCPD tracking mechanisms were not taken seriously andcorrected accordingly. Though the professional associa-tions developed ethical codes, CPD courses, and theSOP for their professions, these resources were notwidely utilized. In 2002, a health professional councilwas established and tasked with an advisory role for thenational regulatory body. But the council worked onlyfor few years and was ineffective [24]. In Cambodia, col-laboration with stakeholders was also reported as weak[30]. In contrast to the situation in Ethiopia, low andmiddle income countries like Egypt, Nigeria andPakistan have had functional professional councils toguide health workforce regulation [32].Global evidences recommend establishing stronger
ethics support systems for health professionals [33, 34].However, a lack of robust ethics support functions at alllevels of the health system in Ethiopia might have con-tributed to low ethics awareness and high malpracticeamong health professionals. Our study findings showedthat health professionals were not supported and moni-tored with proper health ethics and code conduct func-tions. Researches from Ethiopia and other countries alsoreported similar problems [35–37]. Since ethical di-lemmas during clinical care are generally prevalent(Challa: Ethical dilemmas and decision making processin emergency departments of experiences of physiciansin Addis Ababa, Ethiopia, unpublished), in the absenceof such ethics support system, the health professionalsin Ethiopia might not be able to provide safe and indi-vidualized care that satisfy patients [38]. Therefore, theGovernment of Ethiopia should strengthen health ethicssupport system through building local capacity, anddelegating some functions to health facilities and profes-sional associations.In the ideal context, health professionals should prac-
tice under professional SOP: competencies they wereadequately trained on. But this was not happening for anumber of reasons like shortage of professionals, lowhealthcare access and others [39, 40]. In our study, prac-tice beyond scope limits was common especially amongnurses and midwives in rural areas where there wasshortage of doctors. This might be exacerbated by theoccurrence of health emergencies and poor referral link-age. Because of this, many facility managers perceivedworking beyond one’s SOP to be ok. The unfinished na-tional SOP directive was one of underlying reasons forthe problem. Health facilities had difficulties to developand communicate job descriptions to healthcare pro-viders, which might have created clarity on the scopes.Endorsing the national SOP directive would informstakeholders to ensure professional practice within the
scope limits. Health facilities should communicate up-dated job descriptions in line with the SOP directive andfollow the implementation.The lower CPD participation rate in our study could
be due to poor awareness of the importance of CPD asreported elsehwere [41–43]. It could also be the misper-ception that CPD is only short term face to face training.Health professionals might not report clinical updatemeetings, rounds, online courses, conferences, self-studyand others as CPD undertakings. In contrast, health pro-fessionals in Malawi had high CPD participation rate asthey were using various CPD means [44]. To be more ef-fective, CPD must be need based and mandatory for allprofessionals and linked to relicensing. This was empha-sized in the Ethiopian CPD directive [24]. But, the re-spondents in our study rarely identified their CPDneeds. Removing barriers, providing incentives and de-signing individualized CPD events could improve CPDparticipation among the health professionals. The CPDcourses were more donor driven and implemented byNGOs. With the large limitation of the CPD system inthe country, Ethiopia might not be able to improve per-formance of health professionals and patient outcomesto the desired level [45].The huge regulatory gaps found in our study might
have detrimental effects on the health system perform-ance. Unless meaningful measures are taken to revitalizenational regulatory capacity, it will be difficult to ensurepatient safety and quality of care. Further studies arerecommended on the effects and costs of weak regula-tion on the health system.
Strengths and limitationsThe fact that our study was based on a national sampleof the major clinical workforce should be considered astrong point. The addition of a qualitative study tounderstand the regulatory challenges and weaknesses inways that might not have been known in a quantitativesurvey alone is another strength. However, our study in-cluded only a negligible number of health professionalswith postgraduate qualifications. We also recognize thatthe findings may not be generalizable to health profes-sionals in the private sector. We acknowledge that across-sectional study based on self-report is susceptibleto recall and social desirability biases.
ConclusionsDespite favorable legal frameworks for health profes-sional regulation, the implementation lagged behind.Multiple gaps in the health profession regulation prac-tices were observed. Significant strides to translate regu-lation policy into actions are needed through buildingcapacity of the national and subnational regulators withappropriate staff, resources and technology. Finalizing
Dejene et al. Global Health Research and Policy (2019) 4:36 Page 10 of 12

and implementing the regulation directives and guide-lines require attention. Reinstituting health professionalcouncil and enforcement strategies would improve theregulation practices. Strengthening ethics supportfunctions at facilities is imperative. Health professionalsshould be trained for the additional tasks before job as-signment if there is a need for them to go outside theirbasic scope limits. Access to need-based CPD linked tore-licensing should be prioritized. Providing incentivesand removing barriers can improve CPD uptake amonghealth professionals. Besides, future studies are sug-gested for assessing the effects and costs of poor regula-tion on the health system.
Supplementary informationSupplementary information accompanies this paper at https://doi.org/10.1186/s41256-019-0127-x.
Additional file 1: Table S1. Experiences on CPD, exploring healthworkforce regulation practices and gaps, Ethiopia, March 2015.
AbbreviationsAOR: Adjusted odds rate; BPR: Business process reengineering; CDC: Centerfor Disease Control and Prevention; CI: Confidence interval; CPD: Continuingprofessional development; FMHACA: Food, Medicine, HealthcareAdministration and Control Authority; FMOH: Federal Ministry of Health;HD: Hospital director; HM: Health manager; HR: Health regulator;HRH: Human resources for health; HSTP: Health Sector Transformation Plan;ICN: International Council for Nurses; IRB: Institutional Review Board;JHU: Johns Hopkins University; KII: key informant interview/s; NGOs: Non-governmental organizations; RHBs: Regional Health Bureaus; SOP: Scope ofpractice; WHO: World Health Organization
AcknowledgementsThe authors would like to acknowledge the following organizations andpersons for providing unreserved support and motivation to complete thisimportant study:1. United States of Agency for International Development (USAID)2. Jhpiego-Ethiopia country office and the Strengthening Human Resourcesfor Health (HRH) Project3. Federal Ministry of Health (FMOH) of Ethiopia4. Food, Medicine, Healthcare Administration and Control Authority and itsubnational bodies5. Hospitals and health centers6. Health professionals and managers who participated in the study
Authors’ contributionsDD- supported designing and development of proposal and data collectioninstruments, data analysis, and write up of this study. TY – supported thedesigning and development of proposal, data collection instruments, dataanalysis and write up of this study. SM- supported the designing anddevelopment of proposal, data collection instruments, data collection, andanalysis. FA- supported the designing and development of data collectioninstrument, data collection, data analysis and write up. MK – supported datacollection, data analysis and write up. DW – supported data analysis andwrite up. All authors read and approved the final manuscript.
FundingThis study was financially supported during proposal development, datacollection, data analysis and manuscript development by strengtheninghuman resources for health (HRH) project funded by USAID.
Availability of data and materialsThe datasets used and/or analyzed during this study are available from thecorresponding author up on reasonable request.
Ethics approval and consent to participateAuthors declare that the study was conducted after securing ethicalclearance from Johns Hopkins School of Public Health IRB and obtainingconsents from study participants.
Consent for publicationNot applicable.
Competing interestsThe authors declare that they have no competing interests.
Author details1Jhpiego, Kirkos Subcity, PO Box 2881, Code 1250 Addis Ababa, Ethiopia.2Individual consultant, Addis Ababa, Ethiopia.
Received: 16 August 2019 Accepted: 14 November 2019
References1. World Health Organization. Monitoring the building blocks of health
systems: a handbook of indicators and their measurement strategies: TheWHO press; 2010. https://www.who.int.
2. World Health Organization. Global strategy on human resources for health:workforce 2030: The WHO Press; 2016. https://apps.who.int.
3. Speybroeck N, Kinfu Y, Dal Poz MR, Evans DB. Reassessing the relationshipbetween human resources for health, intervention coverage and healthoutcomes. Evidence and information for policy: World Health Organization;2006. https://pdfs.semanticscholar.org/fb21/eb31a783e802b2869f291ad29c80bf26ff04.pdf.
4. World Health Organization and Australian Health Practitioner RegulationAgency. Health workforce regulation in the Western Pacific region: TheWHO Press; 2014. https://apps.who.int.
5. McKimm J, Newton PM, Da Silva A, Campbell J, Condon R, et al. Regulationand licensing of healthcare professionals: a review of international trendsand current approaches in Pacific Island countries. Sydney: HumanResources for Health Knowledge Hub; 2013.
6. Barry J. Regulatory board governance toolkit. ICN regulation series:International council for nurses; 2014. https://www.icn.ch.
7. World Health Organization. Transforming and scaling up health professionaleducation and training. Policy brief on regulation of health professionseducation: The WHO press; 2013. https://apps.who.int/iris/bitstream/handle/10665/93635/9789241506502_eng.pdf;jsessionid=F9018319F24B7B1A1295B75039CD06FA?sequence=1.
8. World Health organization. Transforming and scaling up healthprofessionals’ education and training: World health Organization guidelines;2013. https://www.who.int/hrh/resources/transf_scaling_hpet/en/.
9. The Federal Democratic Republic of Ethiopia Ministry of Health. Healthsector transformational plan (HSTP). 2015/16–2019/20. Ethiopia; 2015.https://www.globalfinancingfacility.org/sites/gff_new/files/Ethiopia-health-system-transformation-plan.pdf.
10. The Federal Democratic Republic of Ethiopia Ministry of Health. Nationalhuman resources for health strategic plan for Ethiopia. 2016–2025. 2016.
11. Feyisa B, Herbst CH, Lemma W, Soucat A. The health workforce in Ethiopia:addressing the remaining challenges, a World Bank study; 2012.
12. Council of ministers. Regulation number 299/2013. To provide food,medicine, health care administration and control, Federal negarit gazzetta.2014.
13. Council of ministers, Regulation number 76/2002. Ethiopian healthprofessions council establishment, Federal negarit gazzetta. 2002.
14. Higher education relevance and quality agency and Federal Ministry ofHealth. Revitalizing the quality of health profession education in Ethiopia.2014.
15. Mccarthy CF, Voss J, Salmon ME, Gross JM, Kelley MA, Rilley PL. Nursing andmidwifery regulation reform in east, central and south Africa. A survey ofstakeholders. Hum Resour Health. 2013;11:29.
16. Jafari M, Currie S, Qarani WM, Azimi MD, Manalai P, Zyaee P. Challenges andfacilitators to establishment of a midwifery and nursing council inAfghanistan. Midwifery. 2019;75:1.
17. Ministry of Health and Sanitation. Human resources for health Sierra Leonecountry profile. 2016.
Dejene et al. Global Health Research and Policy (2019) 4:36 Page 11 of 12
18. World Health Organization. Assessment of human resources for health:survey instruments and guide to administration. 2002.
19. Center for Disease Control (CDC). Epi Info™, a database and statisticsprogram for public health professionals. Atlanta, GA, USA. 2011.
20. StataCorp LP. Stata Statistical Software: Release 13. College Station, TX; 2013.21. University of Umeå. ICT Services and System Development and Division of
Epidemiology and Global Health. OpenCode 3.6. Sweden. 2013.22. Benton DC, González-Jurado MA, Beneit-Montesinos JV. Defining nurse
regulation and regulatory body performance: a policy Delphi study. Int NursRev. 2013;60:303–12.
23. Benton DC. Analysis and priorities: developing a modern, effective,regulatory framework. J Nurs Regul. 2017;8(Issue supplement 2):S44.
24. Ethiopian Food, Medicine and Healthcare Administration and ControlAuthority. Directive on continuing professional development for healthprofessionals. Addis Ababa: FMHACA; 2013.
25. Ethiopian Food, Medicine and Healthcare Administration and ControlAuthority. Directive of registration and licensure for health professionals.Addis Ababa: FMHACA; 2014.
26. Ethiopian Food, Medicine and Healthcare Administration and ControlAuthority. Directive on health professional scope-of-practice. Addis Ababa:FMHACA; 2014.
27. Solomon L. Framework and enforcement strategy for health professionsregulation in Ethiopia; 2012.
28. Federal ministry of health. Annual performance review report: health sectortransformation plan 2015/16. 2016.
29. Wardle JL, Sibbritt D, Broom A, Steel A, Adams J. Is health practitioners’regulation keeping pace with change in practitioner and health carelandscape? An Australia perspective. Front Public Health. 2016;4:91.
30. Clarke D, Duke J, Wuliji T, Smith A, Phuang K, San U. Strengthening healthprofessional regulation in Cambodia: a rapid assessment. Hum ResourHealth. 2016;14:9.
31. Gross JM, Kelley M, McCarthy C. The model for advancing professionalnursing collaboration. Africa health professions regulation collaborative. JNurse Regul. 2015;6(3). www.journalofnursingregulation.com.
32. de Vries H, Sanderson P, Janta B, Rabinovich L, et al. Internationalcomparison of ten medical regulatory systems: Egypt, Germany, Greece,India, Italy, Nigeria, Pakistan, Poland, South Africa and Spain. Santa Monica:RAND Corporation; 2009.
33. World health organization. Global health ethics key issues, global networksof WHO collaborating centers on bioethics. 2015.
34. Rasaol D, Skovdahl K, Gifford M, Kihlgren A. Clinical ethics support for healthprofessionals: an integrative literature review. HEC Forum. 2017;29:313.
35. Tiruneh MA, Ayele BT. Practice of code of ethics and associated factorsamong medical doctors in Addis Ababa Ethiopia. PLoS One. 2018;13(8):e0201020.
36. Milieteig I, Onaheim K, Johansson KA BF, Dessalegn D. Ethics capacitybuilding in low-income countries: Ethiopia as a case study. Tidsskrift for denNorske Legeforening. 2017;137(22). https://tidsskriftet.no/sites/default/files/generated_pdfs/49805-ethics-capacity-building-in-low-income-countries-ethiopia-as-a-case-study.pdf.
37. Adhikari S, Aro AR, Paudel K, Adhikari TB. Knowledge, attitude and practiceof healthcare ethics among resident doctors and ward nurses in resourcepoor setting, Nepal. BMC Med Ethics. 2016;17:68.
38. Ogunbanjo GA, Knapp van Bogaert D. Ethics in health care, the practice ofdefensive medicine. S Afr Fam Pract. 2014;56:S6.
39. Federation of state medical boards. Assessing scope of practice in healthcare delivery. critical questions in assuring public access and safety USA.2005.
40. Dower C, Moore J, Langelier M. It is time to restructure health professionals’scope of practice regulations to remove barriers to care: analysis andcommentary. Health Aff. 2013;32:1971.
41. Assemelash D, Binega G, Kass M. Involvement of community pharmacist incontinuing professional development (CPD). A baseline survey Gondor,Northwest Ethiopia. Global Health. 2018;14(1):15. https://www.ncbi.nlm.nih.gov/pubmed/29391021.
42. Wiam E, Elamrdi A, Alyafie S, Abuzaid M. Continuing professionaldevelopment in radiography: practice, attitude and barriers; 2015.
43. Feldack C, Pintye J, Jacob S, Chung MS, Middleton L. Continuingprofessional development for medical, nursing, and midwifery cadres inMalawi, Tanzania and South Africa: A qualitative evaluation. PLoS One. 2017;12:e0186074.
44. Muula AS, Misiri H, Chimalizeni Y, Mpando D, Phiri C, Nyaka A. Access tocontinued professional education among health workers in Blantyre,Malawi. Afr Health Sci. 2004;4(3):182.
45. Mathers N, Mitchell C, Hunn A. A study to assess the impact of continuingprofessional development (CPD) on doctors’ performance and patient/service outcomes for the GMC; academic unit of primary care, TheUniversity of Sheffield, Capta Health; 2012.
Dejene et al. Global Health Research and Policy (2019) 4:36 Page 12 of 12





























