Embed Size (px)
Citation preview

This article was downloaded by: [Northeastern University]On: 16 December 2014, At: 15:39Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registeredoffice: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Ethnicity & HealthPublication details, including instructions for authors andsubscription information:http://www.tandfonline.com/loi/ceth20
Exploring health beliefs and care-seeking behaviors of older USA-dwelling Mexicans and Mexican-AmericansAnissa T. Rogers aa Department of Social and Behavioral Sciences , University ofPortland , 5000 N. Willamette Blvd, Portland, OR, 97203, USAPublished online: 06 Aug 2010.
To cite this article: Anissa T. Rogers (2010) Exploring health beliefs and care-seeking behaviorsof older USA-dwelling Mexicans and Mexican-Americans, Ethnicity & Health, 15:6, 581-599, DOI:10.1080/13557858.2010.500018
To link to this article: http://dx.doi.org/10.1080/13557858.2010.500018
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the“Content”) contained in the publications on our platform. However, Taylor & Francis,our agents, and our licensors make no representations or warranties whatsoever as tothe accuracy, completeness, or suitability for any purpose of the Content. Any opinionsand views expressed in this publication are the opinions and views of the authors,and are not the views of or endorsed by Taylor & Francis. The accuracy of the Contentshould not be relied upon and should be independently verified with primary sourcesof information. Taylor and Francis shall not be liable for any losses, actions, claims,proceedings, demands, costs, expenses, damages, and other liabilities whatsoeveror howsoever caused arising directly or indirectly in connection with, in relation to orarising out of the use of the Content.
This article may be used for research, teaching, and private study purposes. Anysubstantial or systematic reproduction, redistribution, reselling, loan, sub-licensing,systematic supply, or distribution in any form to anyone is expressly forbidden. Terms &Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions

Exploring health beliefs and care-seeking behaviors of olderUSA-dwelling Mexicans and Mexican-Americans
Anissa T. Rogers*
Department of Social and Behavioral Sciences, University of Portland, 5000 N. Willamette Blvd.,Portland, OR 97203, USA
(Received 21 January 2010; final version received 7 June 2010)
Objective. This study explored health beliefs and healthcare-seeking behaviors ofolder USA-dwelling Mexicans and Mexican-Americans using the Theory ofPlanned Behavior (TPB) as a conceptual guide.Design. A mixed-method cross-sectional design was utilized using semi-structuredinterviews to obtain detailed descriptions of 31 older (50�) participants’behavioral, normative, and control beliefs about health and healthcare utilization.An interview schedule consisting of open-ended and demographic questions andone standardized tool, the Bidimensional Acculturation Scale (BAS) forHispanics, was used to collect data.Results. Several themes emerged for each belief area. Behavioral belief themesreflect participants’ faith in, comfort with, and knowledge of traditional methodsof care (e.g., herbs, teas, and use of curanderas) as well as their faith in theeffectiveness of conventional care (e.g., medicine, technology, and use ofphysicians). Normative belief themes indicate that participants perceive thatfamily and community contacts support participants’ use of traditional methodsand that family supports use of conventional methods. Control belief themessuggest that traditional methods are accessible and affordable but that conven-tional methods are not. BAS scored indicated that most (90.3%) participantsadhered to Hispanic culture. Two (6.5%) participants adhered to non-Hispanicculture and one (3.2%) scored as bi-cultural.Conclusions. Themes from the data suggest that beliefs about healthcare impactthe types of care utilized and the ways in which they are utilized. Clinicians andresearchers striving to reduce health disparities and develop more culturallycompetent healthcare services for ethnic minority groups should work toward abetter understanding of minority groups’ belief systems about healthcare and itsutilization. Utilization of the TPB allows for empirical model development thatcan better predict healthcare utilization behavior, further augmenting efforts toprovide services that will help reduce health disparities for older Mexicans andMexican-Americans and other populations.
Keywords: Latino/a; health; immigrants; cultural competence practice; disparities(health, racial)
Introduction
As a group, Latinos in the USA suffer from poorer health outcomes than their non-
Hispanic White counterparts (Smedley et al. 2003, Nielsen-Bohlman et al. 2004,
Kaiser Family Foundation 2005a). Factors contributing to health disparities include
*Email: [email protected]
Ethnicity & Health
Vol. 15, No. 6, December 2010, 581�599
ISSN 1355-7858 print/ISSN 1465-3419 online
# 2010 Taylor & Francis
DOI: 10.1080/13557858.2010.500018
http://www.informaworld.com
Dow
nloa
ded
by [
Nor
thea
ster
n U
nive
rsity
] at
15:
39 1
6 D
ecem
ber
2014

advancing age, language barriers, and poor health literacy (U.S. Department of
Health and Human Services 2004). While various socioeconomic characteristics are
associated with health disparities, these characteristics only partially explain why
Latino people in general, and older Latino people in particular, have highermorbidity and mortality rates and poorer access to healthcare services than non-
Latino Whites. Indeed, health disparities experienced by Latino groups are thought
to be the result of complex interactions between and among cultural, socioeconomic,
and environmental variables (U.S. Department of Health and Human Services 2000).
While constructs such as health beliefs, health practices, and cultural norms about
health are likely to contribute to health disparities, little is known about how these
factors influence perceptions about health, which in turn influence health-related
behaviors.Because of the complexity of grouping diverse Latino cultures under the rubric of
‘Hispanic’ or ‘Latino,’ methodological shortfalls in capturing cultural subtleties
between and within Latino groups, and health issues specific to older Latinos,
particularly as they age in place in the USA, there is a need for more qualitative
approaches that investigate individual beliefs related to health behaviors and better
articulate relationships between various constructs (such as cultural norms and
perceived control over health) and behaviors that lead to poor health outcomes.
Further, more research is needed to determine how to organize constructs in a modelthat can be tested, replicated, and explain how these constructs interact to determine
specific health outcomes (National Academies Press 2003, Kaiser Family Founda-
tion 2005b). Thus, the aim of this study was to explore the health beliefs of a specific
group of Latinos, older Mexicans, and Mexican-Americans living in the USA, using
the Theory of Planned Behavior (TPB) (Ajzen 1991) as a conceptual guide. By
understanding health-related beliefs, it is possible to better articulate the processes
that influence people’s actions in health-related situations, leading to more accessible,
effective, and culturally competent approaches to health services that will reducehealth disparities for underserved populations.
Health disparities and care-seeking behaviors among older Mexicansand Mexican-Americans
Many researchers and healthcare professionals agree that the key to decreasing
health disparities is to improve the quality of and access to healthcare, particularly
for older patients. Research indicates that health disparities can be accounted for, inpart, by problems in communication, poor ‘cultural matches’ between patients and
providers, and specific behaviors of patients and providers (Kaiser Family Founda-
tion 2005b). However, many other factors contribute to health disparities for older
Mexicans and Mexican-Americans. Social context, which includes culture, is
important to consider when examining health outcomes, yet it is poorly understood
(Kaiser Family Foundation 2005a). Culture, or the norms, beliefs, values, and
traditions that influence people’s world views (Helman 1994), gives meaning to
health, health information, and perceptions about appropriate health-relatedbehaviors. It determines the type and quality of communication between individuals,
families, communities, and providers about health, illness, and healthcare-seeking
behaviors. The experience of culture also is not static. Often as people age, move, and
gain experiences, their perceptions change as they adapt to new situations and
582 A.T. Rogers
Dow
nloa
ded
by [
Nor
thea
ster
n U
nive
rsity
] at
15:
39 1
6 D
ecem
ber
2014

environments. Acculturation, then, as part of culture, impacts how people think
about health and interact with various healthcare systems (Nielsen-Bohlman et al.
2004).
Individual characteristics also interact with cultural characteristics to furtherinfluence a person’s perceptions and behaviors. Personal beliefs and attitudes about
health, illness, what should be done in case of illness, and perceived access to desired
care all influence individual health behaviors. Further, age, income, education,
transportation, legal status, health literacy, language ability, familial patterns,
geographic location, community support and resources, and ability to navigate
healthcare systems are only a few of the factors that, combined with cultural factors,
affect care-seeking behaviors and the perceived control people feel they have over
accessing care (National Academies Press 2002, Kaiser Family Foundation 2005a,Rogers and Gallegos 2007).
Institutional and other barriers also contribute to disparate health outcomes. For
example, health jargon, language barriers, and competing and conflicting health
messages and sources of information can create insurmountable barriers to care
(Nielsen-Bohlman et al. 2004). Geographical and physical barriers to facilities,
negative interactions with healthcare systems, and a lack of knowledge about how to
utilize systems can create problems for patients, particularly older patients. Time
constraints and biases or uncertainties about how to work with older minoritypatients may create problems for providers (Smedley et al. 2003). Age and race
discrimination are even larger, more entrenched institutional issues that contribute to
health disparities and create barriers for older minority individuals in receiving
equitable effective care (National Academies Press 2003).
Theoretical background and conceptualization
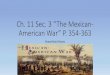
To conceptualize and explore how individual and cultural factors influence healthbehaviors, the TPB (Ajzen 1991) was used to guide and organize constructs in this
study. According to the TPB, behavioral beliefs are personal beliefs that underlie
people’s attitudes about particular behaviors. Normative beliefs are beliefs that people
perceive are held by individuals or groups within one’s culture or environment about
behaviors, and these beliefs underlie people’s subjective norms about particular
behaviors. Control beliefs are beliefs that people perceive either hinder or help to
facilitate behaviors, and they underlie people’s perceived behavioral controls. This
theory posits that ‘salient’ beliefs, or the most important beliefs about behaviors, arethe determinants of behavioral intentions (Ajzen and Fishbein 1980, 2000, Ajzen
1988, 1991). Figure 1 offers a visual display of the theoretical concepts and how they
function to influence behavior.
This theory emphasizes the importance of beliefs about healthcare-seeking
behaviors, which is an important step to understanding the complex interplay
between cultural and individual factors that influence people’s care-seeking
behaviors. Using the TPB, this study explores beliefs of older Mexicans and
Mexican-Americans regarding use of various types of healthcare. Because of thecomplexity of problems related to health disparities, a better understanding of
cultural and individual beliefs that affect health-related attitudes, norms, and
perceived control over health is needed to better articulate how these factors impact
decision-making processes about healthcare. This enhanced understanding will assist
Ethnicity & Health 583
Dow
nloa
ded
by [
Nor
thea
ster
n U
nive
rsity
] at
15:
39 1
6 D
ecem
ber
2014

in developing and implementing more effective, accessible, comprehensive, and
culturally appropriate healthcare services that will help to permanently reduce health
disparities among older Mexicans and Mexican-Americans and other ethnic
minority groups (National Academies Press 2003, Kaiser Family Foundation 2005b).
Methods
This study employed a non-experimental, mixed-method (Morse 1994, Creswell
2003), cross-sectional design to explore participants’ behavioral, normative, and
control beliefs regarding use of traditional (e.g., herbs, sweat lodges, and providers of
care, such as curanderos and yerberos) and conventional (e.g., medications,
technology, providers of care such as nurses and physicians) healthcare using one-
on-one in-depth interviews. Researchers argue that qualitative approaches are the
best methods to use to study health disparities because of the complex factors related
to the issue (Smedley et al. 2003). When guided by a theoretical framework,qualitative methods offer a better understanding of individual perceptions than can
be gained through quantitative means alone. Further, qualitative methods allow for
theory development by allowing for exploration of the meaning of constructs and
interrelationships between them that may not have been identified in previous
research (Creswell 1998). Thus, in-depth explorations of concepts related to health
expand our knowledge of these issues and assist in developing more effective
culturally competent solutions to health disparities.
To assist with the project, a research team was formed that included leaders in theLatino community, bilingual/bicultural interviewers, and community-based advisory
committee members. This team informed the development and implementation of
the project and assisted in identifying community targets that could benefit from
dissemination of results. Before the study began, research ethics approval was
secured through the author’s home institution and the governmental entity
overseeing the agencies from which participants were recruited.
Participants
A convenience sample of 31 older community-dwelling Mexican and Mexican-
American adults living in a northwest metropolitan area in the USA were recruited
through several non-health-related community agencies. Members of the research
team identified community agencies known to serve large numbers of older Latinos
Behavioral
Beliefs
Normative
Beliefs
Control
Beliefs
Perceived
Behavioral
Control
Subjective
Norm
Attitude
Intention Behavior
Figure 1. The Theory of Planned Behavior.
584 A.T. Rogers
Dow
nloa
ded
by [
Nor
thea
ster
n U
nive
rsity
] at
15:
39 1
6 D
ecem
ber
2014

and contacted staff of these agencies to recruit participants for the study. Staff of
these agencies discussed the purpose of the study with clients meeting eligibility
requirements and referred participants to the project’s research assistant, who set up
appointments between interviewers and participants. Clients were deemed eligible to
participate if they were aged 50�, identified Mexico as their country of origin
(whether first or subsequent generation), and showed no cognitive impairments that
would hinder the interview. Participants received $15.00 compensation for their time.
Selected demographic information was collected on individuals who chose not to
participate (N�3); analyses on these data indicated no significant differences on
demographic characteristics between participants and non-participants.
The age range of the participants was 54�85 (M�68) and most were female
(87%). On average, participants reported suffering from two illnesses, primarily
diabetes and high blood pressure. Participants reported, on average, taking two
medications for their ailments. They also reported, on average, turning to teas and
vitamins to help manage their physical symptoms and health. Table 1 displays
demographic characteristics of the sample.
Age 50 was selected as the minimum age for study inclusion for two reasons.
First, the Latino population in general is young; the median age is approximately 25
(Bureau of the Census 2000). Further, Latinos as a group suffer from dispropor-
tionate rates of disability and mortality at young ages from chronic illnesses
compared to other ethnic groups (National Institutes of Health 2000), which
underscores the need to consider aging from a functional (versus chronological)
standpoint to ensure adequate sample size.
An attempt was made to recruit equal numbers of women and men and select
individuals with varying demographic characteristics (e.g., income and education
levels; time living in the USA) to reflect a wide range of experiences. Given the
diverse cultural, political, economical, historical, and geographical experiences
captured by the term ‘Latino,’ participants were limited to a subgroup of ‘Latino’
defined as individuals who identify Mexico as their country of origin to allow for
comparison of beliefs within the sample. Immigrant or first, second, or third
generation Mexican-Americans were recruited to account for levels of acculturation.
Though care was taken to oversample men to obtain equal numbers of men and
women, only a few men were recruited. This may be a function of few men utilizing
services in the targeted agencies. Further, authors of the TBP (Fishbein and Ajzen
1975, Ajzen and Fishbein 1980, 2000, Ajzen 1988, 1991) and other researchers
(Godin and Kok 1996) recommend a sample size of 25 for eliciting beliefs. Thus, 31
participants were interviewed to ensure that at least 25 valid interviews were realized.
Data collection
An interview schedule consisting of open-ended and demographic questions and one
standardized tool was used. Three sets of qualitative questions were developed using
guidelines from the TPB (Francis et al. 2004) and community partner input. One set
explored participants’ behavioral beliefs or perceived advantages and disadvantages
of using traditional and conventional methods of care; another set explored
participants’ normative beliefs or participants’ perceptions of what significant others
think about participants using traditional and conventional types of care; and the
Ethnicity & Health 585
Dow
nloa
ded
by [
Nor
thea
ster
n U
nive
rsity
] at
15:
39 1
6 D
ecem
ber
2014

Table 1. Participant demographics (N�31).
Variable N %
Gender
Female 27 87.1
Male 4 12.9
Marital status
Married 9 29.0
Divorced 2 6.5
Widowed 12 38.7
Single 7 22.6
Separated 1 3.2
Income
$0�$10,000 26 83.9
$10,001�$20,000 1 3.2
$20,001�$30,000 3 9.7
$30,001�$40,000 0 0.0
$40,001�$50,000 1 3.2
Educationa
Primary school completed 16 51.6
Secondary school completed 9 29.0
Professional school completed 6 19.4
University education completed 2 6.5
Graduate school completed 0 0.0
Religion
Catholic 27 87.1
Adventist 2 6.5
Jehovah’s witness 1 3.2
Other (‘Christian’) 1 3.2
Employment history
Domestic labor 5 16.1
Teaching 1 3.2
Vending/sales 5 16.1
Agriculture 1 3.2
Skilled labor 6 19.4
Unskilled labor 5 16.1
Formal caregiving 2 6.5
Professional work 2 6.5
Religious work 3 9.7
No work history 1 3.2
Geographic area of origin
USA
Montana 1 3.2
Texas 1 3.2
Mexico
Chihuahua 1 3.2
Distrito Federal 4 12.8
Durango 1 3.2
Guanajuato 2 6.5
Guerrero 1 3.2
Jalisco 5 16.1
586 A.T. Rogers
Dow
nloa
ded
by [
Nor
thea
ster
n U
nive
rsity
] at
15:
39 1
6 D
ecem
ber
2014

third set explored participants’ control beliefs or participants’ beliefs about the
extent to which they were able to use traditional and conventional types of care.
Participants also responded to the Bidimensional Acculturation Scale (BAS) for
Hispanics (Marın and Gamba 1996), which is a 24-item Likert-type scale consisting
of three subscales measuring language use, linguistic proficiency, and electronic
media use, where 4�‘very well/almost always’ and 1�‘very poorly/almost never.’
Subscales yield scores for both Hispanic and non-Hispanic acculturation. High
scores on both indicate bi-culturality. The BAS provides effective bidimensional
acculturation measurement (i.e., bidirectional changes in behavior accounting for
acculturation to a new culture and identification to the culture of origin). Concurrent
validity and reliability coefficients range from 0.31 to 0.88, indicating that the
subscales show strong validity and reliability in measuring acculturation (Marın and
Gamba 1996). Examples of questions include, ‘How often do you speak English?’
and ‘How often do you watch television programs in English?’ The BAS has been
translated into Spanish and validated for use with Latino populations. Items from
this scale were used to inform and augment participants’ responses to open-ended
items. Finally, demographic items were included in the interview schedule to describe
the sample and to inform and enhance the meaning gained through qualitative data.
To develop items in the interview schedule, several best-practice guidelines were
followed (e.g., Marın and Marın 1991, Guillemin et al. 1993, Chang et al. 1999, Skaff
et al. 2002, Maneesriwongul and Dixon 2004). The research team met to develop,
translate, and review questions. The open-ended and demographic questions were
reviewed and revised several times to ensure cultural sensitivity and relevancy for the
study population. Items in the interview schedule were then back-translated by the
research team, and pilot-tested to revise and clarify the meaning of questions.
Interviews were conducted by two bilingual/bicultural interviewers trained on
qualitative research methods, cultural issues in interviewing, and administering the
interview schedule. Training also included methods reported to improve reliability
and validity of qualitative studies by decreasing researcher effects (e.g., not ‘inflating’
the problem under study; maintaining a not knowing stance, conducting interviews
in locations comfortable for participants; using probing questions to enhance
meaning; conducting interviews in the participants’ language of choice; and keeping
field notes) (Miles and Huberman 1994). Pilot tests were conducted to establish
Table 1 (Continued )
Variable N %
Michoacan 2 6.5
Mexico 2 6.5
Morelos 3 9.7
Nayarit 2 6.5
Oaxaca 2 6.5
Puebla 2 6.5
Sinaloa 1 3.2
Zacatecas 1 3.2
M Range
Age of migration to the USA 39 5�71
aTotal does not equal 100% since respondents could complete more than one level of education.
Ethnicity & Health 587
Dow
nloa
ded
by [
Nor
thea
ster
n U
nive
rsity
] at
15:
39 1
6 D
ecem
ber
2014

inter-rater reliability for administering the BAS, which yielded strong correlations
(0.80) between raters, and to ensure conformity between interviewers with regard to
following interview protocol, particularly around asking qualitative questions in
identical ways with identical prompts. On average, interviews took about one and ahalf hours to complete. Most interviews were conducted in Spanish and took place at
the recruiting agency or in participants’ homes.
Analyses
Data from interviews were transcribed and, when needed, translated by a trained
bilingual transcriptionist. Qualitative data were analyzed by the primary investigator
on textual, conceptual, and organizational levels using ATLAS-ti (ATLAS.ti, Berlin,Germany). An interpretive�phenomenological methodwas employed to emphasize the
importance of the social context in which participants experience their world and the
ways in which their world impacts their experiences of health and illness (Benner 1994).
Following guidelines from the TPB (Francis et al. 2004), textual data were coded and
analyzed to find themes, or ‘salient beliefs,’ in each belief area. To increase reliability
and internal and external validity of the study, several procedures were employed
throughout the analysis process. First, coded themes were cross-checked for meaning
by a group of Latino leaders who were part of the research team (Miles and Huberman1994, Ryan and Bernard 2003). Second, ‘extreme’ cases were identified and analyzed to
check for representativeness; thus, two cases that scored as ‘acculturated’ on
the BAS were examined to determine that their beliefs did not differ significantly
from the other cases. Third, datawere examined for ‘negative cases’ or those caseswhere
content or themes did not fit the model, disconfirmed patterns, or refuted emerging
constructs; none were found (Miles and Huberman 1994).
Descriptive statistics were generated on demographic and acculturation variables.
Relationships between these variables and open-ended responses were explored todetermine whether any individual differences existed for health beliefs based on
demographic characteristics (e.g., age, income, education level, or acculturation
level). Specifically, different levels of demographic characteristics (e.g., higher income
versus lower income; older age versus younger age) were compared to corresponding
open-ended responses to ascertain whether different demographic characteristics
were correlated to particular open-ended responses. All results were examined for
outlying or extreme cases, ‘surprising’ responses from participants, or responses that
‘disconfirmed’ themes or that refuted a theoretical construct (Miles and Huberman1994).
Results
Table 2 offers a summary of the themes that emerged from the qualitative questions
for each belief area.
Behavioral beliefs
According to themes that emerged from participants’ responses in this belief area,
there were many advantages to using traditional and conventional care. With regard
to traditional care, participants turned to these methods because they were part of a
588 A.T. Rogers
Dow
nloa
ded
by [
Nor
thea
ster
n U
nive
rsity
] at
15:
39 1
6 D
ecem
ber
2014

long cultural tradition, were familiar with these methods, had knowledge about how
to use them, and were comfortable using them. Traditional methods evoked a sense
of familiarity. Quotes from participants exemplify this idea:
And [the methods have] just been passed on, so a lot of traditional things are just passedon down through the families.
I just think from your tradition it is . . . it’s what you’ve been raised with. It’s part of yourculture for healthcare.
Participants also believed that traditional methods are safer and more effective than
conventional methods. Many participants talked about traditional methods offering
relief without dangerous side effects and working much better or faster than
conventional methods. For example, one participant who suffered from chronic
headaches talked about how conventional medications did nothing to relieve the
pain. Indeed, she talked about how medications could damage the body. She went on
to state that traditional methods
. . . do not harm us as much as [conventional] medicines do. Even though the perceptionof [conventional] medicine is that it’s perfect, it also has some bad things that can affectone. It heals the pain, but for example it damages the liver and things like that. So yes,I have resorted to regular medicine, but only if there is no other possibility. I try to gofirst for the things that do not harm us as much.
Table 2. Qualitative responses about beliefs.
TPB belief areas Traditional health care Conventional health care
Behavioral beliefs Advantages Disadvantages Advantages Disadvantages
Knowledge
and tradition
of methods
Methods don’t
always work,
particularly with
severe illness
Methods are
superior
Methods cause
problems and
prolong suffering
Methods are
effective
Methods can be
accessed
quickly
Trust and faith
in methods
Trust and faith
in methods
Normative beliefs Approve Disapprove Approve Disapprove
Family Nobody Family Nobody
Community
Control beliefs Enabling
factors
Non-enabling
factors
Enabling
factors
Non-enabling
factors
Methods are
accessible and
affordable
Methods
sometimes are not
accessible or
affordable
Methods
sometimes are
accessible and
affordable
Methods are not
accessible or
affordable
Ethnicity & Health 589
Dow
nloa
ded
by [
Nor
thea
ster
n U
nive
rsity
] at
15:
39 1
6 D
ecem
ber
2014

Another participant stated that traditional methods ‘are more comfortable and less
dangerous because they don’t poison. And [conventional] medicine � if you take too
much, it poisons you.’
Related to cultural tradition and beliefs in effectiveness, participants also
expressed a great deal of faith in traditional methods. Participants trusted these
methods because they had been established and they were simple, pure, and not
fabricated. Talking about traditional methods, one participant stated:
The advantages are that the plants are more original than medicine because there aremany medicines that are very harmful to some people because we all have differentbodies.
Many participants also talked about the advantages to using conventional methods
of care. One theme that emerged was that conventional methods are superior to
traditional methods with regard to the science behind them and the advances in
knowledge and technology that have taken place in recent decades. Participants often
referred to this superiority in relation to how conventional methods were better at
curing ‘serious’ illness and diagnosing problems more effectively. For example,
several participants stated:
When it’s a serious or advanced condition, there is no natural medicine, no acupuncture,no homeopathic therapy that solves it. Traditional medicine is not a magical cure.
The advantage of using [conventional] methods, when curing something, is thetechnology � it finds and detects your illness. For example, if it is an infection orcancer . . ., and if you receive treatment in time, it can save you. That is one of thegreatest advantages that modern medicine has . . . that it can quickly detect your illnessand save you from a grave illness.
But now everything is advanced, and there are things that are really good and haveserved to make us well, to cure us. In these advanced days, we don’t use [traditionalmethods] because now there are other things more advanced that we know of � pills,medicines are better, no?
Participants also believed that conventional methods allowed for people to get care
more quickly, leading to faster cures of diseases. For example, one participant stated:
It’s important to go to the doctor. You can get more ill and then pass the time that youshould be at the doctor’s so they can give you the medicine you need.
Participants expressed trust in conventional care providers. Participants had faith in
the way that conventional care providers often offered direct advice such as writing
out directions for medications and care plans. For example, two participants stated:
Well the truth is when they examine you, you feel that everything is better. Thateverything is okay.
Here the doctors tell you what you should be eating. That’s to say, pure, healthythings . . .
According to participants, the main disadvantage to using traditional methods was
related to the idea that traditional methods were not as effective as conventional
590 A.T. Rogers
Dow
nloa
ded
by [
Nor
thea
ster
n U
nive
rsity
] at
15:
39 1
6 D
ecem
ber
2014

methods in diagnosing and curing serious illnesses. Many participants also expressed
beliefs that traditional methods are not always effective in relieving symptoms even
in cases of mild illness. However, one theme that emerged with regard to
disadvantages of conventional methods was that these methods often cause
problems and prolong suffering, such as the example given earlier about how
medications can sometimes damage the body. Other examples of these beliefs are as
follows:
If I am very ill they should give me something for the pain yes, but they should not putme on machines, no, those things no. I don’t want that. Prolonging life no.
[The doctors] leave [children] too long in the hospitals. The children suffer so much inthe hospitals. That’s why I never visit the hospitals because they give me so much pain.I feel the pain in my person.
With drugs, they give you your medicine to cure one illness, and it leads to anotherillness.
Normative beliefs
We also examined participants’ beliefs about how others perceived participants’ use
of traditional and conventional care. Several themes emerged in this belief area. The
main theme that emerged with regard to others disapproving of participants’ use of
traditional and conventional methods was that participants believed that no one �not family, friends, church leaders, or community members � disapproved of use of
either type of care.
However, several themes emerged with regard to participants’ beliefs about the
approval of others regarding the use of traditional and conventional methods of care.
Participants believed that family and community groups with whom participants
associate approved of participants’ use of traditional methods. For example, various
participants stated:
A lot of the community groups that I hang out with, they would approve of thetraditional.
I use all the sage and stuff, but my friends are always trying to get me to go to sweatlodges.
We are from Mexico, and yes, people still have that belief. Yes, they have it. People fromMexico, yes, they believe.
My son [believes] the more natural the better and he is an adult now too.
With regard to the use of conventional methods, the theme of family members
emerged as an important group approving of this type of care. Participants talked
about family members, particularly children, growing up in a community
where conventional methods were the norm and readily available, so children were
especially likely to put pressure on the older participants to use conventional care.
For example:
Well family, they were born in a place where it was easier for one to go to a doctor andget cured.
Ethnicity & Health 591
Dow
nloa
ded
by [
Nor
thea
ster
n U
nive
rsity
] at
15:
39 1
6 D
ecem
ber
2014

My daughter-in-law . . . she always thinks I should go to the doctor for certain thingsthat I don’t think I should.
My daughters all say, ‘mom, go to the doctor.’ They ask me ‘why haven’t you gone to thedoctor?’
Control beliefs
Finally, we examined participants’ beliefs about factors that might hinder orfacilitate their use of traditional and conventional care. Several themes emerged in
this belief area, all of which related to access and cost. Participants perceived that
traditional methods were largely accessible and affordable, while conventional
methods largely inaccessible and unaffordable. With regard to traditional methods,
participants believed that these methods were easy to find, easy to use, easy to ‘stock
up on,’ and easily affordable. Examples of these beliefs include:
I know of some people who can get me the herbs that I need.
They are not too expensive. They are always within reach.
It definitely is a lot cheaper. And it’s something that you can do in the comfort of yourhome. The access to the herbal healers or whatever you want to use is good. And I thinkas you get older, you probably have a good supply of them because you stock up.
If you’re going to go to Mexico, or you know someone who is going to Mexico, you say‘hey can you get me this?’ or, if you deal with a pharmaceutical company in Mexico, youcan get a lot of the herbs.
Conversely, participants viewed conventional methods as largely out of reach.
Participants believed that expense, lack of insurance, lack of ‘legal papers,’ language
barriers, and a lack of knowledge of available resources (e.g., transportation and
interpreters) made conventional care inaccessible. Participants described how antici-
pation of not being helped, understood, or respected would be enough to keep them
from seeking conventional care. Two participants described their beliefs in this way:
People don’t have insurance. So they do wait until the last minute, because they can’tafford it. And then if you give them prescriptions, that’s really expensive and a lot ofthem don’t get the prescriptions. So, it’s just out of their reach. It’s not accessible.
I think that some in the medical community are really rude to people who do not speakEnglish and who they feel are low income. People don’t know that they’re going to havesomeone who can consult with them in Spanish.
Well the disadvantage is not knowing the language. Because a lot of times I don’tunderstand or know what they are saying. So for this, yes, it is necessary that theytranslate truthfully � to be able to ask the questions one wants to ask. For instance withmy daughter, whenever I go to the doctor I tell her to go and ask certain questions, buteven like this it is very hard. One feels frighten for not knowing the language. One thinksthings like, I would not be able to answer what I am being asked, or I would not be ableto explain exactly what is it that I am feeling or the symptoms, or even why it is that I amcoming to the hospital. It is very difficult the language barrier that exists, even startingin the registration process at hospitals.
Participants also described beliefs about traditional care being inaccessible at times.
Much of this inaccessibility centered on lack of knowledge of where to find
592 A.T. Rogers
Dow
nloa
ded
by [
Nor
thea
ster
n U
nive
rsity
] at
15:
39 1
6 D
ecem
ber
2014

traditional care or on traditions not being passed down to subsequent generations, so
knowledge of traditional practices is being lost. Some participants even stated that
traditional methods are more expensive than conventional methods. Many partici-
pants expressed problems with finding the exact traditional methods they were used
to finding in Mexico (e.g., names of herbs were not translated the same; teas were
made differently). Two participants stated:
It’s impossible to use traditional if you haven’t access to some of the oils or ingredientsyou need for a salve or for a paste or something. Or as tradition . . . people aren’tcarrying on the traditions. I think there’s less and less people that are caring about thetraditional. So I think that a lot of people growing up don’t know much about this asthey did in the past. I don’t think it’s because conventional is so accessible, I just don’tthink people . . . it was passed on in the families like the Curandera passing on toanother . . . or somebody taking up [the practice]. . . I think every household might havesomeone that does a little bit with the herbs. But I don’t think it’s as prevalent as it usedto be.
One of the disadvantages in the United States is that they change the names. The people,in this case Hispanics, know them by one name. But here sometimes they have othernames. For example zabila here is called ‘aloe vera.’ The manzanilla tea here is called‘chamomile.’
Other participants described conventional methods sometimes being accessible and
affordable. Participants talked about having insurance, family members who could
help with finding resources, or knowing how to access resources, such as free care,
medications, transportation, interpreters, or other programs that can help pay for
care. Participants described their beliefs in these ways:
There is good help for all of us people who do not have a lot of money for a gooddoctor. The advantage is that there are programs, they help a lot.
I call a driver and the driver takes me . . . and he returns to pick me up. He takes me backhome.
Here we see social workers, and they give us an application to fill out and they don’tcharge us. And she herself takes us to the office where we can get emergency medicalservice. We didn’t have insurance or money so my wife stopped taking her diabetesmedicine. But what we didn’t know was that we were ignorant, we didn’t have money formedical insurance. We didn’t know that here, in two or three months, they would give usmedical assistance up to a certain point if it was an emergency.
Acculturation
According to participants’ responses on the BAS, most (90.3%) participants adhered
to Hispanic culture. Two (6.5%) participants adhered to non-Hispanic culture and
one (3.2%) scored as bi-cultural. An analysis of these three cases with regard to their
responses on qualitative questions suggested that they did not differ from the other
participants on their beliefs. However, responses from these three participants did
indicate that they held more cautious views on both traditional and conventional
methods of care; they expressed more directly the pros and cons of both methods of
care, but their beliefs were still congruent with those of other participants. These
three participants also seemed to be more knowledgeable about resources that
allowed them access to both types of care.
Ethnicity & Health 593
Dow
nloa
ded
by [
Nor
thea
ster
n U
nive
rsity
] at
15:
39 1
6 D
ecem
ber
2014

Discussion
This study expands on and enhances prior research on health disparities in several
ways. First, it offers insights into the health beliefs of older Mexicans and Mexican-
Americans, which according to the TPB, can help to predict healthcare-seeking
behaviors. A better understanding of beliefs and behaviors can inform the
development of services that are more culturally appropriate and congruent with
the needs of the older adults they serve, thereby helping to reduce health disparities.
Second, because the TPB is useful for predicting health-related behaviors, this
study provides a foundation on which additional research can be conducted to fully
explore and better understand issues driving healthcare disparities for older
Mexicans and Mexican-Americans. Predictive models focused on how healthcare
beliefs impact behaviors can offer insights into how services can be developed to
improve health outcomes. Related to this, the methods utilized in this study can be
easily replicated and generalized to other populations to provide a more systematic
comprehensive approach to investigation on health disparities.
Using health beliefs to improve service provision
People’s perceptions of health and illness and the ways in which these perceptions
interact with cultural context impact the ways in which people think about, access,
and utilize care (Rogers and Gallegos 2007, Felicity 2010, van Andel and Westers
2010, Waldstein 2010). However, a great deal of the research on health disparities has
been fragmented, focusing on just a few of the factors or barriers thought to be
related to disparities, excluding the context in which these factors exist. Further,
much of this research focuses mainly on assumed barriers � not on what people
actually perceive as barriers. For example, much attention has been given to the role
of health literacy as it relates to health disparities; this is an assumed barrier to care.
Indeed, health literacy, or the extent to which people are able to understand health
information and make health decisions based on that information (U.S. Department
of Health and Human Services 2000), is a particularly pressing problem among the
elderly (because of physical and cognitive ailments) and individuals with English
proficiency limitations (Beers et al. 2003, U.S. Department of Health and Human
Services 2004). While low health literacy contributes to health disparities, prior work
has primarily looked at health disparities from the perspective of a westernized belief
and healthcare system such as how health literacy (as it is narrowly defined) among
certain populations can be improved and how access to care can be facilitated.
However, a limited conceptualization of health behaviors is at risk of failing to
capture the complexity of individual thought processes within social contexts that
influence how individuals receive and process health-related communication (e.g.,
Helman 1994, Kaiser Family Foundation 2005a).While steps have been taken to improve health services (e.g., focusing on health
literacy issues), these efforts have not been successful in eliminating health
disparities; they have taken us a step further in advancing our understanding of
the causes of health disparities and how to make meaningful change in patient and
provider behaviors and communication patterns that lead to health equality, but
there is much more work to be done (Smedley et al. 2003, Kaiser Family Foundation
2005b). Much of these efforts have been focused on specific strategies that are
594 A.T. Rogers
Dow
nloa
ded
by [
Nor
thea
ster
n U
nive
rsity
] at
15:
39 1
6 D
ecem
ber
2014

applied after patients have accessed care, mostly in an attempt to improve patients’
compliance with westernized conventional care. However, these efforts neither have
considered patients’ health beliefs nor have they been couched in patients’ cultural
contexts. For example, responses from participants in this study reflected a need for a
better connection with the healthcare community (e.g., knowing that resources exist,
trusting that they would be met with respect and understanding should they access
care) � not a need for more clarification of technical healthcare jargon. Further,participants’ responses indicated that beliefs about illness and whether or not family
members would support care-seeking behaviors were influential on whether or not
participants would attempt to access conventional care. Understanding the nature of
these beliefs and their impact on care-seeking behaviors could contribute a great deal
to our understanding and implementation of healthcare improvement efforts such as
literacy campaigns (e.g., perhaps efforts are wasted if they are used in care facilities
that people won’t access in the first place).
These implications have been articulated in both national and international
studies examining healthcare beliefs and utilization among various immigrant groups.
For example, studies of immigrant groups from low-income countries in Spain and
Belgium suggest that immigrants’ perceptions that health-related services and
resources do not exist create significant barriers with regard to healthcare access.
Investing in efforts to increase culturally sensitive, community-based education
campaigns may assist to change these perceptions and offer immigrants concrete
information about available services and how to access them (Rue et al. 2008,Manirankunda et al. 2009). Additionally, studies examining the effects of immigrant
patient�care provider relationships on immigrants’ healthcare service utilization in
the Netherlands and Israel suggest that limited awareness of immigrant patients’
cultural beliefs and practices on the part of care providers hinders immigrants’ use of
services. Specifically, limited cultural awareness can lead care providers to make
assumptions about immigrant patients’ level of acculturation, knowledge of
resources, adherence to different beliefs systems around illness and wellness, and
willingness to comply with treatment protocols; these assumptions not only can
impact the care immigrants receive (or do not receive), but they can damage the trust
in the patient�care provider relationship. Thus, increasing care providers’ awareness
around immigrant populations’ health-related beliefs, traditions, and practices could
greatly facilitate patient�care provider relationships that are more responsive to
immigrants’ healthcare needs (Benyamini et al. 2008, Harmsen et al. 2008).
Taking patients’ beliefs into consideration often means deconstructing thinking
about westernized care. For example, a few cities in Mexico and the USA have
established traditional medicine clinics alongside conventional hospitals. Thisapproach allows patients to decide when, where, and in what context they will
access care, depending on their particular beliefs about their situation. Participants
in our study indicated that they would likely pursue traditional methods in cases
where they did not perceive their health situation to be serious. So, with this service
configuration, an older adult suffering from pre-diabetic symptoms could access
traditional care; if and when her illness is perceived to be more serious, she could
access conventional services next door, where she could enjoy a continuity of service
and trust that is congruent with her beliefs. Ideas such as these that are based in
patients’ cultural beliefs can lead to greater healthcare utilization, decreasing the
health disparities for the groups who utilize them. Ultimately, looking at beliefs from
Ethnicity & Health 595
Dow
nloa
ded
by [
Nor
thea
ster
n U
nive
rsity
] at
15:
39 1
6 D
ecem
ber
2014

the patient’s point of view and cultural context might be a more effective approach to
redesigning healthcare environments and means of services. This may be particularly
important for young migrants who age in place in the USA but who continue to hold
beliefs congruent with those from their countries of origin, as was seemingly the casefor participants in this study.
Building a model to predict healthcare behaviors
Several healthcare utilization models exist that can help researchers and healthcare
professionals better understand the complex issues affecting health beliefs and
service use for minority and other populations. These models draw from learning
theory, socio-cognitive perspectives, and other theoretical foundations to helporganize and explain key factors that influence people’s perceptions of health and
illness, intentions to seek care, and systems that impact people’s healthcare use. In
addition to the TPB, other models such as the Self-Regulation Model (Leventhal
et al. 1984), the Health Belief Model (Rosenstock 1966, 1974), Andersen’s (1995)
Sociobehavioral Model, Pescosolido’s (1992) Network Episode Model, and Cramer’s
(1999) Help Seeking Model all attempt to describe the ways in which psychosocial
and cultural factors impact people’s healthcare decision-making and utilization.
While these models contribute to our understanding of healthcare access and use, theTBP pays particular attention to the ways in which beliefs impact people’s intentions
to follow through with certain behaviors; understanding belief systems is critical to
understanding how cultural context impacts people’s actions (Ajzen 1988). Conse-
quently, the TPB can play an important role in better understanding health
disparities among older Mexicans and Mexican-Americans. Using the theory and
its concepts, healthcare-seeking behavioral beliefs, attitudes, norms, and perceived
behavioral controls among this older population can be explored, ultimately
predicting their intentions to act on certain behaviors, in turn predicting their actualhealthcare-seeking behaviors. For example, the salient beliefs or themes identified in
this study can be developed into quantifiable questionnaire items that can measure
the strength of beliefs in each area, which can be tested through advanced statistical
techniques (e.g., structural equation modeling), providing a model through which
health-related behaviors can be predicted (Ajzen 1991, Francis et al. 2004). Given the
complexity of issues underlying people’s healthcare behaviors, it is improbable that
the TBP alone can explain the multitude of factors influencing these behaviors.
However, the TPB does offer a conceptual framework within which other modelscould be incorporated to more comprehensively address the factors involved in
healthcare use. A more comprehensive approach to thinking about healthcare use
may be what is ultimately needed if health disparities are to be reduced. Models such
as these, when combined, can be used to inform the development of improved
healthcare services and generalized to different populations to improve healthcare
access and utilization.
This study has several limitations, particularly with regard to sampling. This
study interviewed participants who were utilizing community services; thus, we donot know anything about the beliefs of people not using services. However,
interviews with this group of participants still yielded rich information about what
people viewed as barriers to healthcare, as many of the participants were not able to
access it even though they were able to access other types of services. Further, while
596 A.T. Rogers
Dow
nloa
ded
by [
Nor
thea
ster
n U
nive
rsity
] at
15:
39 1
6 D
ecem
ber
2014

attempts were made to oversample male participants, we were unable to do so. It may
be that the health beliefs of men and women differ and they have different
experiences in attempting to access care. Thus, future studies should attempt to
explore whether these differences exist.Because cultural context is so important in understanding belief systems, future
studies should attempt within- and between-group comparisons of participants’
beliefs and experiences. While this sample included people from a wide variety of
Mexican states, the sample size of people from each state was small, making
comparisons difficult, and case study analyses for these types of comparisons were
beyond the scope of this paper. Further, while our study included three people who
did not adhere to Hispanic culture, more study is needed to ascertain to what degree
acculturation impacts healthcare beliefs and behaviors. Results from this studysuggested that acculturation might not significantly influence people’s beliefs, but it
may influence people’s level of knowledge (and skepticism) about existing resources
and healthcare systems.
Conclusions
This study explored the health beliefs of older USA-dwelling Mexicans and Mexican-Americans from the context of the TPB (Ajzen 1991) to better understand how
beliefs translate into health-related behaviors. Because health disparities are the
result of a complex interaction of cultural, socioeconomic, and other variables, the
results of this study offer insights into how beliefs contribute to health-related
outcomes. Results of this study also provide a foundation for future research that
better predicts health-related behaviors, leading to the development of more
accessible, effective, and culturally competent approaches to health services that
will reduce health disparities for underserved populations.
Acknowledgements
This work was supported by a grant from the Hartford Foundation. The author wishes tothank Dr. Peter Maramaldi for his mentorship on the project, the Hartford Foundation whofunded this project, the interviewers (Jeannie Toscano and Denise Garcia), research assistants(Ben Welch and Jo Corder), and community members, including Dr Joseph Gallegos, whoprovided feedback on various portions of the project.
References
Ajzen, I., 1988. Attitudes, personality, and behavior. Chicago, IL: The Dorsey Press.Ajzen, I., 1991. The theory of planned behavior. Organizational Behavior and Human Decision
Processes, 50, 179�211.Ajzen, I. and Fishbein, M., 1980. Understanding attitudes and predicting social behavior.
Englewood Cliffs, NJ: Prentice Hall.Ajzen, I. and Fishbein, M., 2000. Attitudes and the attitude�behavior relation: reasoned and
automatic processes. In: W. Stroebe and M. Hewstone, eds. European review of socialpsychology, 11, 1�33.
Andersen, R.M., 1995. Revising the behavioral model and access to medical care: does itmatter? Journal of Health and Social Behavior, 36, 1�10.
Beers, B.B., et al., 2003. Disparities in health literacy between African American and non-African-American primary care patients. Journal of General Medicine, 18 (Suppl. 1), 169.
Benner, P., 1994. Interpretive phenomenology. Thousand Oaks, CA: Sage.
Ethnicity & Health 597
Dow
nloa
ded
by [
Nor
thea
ster
n U
nive
rsity
] at
15:
39 1
6 D
ecem
ber
2014

Benyamini, Y., et al., 2008. Cultural and educational disparities in the use of primary andpreventive health care services among midlife women in Israel. Women’s Health Issues, 18(4), 257�266.
Bureau of the Census, 2000. Age of the U.S. population: 2000 [online]. Available from: http://www.census.gov/mso/www/rsf/hisorig/sld033.htm [Accessed 21 September 2006].
Chang, A., Chau, J., and Holroyd, E., 1999. Translation of questionnaires and issues ofequivalence. Journal of Advanced Nursing, 29 (2), 316�322.
Cramer, K.M., 1999. Psychological antecedents to help-seeking behavior: a reanalysis usingpath modeling structures. Journal of Counseling Psychology, 46, 381�387.
Creswell, J., 1998. Qualitative inquiry and research design. Thousand Oaks, CA: Sage.Creswell, J., 2003. Research design: qualitative, quantitative, and mixed methods approaches. 2nd
ed. Thousand Oaks, CA: Sage.Felicity, T., 2010. Transnational health and treatment networks: meaning, value, and place in
health seeking amongst southern African migrants in London. Health and Place, 16, 606�612.
Fishbein, M. and Ajzen, I., 1975. Belief, attitude, intention, and behavior: an introduction totheory and research. Reading, MA: Addison-Wesley.
Francis, J.J., et al., 2004. Constructing questionnaires based on the theory of planned behavior: amanual for health services researchers. Newcastle-upon-Tyne: Centre for Health ServicesResearch, University of Newcastle.
Godin, G. and Kok, G., 1996. The theory of planned behavior: a review of its applications tohealth-related behaviours. American Journal of Health Promotion, 11 (2), 87�98.
Guillemin, F., Bombardier, C., and Beaton, D., 1993. Cross-cultural adaptation of health-related quality of life measures: literature review and proposed guidelines. Journal of ClinicalEpidemiology, 46 (12), 1417�1432.
Harmsen, J.A.M., et al., 2008. Patients’ evaluation of quality of care in general practice: whatare the cultural and linguistic barriers? Patient Education and Counseling, 72, 155�162.
Helman, C., 1994. Culture, health, and illness. London: Wright.Kaiser Family Foundation, 2005a. Inaugural health education research disparities summit:
health disparities and social inequities. Plenary II � framing solutions for the elimination ofhealth disparities, 8 August [online]. Available from http://www.kaisernetwork.org/health_-cast/hcast_index.cfm?display=detail&hc=1477 [Accessed 1 September 2005].
Kaiser Family Foundation, 2005b. Inaugural health education research disparities summit:health disparities and social inequities. Plenary IV: methodological approaches todissemination in health education: using community-based participatory research and thesocial ecological framework, 9 August [online]. Available from http://www.kaisernetwor-k.org/health_cast/hcast_index.cfm?display=detail&hc=1477 [Accessed 1 September 2005].
Leventhal, H., Nerenz, D.R., and Steele, D.F., 1984. Illness representations and coping withhealth threats. In: A. Baum and J. Singer, eds. A handbook of psychology and healthHillsdale, NJ: Lawrence Erlbaum Associates, 219�252.
Maneesriwongul, W. and Dixon, J.K., 2004. Instrument translation process: a methods review.Journal of Advanced Nursing, 48 (2), 175�186.
Manirankunda, L., et al., 2009. ‘It’s better not to know’: perceived barriers ti HIV voluntarycounseling and testing among sub-Saharan African migrants in Belgium. AIDS Educationand Prevention, 21 (6), 582�593.
Marın, G. and Gamba, R.J., 1996. A new measure of acculturation for Hispanics: theBidimensional Acculturation Scale for Hispanics (BAS). Hispanic Journal of BehavioralSciences, 18 (3), 297�316.
Marın, G. and Marın, B.V., 1991. Research with Hispanic populations. London: Sage.Miles, M. and Huberman, A.M., 1994. Qualitative data analysis: an expanded sourcebook.
Thousand Oaks, CA: Sage.Morse, J.M., 1994. Designing funded qualitative research. In: N.K. Denzin and Y.S. Lincoln,
eds. Handbook of qualitative research. Thousand Oaks, CA: Sage, 220�235.National Academies Press, 2002. Speaking of health: assessing health communication strategies
for diverse populations. Committee on Communication for Behavior Change in the 21stCentury: improving the health of diverse populations, Board on Neuroscience andBehavioral Health. Washington, DC: National Academies Press.
598 A.T. Rogers
Dow
nloa
ded
by [
Nor
thea
ster
n U
nive
rsity
] at
15:
39 1
6 D
ecem
ber
2014

National Academies Press, 2003. New horizons in health: an integrative approach. Committeeon future directions for behavioral and social sciences research at the national institutes ofhealth. Commission on behavioral and social sciences and education national researchcouncil. Washington, DC: National Academy Press.
National Institutes of Health, 2000. Addressing health disparities: the NIH program of action[online]. Available from: http://healthdisparities.nih.gov/whatare.html [Accessed 21 September2006].
Nielsen-Bohlman, L., Panzer, A.M., and Kindig, D.A., eds., 2004. Health literacy: aprescription to end confusion. Institutes of Medicine of the National Academies.Washington, DC: The National Academies Press.
Pescosolido, B.A., 1992. Beyond rational choice: the social dynamics of how people seek help.The American Journal of Sociology, 97, 1096�1138.
Rogers, A. and Gallegos, J., 2007. Pathways to health and mental health service utilizationamong older Mexicans and Mexican Americans. International Social Work, 50 (5), 654�670.
Rosenstock, I.M., 1966. Why people use health services. Milbank Quarterly, 44, 94�106.Rosenstock, I.M., 1974. Historical origins of the health belief model. Health Education
Monograph, 2, 328�335.Rue, M., et al., 2008. Emergency hospital services utilization in Lleida (Spain): A cross-
sectional study of immigrant and Spanish-born populations. BMC Health ServicesResearch, 8, 81�88.
Ryan, G.W. and Bernard, R., 2003. Data management and analysis methods. In: N.K. Denzinand Y.S. Lincoln, eds. Collecting and interpreting qualitative materials. Thousand Oaks, CA:Sage, 259�309.
Skaff, M.M., et al., 2002. Lessons in cultural competence: adapting research methodology forLatino participants. Journal of Community Psychology, 30 (3), 305�323.
Smedley, B.S., Stith, A.Y., and Nelson, A.R., eds., 2003. Unequal treatment: confronting racialand ethnic disparities in health care. Washington, DC: National Academy Press.
U.S. Department of Health and Human Services, 2000. Healthy people 2010 [online]. Availablefrom: http://www.health.gov/healthypeople/ [Accessed 4 September 2005].
U.S. Department of Health and Human Services, 2004. Literacy and health outcomes summary.Washington, DC: U.S. Department of Health and Human Services, Agency for HealthcareResearch and Quality.
van Andel, T. and Westers, P., 2010. Why Surinamese migrants in the Netherlands continue touse medicinal herbs from their home country. Journal of Ethnopharmacology, 127, 694�701.
Waldstein, A., 2010. Popular medicine and self-care in a Mexican migrant community: towardan explanation of an epidemiological paradox. Medical Anthropology, 29 (1), 71�107.
Ethnicity & Health 599
Dow
nloa
ded
by [
Nor
thea
ster
n U
nive
rsity
] at
15:
39 1
6 D
ecem
ber
2014


![Losers [anyone buying with pesos] 1. Mexicans who buy American products 2. Mexican businesses that buy supplies from the U.S. 3. American businesses that](https://img.pdfslide.us/doc/110x75/5516359d550346b2068b4e85/losers-anyone-buying-with-pesos-1-mexicans-who-buy-american-products-2-mexican-businesses-that-buy-supplies-from-the-us-3-american-businesses-that.jpg)