Embed Size (px)
Citation preview

University of Colorado, BoulderCU Scholar
Undergraduate Honors Theses Honors Program
Spring 2016
Exploring a possible correlation between thehuman oral microbiome and body mass indexIvy S. [email protected]
Follow this and additional works at: http://scholar.colorado.edu/honr_theses
Part of the Biodiversity Commons, Computational Biology Commons, and the Other PublicHealth Commons
This Thesis is brought to you for free and open access by Honors Program at CU Scholar. It has been accepted for inclusion in Undergraduate HonorsTheses by an authorized administrator of CU Scholar. For more information, please contact [email protected].
Recommended CitationMcDermott, Ivy S., "Exploring a possible correlation between the human oral microbiome and body mass index" (2016).Undergraduate Honors Theses. Paper 1187.

Exploring a possible correlation between the
human oral microbiome and body mass
index
By
Ivy McDermott
Department of Molecular, Cellular, and Developmental Biology
University of Colorado at Boulder
Defense date: March 28, 2016
Thesis Advisor:
Dr. Kenneth Krauter, Department of Molecular, Cellular, and Developmental Biology
Defense Committee:
Dr. Kevin Jones, Department of Molecular, Cellular, and Developmental Biology
Dr. Noah Fierer, Department of Ecology and Evolutionary Biology

2
Table of Contents
Abstract……………………………………………………………………………………....3
Introduction………………………………………………………………………………......4-5
Significance…………………………………………………………………………………..5-6
Materials and Methods………………………………………………………………....…….6-8
Results………………………………………………………………………………………..9-14
Discussion……………………………………………………………………………………15-16
Acknowledgements…………………………………………………………………………..16
References…………………………………………………………………………................17-21
Appendix I................................................................................................................................22-23

3
Abstract:
Obesity is a growing health problem in America affecting more than a third of
Americans25 and is quickly becoming a global health crisis34. Recently there has been much
interest in the possible link between the human gut microbiome and obesity as fecal transplants
may serve as a potential therapeutic treatment. However, not much research has been done
looking at a potential association with the human oral microbiome and obesity. In this thesis, I
examined 976 individuals previously sequenced for their oral microbiome. Each sample was
classified as underweight, normal, overweight, or obese, according to their BMI. I measured the
microbial diversity of each sample and compared the relative diversity of each class through
alpha and beta diversity. Alpha diversity measures the microbial diversity within an individual
while beta diversity measures the microbial diversity between individuals. I also investigated
whether there was a clear association between monozygotic twins who were discordant in
phenotype. While phyla-level changes were detected in the different weight class, overall the
oral microbiome does not appear to be associated with human weight.

4
Introduction:
The human oral microbiome is composed of a diverse community of microorganisms
which is comprised of a core set of bacterial genera that are commonly shared among
individuals12,18,23. Bacteria accumulate in biofilms on various surfaces such as teeth and soft
tissues like the gums5,6,23. The oral microbiome also exhibits long-term stability18 though this
stability may be altered or influenced by a variety of factors including the environment of the
host such as tooth loss as well as external factors like smoking and oral hygiene. Oral diseases,
such as periodontitis and dental caries2,19,22,24, as well as other diseases such as diabetes14,24 and
cancer 24have been associated with the oral microbiome. Currently there is much interest in the
association between human weight and the gut microbiome, however, the role of the human oral
microbiome and human weight is not well understood.
The association of the human gut microbiota and obesity has been the focus of intense
investigation recently. Studies have characterized the composition and diversity of humans and
mice exhibiting lean and obese phenotypes20,7. These studies have shown that obese individuals
exhibit phyla-level changes in their gut microbiome as well as a decrease of microbial
diversity7,13,21. Many papers have focused on the ratio of Firmicutes to Bacteroidetes in obese
and lean individuals with obese individuals displaying higher levels of Firmicutes and lower
levels of Bacteroidetes13,21,30,33,36. Other papers have contested these results7,35. Fecal transplant
experiments in mice also demonstrate a link between the gut microbiome and obesity21.
The oral microbiome may serve as a biomarker for diseases related to the gut such as
irritable bowel syndrome12,28 which suggests that the two microbiomes are correlated. Previous
research has shown that both the human oral and gut microbiomes were correlated to biomarkers
of atherosclerosis14 and the oral microbiome has been linked to irritable bowel syndrome26. The

5
mouth is also a “gateway” to the rest of the body. Bacteria that accumulate on the different
intraoral tissues slough off into the saliva. The microorganisms in the saliva may also move
along contiguous epithelial surfaces within the mouth and into the gut.
Significance
Understanding the role of the microbiome in human health and disease is crucial for the
development of disease diagnostics, therapeutics, and potentially personalized medicine24,32. The
oral microbiome has been implicated in oral and systemic diseases as particularly severe forms
of oral diseases may cause systemic diseases2,5,22,24. Periodontitis has been positively correlated
with both diabetes and cardiovascular disease (CVD) suggesting that the oral microbiome may
also be related to these systemic diseases5,14,24. Since obesity has been linked to diabetes and
CVD the oral microbiome may also be associated with weight15,16. It has been previously
suggested that oral bacteria may be related to the pathology of obesity8, however this finding has
been contested in other papers3.
I investigated a possible correlation between the human oral microbiome and body mass
index (BMI). I chose to use BMI because weight alone is not an adequate measurement of
obesity since BMI also factors in an individual’s height. This research holds the promise that if
successful, the oral microbiome may prove a useful surrogate to studies of the gut microbiome
that are more complicated to carry out. My plan was to investigate the microbial diversity in
relation to four BMI phenotypes: underweight, normal, overweight, and obese. I intended to look
at this correlation in all samples with height and weight data available, controlling for age and
genetics. I also wanted to examine discordant twin pairs as well as twins whose phenotype

6
changed over two time points. I was able to analyze the first group as well as the discordant
monozygotic twins, but I did not have time to investigate the other twin groups.
Materials and Methods:
Samples
Saliva samples were received from the Center of Antisocial Drug Dependence as well as
the Colorado Twin Registry. DNA from samples was isolated in the laboratory as described
previously42.
Sequencing of Bacteria
The V4 region of the bacterial 16S small ribosomal subunit rDNA was sequenced via
Illumina MiSeq as previously described4. The 16S rDNA region has constant and variable
regions that can be sequenced to determine OTUs present in each sample. Samples were
prepared in triplicate and amplified via Polymerase Chain Reaction (PCR) with barcoded primers
to amplify the 16S region of rDNA. Primers were designed as previously described1. The
triplicates were pooled together after PCR to limit variation due to technique such as pipetting
error and PCR machine variability. The samples were then run on a 2% e-gel for 20 minutes to
verify that samples were amplified. PCR products were quantified using a picogreen assay
according to manufacturer’s instructions. The PCR products from each barcoded subject were
pooled in equimolar amounts (240ng/sample) by a graduate student, Brittany Demmitt,
according to the Earth Microbiome1 protocol and then sent to the CU DNA Sequencing facility
for sequencing on an Illumina MiSeq instrument.

7
Sample Selection
Data sets were assembled using RStudio (Version 0.99.441). The body mass index (BMI)
was calculated according to a formula provided by the CDC as the weight in pounds divided by
the height in inches multiplied by a constant ([(𝐿𝑏𝑠
𝑖𝑛2) × 703]). and subjects were divided into
obese, underweight, overweight or normal classes according to age-appropriate target BMI15.
Samples collected only via a scope collection method were used (n=2110). I took the complete
set and removed any duplicate family members. In other words, I only kept one member of each
family in order to control for genetics. For retention, I prioritized subjects who were classified,
in order, as obese, underweight, overweight, and normal. This left me with 1020 subjects.
Finally, each weight class was manipulated so that the mean age of each group was statistically
similar to each other using a pair-wise t-test (n=976). I considered controlling for sex, but
there’s no evidence that sex influences the oral microbiome18.
While doing this initial investigation, I noticed that there were a large number of
discordant twins. I identified 24 discordant monozygotic twin pairs, meaning they had identical
genomes but differing phenotypes. I chose only pairs where one cotwin was obese and the other
was normal weight. The discordant phenotypes in these twins suggests that a factor other than
genetics may be driving their weight classes. The microbial diversity of these discordant twins
were compared to the microbial diversity of 16 pairs of normal weight concordant monozygotic
cotwins and 16 pairs of obese concordant cotwins. There were considerably more normal
concordant cotwins than obese cotwins, 16 pairs of normal concordant cotwins were randomly
chosen out of the larger set.

8
Statistical Analyses
All statistical analyses were performed in QIIME29 (1.9.1) and RStudio37. The sequences
from the Illumina MiSeq run were categorized into different operational taxonomic units (OTU)
which is a categorization of the microbes based solely on their DNA sequence similarities.
Brittany Demmitt created a table that contained the counts of the OTUs in all samples sequenced.
I matched the sample IDs of the data sets described above to the OTU table in order to find the
frequency of OTUs of each individual. The filtered OTU table was then rarefied to a depth of
2500 reads/sample. OTUs were then filtered for abundance. The OTUs were filtered to those
present in 50% of the respective samples and were present a minimum of 5 times. Alpha
diversity, which measures the microbial diversity within an individual, was performed using a
PD whole tree metric. This metric is based on a phylogenetic tree and uses branch length to
determine diversity39. Beta diversity analysis, a measure of microbial diversity between
individuals, using the Bray-Curtis metrics were used on all data sets. Bray-Curtis quantifies the
compositional diversity between individuals based on OTU counts40. Results were plotted on a
principal component plot via emperor38. A linear regression analysis was performed on the total
sample set (n=976) of the principal components, independent variable, and the weight classes as
well as the raw BMI scores, dependent variable. Other covariates (age, sex, MiSeq run, and
sample collection year) were all controlled for in all regression analyses. An alpha diversity
analysis was performed for both data sets as well, and a comparison of the frequency of different
phyla-level OTUs was performed on each data set.

9
Results
Correlation between weight and the oral microbiome in unrelated individuals
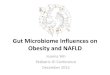
I looked at the alpha diversity of the different weight classes using the PD whole tree
metric. Unlike the results seen in the gut microbiome between lean and obese individuals the
alpha diversity between all phenotypes was similar (Figure 1). This suggests the microbial
diversity between all the weight classes is the same, and there are no significant differences in
the oral microbiome between any of the four phenotypes.
Figure 1: Alpha diversity of all samples
Alpha diversity curve showing the four different weight classes. Alpha diversity was measured using
PD_whole_tree metrics. Red is normal, blue is obese, orange is overweight and green is underweight.
I next performed a beta diversity analysis using the non-tree based Bray-Curtis metrics on
all the unrelated individuals (n=976). Figure 2 represents a 2D plot of the beta diversity analysis
of the first three principal components. No clear clustering of the different weight classes was
observed from beta diversity, suggesting that the oral microbiome is not sufficiently distinct
between obese and lean individuals. However, I noticed that many of the obese samples were

10
near principal coordinate 1 (PC1) which explains about 20% of the variation in the sample and
principal coordinate 2 (PC2) which explains about 8% of the variation in the sample. I then
performed a multivariate linear regression against PC1 and PC2 to see if either of these
components were significantly related to the obese phenotype.
Figure 2: Beta diversity of all unrelated individuals
2D plots of the first three principal components of Bray-Curtis beta diversity analysis. Each point represents an
individual and is plotted in a distance matrix relatively to the diversity of each other. Points are colored by their
respective weight class. Red is normal, blue is obese, orange is overweight, and green is underweight.

11
Linear regression of PC1 and PC2
I performed a linear regression of multiple possible covariates against PC1, PC2 and PC3.
I regressed out the weight classifications using normal weight as the reference phenotype against
other variables (sex, age, MiSeq run, and sample collection year). I also performed a regression
of the principal coordinates for the raw BMI numbers, regressing out the same covariates as
above. For PC1 the beta coefficient of the obese weight class is -0.056 (Table 1) which was
significant (P<0.001). On average individuals of the obese phenotype were 0.056 units below
individual’s of normal phenotype along PC1. When only the raw BMI scores were used I
retained significance (P<0.001). This suggests that the distribution of heavier individuals along
PC1 which explains about 20% of the variation of the population was significantly different
compared to normal weight individuals.
When weight classes were regressed against PC2, the estimate for obese compared to
normal was -0.028 (Table 1) which was also significant (P<0.01). However, when the raw BMI
numbers were regressed against PC2 significance was lost (P>0.1), suggesting that overall
weight did not significantly contribute to plotting along PC2. Both phenotype and BMI scores
were regressed against PC3, but no significance was found (Table 1).

12
PC1 (ß) Coefficient P value
Obese -0.0560 0.0013**
Overweight -0.0200 0.1716 R2=0.0816
Underweight 0.0020 0.9137
BMI -0.0040 0.0011** R2=0.0829
PC2 (ß) Coefficient P value
Obese -0.0284 0.0148*
Overweight -0.0051 0.6052 R2=0.0218
Underweight -0.0039 0.7869
BMI -0.0012 0.1291 R2=0.0201
PC3 (ß) Coefficient P value
Obese 0.0007 0.4510
Overweight -0.0039 0.9420 R2=0.0189
Underweight 0.0037 0.6260
BMI 0.0236 0.3680 R2=0.0213 Table 1: Linear regression analysis of principal components 1 to 3. Weight classifications and raw BMI scores were regressed against principal components 1 through 3. Multiple
covariates were regressed out as well. Weight classes were all baseline to the normal phenotype. ß coefficients are
the average distance of the class as compared to the normal phenotype. *P<0.05, **P<0.01, ***P<-0.001.
Frequency of phyla-level OTUs
I next investigated whether there were any phyla-level changes of OTUs in the different
weight classes of unrelated individuals. The fractional means were obtained via a Kruskal-Wallis
nonparametric test41. While in the gut, the relative abundance of Firmicutes and Bacteroidetes
have often been shown to have a correlation with human weight, in the oral microbiome
Actinobacteria appeared to be significantly less abundant in obese individuals compared to the
other weight classes (Table 2). To ensure that the difference between underweight and obese
individuals was not driving this significance, I next compared only normal and obese individuals
(Table 3). Again, I found that Actinobacteria was significantly less abundant in obese individuals
compared to normal individuals (P <0.001). The relative abundance of Actinobacteria maintains
its significance even with the Bonferroni and FDR corrected p values (Table 2 and 3).

13
Phyla
Test-
Statistic P FDR_P Bonferroni_P obese normal overweight underweight
Actinobacteria 16.67 0.0008*** 0.0041** 0.0041** 0.10 0.12 0.12 0.13
Proteobacteria 5.94 0.1148 0.287 0.574 0.14 0.13 0.12 0.13
Fusobacteria 2.8 0.4232 0.7053 1.000 0.06 0.06 0.06 0.06
Bacteroidetes 0.87 0.8318 0.9301 1.000 0.13 0.13 0.13 0.13
Firmicutes 0.45 0.9301 0.9301 1.000 0.56 0.56 0.56 0.55
Table 2: Relative abundance of different phyla in different weight classes
Table lists five core phyla of the human oral microbiome and their mean fractional abundance in each weight class.
Analysis performed on all unrelated individuals (n=976) A Kruskal-Wallis analysis was done to calculate the p
value. *P<0.5, **P<0.01, ***P<0.001
Table 3: Relative abundance of phyla in normal and obese individuals
Table lists five core phyla of the human oral microbiome and mean fractional abundance. Only individuals classified
as obese or normal were used (n=702). P value calculated from Kruskal-Wallis analysis. *P<0.5, **P<0.01,
***P<0.001
Microbial diversity of discordant monozygotic twins
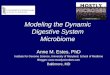
Next I investigated whether the oral microbiome was associated with discordant weight
phenotypes in monozygotic twins. If the oral microbiome plays a role in the discordant
phenotypes, I would expect to see the discordant cotwins plotted more distantly from each other
on a principal coordinate plot, and the concordant cotwins to be closer. I performed a beta
diversity measure on normal weight and obese discordant twins (Figure 3A) in order to visualize
the microbial diversity between twin pairs. The discordant twins generally were plotted with
observable distance between them, however I did not have the time to do the work necessary to
quantify the vectors. They were then compared to concordant normal and concordant obese twin
pairs (Figure 3B-C). Visually, the concordant twins also appear far apart on the principal
component plot indicating that the oral microbiome does not appear to associate with the weight
Phyla Test-Statistic P FDR_P Bonferroni_P obese normal
Actinobacteria 15.65 7.62E-05*** 0.0004 0.0004 0.10 0.12
Proteobacteria 4.58 0.0323* 0.0808 0.1615 0.14 0.13
Fusobacteria 2.12 0.1450 0.2417 0.7251 0.06 0.06
Bacteroidetes 0.64 0.4230 0.5288 1.0000 0.13 0.13
Firmicutes 0.05 0.8306 0.8306 1.0000 0.56 0.56

14
classes in monozygotic twins. Again, due to time the vectors were not quantified, so it is hard to
determine if the discordant twin pairs were significantly more distal to each other than the
concordant twin pairs.
Figure 3: Beta diversity PCoA of discordant and concordant twin pairs Beta diversity was performed using non phylogenetic tree based Bray-Curtis metric. Vectors connect twin pairs to
each other. (A) Discordant twin pairs. Blue indicates obese weight class, red indicates normal weight class. (B)
Concordant normal weight class twin pairs. (C) Concordant obese weight class twin pairs.

15
Discussion
Although there has been plenty of evidence correlating the gut microbiome to human
weight and obesity, the oral microbiome does not appear to have an association with human
weight as has been previously discussed3. Although some oral diseases have been linked to
systemic diseases that are related to obesity, I did not see a clear correlation of oral microbial
diversity and BMI. This may be due to the fact that I did not have information on the oral health
of these individuals, and they were not collected for oral diseases. Drug usage may have also
affected the results as many drugs such as tobacco and alcohol may affect the oral microbiome.
I did find significance in the distribution of the obese weight class and BMI raw numbers
along PC1, indicating that the obese phenotype in this population is clustering around this
principal component that explains most of the variation in the population as a whole. However,
looking at the beta and alpha diversity, the association between the oral microbiome and body
weight ultimately appears unrelated in this population.
Similar to the gut microbiome, phyla-level changes were observed in the different weight
classes. It has been previously proposed that higher levels of Actinobacteria20 in the gut
microbiome is associated with obesity. However, in the oral microbiome, obesity was related to a
decrease in the total fractional mean of Actinobacteria compared to all other phenotypes and the
normal phenotype. Actinobacteria is one of the core phylum of the oral microbiome, but whether
one species of bacteria from this phyla may act as a marker remains unknown. It has also been
previously found that the presence of Selenomonas noxia in the oral microbiome was linked to
overweight women8. The selenomonas genus was not present in this data set, so I could not look
at it as a biomarker.

16
The results of the monozygotic twins remain unclear though the oral microbiome does
not appear to be related to the discordant phenotype in twin pairs. Qualitatively, the beta
diversity of the coordinate and discordant twin pairs appear similar. However, quantitatively it is
unknown whether any differences are observed between the different twin groups.
While I believe my results do not show a clear correlation between the human oral
microbiome and BMI, the correlation between the obese phenotype and PC1 as well as the
phyla-level changes detected in the obese weight class are promising. A larger and better-defined
sample would clarify this. Considering the possible link between periodontitis and other systemic
diseases correlated to obesity, this sample population may not have revealed a clear correlation
due to the lack of medical information available. These samples were not collected for
periodontitis or other diseases that have a link to obesity. Further studies that control for the
potential link between oral diseases and other systemic diseases may reveal an association with
the oral microbiome and human weight.
Acknowledgements
I would like to sincerely thank my thesis advisor, Dr. Kenneth Krauter, for mentoring
during my undergraduate career and for guiding me on this thesis project. I would also like to
extend my gratitude to the other members of my thesis committee, Dr. Kevin Jones and Dr. Noah
Fierer, for volunteering their time to participate in my thesis defense. I appreciate your time and
commitment to be on my committee. And for her help and support, I would like to thank
graduate student Brittany Demmitt for guiding me in this project and providing support and
mentorship. Thank you all so much.

17
References
1) “16S rRNA Amplification Protocol.” Earth Microbiome Project. 2011. Web. 14 August
2014.
2) Amerongen Nieuw AV, Veerman ECI Saliva—the defender of the oral cavity. Oral
Diseases. 8: 12-22 (2002).
3) Belstrøm D et al. Bacterial profiles of saliva in relation to diet, lifestyle factors, and
socioeconomic status. Journal of Oral Microbiology. 6: doi:10.3402/jom.v6.23609
(2012).
4) Caporaso JG et al. Ultra-high-throughput microbial community analysis on Illumina
HiSeq and MiSeq platforms. The ISME Journal. 6:1621-1624 (2012).
5) Cho I, Blaser MJ. The human microbiome: at the interface of health and disease. Nature
Reviews. 13: 260-270 (2012).
6) Dewhirst FE et al. The Human Oral Microbiome. Journal of Bacteriology. 192(19):
5002-50017. doi:10.1128/JB.00542-10 (2010).
7) Finucane MM, Sharpton TJ, Laurent TJ, Pollard KS. A Taxonomic Signature of Obesity
in the Microbiome? Getting to the Guts of the Matter. PLoS ONE 9(1): e84689.
doi:10.1371/journal.pone.0084689 (2014).
8) Goodson JM, Groppo D, Halem S, Carpino E. Is obesity an oral bacterial disease? J Dent
Res 88(6):519-523(2009).
9) Hamady M, Knight R. Microbial community profiling for human microbiome projects:
Tools, techniques, and challenges. Genome Research. 19: 1141-1152 (2009).
10) Hildebrandt MA et al. High-Fat Diet Determines the Composition of the Murine Gut
Microbiome Independently of Obesity. Gastroenterology. 137: 1716-1724 (2009).

18
11) Hubert HB, Feinleib M, McNamara PM and Castelli WP. Obesity as an Independent Risk
Factor for Cardiovascular Disease: A 26-year Follow-up of Participants in the
Framingham Heart Study. Circulation. 67: 968-977.
ttp://circ.ahajournals.org/content/67/5/968. (1983).
12) The Human Microbiome Project Consortium. Structure, function and diversity of the
healthy human microbiome. Nature. doi:10.1038/nature11234 (2012).
13) Ignacio A, Fernandes MR, Rodrigues VAA, Groppo FC, Cardoso AL, Avila- Campos MJ,
Nakano V, Correlation between body mass index and fecal microbiota from children,
Clinical Microbiology and Infection. doi: 10.1016/j.cmi.2015.10.031 (2015).
14) Koren O et al. Human oral, gut, and plaque microbiota in patients with atherosclerosis.
PNAS. www.pnas.org/cgi/doi/10.1073/pnas.1011383107 (2011).
15) Kuczmarski RJ et al. CDC growth charts for the United States: Methods and
development. National Center for Health Statistics. Vital Health Stat 11(246) (2000).
16) Leong KS, Wilding JP. Obesity and diabetes. Bailliére’s Clinical Endocrinology and
Metabolism. 13(2): 221-237 (1999).
17) Lois K, Kumar S. Obesity and diabetes. Endocrinol Nutr. 56(Supl4): 38-42 (2009).
18) Stahringer SS et al. Nurture trumps nature in longitudinal survey of bacterial
communities in twins from early adolescence to early adulthood. Genome Research.
22:2146-2152 (2012).
19) Takeshita T et al. Bacterial diversity in saliva and oral health-related conditions: the
Hisayama Study. Scientific Reports. doi:10.1038/srep22164 (2016).
20) Turnbaugh PJ et al. A core gut microbiome in obese and lean twins. Nature.
doi:10.1038/nature07540 (2009).

19
21) Turnbaugh PJ, Ley RE, Mahowald MA, Magrini V, Mardis ER, Gordon JI. An obesity-
associated gut microbiome with increased capacity for energy harvest. Nature.
doi:10.1038/nature05414 (2006).
22) Weidlich P, Cimões R, Pannuti CM, Oppermann RV. Association between periodontal
diseases and systemic diseases. Braz Oral Res. (Spec Iss 1): 32-43 (2008).
23) Xu X et al. Oral cavity contains distinct niches with dynamic microbial communities.
Environmental Microbiology. 17(3): 699-710 (2015).
24) Zarco MF, Vess TJ, Ginsburg GS. The oral microbiome in health and disease and the
potential impact on personalized dental medicine. Oral Diseases. 18, 109–120
doi:10.1111/j.1601-0825.2011.01851.x (2012).
25) Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of childhood and adult obesity in
the United States, 2011-2012. JAMA. 311(8):806-814 doi:10.1001/jama.2014.732 (2014).
26) Fourie NH et al. The microbiome of the oral mucosa in irritable bowel syndrome. Gut
Microbes. doi:10.1080/19490976.2016.1162363 (2016).
27) Yoshizawa JM, Schafer CA, Schafer JJ, Farrell JJ, Paster BJ, Wong DTW. Salivary
biomarkers: toward future clinical and diagnostic utilities. Clincial Microbiology. 26:781-
791 (2013).
28) Costello EK et al. Bacterial community variation in human body habitats across space
and time. Science 326:1694-1697 (2009).
29) Caporaso JG et al. QIIME allows analysis of high-throughput community sequencing
data. Nat Methods 7:335-336 (2010).
30) Bervoets L et al. Differences in gut microbiota composition between obese and lean
children: a cross-sectional study. Gut Pathogens 5(1):1-10 (2013).

20
31) Suvan J, D’Aiuto F, Moles DR, Petrie A, Donos N. Association between
overweight/obesity and periodontitis in adults. A systematic review. Obes Rev 12:381-
404 (2011).
32) Kaplan JB. Biofilm dispersal: mechanisms, clinical implications, and potential
therapeutic uses. J Dent Res 89:205-218 (2010).
33) Ferrer M et al. Microbiota from distal guts of lean and obese adolescents exhibit partial
functional redundancy besides clear differences in community structure. Environmental
Microbiology. 15:211-226 doi:10.1111/j.1462-2920.2012.02845.x (2013).
34) Kelly T, Yang W, Chen C-S, Reynolds K, He J. Global burden of obesity in 2005 and
projections to 2030. International Journal of Obesity. 32:1431-1437
doi:10.1038/ljo.2008.102 (2008).
35) Patil DP et al. Molecular analysis of gut microbiota in obesity among Indian individuals.
Journal of Biosciences. 37(4):647-657 (2012).
36) Ley RE, Backhed F, Turnbaugh P, Lozupone CA, Knight RD, Gordon JI. Obesity alters
gut microbial ecology. PNAS. 102(31):11070-11075 (2005).
37) Team, R. (2014). RStudio: integrated development for R. RStudio, Inc., Boston, MA. URL
http://www. RStudio. com/ide.
38) Vázquez-Baeza Y, Pirrung M, Gonzalez A, Knight R. EMPeror: a tool for visualizing
high-throughput microbial community data. GigaScience 2:16 (2013)
39) Werner, J. “E. Alpha Diversity.” WernerLab. Website. 15 March 2016.
40) Bray, J. R. and J. T. Curtis. An ordination of upland forest communities of southern
Wisconsin. Ecological Monographs 27:325-349 (1957).

21
41) Kruskal; Wallis (1952). Use of ranks in one-criterion variance analysis. Journal of the
American Statistical Association 47 (260): 583–
621. doi:10.1080/01621459.1952.10483441
42) García-Closas, M et al. Collection of genomic DNA from adults in epidemiological
studies by buccal cytobrush and mouthwash. Cancer Epidemiology 10:687-696 (2001).

22
Appendix I
Verifying imputations
Along with this thesis project, I verified single nucleotide polymorphism (SNP)
genotypes via sanger sequencing from imputations. An imputation is a prediction of a
individual’s SNP genotype based on haplotype blocks. Each sample received a dosage score
which expressed confidence for the imputation. I verified these imputation predictions by
sequencing individual’s to assess their genotype for the SNP. I sequenced two SNPs, rs7444887
(n=53) and rs77693952 (n=13). Primers were designed through Primer Design and Tools
provided by BiSearch (Figure 1A-B) and oligos were ordered from IDT Inc. Primers were
optimized for polymerase chain reaction (PCR) before samples were run on the optimized PCR
program and then run on a 1% agarose gel to ensure that all samples were amplified.
To prepare the samples for sequencing, they were purified via the QIAquick PCR
purification kit according to manufacturer’s instructions (Qiagen). Purified samples were
quantified for DNA concentration [ng/µl] on a Nanodrop2000 spectrometer. Samples were then
diluted and prepared for sequencing by ACGT Inc. according to their low-cost option (LCO)
single-pass DNA sequencing standards. Samples were diluted down to 3ng in 5 µl and the
forward and reverse primers were custom mixed in at a concentration of 10pmol/µl. Prepared
samples were then sent for sequencing at ACGT Inc. Examples of the results can be seen in
Figure 1C-D. Of the 53 samples for rs7444887 all controls validated, and only 3 individuals with
low dosage scores (<0.5) did not validate. For rs77693952 all controls validated, but 1 individual
with a high dosage score (>0.99) did not validate.

23
Figure 1: Primers and sequencing results for imputation samples (A) The forward and reverse primers designed for rs7444887. (B) The forward and reverse primers designed for
rs77693952. (C) Example sequencing results for two different samples using rs7444887 primers. Reference allele is
A/T. Highlighted peak is the SNP. Top picture shows a homozygous genotype call while bottom picture shows a
heterozygous genotype call. (D) Example sequencing results for two different samples using rs77693952 primers.
Reference allele is G/C. Highlighted peak is the SNP. Top picture shows a homozygous genotype call while bottom
picture shows a heterozygous genotype call.