Embed Size (px)
Citation preview

Experience with Medication Error Reporting
Systems in an Irish Hospital
Tim Delaney, FPSIHead of Pharmacy
AMNCH Tallaght, Dublin 24, Ireland
First OECD Health Care Quality Indicators Seminar on Improving Patient Safety Data Systems. Farmleigh House, Dublin, June 29-30, 2006

Indicators - starting point for change

Medication Error Reports as Indicators
OECD Health Technical Papers No. 19 (2004), p.29

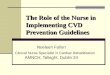
Drugs involved in harmful incidents
0
1
2
3
4
5
6
7
8
9
Top Drugs involved in Reports
Per
cen
tag
e o
f R
epo
rts
Enoxaparin
Paclitaxel
Amiodarone
Insulin
Moxifloxacin
Zoledronic acid
Aspirin
Clopidogrel
Tetracaine
(Kirke C. AnalyzErr Pilot Study 2006)

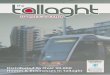
Irish Experience: Errors by stage of the
Medication Use Process (all reports)
0
10
20
30
40
50
60
Presc
ribing
Order
ing
Dispen
sing/
Deliver
y
Admini
strat
ion
Mon
itorin
gN/A
Per
cen
tag
e o
f R
epo
rts
(Kirke C. AnalyzErr Pilot Study 2006)

Stage involved in harmful incidents(Kirke C. AnalyzErr Pilot 2006)
0
10
20
30
40
50
60
Presc
ribing
Order
ing
Dispen
sing
Admini
strat
ion
Mon
itorin
gNA
Per
cen
tag
e o
f R
epo
rts

5 Principles for Creating an Environment for Safety
1. Culture: There should be a non-punitive culture for reporting healthcare errors that focuses on preventing and correcting systems failures and not on individual or organisation culpability.
2. Data Analysis: Information submitted to reporting systems must be comprehensively analysed to identify actions that would minimise the risk that reported events recur.
General Principles for Patient Safety Reporting Systems, (NCCMERP 2003)

5 Principles for Creating an Environment for Safety
3. Confidentiality. Confidentiality protections for patients,
healthcare professionals, and healthcare organizations
are essential to the ability of any reporting system to
learn about errors and effect their reduction.
4. Information Sharing. Reporting systems should
facilitate the sharing of patient safety information among
healthcare organizations and foster confidential
collaboration with other healthcare reporting systems
General Principles for Patient Safety Reporting Systems, (NCCMERP 2003)

5 Principles for Creating an Environment for Safety
5. Legal Status of Reporting System Information. • The absence of legal protection for information submitted
to patient safety reporting systems discourages the use of such systems, which reduces the opportunity to identify trends and implement corrective measures.
• Information developed in connection with reporting systems should be privileged for purposes of state judicial proceedings in civil matters, and for purposes of state administrative proceedings, including with respect to discovery, subpoenas, testimony, or any other form of disclosure
General Principles for Patient Safety Reporting Systems, (NCCMERP 2003)

Legal protection and reporting
• In Ireland, incident report and analysis may be protected under the Freedom of Information Act but are still discoverable in the event of civil litigation
• This is a significant deterrent to the production of RCA reports.

Factors to Consider when Comparing Reporting Rates
• Reporting Culture
• Differences in the types of reporting and detection system
• Differences in the patient populations served
• Definition of error

1. Culture
• Differences in culture among health
care organisations can lead to
significant differences in the level of
reporting of medication errors.

Culture - sense-making in a community of practice
Fellenz. M. (Trinity College Dublin / Irish Management Institute, 2006)

Drive out fear!
Great loss is associated with fear, when workers are afraid to ask a question of to take a position.
A secure worker will report faults and point to conditions that impair quality
W. Edwards Deming : “Out of the Crisis” (1986)

Staff Values (1998)
RespectCaringOpennessPartnership &
teamworkFairness & equity
Reporting Culture (2000) Blame Punishment Secrecy Adversity Cynicism Unfairness &
inequity
AMNCH – A culture of safety?

100%99%97%
83%
49%
0
20
40
60
80
100
120
140
160
Pharmacists Nurses Pharmacytechnicians
Doctors Dieticians
No
. R
epo
rts
(Oct
-Dec
200
4)
0%
20%
40%
60%
80%
100%
Cu
mu
lati
ve %
Rep
ort
s
Frequency Cumul %
Reporting culture varies between professions at AMNCH

2. Populations Served
• Differences in the patient populations served by various health care organisations can lead to significant differences in the number and severity of medication errors occurring among organisations.

3. Definition of error
• Differences in the definition of a
medication error among health care
organisations can lead to significant
differences in the reporting and
classification of medication errors.

Definition – what’s in a name?
Hierarchy of Medication Safety Incidents
N e a r M iss H a za rd o u s C o n d it ion
P o te n tia lA d ve rse D ru g E ve n t
(P A D E )
A d ve rse D ru g R e a c tion(A D R )
M e d ica tio n E rro r
A d ve rse D ru g E ve n t(A D E )
M e d ica tionS a fe ty
In c id e n t
Source: AMNCH Tallaght: Medication Safety Incident Reporting Policy DTC4/2002

OECD uses JCAHO operational definition
OECD Health Technical Papers No. 19 (2004), p.29

NCC MERP Definition “Any preventable event that may cause or lead to
inappropriate medication use or patient harm while the medication is in the control of the health care professional, patient, or consumer. Such events may be related to professional practice, health care products, procedures, and systems, including prescribing; order communication; product labelling, packaging, and nomenclature; compounding; dispensing; distribution; administration; education; monitoring; and use."
NCCMERP (1998)


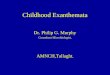
4% of reported incidents involved patient harm
(AMNCH data 2004)
67 69
119
318 4 0 0 1
0
50
100
150
A B C D E F G H I
NCCMERP Category
Num
ber o
f Rep
orts
(Kirke C. AMNCH Data Oct-Dec 2004)

7% of reported incidents involved patient harm
(5 Irish Hospitals Pooled Data, 2006)
0
10
20
30
40
50
60
70
80
90
100
A B C D E F G H I
NCC-MERP Category
Per
cen
tag
e o
f R
epo
rts
Cu
mu
lati
ve P
erce
nta
ge
Percentage ofReports
CumulativePercentage
(Kirke C. AnalyzErr Pilot Study 2006)

Issues with definitions
• OECD definition is equivalent to NCC MERP Categories G and I
• Covers only 2 of 5 NCC MERP sub-categories of errors causing harm
• Excludes a major harm category -errors where emergency intervention was needed to sustain life

4. Reporting Systems
• Differences in the types of reporting
and detection systems for medication
errors among health care organizations
can lead to significant differences in the
number of medication errors recorded

Medication Safety Incident Reports Received Monthly
Jan 2001 - December 2005
0
20
40
60
80
100
120
140
160
Jan-
01
Mar
-01
May
-01
Jul-0
1
Sep
-01
Nov
-01
Jan-
02
Mar
-02
May
-02
Jul-0
2
Sep
-02
Nov
-02
Jan-
03
Mar
-03
May
-03
Jul-0
3
Sep
-03
Nov
-03
Jan-
04
Mar
-04
May
-04
Jul-0
4
Sep
-04
Nov
-04
Jan-
05
Mar
-05
May
-05
Jul-0
5
Sep
-05
Nov
-05
Target Total Medication Safety Incidents Reported in Adult and Paediatric Services Six-Monthly Mean
Monthly Medication Safety Incident Reporting at AMNCH 2001-2005

AMNCH Tallaght Dispensary Errors 2004/2005
Errors detected in Pharmacy 2004 2,125Errors detected on Ward 81Errors reaching patient 41
Detection in Pharmacy per 100,000 items 709Detection in Ward per 100,000 items 27Not detected (given to patient) per 100,000 items 14
Errors detected in Pharmacy 2005 2,795Errors detected on Ward 77Errors reaching patient 21
Detection in Pharmacy per 100,000 items 1067Detection in Ward per 100,000 items 29Not detected (given to patient) per 100,000 items 8

Limitations of passive reporting
OECD Health Technical Papers No. 19 (2004), p.30

What is counted? Medication Error reporting at AMNCH Tallaght
2002-5
0100020003000400050006000700080009000
10000
2002 2003 2004 2005
Nu
mb
er o
f R
epo
rts
Dispensary errors
Medication Safety Incident Reports
Aseptic Unit Errors
Clinical pharmacist QA Interventions

What CIS sees Medication Error reporting at AMNCH Tallaght
2002-5
0100020003000400050006000700080009000
10000
2002 2003 2004 2005
Nu
mb
er o
f R
epo
rts
Dispensary errors
Medication Safety Incident Reports
Aseptic Unit Errors
Clinical pharmacist QA Interventions


“ Mistakes are
the portals
of discovery.”James Joyce