Embed Size (px)
Citation preview

1
EXPENDITURE ON
PREVENTION ACTIVITIES
UNDER SHA 2011:
SUPPLEMENTARY GUIDANCE
June 2013 Version
_
Health Division
www.oecd.org/health
Directorate for Employment, Labour and Social
Affairs
Contacts: David Morgan (OECD) / John Henderson (UK Department of Health)

2
ACKNOWLEDGEMENTS
1. The report was prepared by John Henderson of the UK Department of Health. Useful
comments and advice were received from colleagues in the OECD Health Accounts team,
Patricia Hernandez-Pena and Cor van Mosseveld from WHO NHA team, and the participants
of the 14th Meeting of National Health Account Experts. Health accounts experts in
Australia, Denmark, Finland, France, Korea, Netherlands, Norway and Switzerland, as well
as from Eurostat, provided helpful comments and suggestions.
2. This project was funded under EU contribution agreement 2011 53 01.

3
TABLE OF CONTENTS
ACKNOWLEDGEMENTS .............................................................................................................. 2
EXECUTIVE SUMMARY .............................................................................................................. 4
1. INTRODUCTION ........................................................................................................................ 5
2. GENERAL CONSIDERATIONS AND THE ACCOUNTING BOUNDARIES OF
‘PREVENTION’ ............................................................................................................................... 8
Main boundary criteria used in SHA 2011 .................................................................................... 8
A. Prevention versus non-health spending ................................................................................. 12
B. Prevention versus health-related spending ............................................................................. 15
C. Prevention versus other health spending ................................................................................ 18
Summary of the prevention boundary under SHA 2011 ............................................................. 20
3. MAPPING TO NEW 2ND
DIGIT PREVENTION CLASSES ................................................... 23
Mapping from SHA 1.0 to SHA 2011 – examples from England ................................................ 23
Some additional guidance on using SHA 2011 2nd
digit prevention classes ............................... 23
HC.6.1 .......................................................................................................................................... 24
HC.6.2 .......................................................................................................................................... 24
HC.6.3 .......................................................................................................................................... 25
HC.6.4 .......................................................................................................................................... 25
HC.6.5 .......................................................................................................................................... 26
HC.7.1 .......................................................................................................................................... 26
4. CONCLUSIONS......................................................................................................................... 28
REFERENCES ............................................................................................................................... 29

4
EXECUTIVE SUMMARY
3. Experience from the substantial health gains of the 20th century suggests that spending on
prevention could be an important factor. Therefore, gathering data on such spending that are
consistent and comparable, both over time and across countries, is potentially very useful.
This paper aims to help clarify what should be included as spending on prevention under SHA
2011 to facilitate accurate comparisons.
4. Prevention can change progression through the natural history of disease for the better,
and takes in any measure that aims to avoid or reduce the severity of injuries or diseases. It
includes both collective measures and individual services.
5. A key criterion for inclusion under SHA 2011 is whether the primary purpose of the
spending is health. Therefore, some policies which address the wider determinants of health
and have known impacts upon health – e.g. improving or increasing incomes, employment,
housing, or active travel – are considered outside the SHA boundary as they have some other
primary purpose. However, much of public spending to improve occupational health and
safety and environmental health, to prevent mortality and injuries in road and transport
accidents, and to increase food safety, do fall within the boundary of prevention.
6. The document strives to better define the prevention boundaries in three ways: in relation
to other health spending, health-related spending, and non-health spending. Thus, the
legislative and regulatory process to increase health and safety, or curtail the advertising and
promotion of hazardous behaviour, are considered part of health governance rather than
spending on prevention per se; while the enforcement of such regulations is classed as health-
related spending. The costs of compliance with regulations by individuals and companies
may have the purpose of avoiding the penalties for contravention, so any expenditure in this
domain is also outside the boundary of prevention and health. Likewise, voluntary measures
by individuals and companies may have a primary purpose other than health, and so are
outside the boundary too. When their purpose is prevention, public health programmes and
personal preventive healthcare services are within the prevention boundary, including when
requested by patients – these include many forms of information, education, counselling and
mass communication, plus immunisation, screening and check-ups. Pharmaceutical spending,
including prophylactic medication and contraceptives, is classed with medical goods rather
than preventive spending under SHA 2011.
7. At the 2nd
digit level within the SHA functional classification, spending should be
allocated according to its primary intent, including to its dominant purpose where there is
more than one purpose. Guidance is also offered, for example, on distinguishing screening
programmes from check-ups, and programme planning from governance. Tables and
examples are incorporated to illustrate what should and should not be included as prevention
spending.

5
1. INTRODUCTION
8. Prevention is of great importance in the story of health gains over the 20th century and has
the potential to play a major role in the 21st. On the face of it, spending on prevention seems
to vary greatly across countries (OECD, 2011) – both in terms of absolute amounts and shares
of total health spending. Some countries like to benchmark their spending on prevention by
making comparisons with what other countries spend. Harmonising methods of calculating
such expenditure should help to ensure that reported differences are real, rather than
attributable to varying methods or inclusions.
9. The prevention category in SHA 2011 is one of the most changed areas compared with
SHA 1.0. SHA 2011 takes a different approach to the organisation of prevention; it
emphasises purpose – i.e. primary and secondary prevention – as well as type of service, to
define prevention sub-classes – and includes both individual and collective prevention
spending.
10. SHA 2011 explains the refinement of the functional classification of prevention as
follows:
“Prevention. The functional category in the new manual has been better aligned to the purpose of consumption, i.e. one of the objectives of contacting the health system is to receive preventive care. The boundary criteria (as described in Chapter 4 [of SHA 2011]) have been applied to better differentiate health prevention from the health care-related categories (HCR) of SHA1.0. Refined definitions should ensure comprehensive, exhaustive and mutually exclusive categories and increase the comparability of HC classes across countries. The “prevention and public health” class of SHA 1.0 has been unclear in its content, because the categories were based on a mix of criteria: “public” referred at the same time to government-financed services, place of delivery (public-owned services) and the beneficiaries involved (population priority groups). Thus, “prevention and public health” has been restructured into a preventive class, which is better distinguished by purpose from the curative components.” (SHA 2011, p74).
11. SHA 2011 sets out a rationale behind the categories of the functional classification using
the progression of illness and disease from a healthy state. “The natural history of disease
qualifies the various components of the health system contact and allows a breakdown by
specific type of service.” (SHA 2011, p76)
“The starting point of this process is a healthy condition. At this stage, interventions aim to enhance health status and to maintain a condition of low risk of diseases, disorders or injuries – in other words, to prevent their occurrence (HC.6), through vaccinations or an injury prevention programme, for example. Preventive interventions also cover individuals at specific risk and those who have either no symptoms of the disease or early signs and symptoms, where early case detection will assist in reducing the potential damage by enabling a more successful intervention. Take the examples of breast and prostate cancer, where age and sex affect the risk; certain lifestyle choices increase the risks, as smoking does for lung cancer.” (SHA 2011, p76)
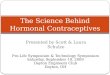
12. This is depicted in Figure 1.1.1 This illustrates two different types of preventive services:
some are consumed collectively – “epidemiologic surveillance and risk and disease control
1 Figure 5.1 of SHA 2011.

6
programme management” – while others are personal prevention services consumed by
individuals – “information and counselling, immunization, early case detection, healthy
condition monitoring”. Expenditure on both collective and individual services is included
under SHA 2011.
Figure 1.1. The natural history of disease and the purpose of health care goods and services
13. It may also be helpful to expand the issue of risk status and interventions to reduce risks –
which can usefully be illustrated using the example of non-communicable diseases (NCDs),
such as cardiovascular disease (CVD)2. WHO has categorised NCD risk factors as
“behavioural” and “physiological”.
Risk factors3
Modifiable behavioural risk factors Tobacco use, physical inactivity, unhealthy diet and the harmful use of alcohol increase the risk of or cause most NCDs.
Tobacco accounts for almost 6 million deaths every year (5.1 million from direct tobacco smoking and 600 000 from exposure to second-hand smoke), and is projected to increase to 8 million – or 10% of all deaths every year – by 2030.
About 3.2 million deaths annually can be attributed to insufficient physical activity.
Approximately 1.7 million deaths are attributable to low fruit and vegetable consumption.
Half of the 2.3 million annual deaths from harmful drinking are from NCDs.
2 Non-communicable diseases - or NCDs - like heart attacks and strokes, cancers, diabetes and chronic respiratory
disease account for over 63% of deaths in the world today. That is why global leaders met at the
United Nations in New York from 19-20 September 2011 to set a new international agenda on NCDs.
http://www.who.int/nmh/events/un_ncd_summit2011/en/
3 WHO fact sheet on Non-Communicable Diseases, September 2011:
http://www.who.int/mediacentre/factsheets/fs355/en/index.html
Natural History of Disease Personal consumption Collective consumption
Low risk
At risk
Disease
Dsability (body
structure and
function)
Chronic
Condition and
Functional
decline
Dependency for
self care
Death
Collective consumption
Collective prevention:
Epidemiologic
surveillance & risk and
disease control
programme
management
Personal prevention:
Information & counseling,
Immunization, Early case
detection, Health condition
monitoring
Governance and
Health system
administration
Early signs &
symptoms
Cure - Treatment -
Rehabilitation
Maintenance - LTC - Palliative
care

7
Metabolic/physiological risk factors These behaviours lead to four key metabolic/physiological changes that increase the risk of NCDs: raised blood pressure, overweight/obesity, hyperglycemia (high blood glucose levels) and hyperlipidemia (high levels of fat in the blood). In terms of attributable deaths, the leading NCD risk factor globally is elevated blood pressure (to which 13% of global deaths are attributed), followed by tobacco use (9%), raised blood glucose (6%), physical inactivity (6%), and overweight and obesity (5%).
14. Efforts by the healthcare system to change modifiable behavioural risk factors are
included as part of prevention, when these take the form of risk status assessment or early
case detection by a health professional, and information, education and counselling with the
intent of changing behaviour and reducing risk. However, efforts to tackle the “causes of the
causes” (why people behave in ways that put their health at risk) by changing the “social
determinants of health”4, might be difficult to distinguish from other programmes with a non-
health primary purpose. Likewise, some interventions by the healthcare system to change
modifiable physiological risk factors might be difficult to distinguish from tertiary prevention
and treatment. These issues are addressed further in Section 2 below.
15. The rest of this paper aims to address some of the possible ambiguities that may remain,
notwithstanding the further guidance in SHA 2011, to illustrate some example areas, to
compare the implications of moving from SHA 1.0 to SHA 2011, and to offer some further
clarifications about the functional classification of prevention expenditure.
4 Prof Sir Michael Marmot, on behalf of the Commission on Social Determinants of Health: ‘Achieving health
equity: from root causes to fair outcomes’: “Health equity is central to this premise and to the work of the
Commission on Social Determinants of Health. Strengthening health equity—globally and within countries—
means going beyond contemporary concentration on the immediate causes of disease. More than any other global
health endeavour, the Commission focuses on the “causes of the causes”—the fundamental structures of social
hierarchy and the socially determined conditions these create in which people grow, live, work, and age.” The
Lancet, Volume 370, Issue 9593, pp 1153-63, 29 September 2007.

8
2. GENERAL CONSIDERATIONS AND THE ACCOUNTING BOUNDARIES
OF ‘PREVENTION’
16. This section addresses the setting of boundaries of prevention in the SHA 2011
classification of health care functions, and other general considerations. The boundary issues
can be divided into the three following groupings:
A. The global boundary of healthcare as it affects prevention – i.e. prevention versus
non-health spending;
B. The HCR boundary – i.e. prevention within health spending versus healthcare-
related spending;
C. The prevention boundary – i.e. spending on prevention versus other areas of health
spending.
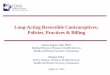
Figure 2.1. Boundaries of the health system
Based on: WHO ‘Health Systems Performance Assessment’ (HSPA)5
Main boundary criteria used in SHA 2011
17. In setting the boundaries of health spending (and that of prevention), there has been some
shift in emphasis in the ranking of the criteria used to define health care between SHA 1.0 and
SHA 2011. SHA 2011 overtly gives primacy to the criterion of purpose or intent: “The
main criterion to include or exclude certain activities relates to their role in enhancing health
5 WHO ‘Health Systems Performance Assessment’ (2003) http://www.who.int/publications/2003/hspa/en/
Health
Personal medical
Non-personal
health services
Intersectoral
action
Other factors
C O
V E
R A
G E

9
status, diminishing ill-health, or preventing the deterioration of the health of individuals
and/or the population as a whole.” (SHA 2011, p56)6.
18. Other criteria can also be relevant in practice. These may include the following:
Sometimes there is ambiguity over primary purpose – it may be unclear if the
main intent of the activity is either to promote health or prevent disease. If there is a
strong chance that the primary purpose is non-health, this could be a reason for
exclusion.
The distinction between the health care system and the broader health system.
Figure 2.1 above illustrates this, and the source states (p7) “The third definition
includes all actors, institutions and resources that undertake health actions—where
the primary intent of a health action is to improve health. It is broader than personal
medical and non-personal health services. It incorporates selected intersectoral
actions in which the stewards of the health system take responsibility to advocate
for health improvements in areas outside their direct control, such as legislation to
reduce fatalities from traffic accidents. This is shown by the largest circle” in Figure
2.1. Many activities with a preventive effect are part of “intersectoral action” – and
part of the health system, but not the health care system.
Practicality of extracting relevant data and or disaggregating data by functions. For
example, an institution (such as the UK’s Health and Safety Executive) might
undertake a mixture of activities some of which are inside the SHA boundary and
others of which are outside. Ideally the appropriate expenditure shares on the
different activities should be allocated accordingly. However, sometimes this may
be impracticable, and the options may be to include all of the institution’s
expenditure, or none, if further disaggregations are problematic. How much effort
to put into overcoming such problems will partly depend on the usefulness of the
results – for example, the larger the sums involved, the more useful the effort to
disaggregate the spending is likely to be7.
Prevention at the individual’s own initiative may be excluded, as: (i) there may be
ambiguity over primary intent (e.g. the primary intent might be comfort or social
acceptability); and (ii) in practice, data on such spending may be embedded in other
expenditure data and difficult to extract. However, with health systems putting
increasing emphasis on personal responsibility and choice, it is possible that a
growing share of prevention activities may fall into the category of “the individual’s
own initiative”. If so, it would be important not to lose sight of such spending8.
19. A key boundary issue is the role of the health system in the process of deciding preventive
measures. Prevention includes identifying measures to avoid risks and their health
consequences, and determining measures appropriate to a specific health system, in a specific
country, for a specific risk or disease. The general surveillance of specific and strategic
collective risks is a responsibility of the health system and is also included as prevention.
6 The SHA explains that the other criteria (over which purpose takes precedence) are: qualified medical or health
care knowledge and skills are needed in carrying out the function, or to supervise the function (or the
function is governance, administration or financing); consumption is for the final use of health care
goods and services of residents; and there is a transaction of health care services or goods.
7 If many countries were spending large amounts on, say, ensuring food safety, it may be useful to disaggregate the
expenditure and record the preventive part of such spending (which might then facilitate analysis of its
costs and efficiency).
8 It would therefore be sensible to try to maintain records of such spending where possible, and It would also be
helpful to review this convention periodically to ensure that its application remains helpful.

10
20. Preparatory work for preventive regulations relies on the health system but it may involve
different types of activities, such as research9 and surveillance as well as evidence gathering.
Regulatory work to address health risks may involve other sectors, e.g. for road safety risks,
the role of the health system may be to help design or to certify or to sanction the validity of
the health preventive components, but regulation of road safety matters remains under the
road authorities.
21. The regulatory agency in the relevant sector will take care of its enforcement – e.g. in the
road safety example, the road authorities. In this case enforcement is classed as healthcare-
related, and therefore outside the SHA healthcare boundary. For health laws involving the
health system itself, responsibility for compliance and enforcement remains with the health
system. Therefore enforcement of healthcare regulations, applying to healthcare providers, is
inside the SHA healthcare boundary (and enforcement of prevention regulations applying to
prevention providers is within the prevention boundary). (SHA 2011, p107) Sanctions are
usually linked to legal procedures.
22. The charts below try to illustrate some areas that are inside the SHA 2011 prevention
boundary, and others that are not. Figure 2.2 aims to explain the rationale for the SHA
classification of relevant activities.
9 Research needed may involve both health matters as well as non-health matters, such as the materials for the
seatbelt and their ergonomics, which are out of the scope of health. But epidemiological research is
also needed to support the role of the health system to propose measures, to define a road safety
preventive program and to sanction the health component of the regulatory proposal by the road
authority.

11
Figure 2.2. Types of activities and rationale for their SHA classification
Collective measures10
Individual actions11
23. In the following sections, various areas that might be included in prevention spending,
non-prevention health spending, healthcare-related spending or excluded from the health
spending boundary, are illustrated.
10 Collective measures typically can be consumed by groups of people simultaneously, and use of the measure by
one person does not reduce its availability for others.
11 Individual actions typically involve personal consumption and use by one person does reduce availability for
others. Enforcement may have elements that are “collective” – e.g. monitoring data and compliance
report publishing – and elements that are “individual” – e.g. inspections and prosecutions.
Healthcare services – where the primary purpose is prevention. Broader services and programmes – any measure whose primary aim is to avoid disease or injury, or detect risks to health so that the risks can be lowered consequently reducing the number or the severity of diseases and injuries.
Individual services – where the primary purpose is prevention. Includes: informing individuals; assessing their risks; and efforts to reduce their risks.
HC.6
Pharmaceuticals and medical goods There is a specific functional classification for pharmaceuticals that should be used (unless spending on the pharmaceuticals or medical goods is inseparable from the rest of the preventive programme spending).
Governance of healthcare and the health system. Includes: regulation to protect public health; other methods of exerting strategic influence; strategic management of health systems to improve health.
HC.7.1
Broader policies Policies may incidentally improve health, but where there is likely to be another main motivation then these are to be classified according to the primary intent.
Voluntary measures Companies pursue corporate social responsibility, for example, but the primary intent may be sales or profits, rather than health. Individuals undertake actions that incidentally improve their health, but where the primary intent may be another motivation.
excluded
Compliance costs Individuals and companies incur costs in complying with regulations, but the primary intent may be to avoid penalties (financial, reputational, etc) for contravention.
excluded
Enforcement Regulations give rise to costs of monitoring compliance, surveillance, and upholding the law. These are classed as healthcare-related.
HCR.2
Multi-sectoral health promotion In joint efforts with other sectoral programmes, prevention and health promotion may be secondary, and outside the healthcare boundary.
HCR.2.1 &
HCR.2.2
HC.5
HC.6
Enforcement within healthcare When regulations apply within healthcare, then inspecting prevention providers and tackling contraventions, etc, by such providers is classed as part of prevention.

12
A. Prevention versus non-health spending
24. SHA 2011 contains a section explaining the considerations of boundary setting with
regards to prevention (SHA 2011, pp100-102). Here those considerations and the above
criteria are used to provide further clarification in some specific areas.
25. There are changes between SHA 1.0 and SHA 2011 in what falls within the boundary of
prevention spending. For example, SHA 1.0 states in Para. 3.4 “In the context of the SHA,
general public safety measures like technical standards monitoring, road safety, etc., are not
considered as application of medical technology and are, for that reason, excluded from the
core health care functions.” On the other hand, SHA 2011 states that “Prevention is any
measure that aims to avoid or reduce the number or the severity of injuries and diseases, their
sequelae and complications” (p100).
26. A specific example of a change is the treatment of health and safety at work, much more
of which is included under a broader boundary in SHA 2011.
SHA 1.0 p123: “Occupational health activities to improve ergonomy, safety and health and environmental protection at the workplace, accident prevention, etc., should be distinguished from occupational health care. They are not to be recorded under health care activities in the SHA.”
SHA 2011 p105, Table 5.2: Included under SHA2011 in HC.6 • Ergonomy, safety (health part) • Health and environmental protection at work (health part) • Accident prevention at work (health part) [excluded under SHA1]
27. However, several OECD countries may already include spending on occupational health
protection and safety (in addition to occupational health) in their public health and prevention
expenditure (i.e. as reported under SHA 1.0).
28. To determine inclusion or otherwise, SHA 2011 uses as the main criterion the primary
purpose or intent. Therefore, prevention of mortality and morbidity due, for example, to
occupational, transport and other hazards would be included – where it is clear that the
primary intent of the action is prevention of harm to human health. However, this does not
mean that all spending on programmes, or all parts of programmes in occupational health and
safety, and transport safety, for example, are to be included in category HC6. The components
not included are those associated with other primary intents, e.g. transport or economy.
29. Figure 2.3 below shows how the considerations illustrated in Figure 2.2 apply in the
specific areas of domestic, fire, occupational and transport risks, using the same “colour
coding”.

13
Figure 2.3. Approaches to tackling risks, and their SHA classification
Collective measures Individual actions
30. Using the above guidance, the Table below indicates where to classify aspects of
prevention spending on activities that tackle the above risks.
SHA 2011 code
Prevention / activities
Domestic & Fires Occupational Transport
HC.1 Treatment of injuries caused by domestic accidents or fires
Treatment of diseases with occupational causes to reduce sequelae and damage in affected populations
Treatment of injuries caused by transport accidents
HC.6.5 Data collection on risks to health & epidemiological assessment – e.g. trends in mortality due to falls, fires, or other causes
Data collection on risks to health & epidemiological assessment
Data collection on risks to health & epidemiological assessment – e.g. trends in accidents by different modes of transport (cars, cycles, pedestrians, etc), times and seasons, etc
HC.6.5 Prevention programme planning and design (e.g.
Prevention programme planning and design (eg
Prevention programme planning and design (e.g.
Collective preventive services – e.g. Epidemiology
- assessment of risks from hazards, and reductions expected from interventions
Information & communications - warnings about dangers, and
best practice guidance
Governance for health – e.g. Formulating regulations
- mandatory procedures to be followed; prohibitions; licensing
Other methods of exerting strategic influence
- designing incentive schemes for healthy/safe practice
Health-related actions – e.g. Enforcement of health regulations
- inspections - monitoring compliance - tackling contraventions
Individual preventive services – e.g. Advising individuals
- explaining risks from hazards, and how to reduce them
Health monitoring - assessing risk exposure, and
checking health Subsidies for protective equipment
- if primary purpose is health
Actions where primary motivation is likely to be other than health – e.g. Compliance with regulations, etc
- costs of following mandatory procedures
- licence fees - fines, taxes paid
Voluntary measures by individuals and companies could have a primary motivation other than health – e.g. Radon remediation
- increases property sale value?
Non-mandatory training - increases productivity?
Corporate social responsibility
Examples of Risks
Domestic
Occupational
Transport
Fires
Policies where primary motivation is likely to be other than health – e.g. Active travel policies [CO2 reduction]
- safer walking/cycling routes Employment policies
- reducing unemployment

14
deciding which interventions are most cost-effective)
deciding which interventions are most cost-effective)
deciding which interventions are most cost-effective – and for which groups – children, young people, older people, etc)
HC.6.1 Providing health & safety information to the public – e.g. about causes of fires and accidents, and how to reduce risks to health
Providing health & safety information to firms and workers about sources of hazards, and how to reduce risks – e.g. the importance of wearing hard hats, and safe handling of dangerous materials such as asbestos
Providing health & safety information to the public about sources of hazards, and how to reduce risks – e.g. the importance of wearing seatbelts and helmets, and teaching children how to cycle safely
HC.6.1 Provision of public services – e.g. advisers providing information and advice about reduction of high levels of radon in homes.
Provision of preventive services – e.g. occupational health and safety guidance, and health advisers such as occupational health doctors, nurses, physiotherapists, hygienists or ergonomists
Provision of public services – e.g. crossing supervisors outside schools to reduce accident risks for young children (if primary purpose is injury prevention)
12
HC.7.1 Making regulations to protect public health – e.g. building and other regulations to reduce carbon monoxide poisoning
Making regulations to protect employees’ and public health and safety – e.g. to make the wearing of hard hats mandatory, or bringing in a licensing regime for work involving asbestos
Making regulations to protect public health and safety – e.g. to make the wearing of seatbelts or helmets mandatory
HC.R.2 Enforcing such regulations – e.g. inspection, monitoring, tackling contraventions.
Enforcing such regulations – e.g. inspection, monitoring, tackling contraventions
Enforcing such regulations – e.g. inspection, monitoring, tackling contraventions
Excluded Cost of compliance with regulations – e.g. mandatory changes to buildings or fittings to reduce carbon monoxide poisoning
Costs to firms and public bodies of complying with regulations – e.g. undertaking mandatory training in how to handle asbestos
Cost of compliance with regulations – e.g. motor industry fitting seatbelts to vehicles
Excluded Broader policies – e.g. mandatory building insulation standards (primary purpose may be other than health)
Broader policies – e.g. mandatory leave entitlements (primary purpose may be social rather than health)
Broader policies – e.g. to promote walking or use of bicycles (primary purpose may be other than health)
Excluded Costs of voluntary measures to reduce risks – e.g. measures by householders to reduce accumulation of radon in homes
Costs of voluntary measures to reduce risks – e.g. private purchase of training
Costs of voluntary measures to reduce risks – e.g. purchase and use of (non-mandatory) helmets by cyclists
12
Epidemiological studies have demonstrated that strategic points, such as outside schools, are linked to higher
rates of road traffic accidents, mortality and injuries to children, and where prevention of these is the
primary intention this is classed as a health education intervention.

15
B. Prevention versus health-related spending
31. SHA 2011 offers clarification concerning the boundary between prevention under health
spending and that under healthcare-related expenditure (SHA 2011, p101 and pp115-116).
32. SHA 2011 explains that “the type of services included in the health prevention boundary
is restricted to those components with a primary health purpose. Interventions that go beyond
the health care boundary but are policy relevant can be reported as health care-related items.”
(p101) So, SHA 2011 has the class “HCR.2 Health promotion with a multi-sectoral
approach”. “The aim of this class is to account for health promotion resources that may go
beyond the health care boundary, though nevertheless clearly involved with a health interest.”
(p114) (See also Figure 2.1, and paragraph 18.)
33. Figure 2.4 below shows how the considerations illustrated in Figure 2.2 apply in the
specific areas of environmental, food safety and behavioural risks, using the same “colour
coding”.
Figure 2.4. Approaches to tackling risks, and their SHA classification
Collective measures Individual actions
Collective preventive services – e.g. Epidemiology
- assessment of risks from hazards, and reductions expected from interventions
Information & communications - warnings about pollution levels,
other dangers, and mass media health campaigns
Governance for health – e.g. Formulating regulations
- Emissions limits; labelling; mandatory procedures to be followed; prohibitions; advertising restrictions
Methods of exerting strategic influence - designing incentive schemes or
co-regulation (alcohol reduction)
Individual preventive services – e.g. Advising individuals
- explaining risks from hazards, and how to reduce them
Health monitoring - health check-ups
Financial incentives for healthy behaviour - e.g. to quit smoking
Voluntary measures by individuals and companies may have a primary motivation other than health – e.g. Increase in consumption of fruit,
vegetables, lower fat foods Purchase of bicycles, gym
memberships Corporate social responsibility
Actions where primary motivation is likely to be other than health – e.g. Compliance with regulations, etc
- costs of following mandatory procedures, etc
- licence fees - fines, taxes paid
Policies where primary motivation is likely to be other than health – e.g. Fiscal and licensing policies
- e.g. raising revenue Active travel policies [CO2 reduction]
- safer walking and cycling routes
Examples of Risks
Pollution
Food safety
Unhealthy diet
Inactivity
Smoking
Harmful drinking
Other risky behaviours
Multi-sectoral health promotion Health protection may be an important
secondary goal rather than the primary purpose – e.g. - food & water security measures - safe management of waste - tackling drunkenness
Health-related actions – e.g. Enforcement of health regulations
- inspections - monitoring compliance - tackling contraventions

16
34. Using the above guidance and illustrations relating to environmental and food safety risks,
and risky behaviour that contributes to NCDs, the Table below indicates where to classify
aspects of prevention spending on activities that tackle the above risks.
SHA 2011 code
Prevention / activities
Environmental Food safety Behavioural risks
HC.6.1 Media campaigns or web-pages: Providing information to the public – e.g. about elevated pollution levels, and how to reduce risks to health (e.g. avoiding ozone or particulates hotspots)
Media campaigns or web-pages: Safe handling of foods (to avoid food poisoning).
Mass media campaigns: Providing health information to the public or specific groups, about how to reduce risks – e.g. the importance of good diet and regular exercise.
HC.6.1 Professional advisory services Providing information and advice to firms about sources of hazards, and how to reduce risks – e.g. (if primary purpose is health) how to control contaminants or emissions that are dangerous to human health
Professional advisory services Providing information and advice to firms and workers about sources of hazards, and how to reduce risks – e.g. the importance of personal hygiene, and safe handling of potential sources of pathogens
Physician counselling; and interventions in schools and workplaces
Services such as provision of advice – e.g. from physicians and other healthcare professionals, such as school nurses, community nurses, dieticians and pharmacists
HC.6.5 Financial incentives to reduce risks Subsidies – if it is clear that the primary purpose is to prevent morbidity or deaths – e.g. for adoption of lower-harm technologies
Financial incentives to reduce risks Subsidies – if it is clear that the primary purpose is to prevent morbidity or deaths – e.g. for fortification of certain foods
Financial incentives to reduce risks e.g. rewards for weight loss amongst overweight people, or provision of vouchers for fresh fruit and vegetables to promote healthier diet
HC.6.5 Data collection on risks to health & epidemiological assessment – e.g. if for a health purpose, monitoring whether pollutants such as particulates, ozone, and toxic or carcinogenic pollutants have reached hazardous levels; monitoring water for water-borne disease risks
Data collection on risks to health & epidemiological assessment – e.g. E coli, etc
Data collection on risks to health & epidemiological assessment – e.g prevalence of smoking, heavy drinking, BMI, etc
HC.6.5 Prevention programme planning and design (e.g. deciding which interventions are most cost-effective)
Prevention programme planning and design (e.g. deciding which interventions are most cost-effective)
Prevention programme planning and design (e.g. deciding which interventions are most cost-effective)
HC.7.1 Regulations Making regulations to protect public health – e.g. to reduce anthropogenic emissions of pollutants that harm health
Regulations Making regulations to protect public health – e.g. to make mandatory training in hygiene and display training success certificates; prohibition of substances that are, or may be, toxic, carcinogenic, etc
Advertising regulations: Making regulations to protect public health – e.g. to prevent the advertising of “junk food” to children
HC.7.1 Disclosure regulations: Making regulations to require firms to disclose their emissions – e.g. (if primary purpose is health) disclosure of toxic or carcinogenic substances emitted
Labelling regulations: Making clear when products contain nuts or other potential hazards; requirements to specify additives such as potential carcinogens (e.g. food colourants and preservatives)
Labelling regulations: Making regulations to promote public health – eg mandatory inclusion of labels showing calories, saturated fat and salt contents of foods, so that consumers can consume healthier diets

17
HCR.2.1 (or HCR.2.3)
Enforcing regulations – e.g. inspection, monitoring, tackling contraventions
Enforcing regulations – e.g. inspection, monitoring, tackling contraventions
Enforcing regulations – e.g. inspection, monitoring, tackling contraventions
HCR.2.1 or HCR.2.2
Joint efforts in environmental programmes – e.g. waste management; pollution abatement; and noise control – where the health intent is secondary to an environmental purpose
Joint efforts in food and water programmes – e.g. food and water security, control and distribution
Assessing new technologies for safety and risk reduction; enhancing risk communication and advocacy
Exclude Cost of compliance with regulations – e.g. fitting emissions control technologies
Costs to firms of complying with such regulations – e.g. undertaking mandated training in hygiene
Costs to firms of complying with such regulations – e.g. costs of new labelling
Exclude Self-regulation by industry Costs of voluntary measures to reduce emissions – e.g. corporate social responsibility
Self-regulation by industry Costs of voluntary measures to reduce risks – e.g. removal of colourants
Self-regulation by industry Costs of voluntary measures to reduce risks – e.g. corporate social responsibility
Exclude The collection, treatment and remediation of environmental risks.
Fiscal measures: Taxes on substances that are hazardous to health – e.g. on tobacco, alcohol, saturated fat
35. Although compliance costs are excluded, these are costs that are incurred due to
regulations with a preventive intent, and as they can be very substantial expenditure, it may
well be policy relevant to monitor their scale (as recommended in best practice on assessing
regulatory impacts). If so, a country-specific memorandum item could be reported13
.
36. The categorisation of incentive schemes designed to change risky behaviour may not be
obvious in SHA 2011. When part of an approach to empower and encourage people to
change their behaviour, through improving their knowledge, beliefs and attitudes, perhaps
using techniques such as motivational interviewing14
, these could be seen as part of
“counselling” within IEC (information, education and communication) and thus in HC.6.1.
Some schemes go beyond counselling and include rewards to participants for successful
behaviour change – e.g. a financial reward that varies according to weight lost15
. In the latter
case they could be seen as part of a risk control programme, and thus in HC.6.5.
13 If a number of countries find this useful, and do hereafter report such expenditure, then it may be helpful in
future to make recommendations on methods, for consistency.
14 Motivational interviewing attempts to increase the client's awareness of the potential problems caused,
consequences experienced, and risks faced as a result of the behaviour in question, and to improve
their motivation to change http://en.wikipedia.org/wiki/Motivational_interviewing
15 ‘The ‘Pounds for Pounds’ weight loss financial incentive scheme’, Relton et al (2011):
http://jpubhealth.oxfordjournals.org/content/early/2011/03/28/pubmed.fdr030.full

18
C. Prevention versus other health spending
37. SHA 2011 introduced some changes and clarifications that affect the allocation of
expenditure between prevention and other healthcare expenditure.
School health services
38. School health services need to be distinguished by purpose. If the purpose is prevention –
e.g. health education – then this would be included in HC.6.1, in this example. Any basic
medical treatment provided in a school setting, for example by an on-site medical centre,
would be treated as curative care (e.g. outpatient curative care, HC.1.3).
Collective services
39. Some collective services, such as running blood banks, were included in public health and
prevention under SHA 1.0, but are not classed as prevention under SHA 2011 (SHA 2011,
p105; they are now classed as ancillary services in HC.4.1).
Social programmes versus patient-initiated requests
40. Under SHA 1.0 only prevention “provided as a social programme” was included (at least
for non-communicable diseases; SHA 1.0 p122) – so if the health care system initiated the
preventive activity the expenditure was included, but usually not if the patient initiated the
preventive activity. Hence breast cancer screening would be within HC.6 if the invitation
came from the health care system, but might be classed as treatment (HC.1) if the patient
requested a screen – e.g. if she was, say, above the screening programme age threshold. The
latter exclusion from prevention was largely due to the practical issue of being able to gather
data on spending outside of organised prevention programmes.
41. With increasing autonomy being given to patients in organising their care, it may be more
common for preventive activity to be initiated by patients. Therefore, SHA 2011 does not
explicitly exclude such patient-initiated preventive activity (SHA 2011 p100). In particular,
where the health system invites patients to request preventive care as part of an organised
programme, this should not be excluded from prevention.
Pharmaceuticals and medical goods for prevention
42. Some pharmaceuticals and medical goods may have a preventive function (e.g. to prevent
first occurrence of coronary heart disease or cerebrovascular disease, by reducing blood
pressure or lipids). However, unless they are an integral part of a prevention programme (e.g.
in the case of anti-malaria bed nets, they should be accounted for within the malaria
programme when they are distributed during malaria interventions), any medical goods
dispensed against a prescription or purchased over the counter should be included under
HC.5, medical goods, irrespective of their final purpose.
43. That said, pharmaceuticals for preventive use can be a significant expenditure item
(antihypertensives and statins, for example) and it may well be policy relevant to monitor
their use. In such a case, a country-specific sub-category of HC.5 for preventive medical
goods may be recommended which can be aggregated with all or part of HC.6 categories to
provide a more extensive memorandum item of preventive expenditure.16
16 If a number of countries find this useful, and do hereafter report such preventive pharmaceutical expenditure, then it may be
helpful in future to make recommendations on which specific drugs should be included, perhaps using an
international coding system.

19
Health interventions to reduce metabolic or physiological risk factors
44. As noted in section 1, some interventions by the healthcare system to change modifiable
metabolic or physiological risk factors might be difficult to distinguish from tertiary
prevention and treatment. A key criterion will be whether the intervention is tackling a risk,
or treating a disease. If the primary aim is, say, to prevent a first heart attack, stroke, or other
major cardiovascular disease, then interventions to reduce metabolic or physiological risk
factors would be included as prevention. It is recognised that it may well be easier to identify
expenditure on organised preventive programmes to tackle, say, high blood pressure in groups
likely to be at risk, than to identify expenditure on similar preventive interventions carried out
individually in regular clinical interactions such as GP visits. As noted above (if separable)
pharmacotherapy is recorded as HC.5, as are contraceptives.
45. Figure 2.5 below illustrates ways of tackling communicable and non-communicable
disease risks, using the same “colour coding” system as Figure 2.2.
Figure 2.5. Approaches to tackling risks, and their SHA classification
Collective measures Individual actions
Collective preventive services – e.g. Epidemiology & programme design Information & communications
- warnings about dangers, and mass media health campaigns
Promotion of prevention services - encouraging uptake of
immunisation, screening, etc Infection prevention/control services
Governance for health – e.g. Formulating safety regulations
- consumer products/services, like sunbeds and tanning
- screening and other services - behavioural services
Exerting strategic influence - Incentives or co-regulation
Health-related actions – e.g. Enforcement of health regulations
- Inspections - monitoring compliance - tackling contraventions
Individual preventive services – e.g. Advising individuals
- assessing risk status and how to reduce risk levels
Immunisation and vaccination Screening and health monitoring Referral to other services
- e.g. behavioural therapies to change risky behaviour
Incentive schemes for healthy behaviour - e.g. to quit smoking
Voluntary measures by individuals and companies may have a primary motivation other than health – e.g. Dietary change
- eg reduced salt, fat, calories Exercise change
- eg use of gyms, bicycles, etc Corporate social responsibility
Pharmaceuticals / medical goods – e.g. Antihypertensives Statins / lipid modifiers Prophylactic anti-obesity and weight
loss drugs Prophylactic anti-viral medication Other prophylactic drugs Oral and barrier contraceptives
Policies where primary motivation is likely to be other than health – e.g. Active travel policies
- safer walking and cycling routes Fiscal and licensing policies
Examples of Risks
Infections
Cancer
Overweight
Blood pressure
Blood lipids
Other Non-Communicable
Diseases

20
Summary of the prevention boundary under SHA 2011
46. Using the above guidance, the Tables below indicates where to classify different areas of
prevention spending.
Individual prevention services
Prevention category
SHA 2011 code
Examples of relevant activities
Information, education and communication “IEC”
HC.6.1 Providing health and safety-related information to the public, or specific groups (eg firms or workers), about risks and how to reduce them, e.g.:
the importance of specific risks and their potential to kill people, or injure, or cause harm to human health
how to avoid risks, how to increase safety
information about obligations under relevant regulations
production of guidance documents and other media
working with other professionals to design safety or health campaigns [intermediate consumption, but can be allocated to the relevant service]
designing training courses that teach healthy and safe practices [intermediate consumption, but can be allocated to the relevant service]
provision of advisers or counsellors who advise about risks and their reduction
promotion of uptake of any of above
Counselling, behaviour change programmes, and “nudges”
HC.6.1 Motivating to change behaviour, provided primary intent is health – to reduce risks of disease, injury or death
counselling to improve motivation
behavioural counselling
changing presentation of choices, and similar “nudges”
Incentive schemes HC.6.5 Incentive payments or rewards for behaviour change – e.g. for quitting smoking or losing weight
subsidies for healthier consumption – e.g. vouchers for eating more fruit and vegetables
subsidies for personal protective equipment
Immunisation programmes
HC.6.2 Vaccination – typically undertaken by clinical professionals
Screening programmes
HC.6.3 Early detection of disease or risks before disease appears
eg prostate specific antigen testing, or mammography – typically undertaken by clinical professionals
Healthy condition monitoring
HC.6.4 Check-ups, which may be targeted at specific groups
eg regular pregnancy or dental checks – typically undertaken by clinical professionals
Pharmacotherapy HC.5 Preventive medicines such as antihypertensives, statins, other prophylactic medication and contraceptives [where separable from preventive programmes] – from pharmacies or prescribed by clinical professionals

21
Collective prevention services
Prevention category
SHA 2011 code
Examples of relevant activities
Information, education and communication “IEC”
HC.6.1 Mass media and advertising campaigns
Changing presentation of choices, and similar “nudges”
Surveillance and analysis of risks, and control programmes
HC.6.5 Data collection on risks to human health and safety – eg mortality and morbidity rates
Data recording and information systems – those parts that relate to health and safety risks
Epidemiological assessment, and analysis of causes and consequences of risks, trends, etc
Prevention programme planning and design – eg deciding which programmes are most effective and cost-effective
Evaluation of health and safety programmes
Monitoring of drinking water in public health laboratories
On the job training to better perform these activities
Preparing for disasters, emergencies and response
HC.6.6 Includes designing capacity to respond to health and safety extreme events, and training in how to respond
Governance (making regulations)
HC.7.1 Design and formulation of regulations to protect human health, reduce hazards and increase human safety – eg:
Making provision, or use, of safety equipment mandatory
Requiring specific design amendments, to reduce human mortality or morbidity risks
Prohibitions, such as emissions of health-damaging pollutants or use of carcinogens
Requiring training in safe handling of potentially hazardous substances
Restrictions on advertising (in order to protect health)
Making mandatory health or safety warnings and labelling requirements
Co-regulation (Govt support for this)
HC.7.1 Government efforts to organise and promote a response from other organisations, so as to protect human health, reduce hazards and increase human safety, as an alternative to bringing in regulations

22
Other services
Category SHA 2011 code
Examples of relevant activities
Enforcement (by official enforcers)
HCR.2 Enforcing health and safety regulations – e.g. inspection, monitoring, and tackling contraventions – costs to the public sector
Multi-sectoral health promotion
HCR.2 Health protection may be an important secondary goal rather than the primary purpose – e.g.
food & water security measures
safe management of waste
tackling drunkenness
Planning fiscal measures (Govt support for this)
[other gov’t]
Design and formulation of taxes on substances that are hazardous to health – eg on tobacco, alcohol, saturated fat Design and formulation of tax exemptions or rebates on things that protect health and reduce mortality and morbidity risks
Compliance costs [other private]
Costs to those regulated:
costs of following mandatory procedures, equipment, training, record keeping, etc
licence fees
fines, taxes paid

23
3. MAPPING TO NEW 2nd
DIGIT PREVENTION CLASSES
47. The 2nd
digit classes of prevention in SHA 2011 are organised in a different way to those
of SHA 1.0 – following disease stage, type of service, and purpose. SHA 2011 has a table to
help with the mapping from SHA 1.0 to SHA 2011 (Table 3.1).
Table 3.1 Preventive and public health components in SHA 1.0 and SHA 2011
Mapping from SHA 1.0 to SHA 2011 – examples from England
48. Prevention expenditure in England was the subject of a special study.17
This study has
been updated and expenditures classified according to both the SHA 1.0 and SHA 2011
prevention 2nd
digit classes. The exercise was useful in indicating the large share – around
half – of preventive spending going to “healthy monitoring”, HC.6.4, such as routine check-
ups. It also highlighted that preventive pharmaceuticals would be the largest single element
(and was recorded as a memorandum item). The effect of boundary changes between SHA
1.0 and SHA 2011 was to increase prevention expenditure by about 6%. This mapping
exercise raised a number of other issues, which are covered below.
Some additional guidance on using SHA 2011 2nd
digit prevention classes
Data disaggregation
49. One general issue concerns aggregation of data. Sometimes the available data are
aggregated to a relatively high level, and therefore cover more than one prevention category.
17 Health England (2009) http://www.healthengland.org/publications/HealthEnglandReportNo4.pdf
Content: mostly as described in SHA.1Programme
Code SHA.2
New
item
Programme
Code SHA.1Content: mostly as described in SHA.1
Programme
Code SHA.2
New
item
Programme
Code SHA.1
Maternal and child health; family planning and
counselling HC.6.1 Prevention of non-communicable diseases HC.6.4
Genetic counselling HC.6.1 HC.6.1 Health education HC.6.1 HC.6.4
Identification of genetic abnormalities HC.6.3 HC.6.1 Disease prevention HC.6 HC.6.4
Prenatal and postnatal medical care HC.6.4 HC.6.1 Health promotion HC.6. HC.6.4
Baby health care HC.6.4 HC.6.1 Programmes of risk avoidance HC.6.1 HC.6.4
Pre-school and school child health HC.6.4 HC.6.1
Improvement of health status not directed specifically
towards communicable disease HC.6.4 HC.6.4
Programme design, monitoring and evaluation HC.6.5
Interventions against smoking, alcohol and substance
abuse HC.6.1 HC.6.4
Regulation linked to basket of services and population
coverage on MCH, FP HC.7.1 Activities by community workers HC.6 HC.6.4
School health services HC.6.2 Services provided by self-help groups HC.6.1 HC.6.4
Education HC.6.1 HC.6.2 General health education and health information HC.6.1 HC.6.4
Screening HC.6.3 HC.6.2 Health education campaigns HC.6.1 HC.6.4
Disease prevention HC.6 HC.6.2 Campaigns in favour of health promotion (life style, sex, etc) HC.6.1 HC.6.4
Health promotion HC.6 HC.6.2 Information exchanges (alcoholism, drug addiction) HC.6.1 HC.6.4
Basic medical treatment (including dental care) HC.1 HC.6.2 Public health environmental surveillance HC.6.5 HC.6.9
Interventions against smoking, alcohol and substance
abuse (in school) HC.6.1 HC.6.2 Public information on environmental conditions HC.6.1 HC.6.9
Vaccination programmes HC.6.2 HC.6.3 Programme design, monitoring and evaluation HC.6.5
Programme design, monitoring and evaluation HC.6.5
Regulation linked to basket of services and population
coverage on non-communicable diseases HC.7.1
Regulation linked to basket of services and population
coverage on school health HC.7.1 Occupational health care HC.6.5
Prevention of communicable diseases HC.6.3 Surveillance of employee health HC.6.4 HC.6.5
Compulsory reporting and notification of diseases HC.6.5 HC.6.3 Routine medical check up HC.6.4 HC.6.5
Epidemiologic enquiries of communicable diseases HC.6.5 HC.6.3 Therapeutic care, including emergency services HC.1 HC.6.5
Trace contacts and origin of disease HC.6.5 HC.6.3 Ergonomy, safety HC.6 (health part) Excluded
Prevention of tuberculosis HC.6 HC.6.3 Health and environmental protection at work HC.6 (health part) Excluded
Tuberculosis control (screening) HC.6.3 HC.6.3 Accident prevention at work HC.6 (health part) Excluded
Immunization/vaccination (compulsory and voluntary) HC.6.2 HC.6.3 Programme design, monitoring and evaluation HC.6.5
Vaccination under maternity and child care HC.6.2 HC.6.3
Regulation linked to basket of services and population
coverage on occupational health HC.7.1
Vaccination for occupational health HC.6.2 Exc HC.6.5 All other miscellaneous public health services HC.6.9
Vaccination for travel and tourism on patient's initiative HC.1 HC.1 Operation and administration of blood and organ banks HC.4.1.2 HC.6.9
Programme design, monitoring and evaluation HC.6.5 Public health environmental surveillance HC.6.5 HC.6.9
Regulation linked to basket of services and population
coverage on communicable diseases HC.7.1 Public information on environmental conditions HC.6.1 HC.6.9

24
If data cannot be disaggregated further, then a general rule is that the aggregated expenditure
should be allocated to that area which takes the largest part of the spending.
50. For example, it may not be possible, in some countries, to disaggregate some services
such as child health or school health. If so, they should be allocated by the dominant purpose.
So if, say, the main purpose was healthy condition monitoring, the spending should be
allocated to HC.6.4.
HC.6.1
Information, education & counselling / contraception
51. Family planning and contraceptives would naturally go together. But the counselling
element would be under HC.6.1 while contraceptives are in HC.5.
52. Guidance. Unless they are an integral part of a prevention programme, any medical goods
dispensed against a prescription or purchased over the counter should be included under
HC.5, irrespective of their final purpose. Therefore, any contraceptives bought or dispensed
outside of a health system contact, e.g. doctor consultation, should be excluded from HC.6.1.
If the costs cannot be disaggregated, then they should be allocated according to whether the
counselling or the contraceptives take the larger part of the spending.
Information & education about health/safety by other ministries / public bodies
53. The UK Department for Transport has for many years produced health and safety
campaigns – for example to explain the need to wear seatbelts and to warn people about the
dangers of drinking alcohol and driving. See the example below.
“THINK! provides road safety information for road users. Our aim is to encourage safer behaviour to reduce the number of people killed and injured on our roads every year.” http://think.direct.gov.uk/index.html
_ 54. Guidance. All spending on health promotion, that aims to avoid or reduce the number or
the severity of injuries and diseases, should be included irrespective of the provider or
financing.
HC.6.2
Immunisation for tourism
55. Vaccination for travel and tourism at the patient’s initiative is allocated to treatment
(HC.1) – see table on page 23 above – whereas immunisation when not for travel and tourism
is allocated to HC6.2. The UK NHS provides (free) travel vaccines for cholera and hepatitis,
for example – so this is part of an organised NHS programme. But, of course, the patient also
has to take the initiative and tell their GP when and where they are going to travel.
56. Guidance. This exclusion from prevention was largely due to the practical issue of being
able to gather data on spending outside of organised prevention programmes. Vaccination is
always aimed at prevention. So, if expenditure is identifiable, it should be included in
HC.6.2.

25
HC.6.3
Early disease detection / prison health
57. The UK has a programme of public health expenditure in prisons. It includes, for
example, screening for hepatitis and other diseases. The activities go wider than this, but
cannot, at present, be disaggregated further.
58. Guidance. In the absence of any other information to allow disaggregation, expenditures
should be allocated to the dominant category.
HC.6.4
Health checks v. screening
59. How clear is the difference between a health check and early disease detection? Does a
health check (initiated by the health system – e.g. for all people aged 50+) for multiple
specific diseases go under HC.6.3 or HC.6.4? (e.g. if the check screens for a range of specific
factors – e.g. smoking status, blood pressure, cholesterol, drinking, etc.)
60. Guidance. There are two potential differences between HC.6.3 and HC.6.4. The first is
that “healthy monitoring” tends to be universally available for all in particular groups – e.g.
all pregnant women, or all people with teeth, can have regular check-ups. Screening
programmes (HC.6.3) tend to select a higher risk group. The second is that screening
programmes tend to try to detect a single disease – eg bowel cancer – or elevated risk of a
particular disease – eg CVD – and use a particular protocol related to that disease. Healthy
monitoring, on the other hand, would tend to look for a wider range of possible diseases or
risks.
Individual development monitoring
61. Within the UK’s NHS the main activities of “health visitors” (trained community nurses)
are the monitoring of the development of newborn infants, and young children. This was not
previously included as prevention under SHA 1.0 as it is a one-to-one service according to
individual need, rather than being seen as a “social programme”.
62. Guidance. SHA 2011 does not make the distinction between a social programme and
individual prevention services in the way that SHA 1.0 did. If it can be identified apart then it
should be included. The phrase “social programme” in SHA 1.0 (p 122) does not have a
narrow definition – e.g. it does not just mean collective provision – and a social programme
can be delivered to individuals according to their specific needs.
Healthy condition monitoring programmes
63. Does this include the monitoring of how well specific risks are controlled? For example,
borderline hypertension may be monitored. How low does a risk have to be to fit the
definition of “healthy condition”?
64. Guidance. There are two potential distinctions between HC.6.3 and HC.6.4 – the breadth
of the group included and the breadth of the disease profile considered. A focus on a
particular group – eg those at high risk of hypertension – and a focus on one particular disease
– eg CVD – would suggest that this should be classified as screening (HC.6.3).

26
HC.6.5
Incentive payments
65. The UK’s “Healthy Start” programme offers financial incentives (vouchers) for a
healthier diet – the vouchers incentivise change to a healthier diet by providing a subsidy to
purchase fruit and vegetables and other healthy foods.
66. Guidance. When the main purpose is to prevent morbidity, financial incentive payments
should be included under HC.6.5. (If, however, there was some other main purpose – eg
reducing poverty – then they should be excluded from health spending altogether.)
67. The categorisation of incentive schemes designed to change risky behaviour may not be
obvious in SHA 2011. When part of an approach to empower and encourage people to
change their behaviour, through improving their knowledge, beliefs and attitudes, perhaps
using techniques such as motivational interviewing18, these could be seen as part of
“counselling” within IEC (information, education and communication) and thus in HC.6.1.
Some schemes go beyond counselling and include rewards to participants for successful
behaviour change – e.g. a financial reward that varies according to weight lost19. In the latter
case they could be seen as part of a risk control programme, and thus in HC.6.5.
Cost-effectiveness advice
68. Should guidance on public health and prevention, from bodies such as UK’s NICE, go
under HC.6.5 (as prevention planning and evaluation) or under HC.6.1 (as advice)? Where
should other NICE guidance relating to “cure” (planning and evaluation) go?
69. Guidance When directed at specific health or risky behaviours, and where the audience
for the guidance is the public, this should be classed as HC.6.1. General guidance on the cost-
effectiveness of preventive services for use by those planning prevention programmes, and
designing the health system, should be allocated to the class HC.6.5. General guidance on the
cost-effectiveness of curative services (and the making of regulations) should be allocated to
the class HC.7.1.
HC.7.1
Regulation and enforcement within the same body
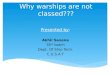
70. The UK’s Food Standards Agency’s expenditure can be allocated to different functions of
IEC, regulation, and enforcement. See Figure 3.1 below. Expenditure on the UK’s Health
and Safety Executive was not previously included under SHA 1.0. Its primary purpose is to
“prevent people being killed, injured or made ill by work” (http://www.hse.gov.uk/). It has a
mix of functions, like the Food Standards Agency. However, its expenditure is not
disaggregated by these functional classes.
71. Guidance. In the absence of any other information to allow disaggregation, expenditures
should be allocated to the dominant category.
18 Motivational interviewing attempts to increase the client's awareness of the potential problems caused,
consequences experienced, and risks faced as a result of the behaviour in question, and to improve
their motivation to change http://en.wikipedia.org/wiki/Motivational_interviewing
19 ‘The ‘Pounds for Pounds’ weight loss financial incentive scheme’, Relton et al (2011):
http://jpubhealth.oxfordjournals.org/content/early/2011/03/28/pubmed.fdr030.full

27
Figure 3.1. Spending by the UK Food Standards Agency, by type of activity20
.
Planning versus governance
72. HC.6.5 (Program design, monitoring and evaluation) is sometimes not easily
distinguishable from HC.7.1 (Governance and health system administration), as the former is
one of the principal functions of health administration.
73. Guidance. The difference between HC.6.5 and HC.7.1 could usefully be explained
further. A key difference for current purposes is whether regulations are involved –
regulations that make something mandatory or proscribe something. The health ministry and
parliament may have the power to make regulations, but other bodies may not have such
authority, in which case the activities of these other organisations could be allocated to
HC.6.5.21
20 Food Standards Agency’s resource needs for 2011-12; source: Food Standards Agency, 2011, “The Food
Standards Agency’s Strategy to 2015”:
http://www.food.gov.uk/multimedia/pdfs/strategy20102015.pdf
21 Programme is a plan of action aimed at accomplishing a clear business objective, with details on what work is to
be done, by whom, when, and what means or resources will be used. Regulation is a principle or rule (with or
without the coercive power of law) employed in controlling, directing, or managing an activity, organization, or
system. ( www.businessdictionary.com ).

28
4. CONCLUSIONS
74. Prevention is a vital investment in health. Prevention spending varies across countries,
but so do reporting methods. While SHA 2011 emphasises purpose in setting boundaries and
categories, in practice other factors may influence what is included or excluded. Important
areas touching the global boundary of health and prevention include transport safety, and
health protection and safety at work, and in the domestic environment; while environmental
health, food safety and individual behaviour touch the health-related boundary; the guidance
proposals in this paper are meant to clarify and harmonise what should be included as
prevention expenditure. Key points include: that, in non-healthcare providers, enforcement of
regulations should be classed as health-related; and except where health services invite or
encourage patients to take the initiative, other actions at the initiative of individuals, firms or
workers should normally be put outside the boundary of “healthcare”.
75. Within health spending, purpose is the key to distinguishing what should be included as
prevention, and into which prevention sub-category expenditure should be allocated.
Proposals are offered to clarify, inter alia, the treatment of patient-initiated requests,
pharmaceuticals and contraceptives, prevention in at-risk groups, and distinguishing planning
from governance.

29
REFERENCES
Commission on Social Determinants of Health (M.Marmot, chair), ‘Achieving health equity:
from root causes to fair outcomes’ The Lancet, Volume 370, Issue 9593, pp 1153-63, 29th
September 2007.
Food Standards Agency, UK, 2011, “Safer Food for the Nation: The Food Standards
Agency’s Strategy to 2015”. http://www.food.gov.uk/multimedia/pdfs/strategy20102015.pdf
Health England (R.Butterfield, J.Henderson & R.Scott), Report No 4: Public Health and
Prevention Expenditure in England. 2009.
http://www.healthengland.org/publications/HealthEnglandReportNo4.pdf
Relton, C., M.Strong & J.Li, ‘The ‘Pounds for Pounds’ weight loss financial incentive
scheme’, Journal of Public Health, 2011, pp1-7, Oxford Journals.
http://jpubhealth.oxfordjournals.org/content/early/2011/03/28/pubmed.fdr030.full
System of Health Accounts 1.0, 2000, OECD, Paris. http://www.oecd.org/health/health-
systems/21160591.pdf
System of Health Accounts 2011, 2011, OECD, Paris. http://www.oecd.org/els/health-
systems/asystemofhealthaccounts2011.htm
WHO ‘Health Systems Performance Assessment, Debates, Methods & Empiricism’ (eds
C.Murray & D.Evans), 2003, WHO Geneva. http://www.who.int/publications/2003/hspa/en/
WHO Fact Sheet on Non-Communicable Diseases, September 2011.
http://www.who.int/mediacentre/factsheets/fs355/en/index.html