Embed Size (px)
Citation preview

Existing Mechanisms, Gaps and Priorities Areas for development in
Health Sector Myanmar
Dr. Nilar Tin
Deputy Director General (Public Health)
Department of Health
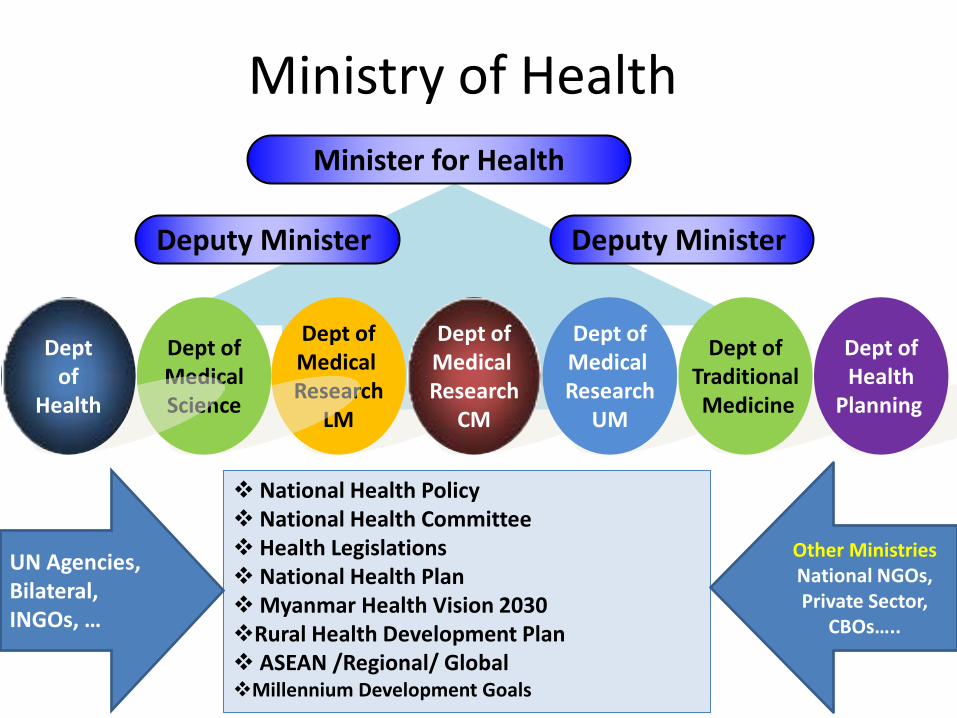
Ministry of Health Minister for Health
TEXT TEXT
Deputy Minister
Dept of Medical Research
LM
Dept of Medical Research
CM
Dept of Medical Research
UM
Dept of Medical Science
Dept of Traditional Medicine
National Health Policy National Health Committee Health Legislations National Health Plan Myanmar Health Vision 2030 Rural Health Development Plan ASEAN /Regional/ Global Millennium Development Goals
Deputy Minister
Dept of
Health
Dept of Health
Planning
UN Agencies, Bilateral, INGOs, …
Other Ministries National NGOs, Private Sector,
CBOs…..
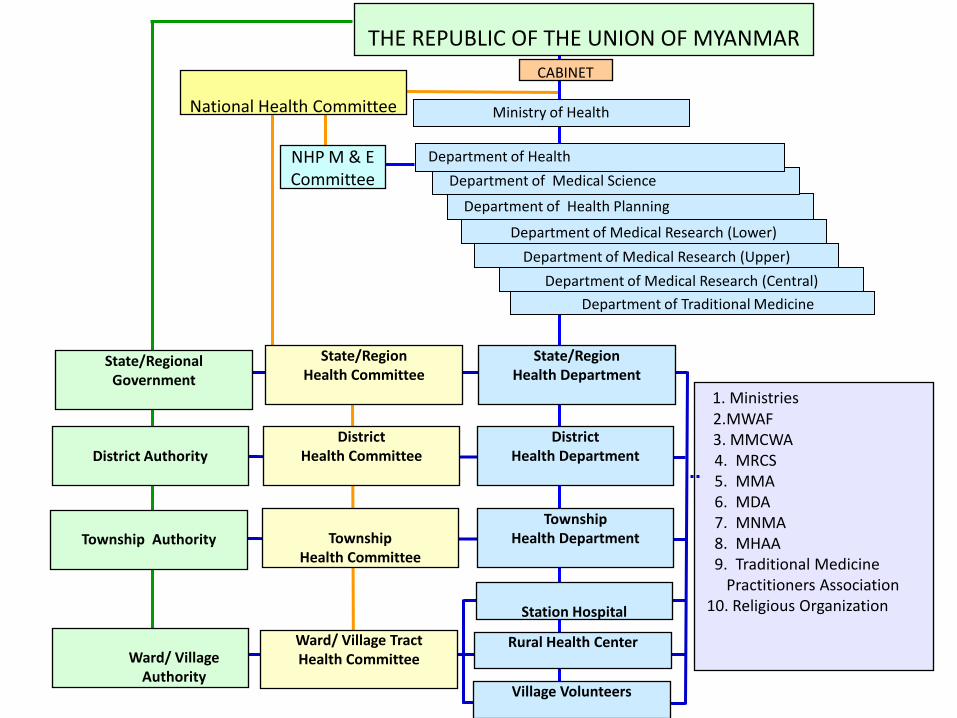
Department of Traditional Medicine
Department of Medical Research (Central)
Department of Medical Research (Upper)
Department of Medical Research (Lower)
Department of Health Planning
THE REPUBLIC OF THE UNION OF MYANMAR
NHP M & E Committee
Ministry of Health
Department of Medical Science
Department of Health
State/Regional Government
1. Ministries 2.MWAF 3. MMCWA
4. MRCS 5. MMA 6. MDA 7. MNMA 8. MHAA 9. Traditional Medicine Practitioners Association 10. Religious Organization
CABINET
District Authority
Township Authority
Ward/ Village
Authority
State/Region Health Committee
District Health Committee
Township
Health Committee
Ward/ Village Tract Health Committee
State/Region Health Department
District Health Department
Township Health Department
Station Hospital
Rural Health Center
Village Volunteers
National Health Committee
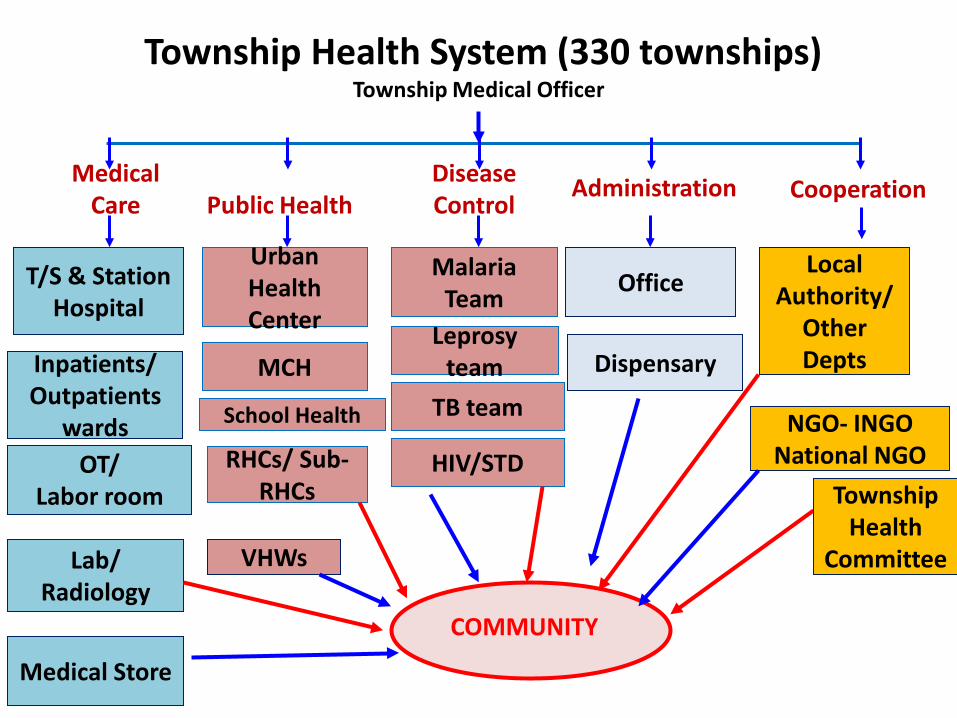
Township Health System (330 townships) Township Medical Officer
Medical Care Public Health
Disease Control
Administration Cooperation
T/S & Station Hospital
Inpatients/ Outpatients
wards OT/
Labor room
Lab/ Radiology
Medical Store
Urban Health Center
Malaria Team
Office Local
Authority/ Other Depts MCH
Leprosy team Dispensary
NGO- INGO
National NGO
School Health TB team
RHCs/ Sub-RHCs
VHWs
HIV/STD
COMMUNITY
Township Health
Committee
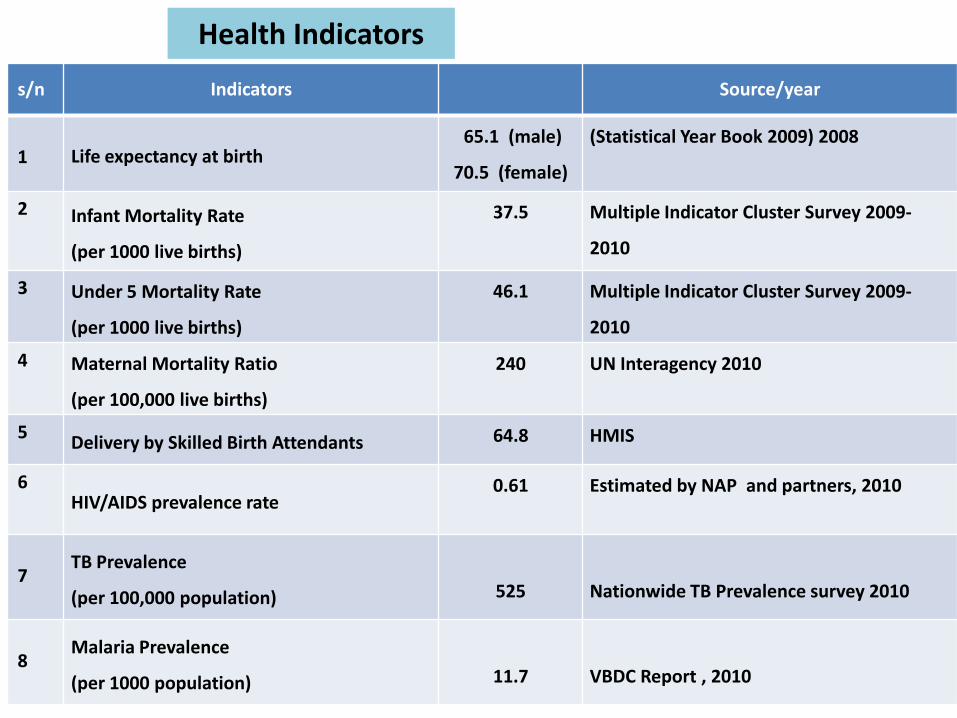
Health Indicators
s/n Indicators Source/year
1 Life expectancy at birth
65.1 (male)
70.5 (female)
(Statistical Year Book 2009) 2008
2 Infant Mortality Rate
(per 1000 live births)
37.5 Multiple Indicator Cluster Survey 2009-
2010
3 Under 5 Mortality Rate
(per 1000 live births)
46.1 Multiple Indicator Cluster Survey 2009-
2010 4 Maternal Mortality Ratio
(per 100,000 live births)
240 UN Interagency 2010
5 Delivery by Skilled Birth Attendants 64.8 HMIS
6 HIV/AIDS prevalence rate
0.61 Estimated by NAP and partners, 2010
7
TB Prevalence
(per 100,000 population)
525
Nationwide TB Prevalence survey 2010
8
Malaria Prevalence
(per 1000 population)
11.7
VBDC Report , 2010
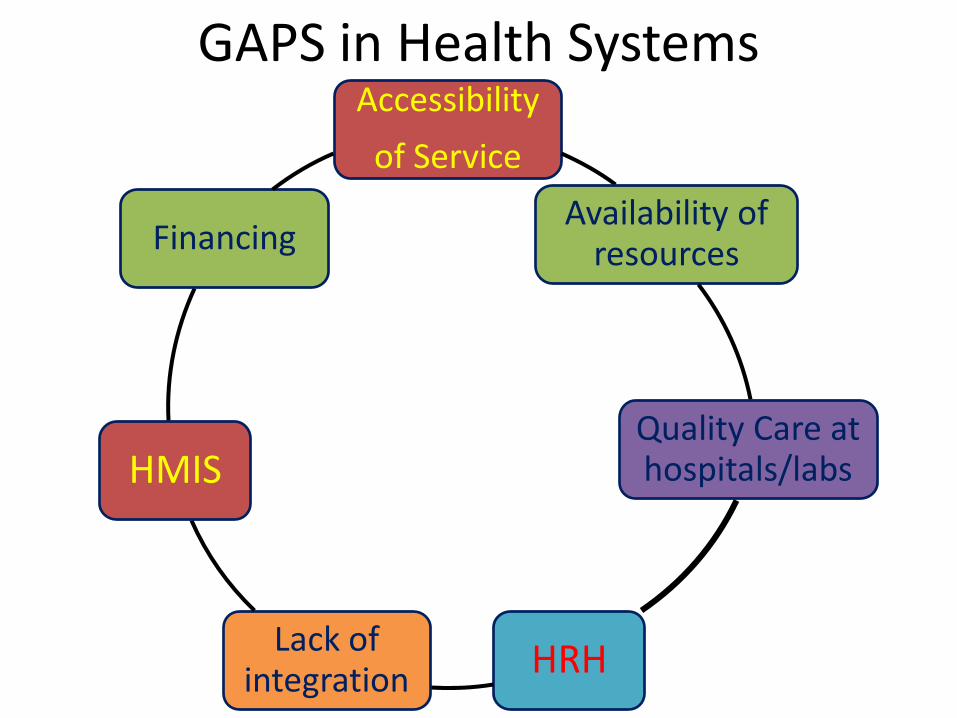
GAPS in Health Systems Accessibility
of Service
Availability of resources
Quality Care at hospitals/labs
HRH Lack of integration
HMIS
Financing
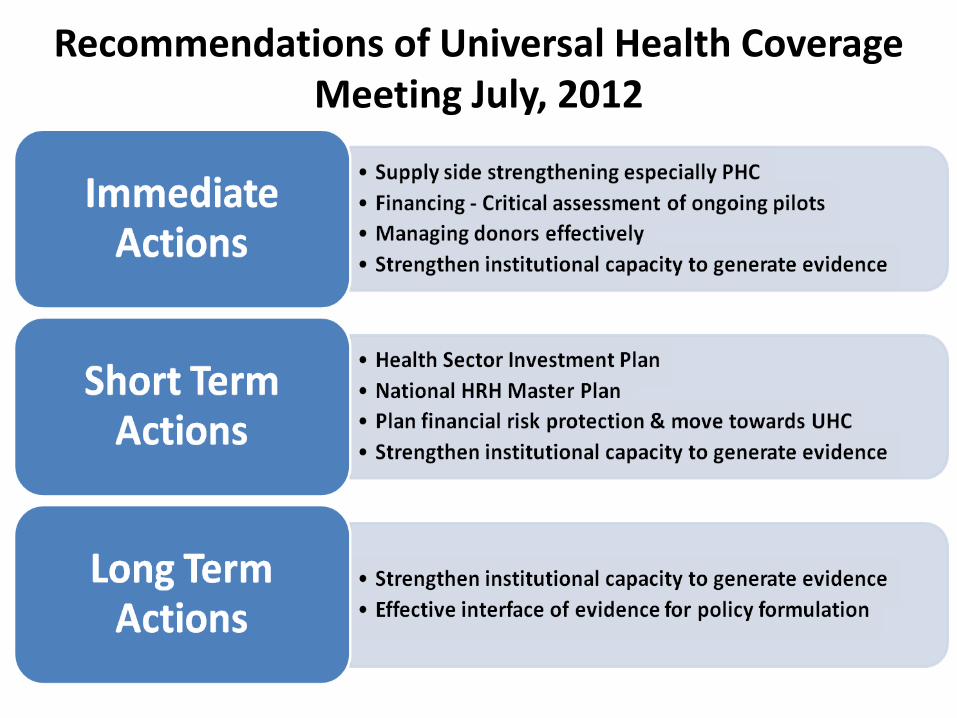
Recommendations of Universal Health Coverage Meeting July, 2012
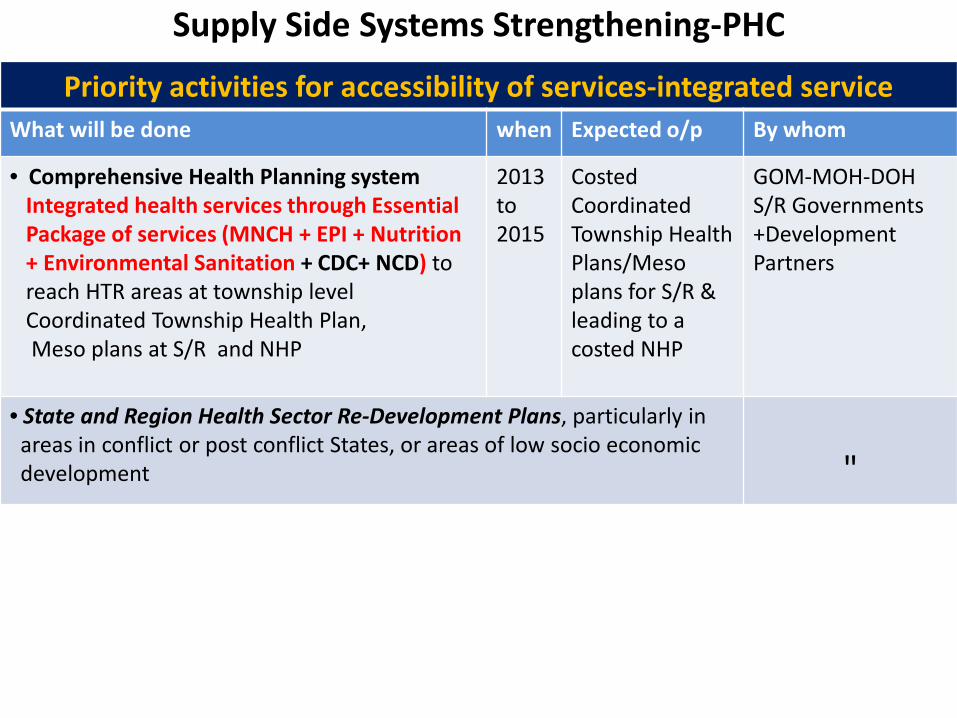
Supply Side Systems Strengthening-PHC
Priority activities for accessibility of services-integrated service What will be done when Expected o/p By whom
• Comprehensive Health Planning system Integrated health services through Essential Package of services (MNCH + EPI + Nutrition + Environmental Sanitation + CDC+ NCD) to reach HTR areas at township level Coordinated Township Health Plan, Meso plans at S/R and NHP
2013 to 2015
Costed Coordinated Township Health Plans/Meso plans for S/R & leading to a costed NHP
GOM-MOH-DOH S/R Governments +Development Partners
• State and Region Health Sector Re-Development Plans, particularly in areas in conflict or post conflict States, or areas of low socio economic development
"
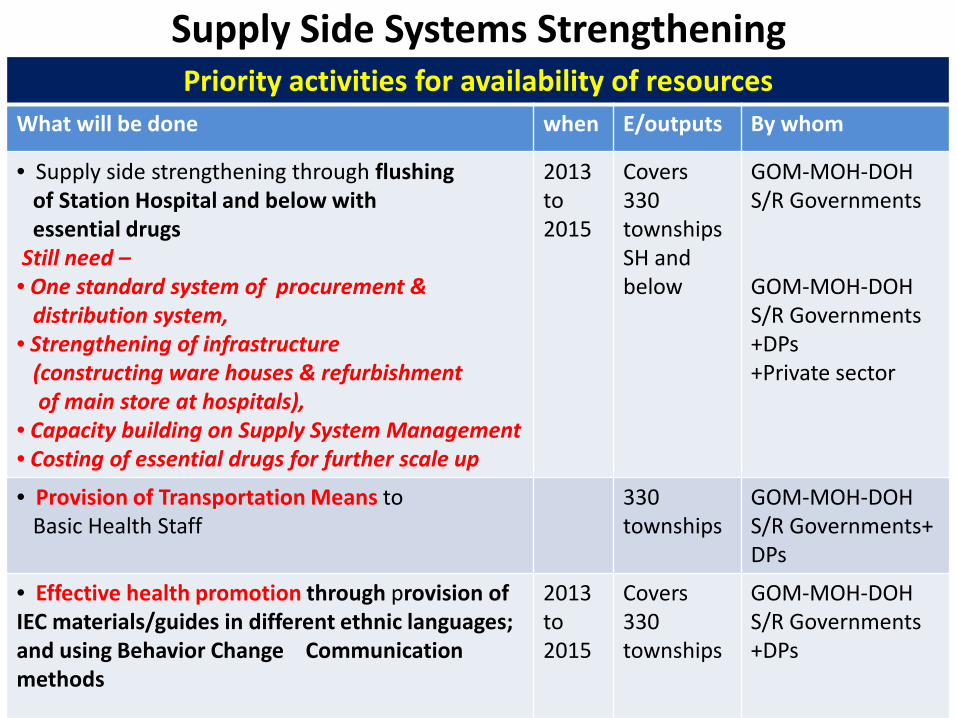
Supply Side Systems Strengthening
Priority activities for availability of resources What will be done when E/outputs By whom
• Supply side strengthening through flushing of Station Hospital and below with essential drugs Still need – • One standard system of procurement & distribution system, • Strengthening of infrastructure (constructing ware houses & refurbishment of main store at hospitals), • Capacity building on Supply System Management • Costing of essential drugs for further scale up
2013 to 2015
Covers 330 townships SH and below
GOM-MOH-DOH S/R Governments GOM-MOH-DOH S/R Governments +DPs +Private sector
• Provision of Transportation Means to Basic Health Staff
330 townships
GOM-MOH-DOH S/R Governments+ DPs
• Effective health promotion through provision of IEC materials/guides in different ethnic languages; and using Behavior Change Communication methods
2013 to 2015
Covers 330 townships
GOM-MOH-DOH S/R Governments +DPs
Gaps in Health Information System
Data Quality-not highly valid
Data Flow- still manual
Timeliness of data affecting
completeness of data
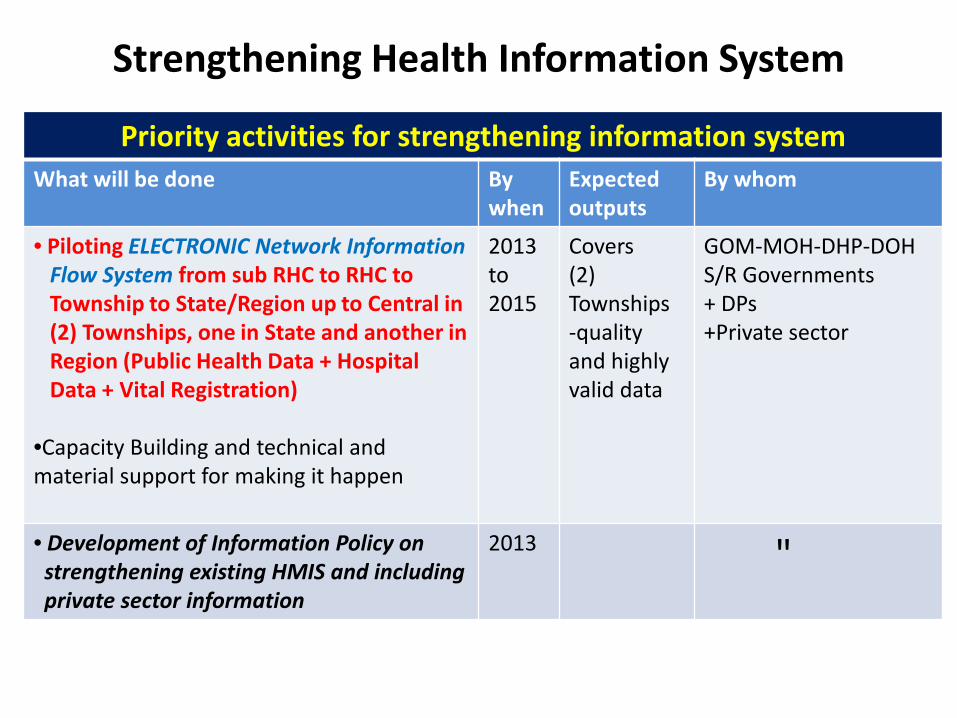
Strengthening Health Information System
Priority activities for strengthening information system What will be done By
when Expected outputs
By whom
• Piloting ELECTRONIC Network Information Flow System from sub RHC to RHC to Township to State/Region up to Central in (2) Townships, one in State and another in Region (Public Health Data + Hospital Data + Vital Registration)
•Capacity Building and technical and material support for making it happen
2013 to 2015
Covers (2) Townships -quality and highly valid data
GOM-MOH-DHP-DOH S/R Governments + DPs +Private sector
• Development of Information Policy on strengthening existing HMIS and including private sector information
2013 "
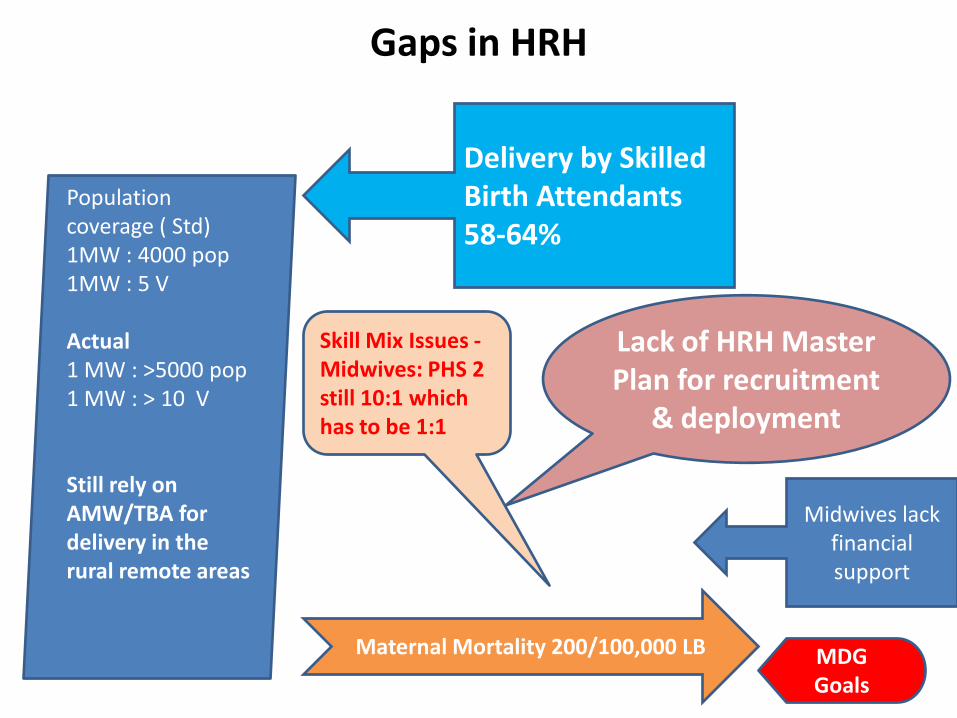
Gaps in HRH
Population coverage ( Std) 1MW : 4000 pop 1MW : 5 V Actual 1 MW : >5000 pop 1 MW : > 10 V Still rely on AMW/TBA for delivery in the rural remote areas
Delivery by Skilled Birth Attendants 58-64%
Lack of HRH Master Plan for recruitment
& deployment
Maternal Mortality 200/100,000 LB
Skill Mix Issues -Midwives: PHS 2 still 10:1 which has to be 1:1
Midwives lack financial support
MDG Goals
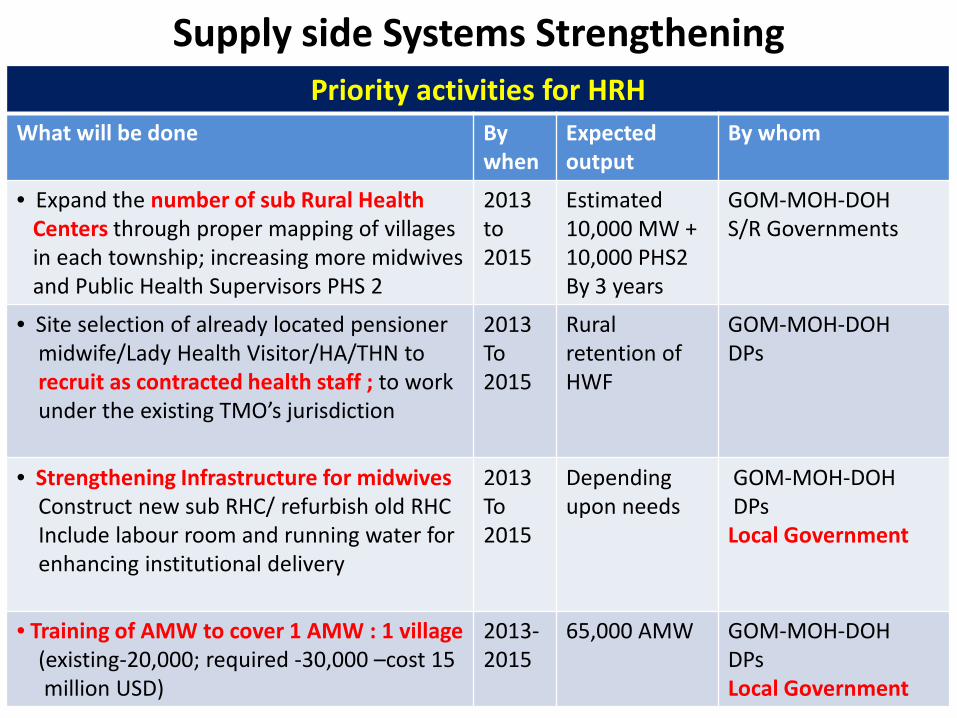
Supply side Systems Strengthening Priority activities for HRH
What will be done By when
Expected output
By whom
• Expand the number of sub Rural Health Centers through proper mapping of villages in each township; increasing more midwives and Public Health Supervisors PHS 2
2013 to 2015
Estimated 10,000 MW + 10,000 PHS2 By 3 years
GOM-MOH-DOH S/R Governments
• Site selection of already located pensioner midwife/Lady Health Visitor/HA/THN to recruit as contracted health staff ; to work under the existing TMO’s jurisdiction
2013 To 2015
Rural retention of HWF
GOM-MOH-DOH DPs
• Strengthening Infrastructure for midwives Construct new sub RHC/ refurbish old RHC Include labour room and running water for enhancing institutional delivery
2013 To 2015
Depending upon needs
GOM-MOH-DOH DPs Local Government
• Training of AMW to cover 1 AMW : 1 village (existing-20,000; required -30,000 –cost 15 million USD)
2013-2015
65,000 AMW GOM-MOH-DOH DPs Local Government
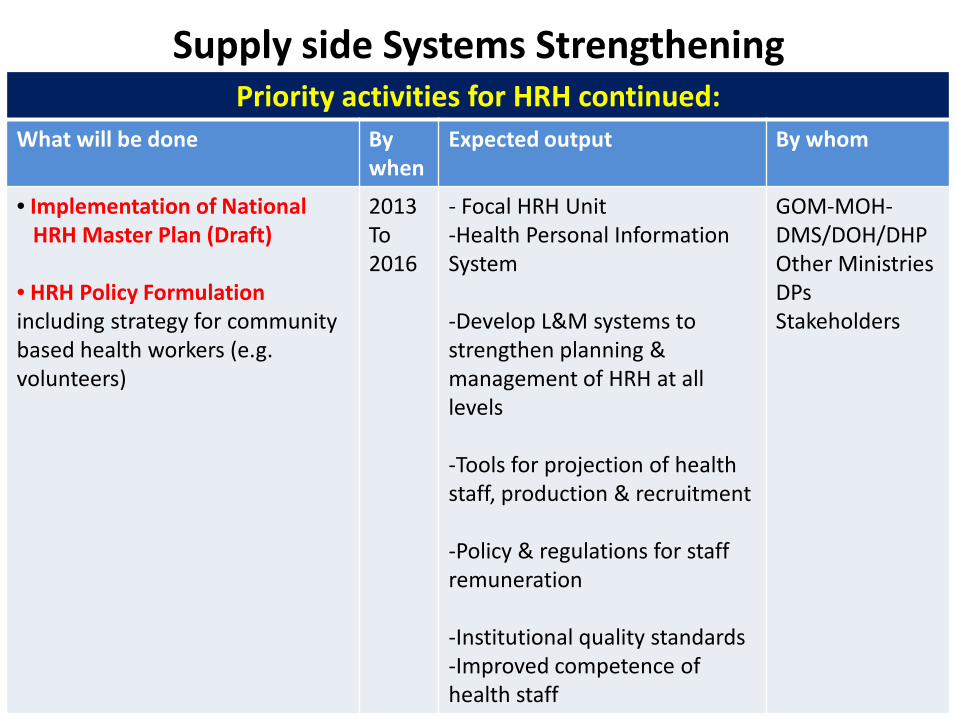
Supply side Systems Strengthening Priority activities for HRH continued:
What will be done By when
Expected output By whom
• Implementation of National HRH Master Plan (Draft) • HRH Policy Formulation including strategy for community based health workers (e.g. volunteers)
2013 To 2016
- Focal HRH Unit -Health Personal Information System
-Develop L&M systems to strengthen planning & management of HRH at all levels -Tools for projection of health staff, production & recruitment -Policy & regulations for staff remuneration -Institutional quality standards -Improved competence of health staff
GOM-MOH-DMS/DOH/DHP Other Ministries DPs Stakeholders
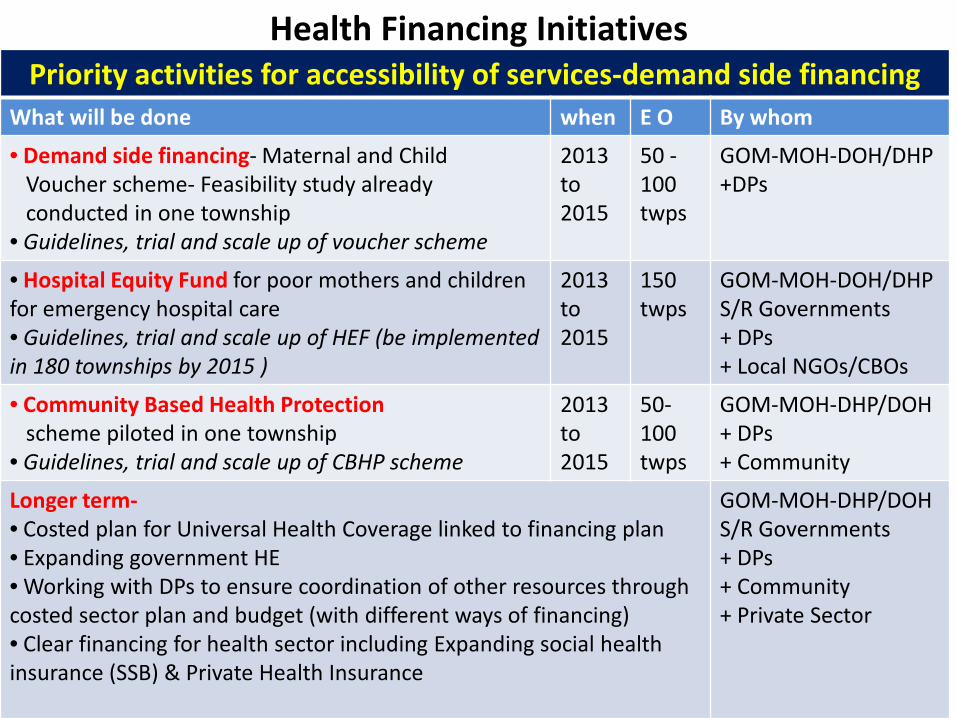
Health Financing Initiatives
Priority activities for accessibility of services-demand side financing What will be done when E O By whom
• Demand side financing- Maternal and Child Voucher scheme- Feasibility study already conducted in one township • Guidelines, trial and scale up of voucher scheme
2013 to 2015
50 -100 twps
GOM-MOH-DOH/DHP +DPs
• Hospital Equity Fund for poor mothers and children for emergency hospital care • Guidelines, trial and scale up of HEF (be implemented in 180 townships by 2015 )
2013 to 2015
150 twps
GOM-MOH-DOH/DHP S/R Governments + DPs + Local NGOs/CBOs
• Community Based Health Protection scheme piloted in one township • Guidelines, trial and scale up of CBHP scheme
2013 to 2015
50-100 twps
GOM-MOH-DHP/DOH + DPs + Community
Longer term- • Costed plan for Universal Health Coverage linked to financing plan • Expanding government HE • Working with DPs to ensure coordination of other resources through costed sector plan and budget (with different ways of financing) • Clear financing for health sector including Expanding social health insurance (SSB) & Private Health Insurance
GOM-MOH-DHP/DOH S/R Governments + DPs + Community + Private Sector
Gaps identified in Health Systems
Gaps in Quality Hospital Services
Need of high standard quality hospital services
Need of high standard imaging services
Need of high standard blood centers
Need of high standard laboratory services
Need of high quality FDA labs
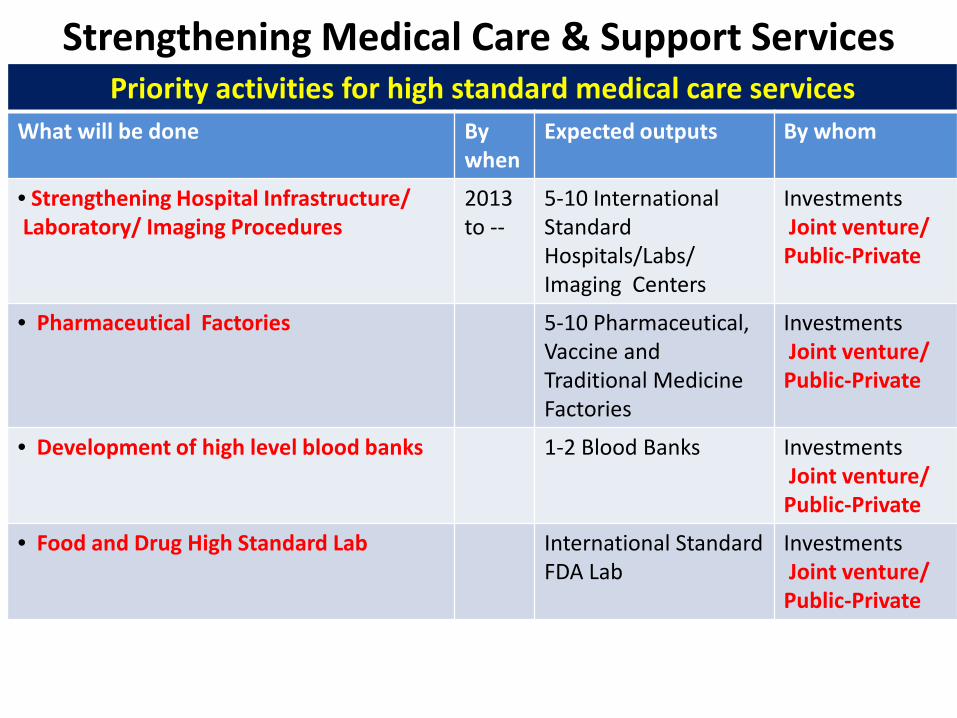
Strengthening Medical Care & Support Services Priority activities for high standard medical care services
What will be done By when
Expected outputs By whom
• Strengthening Hospital Infrastructure/ Laboratory/ Imaging Procedures
2013 to --
5-10 International Standard Hospitals/Labs/ Imaging Centers
Investments Joint venture/ Public-Private
• Pharmaceutical Factories 5-10 Pharmaceutical, Vaccine and Traditional Medicine Factories
Investments Joint venture/ Public-Private
• Development of high level blood banks 1-2 Blood Banks Investments Joint venture/ Public-Private
• Food and Drug High Standard Lab International Standard FDA Lab
Investments Joint venture/ Public-Private
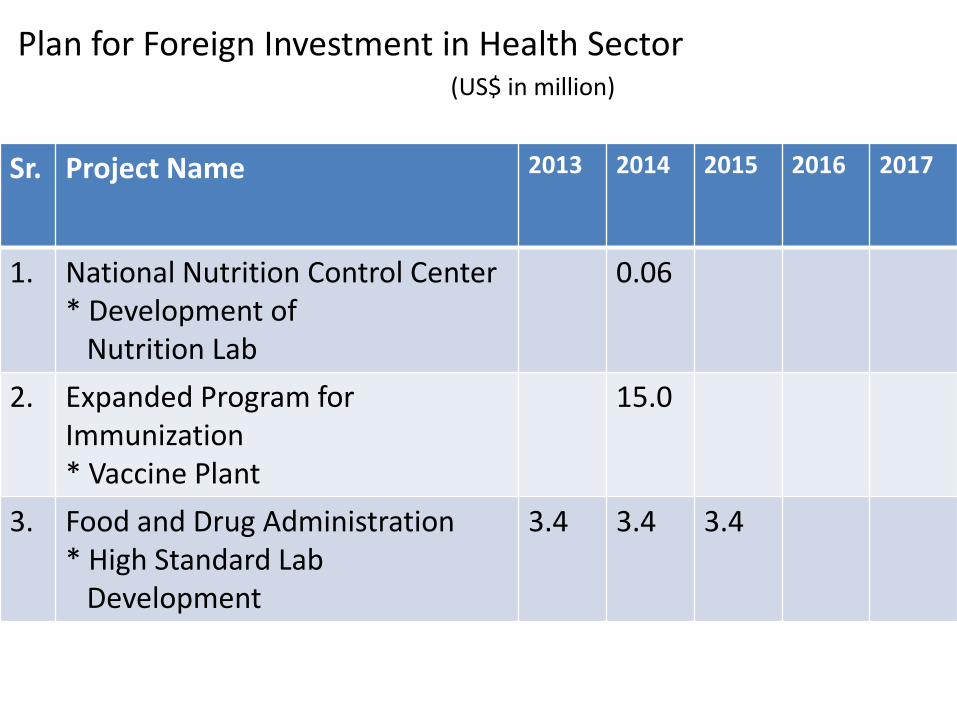
Sr. Project Name 2013 2014 2015 2016 2017
1. National Nutrition Control Center * Development of Nutrition Lab
0.06
2. Expanded Program for Immunization * Vaccine Plant
15.0
3. Food and Drug Administration * High Standard Lab Development
3.4 3.4 3.4
Plan for Foreign Investment in Health Sector (US$ in million)
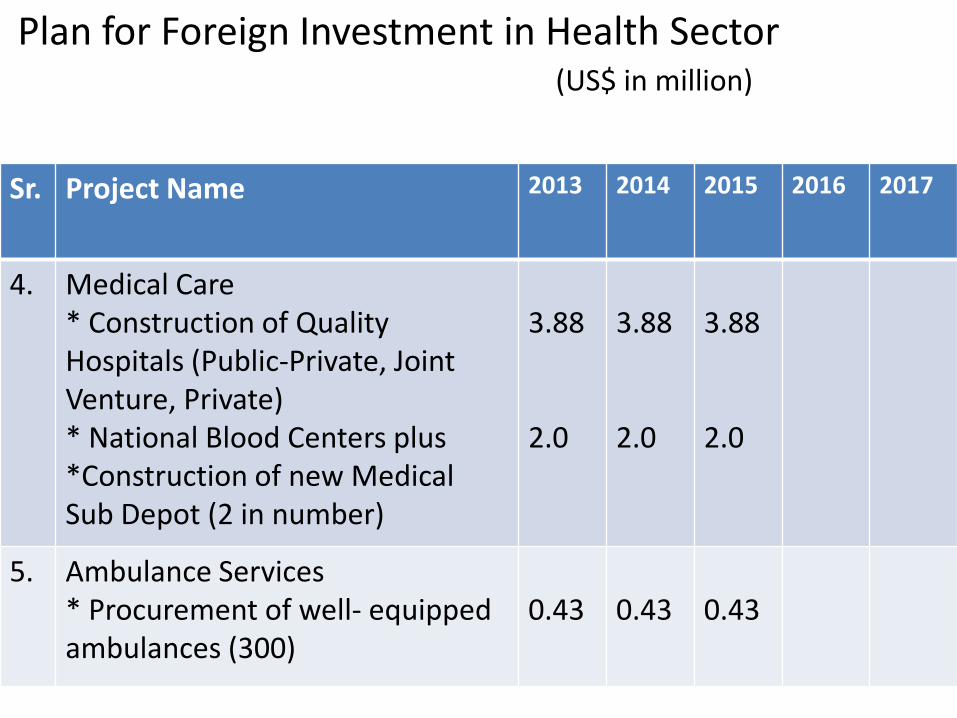
Sr. Project Name 2013 2014 2015 2016 2017
4. Medical Care * Construction of Quality Hospitals (Public-Private, Joint Venture, Private) * National Blood Centers plus *Construction of new Medical Sub Depot (2 in number)
3.88 2.0
3.88 2.0
3.88 2.0
5. Ambulance Services * Procurement of well- equipped ambulances (300)
0.43
0.43
0.43
Plan for Foreign Investment in Health Sector (US$ in million)
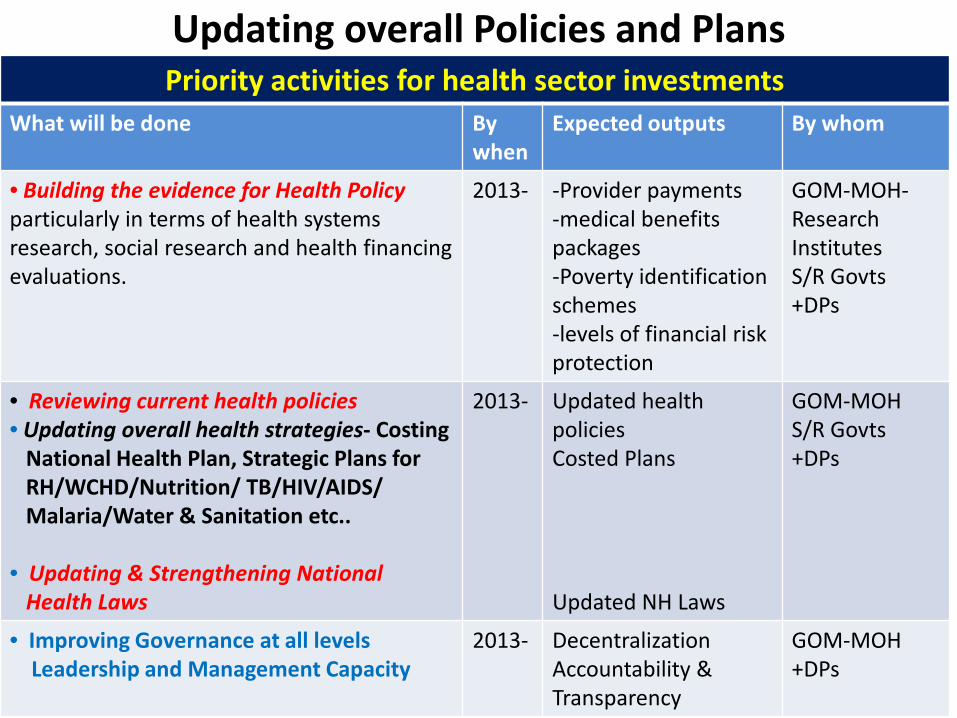
Updating overall Policies and Plans Priority activities for health sector investments
What will be done By when
Expected outputs By whom
• Building the evidence for Health Policy particularly in terms of health systems research, social research and health financing evaluations.
2013- -Provider payments -medical benefits packages -Poverty identification schemes -levels of financial risk protection
GOM-MOH-Research Institutes S/R Govts +DPs
• Reviewing current health policies • Updating overall health strategies- Costing National Health Plan, Strategic Plans for RH/WCHD/Nutrition/ TB/HIV/AIDS/ Malaria/Water & Sanitation etc.. • Updating & Strengthening National Health Laws
2013-
Updated health policies Costed Plans Updated NH Laws
GOM-MOH S/R Govts +DPs
• Improving Governance at all levels Leadership and Management Capacity
2013- Decentralization Accountability & Transparency
GOM-MOH +DPs
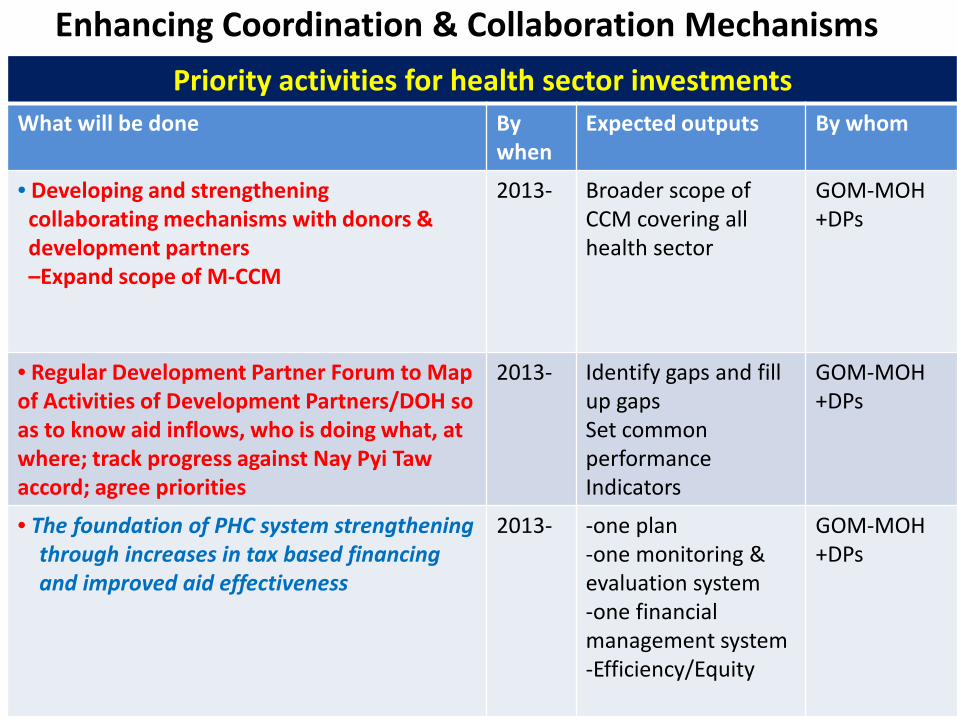
Enhancing Coordination & Collaboration Mechanisms
Priority activities for health sector investments What will be done By
when Expected outputs By whom
• Developing and strengthening collaborating mechanisms with donors & development partners –Expand scope of M-CCM
2013- Broader scope of CCM covering all health sector
GOM-MOH +DPs
• Regular Development Partner Forum to Map of Activities of Development Partners/DOH so as to know aid inflows, who is doing what, at where; track progress against Nay Pyi Taw accord; agree priorities
2013- Identify gaps and fill up gaps Set common performance Indicators
GOM-MOH +DPs
• The foundation of PHC system strengthening through increases in tax based financing and improved aid effectiveness
2013- -one plan -one monitoring & evaluation system -one financial management system -Efficiency/Equity
GOM-MOH +DPs

Thank You





























