Embed Size (px)
Citation preview

JOURNAL OF AEROSOL MEDICINEVolume 20, Number 1, 2007© Mary Ann Liebert, Inc.Pp. 13–18DOI: 10.1089/jam.2006.0567
Exhaled Breath Condensate pH Is Increased afterModerate Exercise
MICHAEL RIEDIKER, Dr.Sc.Nat. and BRIGITTA DANUSER, M.D.
ABSTRACT
Exhaled breath condensate (EBC) of patients with inflammatory diseases has a decreased pH.This could make EBC-pH an interesting tool for studying work-related inflammatoryprocesses, provided that normal work activities would not interfere with the results. We con-sequently tested whether EBC-pH was influenced by moderate exercise. Fifteen healthy non-smoking subjects exercised for 30 min on a treadmill by walking at 60% of predicted maxi-mal heart rate. Four EBC samples were obtained: one to learn the technique, one beforeexercise, one immediately after exercise, and one 60 min later. EBC-pH was significantly in-creased after exercise compared to before (mean of 8.27 vs. 8.20, p � 0.001). It remained sig-nificantly increased after 60 min (8.25, p � 0.02). The increase was strongest for the subjectswith lowest pH. All pH measures were significantly correlated with each other. Light physi-cal activity increases EBC-pH. The persistence of this increase after the end of the exerciseposes a serious challenge if one wants to use this technique for health surveys or for diag-nostic purposes. It could prevent the observation of a lowered EBC-pH that results from aninflammatory response.
Key words: human, adult, exercise, exhaled breath condensate, acidity, pH
13
INTRODUCTION
EXHALED BREATH CONDENSATE (EBC) is the liq-uid that condenses when air is exhaled
through a cooled tube. It originates from watervapor and aerosols, and contains salts and pro-teins that are common to the lung-lining liquids(reviewed in(1,2)). The disease status of patientswith chronic obstructive pulmonary disease(COPD), asthma, and cystic fibrosis is associatedwith altered levels of EBC components such asnitrite,(3) hydrogen peroxide,(4,5) aldehydes,(6,7)
nitrosothiols,(8) leukotrienes and prostaglan-dins,(9) as well as interleukins and interferon
gamma.(10) Consequently, the analysis of EBCcomponents could help obtain information aboutongoing inflammatory processes in the lungs.
Several studies consistently reported EBC to beacidified in the presence of lung inflammation,with the decrease in pH depending on the sever-ity of the disease status. In patients with stablecystic fibrosis, the pH was 0.3 to 0.5 lower com-pared to healthy controls. Exacerbation of thisdisease lowered the pH by another 0.2 to 0.5.(11–13)
For mild asthmatics, no decrease in pH was ob-served,(12,14) but the pH of moderate (by 0.3 to0.4)(11,14,15) and severe asthmatics (by 0.5)(11) waslowered compared to controls. Inhalation of cor-
Institute for Occupational Health Sciences, Lausanne, Switzerland.

ticosteroids partly reversed this acidification inasthmatics.(14,15) Reduced pH was also reportedfor COPD (by 0.4 to 0.8),(16) chronic cough (by0.4)(17) and an extreme reduction of 1.6 in pH inventilated patients with acute lung injury.(18)
Collecting EBC and measuring the pH of theliquid is a fast, noninvasive, and inexpensivemethod. This makes EBC-pH a potentially inter-esting tool for epidemiological surveys or forscreening for work-related lung diseases. Cur-rently the method lacks standardization.(2) Manymethodological questions are unsolved. This isreflected in the above-cited studies where the ab-solute pH-levels of controls as well as patientsdiffered considerably between the studies (con-trols varied between pH 6.1 and 8.3). EBC-pH stillseems to require some standardization regardingcollection and after-treatment protocols to allowcomparison of results obtained with differentmethods.
Studying the health of workers in their work en-vironment requires screening tools that are quickand easy to apply, noninvasive, and inexpensive.This all applies to EBC-pH, which makes it a po-tentially interesting tool for studying work-relatedinflammatory effects. However, before such amethod can be applied, it has to be known howstable and reproducible the results are for normalworking conditions. We therefore tested the influ-ence of light physical work activity: healthy sub-jects walked on a treadmill and EBC-pH sampleswere collected before and after the exercise.
MATERIALS AND METHODS
Subjects
The ethical committee of the Medical School ofthe University of Lausanne approved the study.All subjects gave written informed consent beforetheir participation. Subjects were recruited to beadult (18–60 years) and healthy nonsmokers. Atrained physician examined all subjects for po-tential heart, lung, or other health problems. Sub-jects had to be without heart problems, allergies,asthma, chronic bronchitis, COPD, tuberculosis,repeated pneumonias or other lung problems, notbe on any kind of medication (except contracep-tives), of normal weight with a body mass indexbetween 18 and 28 kg/m2, and nonsmokers as de-fined by not having smoked in the year before en-rollment and less than five pack-years in life.
Subjects were asked to refrain for 24 h beforethe test from caffeine, medication, alcohol, heavyexercise, and heavy air pollutant exposures (in-cluding tobacco smoke). The only beverage al-lowed in the hour before the test was water.
Study procedure
After arrival at the test facility, subjects wereinstructed about the study procedures. They wereequipped with a LifeShirt (Vivometrics, Ventura,CA) for respiration data and a heart rate trans-mitter chest belt (HorizonFitness, Frechen, Ger-many). Subjects entered a test chamber (size 3 �3 � 2.5m), which was ventilated with ambient air.At that time, a learning sample was collected tofamiliarize the subjects with the method. Subjectsbreathed for 10 min through the R-Tube collec-tion device (Respiratory Research, Charlottes-ville, VA), with the aluminum sleeve precooledto �25°C. A first real sample was collected after20 min of rest (“before exercise”). Subjects thenwalked for 30 min with a 1-min pause every 10min on a walking treadmill (Paragon II CS HRC,HorizonFitness, Frechen, Germany), which wasprogrammed to vary the slope so that the pulseremained at 60% maximal predicted heart rate(220 minus age). The second sample was collected1 min “after exercise,” the third “60 minuteslater.”
Sample analysis
EBC samples were recovered from the R-tubefollowing manufacturer guidelines and weighedon a microbalance (Mettler-Toledo, Greifensee,Switzerland). The EBC-pH was measured withinminutes after sampling: 150 �L of the sample was pipetted into a glass vial and gassed out for6 min using nitrogen gas. We found the pH to bestable after this time. The acidity was triplicatemeasured using a microelectrode pH-meter(Metrohm, Herisau, Switzerland).
Statistics
Statistics were calculated using SPlus version6.1 (Insightful Corp., Seattle, WA). The hypothe-sis to be tested was that before and after exercise,EBC-pH differed significantly. The minimal sam-ple size necessary to detect a difference equal toone standard deviation will be 10 successful runs(paired t-test at an alpha of 0.05 and a power of0.8). For the study, 15 subjects were recruited. In
RIEDIKER ET AL.14
the case of full sample validity, this would allowdetecting a difference equal to one standard de-viation at an alpha of 0.05 and a power of 0.95.For the presented analysis, groups were com-pared using the Wilcoxon exact signed-rank test.
RESULTS
Subjects
About 50 people responded by telephone to therecruitment announcements on public bulletinboards in the university and the hospital staffarea. Most of them (about 30) were excluded dur-ing the telephone interview because of allergiesor smoking, and 19 were invited for a physicalexamination. Of these, three were excluded be-cause of heart noises, and one was excluded af-ter participating because he was very nervousand lost samples while handling the collectiontubes. This left a total of 15 subjects—7 male, 8female—with valid samples. Table 1 shows thecharacteristics of the subjects. Respiration dataare available for 14 subjects because theLifeShirt’s recorder failed once. All subjects suc-cessfully walked for 30 min on the treadmill at60% of the maximal predicted heart rate. The av-
erage walking speed was 8.7 km/h with a rangeof 4.9 to 11.8 km/h.
Samples
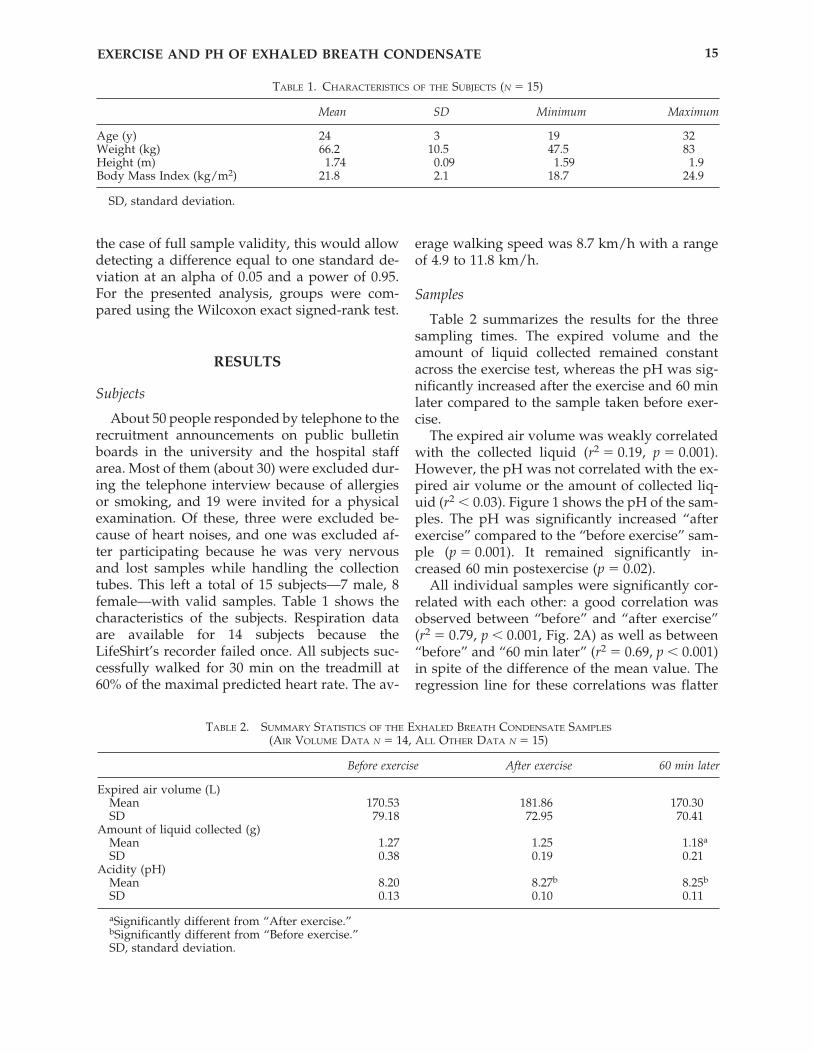
Table 2 summarizes the results for the threesampling times. The expired volume and theamount of liquid collected remained constantacross the exercise test, whereas the pH was sig-nificantly increased after the exercise and 60 minlater compared to the sample taken before exer-cise.
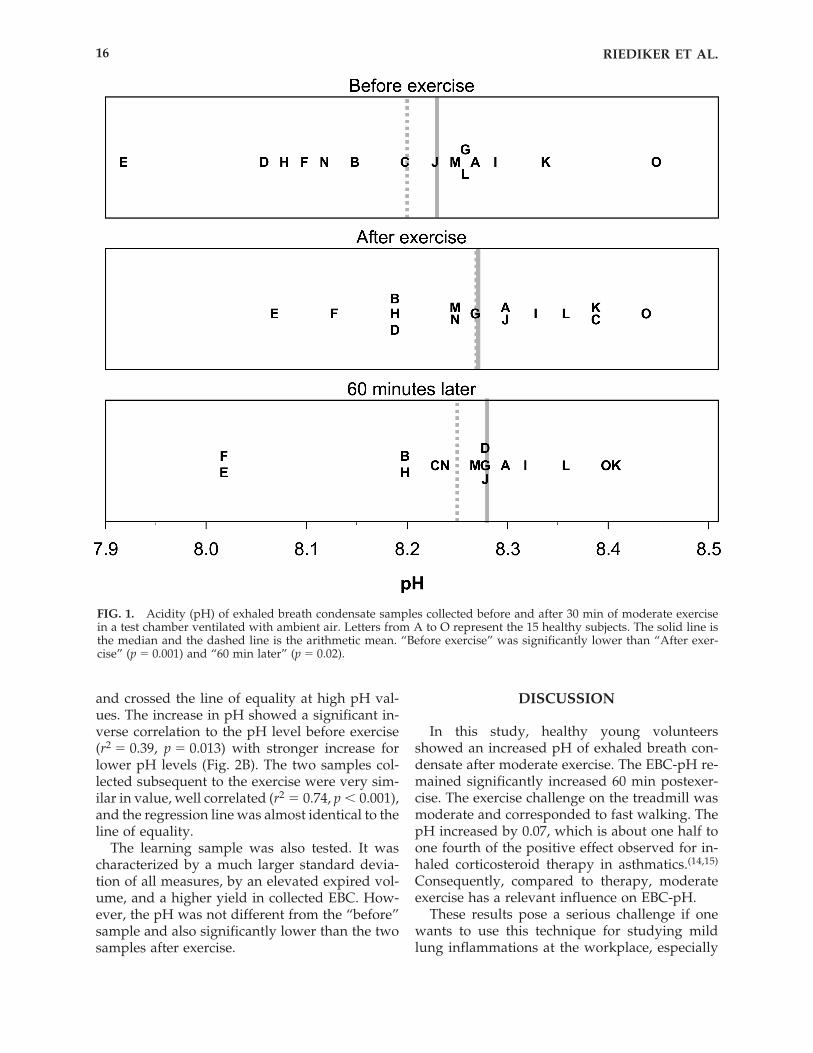
The expired air volume was weakly correlatedwith the collected liquid (r2 � 0.19, p � 0.001).However, the pH was not correlated with the ex-pired air volume or the amount of collected liq-uid (r2 � 0.03). Figure 1 shows the pH of the sam-ples. The pH was significantly increased “afterexercise” compared to the “before exercise” sam-ple (p � 0.001). It remained significantly in-creased 60 min postexercise (p � 0.02).
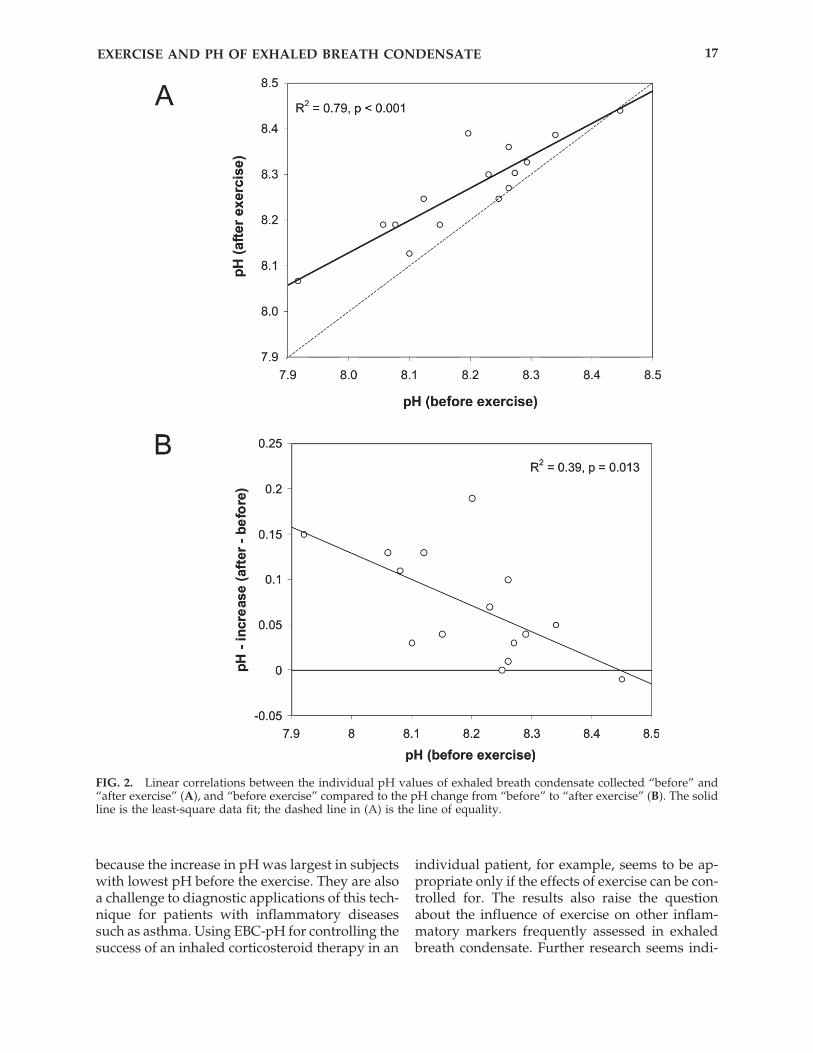
All individual samples were significantly cor-related with each other: a good correlation wasobserved between “before” and “after exercise”(r2 � 0.79, p � 0.001, Fig. 2A) as well as between“before” and “60 min later” (r2 � 0.69, p � 0.001)in spite of the difference of the mean value. Theregression line for these correlations was flatter
EXERCISE AND PH OF EXHALED BREATH CONDENSATE 15
TABLE 1. CHARACTERISTICS OF THE SUBJECTS (N � 15)
Mean SD Minimum Maximum
Age (y) 24 3 19 32Weight (kg) 66.2 10.5 47.5 83Height (m) 1.74 0.09 1.59 1.9Body Mass Index (kg/m2) 21.8 2.1 18.7 24.9
SD, standard deviation.
TABLE 2. SUMMARY STATISTICS OF THE EXHALED BREATH CONDENSATE SAMPLES
(AIR VOLUME DATA N � 14, ALL OTHER DATA N � 15)
Before exercise After exercise 60 min later
Expired air volume (L)Mean 170.53 181.86 170.30SD 79.18 72.95 70.41
Amount of liquid collected (g)Mean 1.27 1.25 1.18a
SD 0.38 0.19 0.21Acidity (pH)
Mean 8.20 8.27b 8.25b
SD 0.13 0.10 0.11
aSignificantly different from “After exercise.”bSignificantly different from “Before exercise.”SD, standard deviation.
and crossed the line of equality at high pH val-ues. The increase in pH showed a significant in-verse correlation to the pH level before exercise(r2 � 0.39, p � 0.013) with stronger increase forlower pH levels (Fig. 2B). The two samples col-lected subsequent to the exercise were very sim-ilar in value, well correlated (r2 � 0.74, p � 0.001),and the regression line was almost identical to theline of equality.
The learning sample was also tested. It wascharacterized by a much larger standard devia-tion of all measures, by an elevated expired vol-ume, and a higher yield in collected EBC. How-ever, the pH was not different from the “before”sample and also significantly lower than the twosamples after exercise.
DISCUSSION
In this study, healthy young volunteersshowed an increased pH of exhaled breath con-densate after moderate exercise. The EBC-pH re-mained significantly increased 60 min postexer-cise. The exercise challenge on the treadmill wasmoderate and corresponded to fast walking. ThepH increased by 0.07, which is about one half toone fourth of the positive effect observed for in-haled corticosteroid therapy in asthmatics.(14,15)
Consequently, compared to therapy, moderateexercise has a relevant influence on EBC-pH.
These results pose a serious challenge if onewants to use this technique for studying mildlung inflammations at the workplace, especially
RIEDIKER ET AL.16
FIG. 1. Acidity (pH) of exhaled breath condensate samples collected before and after 30 min of moderate exercisein a test chamber ventilated with ambient air. Letters from A to O represent the 15 healthy subjects. The solid line isthe median and the dashed line is the arithmetic mean. “Before exercise” was significantly lower than “After exer-cise” (p � 0.001) and “60 min later” (p � 0.02).
because the increase in pH was largest in subjectswith lowest pH before the exercise. They are alsoa challenge to diagnostic applications of this tech-nique for patients with inflammatory diseasessuch as asthma. Using EBC-pH for controlling thesuccess of an inhaled corticosteroid therapy in an
individual patient, for example, seems to be ap-propriate only if the effects of exercise can be con-trolled for. The results also raise the questionabout the influence of exercise on other inflam-matory markers frequently assessed in exhaledbreath condensate. Further research seems indi-
EXERCISE AND PH OF EXHALED BREATH CONDENSATE 17
FIG. 2. Linear correlations between the individual pH values of exhaled breath condensate collected “before” and“after exercise” (A), and “before exercise” compared to the pH change from “before” to “after exercise” (B). The solidline is the least-square data fit; the dashed line in (A) is the line of equality.

cated before EBC can be used for diagnostic pur-poses. At the moment, other tests such as exhalednitric oxide(19) seem better suited to determinelung inflammation.
ACKNOWLEDGMENTS
We would like to acknowledge Annette Af-folter (M.Sc.) and Sabine Marbet (M.Sc.) for su-pervising the exercising subjects and for measur-ing the respiration and the pH. This study wasfinanced by the “Funds for Toxicology” of ETHZurich, Switzerland and the “Fondation Univer-sitaire Romande de Santé au Travail,” Lausanne,Switzerland.
REFERENCES
1. Kharitonov, S.A., and P.J. Barnes. 2001. Exhaled mark-ers of pulmonary disease. Am. J. Respir. Crit. CareMed. 163:1693–1722.
2. Horvath, I., J. Hunt, and P.J. Barnes. 2005. Exhaledbreath condensate: Methodological recommendationsand unresolved questions. Eur. Respir. J. 26:523–548.
3. Ho, L.P., J.A. Innes, and A.P. Greening. 1998. Nitritelevels in breath condensate of patients with cystic fi-brosis is elevated in contrast to exhaled nitric oxide.Thorax 53:680–684.
4. Emelyanov, A., G. Fedoseev, A. Abulimity, K. Rudin-ski, A. Fedoulov, A. Karabanov, and P.J. Barnes. 2001.Elevated concentrations of exhaled hydrogen perox-ide in asthmatic patients. Chest 120:1136–1139.
5. Ho, L.P., J. Faccenda, J.A. Innes, and A.P. Greening.1999. Expired hydrogen peroxide in breath condensateof cystic fibrosis patients. Eur. Respir. J. 13:103–106.
6. Corradi, M., G. Folesani, R. Andreoli, P. Manini, A.Bodini, G. Piacentini, S. Carraro, S. Zanconato, and E.Baraldi. 2003. Aldehydes and glutathione in exhaledbreath condensate of children with asthma exacerba-tion. Am. J. Respir. Crit. Care Med. 167:395–399.
7. Corradi, M., I. Rubinstein, R. Andreoli, P. Manini, A.Caglieri, D. Poli, R. Alinovi, and A. Mutti. 2003. Alde-hydes in exhaled breath condensate of patients withchronic obstructive pulmonary disease. Am. J. Respir.Crit. Care Med. 167:1380–1386.
8. Corradi, M., P. Montuschi, L.E. Donnelly, A. Pesci,S.A. Kharitonov, and P.J. Barnes. 2001. Increased ni-trosothiols in exhaled breath condensate in inflam-matory airway diseases. Am. J. Respir. Crit. CareMed. 163:854–858.
9. Montuschi, P., S.A. Kharitonov, G. Ciabattoni, and P.J.Barnes. 2003. Exhaled leukotrienes and prosta-glandins in COPD. Thorax 58:585–588.
10. Shahid, S.K., S.A. Kharitonov, N.M. Wilson, A. Bush,and P.J. Barnes. 2002. Increased interleukin-4 and de-
creased interferon-gamma in exhaled breath conden-sate of children with asthma. Am. J. Respir. Crit. CareMed. 165:1290–1293.
11. Carpagnano, G.E., P.J. Barnes, J. Francis, N. Wilson,A. Bush, and S.A. Kharitonov. 2004. Breath conden-sate pH in children with cystic fibrosis and asthma:A new noninvasive marker of airway inflammation?Chest 125:2005–2010.
12. Ojoo, J.C., S.A. Mulrennan, J.A. Kastelik, A.H. Morice,and A.E. Redington. 2005. Exhaled breath condensatepH and exhaled nitric oxide in allergic asthma and incystic fibrosis. Thorax 60:22–26.
13. Tate, S., G. MacGregor, M. Davis, J.A. Innes, and A.P.Greening. 2002. Airways in cystic fibrosis are acidi-fied: Detection by exhaled breath condensate. Thorax57:926–929.
14. Kostikas, K., G. Papatheodorou, K. Ganas, K.Psathakis, P. Panagou, and S. Loukides. 2002. pH inexpired breath condensate of patients with inflam-matory airway diseases. Am. J. Respir. Crit. CareMed. 165:1364–1370.
15. Carraro, S., G. Folesani, M. Corradi, S. Zanconato, B.Gaston, and E. Baraldi. 2005. Acid-base equilibriumin exhaled breath condensate of allergic asthmaticchildren. Allergy 60:476–481.
16. Borrill, Z., C. Starkey, J. Vestbo, and D. Singh. 2005.Reproducibility of exhaled breath condensate pH inchronic obstructive pulmonary disease. Eur. Respir. J.25:269–274.
17. Niimi, A., L.T. Nguyen, O. Usmani, B. Mann, and K.F.Chung. 2004. Reduced pH and chloride levels in ex-haled breath condensate of patients with chroniccough. Thorax 59:608–612.
18. Gessner, C., S. Hammerschmidt, H. Kuhn, H.J. Sey-farth, U. Sack, L. Engelmann, J. Schauer, and H. Wirtz.2003. Exhaled breath condensate acidification in acutelung injury. Respir. Med. 97:1188–1194.
19. ATS/ERS recommendations for standardized proce-dures for the online and offline measurement of ex-haled lower respiratory nitric oxide and nasal nitricoxide, 2005. Am. J. Respir. Crit. Care Med. 171:912–930.
Received on April 22, 2006in final form, June 14, 2006
Reviewed by:Gunter Oberdörster, D.V.M., Ph.D.
Mark J. Utell, M.D.
Address reprint requests to:Michael Riediker, Dr.Sc.Nat.
Institute for Occupational Health SciencesRue du Bugnon 19
CH-1005 Lausanne, Switzerland
E-mail: [email protected]
RIEDIKER ET AL.18