-
Physical Activity of Moderate Intensity andRisk of Type 2
DiabetesA systematic review
CHRISTIE Y. JEON, BA1
R. PETER LOKKEN, BA1FRANK B. HU, MD1,2,3
ROB M. VAN DAM, PHD2
OBJECTIVE To systematically evaluate the evidence for an
association between physicalactivity of moderate intensity and risk
of type 2 diabetes.
RESEARCH DESIGN AND METHODS We searched EMBASE and Medline
throughMarch 2006 and examined reference lists of retrieved
articles. We excluded studies that did notassess physical activity
of moderate intensity independent of activities of vigorous
intensity(more than six times the resting metabolic rate).
Information on study design, participantcharacteristics, assessment
of physical activity, and outcomes and estimates of associations
wereextracted independently by two investigators. We calculated
summary relative risks (RRs) usinga random-effects model for the
highest versus the lowest reported duration of activities.
RESULTS We identified 10 prospective cohort studies of physical
activity of moderateintensity and type 2 diabetes, including a
total of 301,221 participants and 9,367 incident cases.Five of
these studies specifically investigated the role of walking. The
summary RR of type 2diabetes was 0.69 (95% CI 0.580.83) for regular
participation in physical activity of moderateintensity as compared
with being sedentary. Similarly, the RR was 0.70 (0.580.84) for
regularwalking (typically 2.5 h/week brisk walking) as compared
with almost no walking. Theassociations remained significant after
adjustment for BMI. Similar associations were observed inmen and
women and in the U.S. and Europe.
CONCLUSIONS These findings indicate that adherence to
recommendations to partici-pate in physical activities of moderate
intensity such as brisk walking can substantially reduce therisk of
type 2 diabetes.
Diabetes Care 30:744752, 2007
The prevalence of type 2 diabetes ishigh and expected to
increase dra-matically in the U.S. and worldwide(1). Type 2
diabetes is a chronic diseaseassociated with premature mortality
andvarious debilitating complications (2). In-tensive treatment
regimens can preventsome but not all complications (3). There-fore,
primary prevention efforts areclearly needed.
Moderately intense physical activi-ties, such as walking and
gardening, arethe most common forms of activity
among adults in the U.S. (4) and may bean easily adoptable,
relatively safe meansto reduce the risk of type 2 diabetes.
Ran-domized trials have shown that physicalactivity alone or in
conjunction with di-etary changes can reduce the incidence oftype 2
diabetes (58). However, the in-tensity of activity required remains
un-clear because the independent role ofmoderately intense
activities has not beendirectly examined in these trials.
Observational studies have consis-tently reported an inverse
association
between physical activity and type 2 dia-betes, but most of
these studies focusedon vigorous activities or physical activityof
various intensities combined (e.g.,9,10). In this article, we
systematicallyreview the epidemiological evidence onthe association
between physical activityof moderate intensity and risk of type
2diabetes.
RESEARCH DESIGN ANDMETHODS We searched EMBASEand Medline through
March 2006 forprospective cohort and cross-sectionalstudies
investigating the association be-tween moderately intense physical
activ-ity and incidence and prevalence of type 2diabetes. The
search terms physical ac-tivity, exercise, and walking wereused in
combination with noninsulin de-pendent diabetes mellitus, NIDDM,and
type 2 diabetes, and references listsof retrieved articles were
examined. Phys-ical activity of moderate intensity was de-fined as
requiring a metabolic equivalenttask (MET) score of 3.06.0 (11).
OneMET corresponds to the energy expendi-ture during rest (quiet
sitting). A typicalactivity of moderate intensity is briskwalking
at 5.6 km/h (3.5 miles/h) on a flatsurface requiring 3.8 MET (12).
Othercommon activities of moderate intensityinclude playing golf,
leisure bicycling at16 km/h (10 miles/h), and gardening(12).
The EMBASE and Medline searcheswere performed independently by
two in-vestigators (C.Y.J. and R.P.L.), yielding491 and 488
articles, respectively. Twoadditional relevant articles were found
byexamination of reference lists of retrievedarticles. Studies were
excluded if they didnot involve human subjects, did notpresent
age-adjusted estimates, involvedstudy populations overlapping with
otherstudies, or combined moderately intenseactivity with strenuous
or light activity.Ten prospective cohort studies (1322)and six
cross-sectional studies (2328)were eligible. Because of the large
hetero-geneity in exposure and outcome mea-sures for the
cross-sectional studies, a
From the 1Department of Epidemiology, Harvard School of Public
Health, Boston, Massachusetts; the2Department of Nutrition, Harvard
School of Public Health, Boston, Massachusetts; and the
3ChanningLaboratory, Harvard Medical School and Brigham and Womens
Hospital, Boston, Massachusetts.
Address correspondence and reprint requests to Rob M. van Dam,
Department of Nutrition, HarvardSchool of Public Health, 665
Huntington Ave., Bldg. 2, Boston, MA 02115. E-mail:
[email protected].
Received for publication 1 September 2006 and accepted in
revised form 2 December 2006.C.Y.J. and R.P.L. contributed equally
to this work.Abbreviations: MET, metabolic equivalent task.A table
elsewhere in this issue shows conventional and Systeme
International (SI) units and conversion
factors for many substances.DOI: 10.2337/dc06-1842 2007 by the
American Diabetes Association.
R e v i e w s / C o m m e n t a r i e s / A D A S t a t e m e n
t sR E V I E W
744 DIABETES CARE, VOLUME 30, NUMBER 3, MARCH 2007
-
Table
1C
ohortstudies
ofm
oderatelyintense
physicalactivityand
riskof
type2
diabetes
Leadauthor,
year(ref.)
Country
SexA
ge(years)
N/n
casesM
oderate-intensityactivity
Diabetes
assessment
Follow-up
(years)A
djustments
Helm
rich,1991(13)
U.S.
M3968
5,990/202N
onvigorous(
5M
ET
h)sports
onlyvs.no
sportsparticipation;w
alking:
15vs.
5blocks/day
Self-reportofphysician
diagnosis14
Age
Lynch,1996(14)
FinlandM
4260897/46
Activities
requiring
5.5M
ET
hfor
atleast
2h/w
eek(yes
vs.no)
OG
TT
orself-report
ofantidiabetesm
edication
4.2A
ge,BMI,baseline
glucoselevel,
durationofvigorous
activities
Hu
FB,1999(15)
U.S.
F4065
70,912/1,419W
alkingin
ME
Th/w
eekam
ongthose
who
didnot
performvigorous
activities(highest
10
ME
Th/w
eekvs.low
est
0.5M
ET
h/week
quintile)
Self-reportofphysician
diagnosis(validated)
8A
ge,BMI,sm
oking,menopausal
status,hormone
therapy,parentalhistory
ofdiabetes,alcoholuse,hypertension,hypercholesterolem
ia
Folsom,2000
(16)U
.S.F
556934,257/1,997
Frequencyofactivities
6.0
ME
Th
(4
times/
week
vs.rareor
never)
Self-reportofphysician
diagnosis12
Age,BM
I,waist-to-hip
ratio,education,sm
oking,alcoholuse,horm
onetherapy
use,fam
ilyhistory
ofdiabetes,dietary
factorsO
kada,2000(17)
JapanM
35606,013/444
Weekend
leisure-time
activity(gardening,
home
repairs,shopping)
vs.beingsedentary
duringw
eekends
OG
TT
10A
ge,BMI,alcoholuse,sm
okingstatus,hypertension,parentalhistory
ofdiabetes,weekday
physicalactivity
Wannam
ethee,2000
(18)U
.K.
M4059
5,159/196R
egularw
alkingor
recreationalactivities(gardening
andhom
erepairs)
vs.sedentary
Primary
carerecords
16.9A
ge,BMI,sm
oking,alcoholuse,socialclass,preexistingcoronary
heartdisease
Hu
FB,2001(19)
U.S.
M4075
37,918/1,058W
alkingin
ME
Th/w
eek(highest
vs.lowest
quintile)
Self-reportofphysician
diagnosis(validated)
10A
ge,smoking,parentalhistory
ofdiabetes,hypertension,BM
I,dietary
factors,vigorousexercise
Hu
G,2003
(20)Finland
M/F
356414,290/373
Leisure-time
physicalactivity
(walking,
cycling,lightgardening)
4
h/week
vs.less
Nationalregistries
12A
ge,BMI,study
year,systolicblood
pressure,smoking
status,education,other
physicalactivity
Weinstein,2004
(21)U
.S.F
45
37,878/1,361W
alking(
4h/w
eekvs.
none)Self-report
ofphysiciandiagnosis
(validated)6.9
Age,BM
I,family
historyof
diabetes,alcoholuse,smoking,
hormone
therapy,hypertension,hypercholesterolem
ia,dietaryfactors,treatm
entgroup,other
physicalactivityH
sia,2005(22)
U.S.
FPost-
menopausal
87,907/2,271W
alking(highest
10
ME
Th/w
eekvs.low
est0
ME
Th/w
eekquintile)
Self-reportof
antidiabetesm
edicaton
5.1A
ge,BMI,alcoholuse,education,
smoking
status,hypertension,hypercholesterolem
ia,dietaryfactors
ME
T
work
metabolic
rate/restingm
etabolicrate.O
GT
T,oralglucose
tolerancetest.
Jeon and Associates
DIABETES CARE, VOLUME 30, NUMBER 3, MARCH 2007 745
-
meta-analysis was only conducted for thecohort studies.
Information on study design, partici-pant characteristics,
definition of moder-ately intense physical activity, adjustmentsfor
potential confounders, and estimatesof associations were abstracted
indepen-dently by two investigators (C.Y.J. andR.P.L.). In all
studies, estimates of relativerisks (RRs) with information about
theirvariance were reported. For studies thatreported more than one
level of moder-ately intense activity, the RR for the high-est as
compared with the lowest level ofactivity was abstracted.
Statistical analysisWe used STATA version 9.1 (STATA,College
Station, TX) for all statistical anal-yses. Summary measures were
calculatedusing random-effects models, which al-low each of the
studies to estimate a dif-ferent effect size (29). P values
forheterogeneity of study results were calcu-lated using Cochrans Q
test (30). Whenavailable, we separately analyzed BMI-unadjusted and
-adjusted results from theoriginal studies to assess the role of
phys-ical activity independent of its associationwith weight. To
examine sources of het-erogeneity, we conducted
metaregressionanalysis with the log RR of studies as depen-dent
variable and country (U.S./other)and sex (male/female) as
independentvariables. We assessed potential publica-tion bias using
funnel plots, plots of RRsversus precision, and the Begg (31)
andEgger (32) tests.
RESULTS
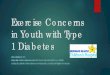
Cohort studiesWe identified 10 cohort studies on phys-ical
activity of moderate intensity and riskof type 2 diabetes,
including a total of301,221 participants and 9,367 incidentcases.
Table 1 shows the characteristics ofthe included studies. Fig. 1
shows the re-sults for moderately intense physical ac-tivity and
risk of type 2 diabetes with andwithout adjustment for BMI. For
onestudy only BMI-unadjusted (13) and forone study only
BMI-adjusted estimateswere presented (22). The summary RR oftype 2
diabetes without BMI adjustmentwas 0.69 (95% CI 0.580.83) for
thehighest as compared with the lowest cat-egory of
moderate-intensity physical ac-tivity. The BMI-adjusted RR of
diabeteswas 0.83 (0.760.90). The P value forheterogeneity in study
results was
0.001 for the BMI-unadjusted and 0.24for the BMI-adjusted
estimates.
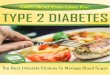
In five of the cohort studies the spe-cific role of walking was
examined(13,15,19,21,22). Figure 2 shows the re-sults for walking
and risk of type 2 diabe-tes. The BMI-unadjusted summary
RRcomparing the highest with the lowestwalking level was 0.70 (95%
CI 0.580.84), and the BMI-adjusted RR was 0.83(0.750.91). P values
for heterogeneitywere 0.08 for the BMI-unadjusted and0.68 for the
BMI-adjusted estimates. Thereported amount of walking for the
refer-ence category was minimal, and theamount in the highest
category was atleast 10 MET h/week (15,22), which isequivalent to
2.5 h/week of brisk walk-ing. Amounts of walking of 23 h/week(21),
2.13.8 MET h/week (15), and 5.110.0 MET h/week (22) have also been
as-sociated with a significantly lower risk oftype 2 diabetes as
compared with beingsedentary.
All but two studies (16,22) consid-ered confounding by vigorous
physicalactivity by adjusting for vigorous activityor excluding
participants that engaged invigorous activities. The studies that
didnot consider potential confounding byvigorous activity did not
consistently re-port stronger or weaker associations thanthe other
studies.
The Egger and Begg tests provided noevidence for publication
bias for the BMI-unadjusted (P 0.63 and P 0.84, re-spectively) and
BMI-adjusted (P 0.83and P 0.40) association between mod-erately
intense physical activity and riskof type 2 diabetes.
Characteristics of the studypopulationThe inverse association
between moder-ately intense physical activity and type 2diabetes
was observed in populationsfrom the U.S., Finland, and the U.K.
(Ta-ble 1). In the Japanese study by Okada etal. (17), no inverse
association was ob-served, but this may have been due to
themoderate-intensity activity definition thatwas restricted to
weekends, included rel-atively light-intensity activities, and
didnot consider duration. We conducted ametaregression analysis for
the associa-tion between moderate-intensity physicalactivity and
did not find significant differ-ences in results between U.S. and
non-U.S. populations (P 0.20). Thesummary RR for the U.S. studies
was 0.68(95% CI 0.560.81), while that of thenon-U.S. studies was
0.75 (0.561.00).
After excluding the study by Okada et al.(17), the RR for
non-U.S. studies was 0.66(0.540.80) and the P value for differ-ence
by region 0.96. For the BMI-adjusted RRs, the P values for
differenceby region was 0.07 before and 0.75 afterexclusion of the
study by Okada et al. Wealso evaluated potential differences bysex.
The BMI-unadjusted association be-tween moderate-intensity physical
activ-ity and diabetes risk was significantlystronger for female
(RR 0.58 [95% CI0.510.65]) than for male (0.82 [0.700.96]) cohorts
(P 0.04). However, afterexcluding the study by Okada et al., theRR
for male cohorts became 0.77 (95% CI0.670.88) and the difference
with thefemale cohorts no longer statistically sig-nificant (P
0.36). For the BMI-adjustedRRs, the P values for differences
betweenmale and female cohorts was 0.17 beforeand 0.81 after
exclusion of the study byOkada et al.
Cross-sectional studiesSix cross-sectional studies that
examinedthe association between moderately in-tense activities and
type 2 diabetes or im-paired glucose tolerance (Table 2)
wereidentified. Results from two Dutch stud-ies suggested inverse
associations for gar-dening and bicycling (which tends to beof easy
pace in this population) but not forwalking (24,26). In a French
study, par-ticipation in moderately intense house-hold activities
was inversely associatedwith type 2 diabetes (25). Two other
stud-ies were consistent with an inverse asso-ciation between
moderately intenseactivities and type 2 diabetes, but CIswere wide
(23,27). In an Australianstudy, 2.5 h/week of moderately
intenseactivities as compared with less timespent on these
activities tended to be as-sociated with a lower prevalence of
abnor-mal glucose metabolism in women butnot in men (28).
CONCLUSIONS In our meta-analysis of 10 prospective cohort
studies,a substantial inverse association was ob-served between
physical activity of mod-erate intensity and risk of type 2
diabetes.Those who regularly engaged in physicalactivity of
moderate intensity had 30%lower risk of type 2 diabetes as
comparedwith sedentary individuals. A similar de-crease in diabetes
risk was observed whenwe specifically examined regular
walking.After adjustment for BMI, the reduction indiabetes risk
remained substantial (17%)
Physical activity and type 2 diabetes
746 DIABETES CARE, VOLUME 30, NUMBER 3, MARCH 2007
-
for both regular moderately intense activ-ity and walking.
Significant inverse associations wereobserved in both men and
women and in
both U.S. and Northern European co-horts. Most studies were
conducted inpredominantly white populations. Nosignificant
association between moderate-
intensity physical activity and type 2 dia-betes was observed in
the two studies thatreported results for other ethnic groups,but
this may have been due to the light
Figure 1RRs for total physical activity of moderate intensity
and incidence of type 2 diabetes for individual cohort studies and
all studies combinedwithout adjustment for BMI (A) and with
adjustment for BMI (B). RR comparing the highest with the lowest
reported level of moderate-intensityactivity are shown in Table 1.
Filled bars and open diamonds indicate 95% CIs. The size of the
squares corresponds to the weight of the study in
themeta-analysis.
Jeon and Associates
DIABETES CARE, VOLUME 30, NUMBER 3, MARCH 2007 747
-
definition of activity (17) and limited sta-tistical power as a
result of lower numbersfor nonwhites (22). In the Diabetes
Pre-vention Program, the lifestyle interven-tion that focused on
both diet and
physical activity resulted in a similar re-duction in incidence
of type 2 diabetes inparticipants of African-American, His-panic,
American-Indian, and Asian eth-nicity as compared with whites
(6,33).
Results from cross-sectional studieswere generally consistent
with an inverseassociation between moderately intensephysical
activity and type 2 diabetes. Re-sults were more heterogeneous than
for
Figure 2RRs for walking and incidence of type 2 diabetes for
individual cohort studies and all studies combined without
adjustment for BMI (A)and with adjustment for BMI (B). RR comparing
the highest with the lowest reported level of walking are shown in
Table 1. Filled bars and opendiamonds indicate 95% CIs. The size of
the squares corresponds to the weight of the study in the
meta-analysis.
Physical activity and type 2 diabetes
748 DIABETES CARE, VOLUME 30, NUMBER 3, MARCH 2007
-
Table
2C
ross-sectionalstudiesof
moderately
intensephysicalactivity
andrisk
oftype
2diabetes
Leadauthor,
year(ref.)
Country
SexA
ge(years)
N/n
casesO
utcome
assessment
Classification
moderate-
intensityactivity
OR
(95%C
I)A
djustments
James,1998
(23)U
.S.M
/F3055
916/78T
ype2
diabetes:FBGor
useof
antidiabetesm
edicationW
alkingfor
15
min
ata
time
orhom
em
aintenance/gardeningvs.inactive
0.51(0.201.28)
Age,sex,education,BM
I,w
aist-to-hipratio
Baan,1999(24)
Netherlands
M5575
503/69T
ype2
diabetes:2-hpostload
glucoseor
useofantidiabetes
medication
Walking
(285
vs.60
min/w
eek)1.45
(0.633.32)A
ge,BMI,w
aist-to-hipratio,
family
historyofdiabetes,
smoking
Bicycling(yes
vs.no)0.26
(0.140.49)G
ardening(yes
vs.no)0.56
(0.291.06)F
5575513/49
Same
asm
aleparticipants
Walking
(270
vs.45
min/w
eek)1.05
(0.472.36)Sam
eas
male
participants
Bicycling(yes
vs.no)0.37
(0.180.78)G
ardening(yes
vs.no)0.46
(0.211.01)D
efay,2001(25)
FranceM
60
1,113/213T
ype2
diabetes:FBGor
useof
antidiabetesm
edicationU
sualintensityof
householdactivities
(moderate
vs.light)
0.67(0.480.94)
None
F
601,419/132
Same
asm
aleparticipants
Usualintensity
ofhousehold
activities(m
oderatevs.light)
0.61(0.400.95)
None
vanD
am,
2002(26)
Netherlands
M6989
424/90IG
Tor
newly
detectedtype
2diabetes:O
GT
TT
akingw
alks(
20m
in/day
vs.none)0.92
(0.461.88)A
ge,otherphysicalactivities
Bicycling(
20m
in/dayvs.none)
0.37(0.200.70)
Gardening
(20
min/day
vs.none)0.33
(0.160.66)
Com
be,2004
(27)France
M2074
3,759/299N
ewly
detectedtype
2diabetes:
FBGW
alking
1h/day
(yesvs.no)
0.81(0.641.04)
None
Dunstan,2004
(28)A
ustraliaM
25
8,299/1,555(m
enand
wom
en)IFG
,IGT
,ornew
lydetected
type2
diabetes:OG
TT
Walking
andother
moderate-intensity
activities(
2.5vs.
2.5
h/week)
0.96(0.661.40)
Age,sex,education,fam
ilyhistory
ofdiabetes,sm
oking,dietaryfactors,
TV
watching,w
aistcircum
ferenceF
25
Same
asm
aleparticipants
Walking
andother
moderate-intensity
activities(
2.5vs.
2.5
h/week)
0.73(0.531.01)
Same
asm
aleparticipants
FBP,fastingblood
glucose;IFG,im
pairedfasting
glucose;IGT
,impaired
glucosetolerance;O
GT
T,oralglucose
tolerancetest.
Jeon and Associates
DIABETES CARE, VOLUME 30, NUMBER 3, MARCH 2007 749
-
the prospective studies, possibly as a re-sult of the smaller
study sizes and differ-ences in the activity classification. In
twocross-sectional studies of Dutch elderly,no association was
observed for walking,whereas other moderately intense activi-ties
were inversely association with type 2diabetes (24,26). This lack
of associationfor walking may have reflected a loweraverage walking
pace in these elderlypopulations. A brisk usual walking pacewas
associated with a substantially lowerrisk of type 2 diabetes
compared with aneasy pace in two U.S. studies (15,19).
Strengths and limitations of the dataBecause our meta-analysis
included onlyobservational studies, it is possible thatthe summary
estimates were influencedby confounding and other biases. Al-though
all studies adjusted for age, not alladjusted for known or
suspected diabetesrisk factors such as dietary factors,
alcoholconsumption, cigarette smoking, andwaist-to-hip ratio. The
inverse associationwas similar in studies with the most com-plete
adjustment for confounding, but wecannot fully exclude residual
confound-ing by unmeasured or imprecisely mea-sured diabetes risk
factors. Lack ofadjustment for light-intensity physical ac-tivity
or sedentary activities may also haveresulted in residual
confounding (15,19).Furthermore, the included studies mostlyfocused
on leisure time physical activity,but commuting and occupational
activi-ties can also contribute importantly to theaccumulation of
moderately intensephysical activity for the reduction of dia-betes
risk (20,34).
The prospective design of the cohortstudies and low loss to
follow-up in moststudies reduced the likelihood of selec-tion bias.
Some misclassification of mod-erate-intensity physical activity
probablyoccurred, but it seems unlikely that thismisclassification
differed by future diabe-tes outcome, and it can thus be expectedto
have biased estimates of associationstoward the null. In the
studies that reliedupon self-report of a physicians diagnosisof
diabetes, differences in detection of di-abetes associated with
physical activitycould have led to diagnostic bias. This isunlikely
given that several cross-sectionalstudies measured glucose
concentrationsin all participants, and restriction tosymptomatic
cases did not substantiallyaffect the results in a cohort study
(15).We did not find any evidence of publica-tion bias based on the
Egger and Begg testand the funnel plot. However, the power
of these tests is known to be limited (35),and we cannot fully
exclude the possibil-ity that publication bias has affected
ourresults.
MechanismsWe found a significant inverse associationbetween
moderately intense physical ac-tivity and type 2 diabetes that
persistedafter adjustment for BMI. In line with thisfinding,
biological mechanisms have beenidentified for beneficial effects of
physicalactivity on glucose metabolism indepen-dent of body
fatness. Exercise has beenshown to increase insulin-stimulated
gly-cogen synthesis through an increased rateof insulin-stimulated
glucose transport byGLUT4 glucose transporters and in-creased
glycogen synthase activity (36).In addition, elevated capillary
prolifera-tion in muscles, increased muscle mass,and a higher
proportion of more insulin-sensitive types of muscle fibers may
con-tribute to beneficial effects of physicalactivity on insulin
sensitivity (37).
Findings from intervention studiesNo large randomized trials
have specifi-cally investigated the effect of increasingphysical
activity of moderate intensity onincidence of type 2 diabetes. A
random-ized trial of moderate-intensity physicalactivity in
individuals with a family his-tory of diabetes did not find a
significantreduction in incidence of type 2 diabetesafter 2 years,
but compliance with theprogram was poor and the number of
par-ticipants small (n 37 in the exerciseprogram) (38). In a 2-year
randomizedcontrolled trial in 179 individuals withtype 2 diabetes,
counseling to achieve 10MET h/ week of moderately intense phys-ical
activity resulted in significantly re-duced body weight and fasting
glucoseand A1C concentrations (39). In a posthoc analysis, a
significant reduction inA1C was observed for participants
thatincreased 1120 MET h/week, but greaterbeneficial effects were
observed in thosewho increased their activity with 2130MET h/week
(39). Several randomizedcontrolled trials tested the effects of
briskwalking on glucose metabolism in indi-viduals without diabetes
(40 42). In-creased walking resulted in reducedplasma insulin
(40,41) or glucose (42)concentrations after 1224 weeks.
A Chinese trial in individuals withimpaired glucose tolerance
found thatthose randomized at the clinic level to acombination of
moderate and vigorousactivities had a 47% reduction in inci-
dence of type 2 diabetes as compared withthe control group (7).
A post hoc analysisof the Finnish Diabetes Prevention Studyexamined
the association between walk-ing during follow-up and incidence
oftype 2 diabetes. After adjustment forother activities, dietary
factors, and BMI,at least 2.5 h/week of walking for exercisewas
associated with a 63% lower risk oftype 2 diabetes as compared with
1h/week (43). In addition, an increase inwalking intensity was
associated with alower risk of type 2 diabetes.
RecommendationsOur systematic review indicates that reg-ular
participation in moderately intensephysical activity is associated
with a sub-stantially lower risk of type 2 diabetes.The association
was partly independent ofBMI, suggesting that
moderate-intensityphysical activity can reduce the risk oftype 2
diabetes even in those who do notachieve weight loss. Findings from
severalprospective studies (15,21,22,43) indi-cate that 30 min or
more of daily moder-ate-intensity activity, as recommended
inmultiple U.S. guidelines (11,44), can sub-stantially reduce the
risk of type 2 diabe-tes as compared with being
sedentary.Moderately intense activity as defined inguidelines (3.0
6.0 MET h) (11) in-cludes walking at brisk pace but not walk-ing at
an easy or casual pace (12), andwalking at brisk pace also seems
prefera-ble for the prevention of type 2 diabetes(15,19,43).
Further studies are needed todefine more specifically what
combina-tions and duration and pace are optimalfor reducing the
risk of type 2 diabetes.However, given that only 31% of adults
inthe U.S. currently meet the general phys-ical activity
recommendations (45), ef-forts to prevent type 2 diabetes
shouldstrongly emphasize the benefit of moder-ately intense
physical activities and en-courage wider participation in
theseactivities.
References1. Wild S, Roglic G, Green A, Sicree R, King
H: Global prevalence of diabetes: esti-mates for the year 2000
and projectionsfor 2030. Diabetes Care 27:10471053,2004
2. Nathan DM: Long-term complicationsof diabetes mellitus. N
Engl J Med 328:16761685, 1993
3. Intensive blood-glucose control with sul-phonylureas or
insulin compared withconventional treatment and risk of
com-plications in patients with type 2 diabetes
Physical activity and type 2 diabetes
750 DIABETES CARE, VOLUME 30, NUMBER 3, MARCH 2007
-
(UKPDS 33): UK Prospective DiabetesStudy (UKPDS) Group. Lancet
352:837853, 1998
4. Crespo CJ, Keteyian SJ, Heath GW, Sem-pos CT: Leisure-time
physical activityamong US adults: results from the ThirdNational
Health and Nutrition Examina-tion Survey. Arch Intern Med
156:9398,1996
5. Tuomilehto J, Lindstrom J, Eriksson JG,Valle TT, Hamalainen
H, Ilanne-ParikkaP, Keinanen-Kiukaanniemi S, Laakso M,Louheranta A,
Rastas M, Salminen V,Uusitupa M: Prevention of type 2
diabetesmellitus by changes in lifestyle amongsubjects with
impaired glucose tolerance.N Engl J Med 344:13431350, 2001
6. Knowler WC, Barrett-Connor E, FowlerSE, Hamman RF, Lachin JM,
Walker EA,Nathan DM: Reduction in the incidence oftype 2 diabetes
with lifestyle interventionor metformin. N Engl J Med
346:393403,2002
7. Pan XR, Li GW, Hu YH, Wang JX, YangWY, An ZX, Hu ZX, Lin J,
Xiao JZ, CaoHB, Liu PA, Jiang XG, Jiang YY, Wang JP,Zheng H, Zhang
H, Bennett PH, HowardBV: Effects of diet and exercise in
prevent-ing NIDDM in people with impaired glu-cose tolerance: the
Da Qing IGT andDiabetes Study. Diabetes Care 20:537544, 1997
8. Ramachandran A, Snehelatha C, Mary S,Mukesh B, Bhaskar AD,
Vijay V, IndianDiabetes Prevention Program: The IndianDiabetes
Programme shows that lifestylemodifications and metformin
preventtype 2 diabetes in Asian Indian subjectswith impaired
glucose tolerance (IDPP-1). Diabetologia 49:289297, 2006
9. Manson JE, Nathan DM, Krolewski AS,Stampfer MJ, Willett WC,
HennekensCH: A prospective study of exercise andincidence of
diabetes among US malephysicians. JAMA 268:6367, 1992
10. Meisinger C, Lowel H, Thorand B, DoringA: Leisure time
physical activity andthe risk of type 2 diabetes in men andwomen
from the general population: theMONICA/KORA Augsburg Cohort
Study.Diabetologia 48:2734, 2005
11. Pate RR, Pratt M, Blair SN, Haskell WL,Macera CA, Bouchard
C, Buchner D, Et-tinger W, Heath GW, King AC, et al.:Physical
activity and public health: a rec-ommendation from the Centers for
Dis-ease Control and Prevention and theAmerican College of Sports
Medicine.JAMA 273:402407, 1995
12. Ainsworth BE, Haskell WL, Whitt MC, Ir-win ML, Swartz AM,
Strath SJ, OBrienWL, Bassett DR Jr, Schmitz KH, Emplain-court PO,
Jacobs DR Jr, Leon AS: Com-pendium of physical activities: an
updateof activity codes and MET intensities. MedSci Sports Exerc
32:S498S504, 2000
13. Helmrich SP, Ragland DR, PaffenbargerRS Jr: Prevention of
non-insulin-depen-
dent diabetes mellitus with physical activ-ity. Med Sci Sports
Exerc 26:824830, 1994
14. Lynch J, Helmrich SP, Lakka TA, KaplanGA, Cohen RD, Salonen
R, Salonen JT:Moderately intense physical activities andhigh levels
of cardiorespiratory fitness re-duce the risk of
non-insulin-dependentdiabetes mellitus in middle-aged men.Arch
Intern Med 156:13071314, 1996
15. Hu FB, Sigal RJ, Rich-Edwards JW, Cold-itz GA, Solomon CG,
Willett WC, SpeizerFE, Manson JE: Walking compared withvigorous
physical activity and risk of type2 diabetes in women: a
prospective study.JAMA 282:14331439, 1999
16. Folsom AR, Kushi LH, Hong CP: Physicalactivity and incident
diabetes mellitus inpostmenopausal women. Am J Public
Health90:134138, 2000
17. Okada K, Hayashi T, Tsumura K, Sue-matsu C, Endo G, Fujii S:
Leisure-timephysical activity at weekends and the riskof type 2
diabetes mellitus in Japanesemen: the Osaka Health Survey.
DiabetMed 17:5358, 2000
18. Wannamethee SG, Shaper AG, AlbertiKG: Physical activity,
metabolic factors,and the incidence of coronary heart dis-ease and
type 2 diabetes. Arch Intern Med160:21082116, 2000
19. Hu FB, Leitzmann MF, Stampfer MJ,Colditz GA, Willett WC,
Rimm EB: Phys-ical activity and television watching in re-lation to
risk for type 2 diabetes mellitusin men. Arch Intern Med
161:15421548,2001
20. Hu G, Qiao Q, Silventoinen K, ErikssonJG, Jousilahti P,
Lindstrom J, Valle TT,Nissinen A, Tuomilehto J:
Occupational,commuting, and leisure-time physical ac-tivity in
relation to risk for type 2 diabetesin middle-aged Finnish men and
women.Diabetologia 46:322329, 2003
21. Weinstein AR, Sesso HD, Lee IM, CookNR, Manson JE, Buring
JE, Gaziano JM:Relationship of physical activity vs bodymass index
with type 2 diabetes inwomen. JAMA 292:11881194, 2004
22. Hsia J, Wu L, Allen C, Oberman A, Law-son WE, Torrens J,
Safford M, LimacherMC, Howard BV: Physical activity and di-abetes
risk in postmenopausal women.Am J Prev Med 28:1925, 2005
23. James SA, Jamjoum L, Raghunathan TE,Strogatz DS, Furth ED,
Khazanie PG:Physical activity and NIDDM in African-Americans: the
Pitt County Study. Diabe-tes Care 21:555562, 1998
24. Baan CA, Stolk RP, Grobbee DE, Witte-man JC, Feskens EJ:
Physical activity inelderly subjects with impaired glucosetolerance
and newly diagnosed diabetesmellitus. Am J Epidemiol
149:219227,1999
25. Defay R, Delcourt C, Ranvier M, LacrouxA, Papoz L:
Relationships between physi-cal activity, obesity and diabetes
mellitusin a French elderly population: the POLA
study. Int J Obes Relat Metab Disord 25:512518, 2001
26. Van Dam RM, Schuit AJ, Feskens EJ, Sei-dell JC, Kromhout D:
Physical activity andglucose tolerance in elderly men: the Zut-phen
Elderly study. Med Sci Sports Exerc34:11321136, 2002
27. Combe H, Vol S, Thevenot A, LasfarguesG, Caces E, Tichet J,
Lecomte P: Compar-ison of men with impaired fasting glycae-mia to
controls and to diabetic subjectswith fasting glycaemia from 7.0 to
7.7mmol/l: clinical, nutritional and biologi-cal status. Diabetes
Metab 30:167174,2004
28. Dunstan DW, Salmon J, Owen N, Arm-strong T, Zimmet PZ,
Welborn TA, Cam-eron AJ, Dwyer T, Jolley D, Shaw JE:Physical
activity and television viewing inrelation to risk of undiagnosed
abnormalglucose metabolism in adults. DiabetesCare 27:26032609,
2004
29. DerSimonian R, Laird N: Meta-analysis inclinical trials.
Control Clin Trials 7:177188, 1986
30. Higgins JP, Thompson SG: Quantifyingheterogeneity in a
meta-analysis. Stat Med21:15391558, 2002
31. Begg CB, Mazumdar M: Operating char-acteristics of a rank
correlation test forpublication bias. Biometrics 50:10881101,
1994
32. Egger M, Davey Smith G, Schneider M,Minder C: Bias in
meta-analysis detectedby a simple, graphical test. BMJ 315:629634,
1997
33. Orchard TJ, Temprosa M, Goldberg R,Haffner S, Ratner R,
Marcovina S, FowlerS, Diabetes Prevention Program ResearchGroup:
The effect of metformin and inten-sive lifestyle intervention on
the meta-bolic syndrome: the Diabetes PreventionProgram randomized
trial. Ann Intern Med142:611619, 2005
34. Nakashini N, Takatorige T, Suzuki K:Daily life activity and
risk of developingimpaired fasting glucose or type 2 diabe-tes in
middle-aged Japanese men. Diabe-tologia 47:17681775, 2004
35. Peters JL, Sutton AJ, Jones DR, AbramsKR, Rushton L:
Comparison of two meth-ods to detect publication bias in
meta-analysis. JAMA 295:676680, 2006
36. Perseghin G, Price TB, Petersen KF, Ro-den M, Cline GW,
Gerow K, Rothman DL,Shulman GI: Increased glucose
transport-phosphorylation and muscle glycogensynthesis after
exercise training in insulin-resistant subjects. N Engl J Med
335:13571362, 1996
37. Goodyear LJ, Kahn BB: Exercise, glucosetransport, and
insulin sensitivity. AnnuRev Med 49:235261, 1998
38. Wing RR, Venditti E, Jakicic JM, PolleyBA, Lang W: Lifestyle
intervention inoverweight individuals with a family his-tory of
diabetes. Diabetes Care 21:350359, 1998
Jeon and Associates
DIABETES CARE, VOLUME 30, NUMBER 3, MARCH 2007 751
-
39. Di Loreto C, Fanelli C, Lucidi P, MurdoloG, De Cicco A,
Parlanti N, Ranchelli A,Fatone C, Taglioni C, Santeusanio F, DeFeo
P: Make your diabetic patients walk:long-term impact of different
amounts ofphysical activity on type 2 diabetes. Dia-betes Care
28:12951302, 2005
40. Aldred HE, Hardman AE, Taylor S: Influ-ence of 12 weeks of
training by briskwalking on postprandial lipemia and in-sulinemia
in sedentary middle-agedwomen. Metabolism 44:390397, 1995
41. Furukawa F, Kazuma K, Kawa M, Mi-yashita M, Niiro K,
Kusukawa R, KojimaM: Effects of an off-site walking programon
energy expenditure, serum lipids, and
glucose metabolism in middle-agedwomen. Biol Res Nurs 4:181192,
2003
42. Asikainen TM, Miilunpalo S, Kukkonen-Harjula K, Nenonen A,
Pasanen M, RinneM, Uusi-Rasi K, Oja P, Vuori I: Walkingtrials in
postmenopausal women: effect oflow doses of exercise and exercise
frac-tionization on coronary risk factors. ScandJ Med Sci Sports
13:284292, 2003
43. Laaksonen DE, Lindstrom J, Lakka TA,Eriksson JG, Niskanen L,
Wikstrom K,Aunola S, Keinanen-Kiukaanniemi S,Laakso M, Valle TT,
Ilanne-Parikka P,Louheranta A, Hamalainen H, Rastas M,Salminen V,
Cepaitis Z, Hakumaki M,Kaikkonen H, Harkonen P, Sundvall J,
Tuomilehto J, Uusitupa M: Physical activ-ity in the prevention
of type 2 diabetes:the Finnish diabetes prevention study. Di-abetes
54:158165, 2005
44. Eyre H, Kahn R, Robertson RM: Prevent-ing cancer,
cardiovascular disease, anddiabetes: a common agenda for the
Amer-ican Cancer Society, the American Diabe-tes Association, and
the American HeartAssociation. Diabetes Care 27:18121824,2004
45. Schoenborn CA, Adams PF, Barnes PM,Vickerie JL, Schiller JS:
Health behaviorsof adults: United States, 19992001. VitalHealth
Stat 10:179, 2004
Physical activity and type 2 diabetes
752 DIABETES CARE, VOLUME 30, NUMBER 3, MARCH 2007