Embed Size (px)
Citation preview

Precision in Public Health 1
TitleRisk biomarkers enable precision in public health
AuthorsWilliam Ollier, Kenneth R. Muir, Artitaya Lophatananon, Arpana Verma, Martin Yuille
AffiliationCentre for Epidemiology, Division of Population Health, Faculty of Biology, Medicine and Health, The University of Manchester, Stopford Building, 99 Oxford Rd, Manchester M13 9PG UK
KeywordsPrecision medicine, prediction models, NHS Health Check, risk factors, data management, resource management, non-communicable chronic disease, obesity, health policy, public policy.
Running titlePrecision in public health
Executive SummaryThe rise of biomarkers
Biomarkers offer the promise of transforming primary prevention in non-communicable chronic diseases, some of which are at global epidemic proportions.
The biomarkers used in diagnosis of - or prognosis in - a non-communicable chronic disease may also act as biomarkers for measuring risk of developing a particular disease. We call the latter “risk biomarkers”.
Among risk biomarkers there are variable-risk biomarkers that change in a timely fashion in one direction with increases in risk and in the opposite direction with decreases in risk. These properties make them ideal for monitoring risk.
The potential of risk biomarkers to contribute to Public Health has prompted use of the term “Precision Public Health” by analogy to Precision Medicine.
Personal disease risk assessment tools
By identifying a statistical association between an event and variables such as risk biomarkers we can construct a Disease Risk Model. This involves use of a training dataset obtained from a population cohort and then use of a validation dataset to estimate the effectiveness of the initial model.
Precision Public Health
Precision Public Health, like Public Health, seeks primary prevention in the population but [a] uses individual risk monitoring at baseline and then during the period of risk reduction; and [b] enables, facilitates or empowers the individual to undertake collective (and individual) actions for risk reduction.
A strategy based on individual risk monitoring has been in place in the UK for some years - the NHS Health Check system - but the epidemics have not been curbed. We are driven to conclude that this strategy needs at least to be supplemented with a strategy based on socialised risk reduction with risk monitoring.
Development of Precision Public Health starts with the tools and infrastructure that we have today. One key tool is the electronic health record. Two essential infrastructures are advanced data management and advanced resource management. Existing disease biomarkers need to be re-purposed as risk biomarkers. The NHS Health Check system provides a good starting point for the UK.
Implementing Precision Public Health

Precision in Public Health 2
Some of the requirements for the creation of a Precision Public Health system are:
o Invitation to the NHS Health Check should include seeking consent for participation in health research.
o Disease risk models should be developed for all common chronic non-communicable diseases and conditions that have at least one modifiable risk factor.
o The first assessment of risk should be at an early age not least because childhood obesity is increasing rapidly. The age of consent seems reasonable.
o Risks-based monitoring should be available throughout life with a frequency determined by the rates and direction of change of risks.
o A fully integrated wide-area EHR system is the basis for on-going automated monitoring that then enable stratification of risk groups.
o The health check needs to be delivered by a trained professional with knowledge and skills in disease risk monitoring and reduction, in research methods and in community development work. On a daily basis, the work will involve face-to-face work with individuals in different settings, outreach work with local businesses and the third sector and some referrals to the healthcare system. Outreach work makes the Precision Public Health professional into a change agent for the community they serve. The change in social habits that is sought is a major task: the professional will need help that can be provided by the professional developing a network of Prevention Champions – volunteers who take it on themselves to put the health of the members of their organisation on the agenda of the organisation.
Future perspectives
Precision Public Health promises to bring together the individual and society in a new way because accurate risk monitoring creates a need for societal systems that are truly effective in empowering the individual to reduce risk. Risk biomarkers are therefore a disruptive technology. Two decades ago the UK government felt that engaging new social actors was necessary for the improvement of population health. Risk biomarkers now make that engagement essential.

Precision in Public Health 3
AbstractPrecision Medicine uses biomarkers to diagnose disease. However they can also be used to measure risk of disease. Thus biomarkers herald a new addition to public health - Precision Public Health. We examine the implications.
Risk biomarkers are identified by analysing population cohorts. They constitute risk factors in mathematical “Disease Risk Models”. The risk may be fixed as in a genetic biomarker or variable as in some protein biomarkers. They help monitor current risk of disease in an individual, thereby aiding efforts to reduce risk.
In the UK, the NHS Health Check system is a universal system for assessing risk and for risk-reduction. The system can now make use of modern biomarkers once appropriate infrastructure and governance are in place.

Precision in Public Health 4
1. The rise of biomarkersThe Human Genome Project was not only a major achievement in biological research but also a landmark that demonstrated the potential of “Big Science” in biology. Its successful completion hinged on international collaboration with open access to resources and data. It initiated extensive collaborative efforts to understand the causes and processes of human disease. While this understanding aids discovery of new treatments, it also offers new ways of preventing disease. This opportunity from Big Biology for improving population health was recognised at the time [1], but we have been slow both to explore and to implement the opportunity.
Twenty centres in China, France, Germany, Great Britain, Japan and the United States undertook the task of sequencing the human genome. A shared set of DNA resources was created and the sequencing data that emerged was shared publicly and immediately under the terms of the 1997 “Bermuda Principles” that project participants themselves established. They stated that “human genomic sequence information…should be freely available and in the public domain in order to encourage research and development and to maximise its benefit to society” [2].
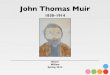
The spirit of these principles is essential in our view not only for health research but also for improving population health. The genome project prompted further successful collaborations to identify common genomic sequence variants (single nucleotide polymorphisms), to describe their geographical distribution and to discover associations between complex diseases and some of the variants. One notable collaboration was the Wellcome Trust Case-Control Consortium which used resources created with support from UK Medical Research Council and others to identify significant associations between these variants and high-impact complex diseases [3]. Rules on sharing were modified in favour of “fair access” [4]. Currently, 9,731 common variants as illustrated in Figure 1 have been reported that have a significant association with over 2,000 diseases and traits [5].
Figure 1 title: Genomic distribution of common sequence variants associated with human disease
Figure 1 legend: Spread across 23 human chromosomes, the diagram shows over 9,300 common sequence variants as circles of different colours. The variants are associated with increased inherited risk of over 2,000 diseases and traits. Taken from the NHGRI-EBI Catalogue of published genome-wide association studies [3].
Identification of these associations has provided insight into possible disease mechanisms and this, in turn, has stimulated new work on medicines development. Moreover, the pharmaceutical industry now acknowledges the value of open innovation through “pre-competitive collaboration” where the assertion of intellectual property rights is a hindrance [6]. But much remains to be done. In the context of population health, while only a fraction of total genetic risk has yet been explained, we may now construct disease risk models comprising risk factors identified from among both genetic and non-genetic biomarkers. These risk factors may be combined in risk

Precision in Public Health 5
models with other new risk factors identified from among geographical and physiological variables (e.g. measuring physical activity, heart rate, environmental exposures and so on) by new personal electronic devices. Molecular biomarker variation and variables measured by electronic devices promise to transform primary prevention.
Molecular biomarkers are those molecules of an organism where one or more properties of the molecule can be assayed to help ascertain one or more states or processes of the organism and are drawn from all human biological macromolecules (including DNA sequence variants), all intermediary metabolites and nutrients. Physiological and imaging measurements are sometimes also considered to be biomarker data. These sources of biomarkers for diagnosis of or prognosis (including therapy) in a particular disease are also sources of biomarkers for measuring risk of developing a particular disease. We thus distinguish between “disease biomarkers” and “risk biomarkers”.
Discovery of both types of biomarker is dependent on access to substantial populations where appropriate data and samples have been collected. Statistical analysis then permits the discovery of associations between variation in biomarkers and diagnosis or risk and the use of those associations to increase lifespan or healthspan respectively. Note that neither type of biomarker is necessarily causative of disease or in treatment responses.
An important distinction among the molecular biomarkers is that some show variation only between individuals (e.g. germline genetic biomarkers) while others also show variation within individuals over time. In individuals therefore, some germline DNA sequence variants give rise to a fixed component of overall risk. By contrast, variation in other biomarker types and variation in physical, chemical, biological and societal exposures to the organism and its components may be risk factors associated with greater or lesser probability of an event in a given period.
From the perspective of the individual, a particular germline DNA sequence at a genetic locus can be associated with a fixed risk of an event in a specified period while a protein or metabolite (or somatic DNA sequence) whose concentration or structure can change can be associated with a variable risk of an event in a specified period (N.B. the numerical value of a component of risk in an individual of course can only be obtained from population estimates). A “risk biomarker” is then a biomarker associated with a fixed or variable risk of an event in a specified period.
Discovery of variable-risk biomarkers has proved more difficult than the discovery of fixed-risk biomarkers in germline DNA sequence. Explanations for this difference include subjective reasons (researchers tend to be interested in causality and DNA sequence variation often provides hypotheses on causation). Other explanations include higher capital and unit costs of technology platforms and the sometimes unsatisfied requirements for a Quality Management System in proteomic and metabolomics [7]. It is clear that these issues can be addressed with the right infrastructure investment but this may well be beyond the control of traditional laboratories [8, 9].
There is an important benefit in variable-risk biomarkers. If, then, such a biomarker changes in a timely fashion in one direction with increases in risk and in the opposite direction with decreases in risk then that biomarker is capable of informing both the key steps of Precision Public Health: baseline risk assessment and risk reduction (see below). This is significant because while improvements to risk assessment have exercised researchers in public health, the whole point of the exercise is to reduce risks in the population. Therefore measures which may give the earliest indications of success in risk reduction are valuable.
The potential of disease biomarkers to contribute in the clinic to diagnosis and to the efficacy and safe use of a medicine has prompted the research community to coin terms such as “Precision Medicine” or stratified medicine or personalised medicine. The potential of risk biomarkers to contribute to Public Health has prompted the research community to coin the term “Precision Public Health” [10].
2. Personal disease risk assessment toolsFor an epidemiologist, a risk factor is one of the “totality of life-course environmental exposures (including lifestyle factors) from the prenatal period onwards” that defines the exposome [11].
For a biologist, the focus is not so much on the exposure but rather on the impact of an exposure on the molecules that make up the human body. The biologist is interested in the pathway from the initial molecular site in the body of interaction with the totality of life-course environmental exposure to the point where, in time, the risk becomes the reality of a disease or condition. This pathway is long and complex and may well be affected by variables familiar to the epidemiologist but which the biologist sees as surrogates for biological processes (e.g. an epidemiologist may see calendar age as a risk factor where the biologist sees biological age – see below).

Precision in Public Health 6
For a mathematician, a risk factor is any variable that contributes to the overall risk of an event. The variable can become a risk factor when it is demonstrated that the variable confers a probability of an event occurring within a specified time. In this mathematical context, the event is the diagnosis of a specified disease or condition in a specified period. There is no restriction on the nature of a risk factor: it needs only to be demonstrated that there is a robust statistical association between the variable and the event. Causality between the variable and the event is immaterial to the mathematics: there is no requirement for knowledge of disease aetiology. By identifying a statistical association between variables and an event, the mathematician is able to construct a risk model: an algorithm that, by combining weighted values for a number of risk factors, permits computation of the current risk of a future event.
We call the type of risk model designed to assess current risk of future disease or condition a “Disease Risk Model” (DRM). Such models may be further categorised if they restrict themselves to one or other type of risk factor. For example a non-clinical DRM would exclude risk factors that can only be measured in the context of a clinic. Such DRMs can be especially valuable for an initial stratification of the members of a population into lower or higher risk groups. When a DRM is deployed in a user-friendly manner, we call it a “tool” – a personalised disease risk assessment tool. A non-clinical risk assessment tool may be suitable for independent use by the individual citizen, although the value of this is unclear if risk monitoring is not tied to risk reduction.
Construction of a DRM involves examination of a data set with many variables measured in a population (usually a population cohort as this allows for temporal relationships in the data to be included). Such data sets need to be large so as to be able to model each risk factor and its relationships. The data must include data on the event (clearly defined and confirmed diagnosis of the disease or condition of interest). The variables can either be binary (e.g. present / not present) or continuous (e.g. a concentration of a molecule). There is no limit to the number of variables in the DRM. A DRM is always the best current approximation. It can be continually improved and refined if more variables are defined and more data are analysed.
Building a Disease Risk Model: two general approachesThere are two general approaches to developing a DRM. In the first approach, a model is generated as a mathematical algorithm based on a combination of known or measured characteristics in a large and representative dataset [12]. A data set from a population cohort is usually suitable only for modelling common disease or conditions. In rarer diseases, DRMs are often derived from case-control studies and converted to estimate a time dimension by using disease incidence or prevalence estimates for the population. Thus the difference between risk measurement from cohort studies and case-control studies is the ability in the former to estimate the time dependent aspects of the model directly from the cohort (for example risk of the disease in 2 or 5 years’ time) while the measurement from case-control studies will provide an overall value which has to be multiplied by externally derived estimates of disease occurrence over time. Use of cohort data sets is clearly preferable. Today there are growing numbers of national cohorts each with ever-longer follow-up times that will enable the development of more and better DRMs. At present, the largest of these is UK Biobank [13].
In the second approach, the risk estimates to be used in the DRM are derived by systematic reviews of existing studies and expert opinion. A weighted score is assigned to each of the risk factors and the total score is then computed. This converts to a probability of developing the disease [14]. Such estimates then need also to be applied to externally available estimates of disease incidence.
Building a Disease Risk Model: a step-by-step guideTo begin DRM construction, a “development” or “training” dataset is obtained from a population cohort containing both affected and unaffected individuals. A second dataset, usually called a “validation” dataset, is required later to estimate the effectiveness of the initial model.
It is clearly important to calculate whether the size of the data sets being used to build the DRM is sufficiently large and statistically powered to be meaningful. The ratio of events per variable (EPV) is often used to determine the sample size for DRM development. The EPV is the number of events in the data divided by the number of regression coefficients in the model. An EPV of 10 or more is required to avoid the problem of over-fitting [15]. For example, if there are 60 events (diagnoses of a disease) and three risk factors are fitted into the model, then the EPV is 60/3 = 20.
Constructing the model requires us first to identify which of the variables is significant. This is achieved by univariate analysis. However, only those variables with independent predictive ability should be included in the DRM and this is achieved by stepwise logistic regression.
The next step is model specification: determining which of these significant variables are independent and which should be included in or excluded from a model. One of the methods used for testing model specification

Precision in Public Health 7
is linktest which creates two new variables: a variable of prediction and a variable of prediction squared. The model is then refitted using these two variables. In a DRM that is correctly specified, if we regress the outcome on the prediction and the prediction squared, then the variable of prediction will have explanatory power (p-value<0.05) while the variable of prediction squared (a measure of the variance) will have no explanatory power (p-value>0.05).
Multi-collinearity is a high degree of correlation (linear dependency) among several independent variables. It commonly occurs when a large number of independent variables are incorporated in a regression model. Variables in the DRM that are not collinear should be excluded. Multi-collinearity is detected using variance inflation factors. A value close to unity for all variables detects multi-collinearity and indicates the parsimony of the model. Tolerance values larger than 0.1 indicate a requirement for all the variables present after stepwise logistical regression. The diagonal of R-1 (inverse of correlation matrix) values close to unity are considered acceptable.
Assessment of model performance
Two tests assess DRM performance: model calibration and model discrimination. Calibration (or ‘reliability’) refers to the agreement between predicted and observed predictions [16]. Discrimination refers to the ability of the model to distinguish between affected and unaffected individuals.
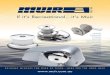
For binary outcomes, discrimination can be quantified by the area under the Receiver Operating Characteristic (ROC) curve Figure 2. This curve is constructed by plotting sensitivity (true positive) against 1-specificity (false negative) for different cut-off points for the predicted risk. The area indicates the probability that an individual with the event has a higher predicted probability than an individual without the event, for random pairs of individuals with and without the event. 95% confidence intervals for the area under the curve (AUCs) are calculated, assuming a bi-negative exponential distribution. An AUC of 0.5 indicates chance prediction (equivalent to a coin toss); whereas a statistic of 0.7 or above indicates that discrimination can be considered as acceptable. The calibration of the DRM is examined by establishing a calibration curve and using the Hosmer and Lemeshow goodness-of-fit test [17]. Satisfactory calibration by the model corresponds to p-value > 0.05. A statistic of 0.7 or above indicates that discrimination is acceptable.
Figure 2. ROC curve for a risk model
Figure 2 legend: Two hypothetical ROC curves are shown. The closer the curve follows the left vertical lines and the top horizontal line, the more accurate the test. The closer the curve is to the 45-degree diagonal, the less accurate the test.
Model validation
Once the DRM has been developed using a training set, it requires validation. This also assesses accuracy. Model validation is a test of how well the model performs in individuals other than those used to develop it. This model validation may be internal (using a non-overlapping set of data from the same cohort as the training set) or external (using data from a second cohort). Good practice calls for both internal and external model validation. Note that internal model validation has an inherent problem of over-estimation [18]. DRMs are often reported with internal model validation: only a few report external model validations.
Cross-validation is the name of the technique for model validation when assessing how the results of a statistical analysis will generalise to an independent data set [19]. In cross-validation, the dataset is randomly divided into k equal-sized parts. Part k is omitted and the model is fitted to the other (k-1) parts combined. Predictions are

Precision in Public Health 8
then obtained for the omitted kth part. If internal model validation by cross-validation yields a ROC with AUC > 0.7, then the model validation is considered satisfactory.
External validation using a second cohort is also satisfactory if AUC>0.7. If that is not the case then it is worthwhile to examine this second cohort for any source of bias that might have been introduced (e.g. selection biases). Detection of a source of bias may then put in question the low AUC value obtained.
3. Precision Public HealthWe have described the rise of biomarkers, referred to the term “Precision Public Health” and outlined the development of disease risk models. Can these activities help us improve population health, what issues then arise and how can we address them?
Public Health, Precision Public Health and Precision MedicinePublic health practice, in the main, provides primary prevention for the population: it acts to reduce risk of disease / morbidity. It is distinct from clinical medicine which mainly detects and treats disease as such. It is distinct from secondary prevention which acts to reduce risk of progression of disease (e.g. through screening programmes for earlier diagnosis when disease is more tractable) and it is distinct from tertiary prevention which aims to reduce the impact of disease.
There are two absolute requirements for reduction of risk of disease: risk assessment (as an observatory for the identification, characterisation and quantitation of factors that reduce population healthspan – the healthy lifespan) and risk reduction (action to increase population healthspan). Of course public health workers do more than this (e.g. work to extend lifespan; promoting public policy development; contributing to commissioning decisions, providing guidance and programmes for direct clinical practice, seeking improvements in socio-economic determinants of health). However, primary prevention itself comprises the activities of risk assessment and risk reduction. Risk assessment involves the measurement of risk factors for a disease or condition. We (individually and collectively) have the ability to change some, but not all, of these risk factors. Risk reduction therefore refers to actions on risk factors that are amenable to modification in the individual and in the population. The two principal risk reduction strategies in use today are general public education (e.g. leaflets and posters) and the promotion of public policy and regulation to reduce or eliminate a risk factor.
Precision Public Health practice also seeks primary prevention in the population but through individual risk monitoring (recurrent risk assessments) at baseline and then during the period of risk reduction. Assessment, of course, makes use of information on risk factors for the population in order to estimate risk of a disease for each individual in the population. When an individual has a risk above some agreed threshold, then Precision Public Health needs to enable, facilitate or empower that individual to undertake individual and collective actions for risk reduction.
Precision Public Health enhances the role of public health as an observatory, in education and in promotion of public policy and regulation. This enhancement arises from the greater granularity introduced by Precision Public Health. Risk monitoring enables continuous observation of risk factors. It permits better education and better decisions by the individual. The individual risk assessment has far-reaching consequences for the actions we take to reduce risk because it can empower the individual in ways that general public education alone cannot. Furthermore, specification of the risks facing each and every individual creates a societal need to enable or facilitate appropriate risk-reduction actions for all. Failure to meet this societal need may come to be considered immoral in the same way as it is considered immoral to diagnose disease without facilitating the most appropriate treatment. It is certainly an inefficient use of resources and may also be immoral to fail to provide on-going support to an individual once they have chosen to reduce a risk. Precision Public Health practitioners may well adopt their own Hippocratic Oath: “First, risk no harm”.
Precision Public Health brings observation closer to practise rather like Precision Medicine brings “the bench closer to the bedside”. Furthermore, Precision Public Health is synergistic with Precision Medicine. Not only may some biomarkers be “swapped” between the two, but the infrastructure for data and resource management may be shared. The data emerging from the practice of Precision Public Health is likely to clarify the distinctions we make between “risk” of disease and disease that is “early”, “pre-symptomatic”, “cryptic”, “occult” or “latent”. Precision Public Health is concerned with what we may call “Stage Minus One” of common chronic non-communicable disease processes before clinical intervention is appropriate and before secondary prevention with prophylactic treatment is an option. Exploring this Stage Minus One disease is a research task in Precision Public Health for the discovery of the earliest possible molecular changes that can be used to assess risk and risk reduction.

Precision in Public Health 9
The practice of both Public Health and Precision Public Health reduces the burden of clinical care. However, Precision Public Health provides a benefit by enabling discovery of incidental findings of undiagnosed disease. Because this discovery is likely to be of early disease, this then favours greater use of secondary prevention methods and less use of more invasive treatments.
If Precision Public Health is precise in its assessment of risk, is it similarly precise in the risk-reduction actions that it seeks? We cannot say, but, today’s public health strategies are not effective and so need change. Public health risk reduction strategy for the current epidemics of obesity, diabetes and cancer is based on advocating weight loss, cardiovascular fitness and tobacco cessation. The strategy has been in place for many years but the epidemics have not been curbed. We are driven to conclude that a strategy based on individual risk reduction needs at least to be supplemented with a strategy based on measuring risk reduction more precisely and on one based on new risk reduction methods that exploit new technologies socialised risk reduction. One successful example where aspects of socialised risk reduction are used is the “buddy system” for smoking cessation [20, 21]. More substantial proposals have been made that draw in a wider range of stakeholders than just public health agencies [22]. As Precision Public Health develops, it will be essential to undertake socialised risk reduction actions that engage all the stakeholders that governments have hoped to engage (individuals, voluntary bodies, businesses, health authorities, local government and government) [23].
Precision Public Health and risk biomarkersThe development of Precision Public Health cannot occur overnight and we are obliged to start with the tools and infrastructure – the capabilities and capacities - that we have today.
Capabilities
The tools we can use today in developing Precision Public Health include the electronic health record. This is a suitable source of measurements of non-clinical risk factors that allow stratification of the population into higher and lower risk groups. Socio-economic risk factors could be included by using small area demographic data. Individuals in a higher risk group might then provide further information and agree to some simple physiological measurements (e.g. spirometry, body composition, heart rhythm, pulse wave velocity etc.) that are readily available in wealthier regions of the world.
Widely assayed types of biomarker include certain proteins (e.g. HbA1c, serum creatinine, alkaline phosphatase, alanine aminotransferase, γ-glutamyl transferase, albumin, thyroid stimulating hormone, alpha-1 antitrypsin, C-reactive protein) and metabolites (e.g. glucose, cholesterol, total bilirubin, serum folate, vitamins, micro-nutrients). These biomarkers are usually measured in a clinical context. Some are known risk biomarkers, others may well be if assessed and validated for more refined DRMs.
In order to use omic approaches in Precision Public Health, genetic variants are the easiest place to start although they contribute only a fixed risk, as defined above. However, epigenetics provides a related and promising starting point where omic approaches can identify variable risk biomarkers. The most useful epigenetic loci are those where altered DNA modification at a locus is associated with a recent change in an individual’s exposome. Changes in white blood cell DNA methylation have been associated with social habits, environmental factors, cancer, CVD and diabetes [24-28]. Moreover, changes in methylation have been observed to arise with increasing age [29] thereby enabling assessment of “biological age”. This is an important concept for Precision Public Health because it enables an individualised assessment of healthspan as well as lifespan. A recent publication used an epigenome-wide approach on a discovery panel and a validation panel drawn from two population cohorts. The authors developed a mortality risk score by examining ten CpGs (loci susceptible to changes in degree of methylation) for their degree of aberrant methylation (i.e. higher or lower levels of methylation than the norm). The larger the number of loci with aberrant methylation, the greater the risk in a specified time of all-causes mortality [30]. These findings offer the prospect of developing the related “morbidity risk score” that can predict years remaining of healthspan. Such information will assist individualised education in and measurement of risk-reduction (assuming loss of aberrant methylation occurs in a timely fashion after risk reduction actions have been initiated).
Capacities
Since 2008 in the UK, the health system has offered a universal health check with invitations to a face-to-face assessment of risk provided after age stratification. The focus of the NHS Health Check system has been on reducing cardiovascular disease where mortality has been in decline for decades. The system has been reorganised several times and it has its critics. However, no critic has identified a better way than universal health checks for improving the health of the population one person at a time and the system is therefore the organisational foundation for the growth of Precision Public Health.

Precision in Public Health 10
The speediest possible exploitation of the potential of Precision Public Health requires us to move away from research based on the population cohort toward real-life observations of risk monitoring and real-life experiments in risk reduction. The same is true for exploiting the potential of Precision Medicine. In both cases the work requires the right infrastructure, administration and governance to be in place.
The two essential infrastructures required for a mature Precision Public Health system are advanced data management and advanced resource management. Advanced data management should aim at ensuring appropriate access to EHR and other data for all individuals in all geographical locations so as to take account of the high level of mobility of the population today. Advanced resource management should aim at ensuring appropriate access to current and historical biological samples so that when a new biomarker is introduced it is possible to evaluate longitudinal changes in the biomarker’s concentration or nature where such changes are associated with changes in risk. The issue of appropriate access to data and resources requires public debate. Major errors have repeatedly been made by governments on data access that have risked undermining the confidence of the public in their retaining ultimate oversight on their own data and resources. Because breaches in data security (though not resource security) appear unlikely to go away, the public debate on these issues in the context of health needs to be continuous with no social groups excluded.
A key administrative need is a system to obtain broad consent across the population for its participation in research. This permits re-contacting that then enables obtaining extra information or new samples and that enables participation by individuals in novel risk reduction actions.
Setting priorities for Precision Public Health
Precise assessment of an individual’s risk of disease is particularly important when prevention of the disease requires sustained action by the individual concerned (unlike in infectious disease where prevention is enabled by immunisation or sanitation). The individual needs feedback on the effectiveness of their risk-reduction actions. Variable risk biomarkers are a promising additional tool for this.
The UK Health Forum and Cancer Research UK predicts [31] that, in 2035, being overweight or obese will be the underlying cause of 440,000 avoidable cases of disease in the UK population each year. This breaks down to 257,200 avoidable cases per annum of type 2 diabetes, 101,000 avoidable cases per annum of coronary heart disease, 43,600 avoidable cases per annum of stroke and 38,500 avoidable cases per annum of cancer. Note that vascular disease and cancer are just two of the groups of diseases associated with obesity.
In December 2015, England’s Chief Medical Officer, identified an obesity epidemic [32]. National statistics show [33] that there was a marked increase for England in the proportion of adults that were obese from 13.2% in 1993 to 26.0% in 2013 for men and from 16.4% to 23.8% for women. The proportions that were overweight-obese increased from 57.6% to 67.1% in men and from 48.6% to 57.2% in women.
The rapid increase in the prevalence of overweight-obesity has meant that the proportion of adults in England with a “healthy” Body Mass Index (BMI) decreased between 1993 and 2014 from 41.0% to 32.7% among men, and 49.5% to 40.4% among women. In England, currently 25.6% of adults (aged 16 years and over) are obese (HSE 2014). By 2050 obesity is predicted to affect 60% of adult men, 50% of adult women and 25% of children. Obesity is set to rise to 35% of 6-15 year olds by 2050.
The fact that healthy BMI is based on population estimates but a specific individual may have a different healthy BMI does not lessen the extent of the health-related and social dangers of obesity. It is a substantial risk factor for the diseases shown in Table 1 [34, 35]. Note that co-morbidity is not uncommon between the diseases listed.
Table 1 title: Diseases whose risk is associated with high Body Mass Index
Health risk DescriptionMetabolic syndrome 30% of middle aged people in developed countries have features of metabolic
diseaseType 2 diabetes 90% of type 2 diabetics have BMI >23 kg m-2. Co-morbidities: renal disease;
peripheral neuropathies including blindness; amputations.Hypertension 5x risk in obesity; 66% of hypertension is linked to excess weight; 85% of
hypertension is associated with BMI >25 kg m-2
Coronary heart disease and stroke
3.6x risk of CAD for each unit change in BMI; dyslipidaemia progressively develops as BMI increases from 21 kg m-2 with rise in small particle low-density lipoprotein; 70% of obese women with hypertension have left ventricular hypertrophy; Obesity is a contributory factor to cardiac failure in >10% of patients. Overweight/obesity is associated with increased risk of ischaemic stroke.

Precision in Public Health 11
Respiratory effects Neck circumference >43 cm in men and >40.5 cm in women is associated with obstructive sleep apnoea, daytime somnolence and development of pulmonary hypertension
Cancers 10% of all cancer deaths among non-smokers are related to obesity. Obesity is a major risk factor in the most common 11 cancers.
Reproductive function 6% of infertility in women is attributable to obesityImpotency and infertility are frequently associated with obesity in men
Osteoarthritis Frequent association in the elderly with increasing body weight – risk of disability attributable to OA equal to heart disease and greater to any other medical disorder of the elderly
Liver and gall bladder disease
Overweight and obesity associated with non-alcoholic fatty liver disease and non-alcoholic steatohepatitis (liver inflammation). 40% of NASH patients are obese; 20% have dyslipidaemia. 3x risk of gall bladder disease in women with BMI >32 kg m-2. 7X risk if BMI >45 kg m-2
Depression Obesity increases the risk of depression while depression is predictive of developing obesity.
In each case, disease biomarkers need to be re-purposed as risk biomarkers or to be discovered and validated so as to improve on today’s disease risk assessment tools. In the meantime, these tools will have to suffice.
In the longer term, Precision Public Health must seek means of reducing risk of onset of a wider range of diseases. Lung disease (chronic obstructive pulmonary disease, emphysema, lung cancers, bronchitis and bronchiectasis) is strongly associated with certain chemical exposures. Where these exposures arise from social habits, their reduction can be facilitated by knowledge of an individual’s risk profile.
From the population’s perspective, the issue of healthspan is somewhat different. It is probably the case that people want to know “when” their healthspan will end at least as much as they want to know “what” will end it. Health planners have a comparable interest, although life insurers focus on lifespan. To encourage greater uptake by the population of health checks, we note that this desire to know “when” could be satisfied with an all-risks morbidity assessment tool. An all-risks mortality tool based on UK Biobank data has been described [36]. Conversion of a mortality tool to a morbidity tool requires knowledge of a date of diagnosis rather than of death. While this work is done, immediate methods for increasing uptake should include optimising invitations by letter and by texts [37], while more intensive methods for increasing uptake may be justified if invitations are based on prior analysis of risks using EHR data. Finally, while financial incentives like tax breaks for increasing uptake could be devised, such individualised policies may undermine socialised risk reduction actions without improving outcomes from individualised risk reduction actions.
4. Implementing Precision Public HealthTo implement Precision Public Health involves specifying some of the requirements for the creation of a Precision Public Health system: Invitation to the NHS Health Check should include seeking consent for participation in health research.
This then enables testing new risk assessments and new risk-reduction actions. Participation will facilitate real-world research. It should yield a “healthy cohort” effect and it comprises a step toward the socialisation of risk reduction. It will expedite the identification of new risks and associated modifiable risk factors.
Disease risk assessment tools should be developed for all common chronic non-communicable diseases and conditions that have at least one modifiable risk factor. While these tools can be used at a distance, the health check nonetheless needs to include a face-to-face element at least in order to initiate risk-reduction actions.
The first assessment of risk should be at an early age not least because childhood obesity is increasing rapidly. The age of consent seems reasonable, although obesity risk biomarkers indicate that risk is congenital [38] thus pointing a need for earlier risk assessment.
Risks-based monitoring should be available throughout life with a frequency determined by the rates and direction of change of risks. The current standard five-year re-invitation for a health check reflects the imprecise character of risk assessment today.
A fully integrated wide-area EHR system is the basis for on-going automated monitoring that can provide timely warning of a significant change in risk. A wide-area EHR also permits continuity when individuals move home and ensures that referrals from the Precision Public Health system to the healthcare system are seamless. Automated monitoring also releases resources for risk reduction.

Precision in Public Health 12
Automated risk monitoring enables stratification of risk groups and permits more precise tests such as risk biomarker tests to be carried out on people that need them most. Miniaturisation of biomarker testing is an important area of innovation.
The health check needs to be delivered by a trained professional with knowledge and skills in both disease risk assessment and reduction as well as in research methods. Since risk reduction will be not only individualised but also socialised, training will require knowledge of community development work. The professional’s practise should be located within the community though not necessarily at a primary care centre. On a daily basis, the work will involve face-to-face work with individuals in different settings [39], outreach work with local businesses and the third sector and some referrals to the healthcare system when there are incidental suspected findings of disease. Knowledge of research methods is necessary because Precision Public Health involves continuous feedback between research and practise.
This outreach work makes the Precision Public Health professional into a change agent for the community they serve. The change in social habits that is sought is a major task: the professional will need help – at least voluntary help. This help can be provided by the professional developing a network of Prevention Champions – volunteers who take it on themselves to put the health of the members of their organisation on the agenda of the organisation. The Prevention Champions also act as intermediaries between the individual receiving risk reduction advice and the particular local organisation of which they happen to be a member.
In Figure 3 we represent the implementation of Precision Public Health in diagrammatic form. It takes the form of a cycle of implementation and improvement and thereby makes a single whole of research and practise. This cyclical character leads us to call the process an “engine” – the Health Engine.
Figure 3 title: The Health Engine for improving population health
At the heart of the engine is a face-to-face health check. This is informed by using disease risk assessment tools that analyse data from the EHR on the individual and their relatives, supplemented where necessary with data from questionnaires and on biomarkers, physiology and socio-economic factors. The tools would be subject to continuous improvement and oversight. If the health check yields suspected early disease, the individual would be referred to the healthcare system. If the health check indicates higher risk of a disease, then the Precision Public Health practitioner provides individual education on risk and risk reduction and encourages and facilitates actions to cut risk. In all cases, individuals are invited to consent to participate in healthspan research.
Are these radical proposals based in reality? We believe that the development of dentistry in past years points to the possibility of extending healthcare from treatment alone to include prevention. Dentistry has extended its work over the last seven decades from acute intervention (extractions and restorative work) to include both primary and secondary prevention (regular oral health checks with oral hygiene maintenance and advice from trained hygienists). Regulatory change (water fluoridation) is also considered to have aided prevention. General public education is undertaken by public health bodies as well as business (e.g. manufacturers of toothpaste).

Precision in Public Health 13
This then suggests [a] individualised primary prevention with population-wide coverage works (up to a point); [b] general public education has retained a role; [c] prevention work calls for professionals with distinct qualifications; [d] the growth of work on prevention has not impeded work on innovative treatments.
5. ConclusionWe have shown that strategies based on identifying multi-factorial risk of chronic disease, including biomarkers, behaviour and environment, can potentially be developed to deliver risk-reduction actions. These strategies and actions include the development of new and improved disease risk models and provide the basis for Precision Public Health. The actions required include the development of appropriate capabilities (the ability to measure in the population risk factors observed in population cohorts) and capacities (advanced data and resource management.). This offers the prospect of stemming the tide of chronic conditions and diseases that afflict societies today across the globe.
6. Future PerspectiveRisk biomarkers can help bring to each of us precision both in the assessment of risk of disease and in the assessment of the effectiveness of actions to reduce risk. It is therefore appropriate to describe this new level of granularity in public health as “Precision Public Health”.
This term, of course, finds its roots in “Precision Medicine” but we suggest that the two practices are not like “two peas in a pod” [40]. Biomarkers are important to both, but nonetheless there are differences as well as similarities as summarised in Table 2.
Table 2: Precision Medicine and Precision Public Health: two peas in a pod?
Precision Medicine Precision Public HealthAims to increase lifespan Aims to increase healthspan (1)Increases lifespan without necessarily curing disease Decreases unhealthy lifespanIncreases specificity and sensitivity of diagnosis Increases specificity and sensitivity of risk
assessmentDirected at individual diagnosis Directed at individual initial risk assessmentDirected at individual treatment Directed at individual and/or collective risk reductionRequires diagnostic, efficacy and safety biomarkers Requires risk assessment and reduction biomarkersRequirement for biomarker discovery and continuous improvement
Requirement for biomarker discovery and continuous improvement
Biomarker change indicates clinical change Biomarker change indicates exposure change (2)Biomarker contributes to clinical decisions Biomarker contributes to public health actionsTable 2 legend: Notes: (1) healthspan (healthy lifespan) means the absence of disability or morbidity; (2) exposure is broadly defined and refers here to the exposures on the biomarker.
While a given biomarker can be valuable to both Precision Medicine and to Precision Public Health, this is not always the case. For example, in infectious disease, the detection of, say, a viral antibody indicates the need for treatment: the time for prevention has passed. By contrast, testing for the prevalence of antibody in a population can contribute to implementing regular public health policy to reduce infection. For prevention of infection in the individual, risk biomarkers are needed that indicate risk of infection (i.e. susceptibility) and risk of severity of symptoms and that thereby help those at greatest risk to reduce their own risk. Another example arises from considering socio-economic variables as potential risk factors. Risk biomarkers have been identified as non-independent variables of socio-economic risk factors (e.g. telomere length and community stress [41-45]). Here the biomarker is of little value to medicine but can inform Public Health practise when measured in the population. In non-communicable disease, exposure to poor nutrition may lead to biomarker changes (metabolite abnormalities) that indicate elevated risk of, say, a deficiency disease. However, the disease itself may be diagnosed with other more specific biomarker abnormalities. The challenge in risk biomarker research in facilitating prevention of non-communicable disease is to specify total risk using fixed and variable risk biomarkers and to identify those risk biomarkers suitable for measuring increases and decreases in risk in a timely fashion. This is a significant challenge.
In the longer term, Precision Public Health promises to bring together the individual and society in a new way. On the one hand, risk biomarkers enable accurate risk monitoring in the individual citizen. But on the other hand, this monitoring creates a need for societal systems that are truly effective in empowering the individual to reduce risk. Risk biomarkers are therefore a disruptive technology. Two decades ago the government felt that engaging new social actors was necessary for the improvement of population health in the UK [23]. In the

Precision in Public Health 14
upshot, engagement has been slow and incomplete. Risk biomarkers make that engagement essential. Therefore, in the medium term over the next decade or so, it is realistic to expect small-scale trials where existing and new risk biomarkers are used to monitor risk in geographically limited areas and where that monitoring is used to encourage groups of individuals to persist in their activities to introduce social habits that reduce risk of non-communicable chronic diseases. In the UK, research funders have begun to turn their attention to this via the UK Prevention Research Partnership [46]. While the UK remains a relatively prosperous country with a relatively integrated universal health system and with a developed civil society, it will provide a relatively satisfactory environment for implementing Precision Public Health. Elsewhere, in countries currently less prosperous, there are a range of impediments to implementation, including a technological deficit. However some countries may have the advantage of greater social cohesion and solidarity to facilitate successful risk reduction activities. This is an important issue that probably requires joint international investigations, coordination and trials in the coming years.

Precision in Public Health 15
References[1] Collins FS, Green ED, Guttmacher AE, Guyer MS. A vision for the future of genomics research. Nature. 422, 835-847 (2003).
[2] Human Genome Organisation. Summary of the Report of the Second International Strategy Meeting on Human Genome Sequencing, Bermuda. 1997. http://web.ornl.gov/sci/techresources/Human_Genome/research/bermuda.shtml Accessed 26 November 2017.
[3] Wellcome Trust Case Control Consortium https://www.wtccc.org.uk/ccc1/wtccc1_studies.html Copyright © EMBL-EBI 2017 Accessed 3 July 2016.[4] Yuille M, Dixon K, Platt A, Pullum S, Lewis D, Hall A, Ollier W. The UK DNA Banking Network: a “fair access” biobank. Cell Tissue Bank. 11(3), 241-251 (2010).
[5] The NHGRI-EBI Catalogue of published genome-wide association studies. https://www.ebi.ac.uk/gwas/search/traits Accessed 30 July 2017.
[6] Vaudano E. The innovative medicines initiative: a public private partnership model to foster drug discovery. Comput Struct Biotechnol J. 6, e201303017 (2013).
[7] Poste G. Bring on the biomarkers. Nature. 469, 156–157 (2011).
[8] Gold L, Ayers D, Bertino J et al. Aptamer-based multiplexed proteomic technology for biomarker discovery. PLoS One. 5(12), e15004 (2010).
[9] Yuille M, Feller PI, Georghiou L, Laredo P, Welch EW. Financial Sustainability of Biobanks: From Theory to Practice. Biopreserv Biobank. 15(2), 85-92 (2017).
[10] Khoury MJ, Iademarco MF, Riley WT. Precision Public Health for the Era of Precision Medicine. Am J Prev Med. 50(3), 398-401 (2016).
[11] Wild CP. Complementing the genome with an "exposome": the outstanding challenge of environmental exposure measurement in molecular epidemiology. Cancer Epidemiol Biomarkers Prev. 14(8), 1847-50 (2005).
[12] Usher-Smith J, Emery J, Hamilton W, Griffin SJ, Walter FM. Risk prediction tools for cancer in primary care. Br J Cancer. 113(12), 1645-1650 (2015)
[13] UK Biobank http://www.ukbiobank.ac.uk/
[14] Colditz GA, Atwood KA, Emmons K et al.. Harvard Report on Cancer Prevention Volume 4: Harvard Cancer Risk Index. Cancer Causes and Control. 11(6), 477-488 (2000).
[15] Pavlou M, Ambler G, Seaman SR et al. How to develop a more accurate risk prediction model when there are few events. BMJ. 351, h3868 (2015).
[16] Cook NR. Statistical evaluation of prognostic versus diagnostic models: beyond the ROC curve. Clin Chem. 54(1), 17-23 (2008).
[17] Hosmer DW, Lemeshow S. Applied Logistic Regression. Wiley. New York. 2013. ISBN 978-0-470-58247-3.
[18] Collins GS, Altman DG. Identifying patients with undetected pancreatic cancer in primary care: an independent and external validation of QCancer® (Pancreas). Brit. J. Gen. Practice. 63(614), e636-e642 (2013).
[19] Geisser S. Predictive Inference. Chapman and Hall. New York. 1993. ISBN 0-412-03471-9.
*[20] West R, Edwards M, Hajek P. A randomized controlled trial of a ‘buddy’ system to improve success at giving up smoking in general practice. Addiction. 93, 1007 –11 (1998).
[21] May S, West R, Hajek P, McEwen A, McRobbie H. Randomized controlled trial of a social support ('buddy') intervention for smoking cessation. Patient Educ Couns. 64(1-3), 235-41 (2006).
[22] Laverack G. Health Promotion Practice: Building Empowered Communities: Building Empowered Communities (UK Higher Education OUP Humanities & Social Sciences Health & Social Welfare). Open University Press. 2007. ISBN-13: 978-0335220571
*[23] Department of Health. Our Healthier Nation: a contract for health. 9 February 1998. www.gov.uk/government/publications/our-healthier-nation-a-contract-for-health
[24] Dick KJ, Nelson CP, Tsaprouni L et al. DNA methylation and body-mass index: a genome-wide analysis. Lancet. 383, 1990–1998 (2014).

Precision in Public Health 16
[25] Gao X, Jia M, Zhang Y, Breitling LP, Brenner H. DNA methylation changes of whole blood cells in response to active smoking exposure in adults: a systematic review of DNA methylation studies. Clin. Epigenetics. 7, 113-123 (2015).
[26] Feinberg AP. Genome-scale approaches to the epigenetics of common human disease. Virchows Arch. 456, 13–21 (2010).
[27] Zhong J, Agha G, Baccarelli AA. The role of DNA methylation in cardiovascular risk and disease: methodological aspects, study design, and data analysis for epidemiological studies. Circ. Res. 118, 119–131 (2016).
[28] Chambers JC, Loh M, Lehne B et al. Epigenome-wide association of DNA methylation markers in peripheral blood from Indian Asians and Europeans with incident type 2 diabetes: a nested case-control study. Lancet Diabetes Endocrinol. 3, 526–534 (2015).
[29] Hannum G, Guinney J, Zhao L et al. Genome-wide methylation profiles reveal quantitative views of human aging rates. Mol. Cell. 49,359–367 (2013).
*[30] Zhang Y, Wilson R, Heiss J et al. DNA methylation signatures in peripheral blood strongly predicts all-cause mortality. Nat Commun. 8, 14617 (2017).
[31] Cancer Research UK and the UK Health Forum. Tipping the Scales: Why preventing obesity makes economic sense. 2016 http://nhfshare.heartforum.org.uk/RMAssets/Modelling/Tipping%20The%20Scales%20-%20CRUK%20Full%20Report.pdf Accessed 6 July 2016.
*[32] Annual Report of the Chief Medical Officer, 2014. The Health of the 51%: Women. 2015. https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/484383/cmo-report-2014.pdf Accessed 6 July 2016.
[33] Lifestyles Statistics Team, Health and Social Care Information Centre. Statistics on Obesity, Physical Activity and Diet: England 2015. 2015. http://www.hscic.gov.uk/catalogue/PUB16988/obes-phys-acti-diet-eng-2015.pdf Accessed 6 July 2016.
[34] Kopelman, P. Health Risks Associated with Overweight and Obesity. Short Science Review. Foresight Tackling Obesities: Future Choices. Obesity Reviews. 8(s1):13–17 (2007).
[35] Luppino FS, de Wit LM, Bouvy PF, Stijnen T, Cuijpers P, Penninx BW, Zitman FG. Overweight, obesity, and depression: a systematic review and meta-analysis of longitudinal studies. Arch Gen Psychiatry. 67(3):220-229 (2010).
[36] Ganna A, Ingelsson E. 5 year mortality predictors in 498,103 UK Biobank participants: a prospective population-based study. Lancet. 386(9993), 533-40 (2015).
[37] Public Health England. Low cost ways to increase NHS Health Check attendance: results from a randomised controlled trial. PHE publication gateway number: 2015284. August 2015. www.healthcheck.nhs.uk/document.php?o=943 Accessed 27 November 2017.
[38] Lau EY, Liu J, Archer E, McDonald SM, Liu J. Maternal weight gain in pregnancy and risk of obesity among offspring: a systematic review. J Obes. 2014, Article ID: 524939, 16 pp (2014).
[39] Woringer M, Cecil E, Watt H et al. Evaluation of community provision of a preventive cardiovascular programme - the National Health Service Health Check in reaching the under-served groups by primary care in England: cross sectional observational study. BMC Health Serv Res. 17(1), 405-416 (2017).
*[40] Khoury MJ. Precision Public Health and Precision Medicine: Two Peas in a Pod. Centers for Disease Control and Prevention. Genomics and Health Impact Blog. 2 March 2015. https://blogs.cdc.gov/genomics/2015/03/02/precision-public/ Accessed 7 July 2016.
[41] Needham BL, Carroll JE, Diez Roux AV, Fitzpatrick AL, Moore K, Seeman TE. Neighbourhood characteristics and leukocyte telomere length: the Multi-Ethnic Study of Atherosclerosis. Health Place. 28, 167-172 (2014).
[42] Theall KP, Brett ZH, Shirtcliff EA, Dunn EC, Drury SS. Neighbourhood disorder and telomeres: connecting children's exposure to community level stress and cellular response. Soc Sci Med. 85, 50-58 (2013).
[43] Yen YC, Lung FW. Older adults with higher income or marriage have longer telomeres. Age Ageing 42(2), 234-239 (2013).

Precision in Public Health 17
[44] Honig LS, Kang MS, Schupf N, Lee JH, Mayeux R. Association of shorter leukocyte telomere repeat length with dementia and mortality. Arch Neurol. 69, 1332-1339 (2012).
[45] Shiels PG, McGlynn LM, MacIntyre A et al. Accelerated telomere attrition is associated with relative household income, diet and inflammation in the pSoBid cohort. PLoS One 6, e22521 6pp (2011).
*[46] UK Prevention Research Partnership https://www.mrc.ac.uk/funding/browse/ukprp/uk-prevention-research-partnership-ukprp-consortium-and-network-awards/. Accessed 26 November 2017.
Starred references*[20] This paper provides important evidence for the effectiveness of socialised prevention.
*[23] This document indicates an understanding from government that improving health is a multi-stakeholder task rather than a task for individual citizens and their clinicians alone.
*[30] This paper illustrates the power of epigenetic biomarkers to ascertain different risks of various health events.
*[32] This document advises government of an important measure to ensure cross-departmental organisation to ensure an end to the obesity epidemic.
*[40] This blog was an important early contribution to the development of concepts in Precision Public Health.
*[46] This document indicates the start of a funding response to the challenge of advancing primary prevention of disease.