-
8/2/2019 Excretion I
1/27
-
8/2/2019 Excretion I
2/27
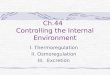
Renal
vein
Inferior
vena cava
Urinary
bladder
Urethra
Renal
artery
Kidney
Aorta
Ureter
Renal
pyramid
Renal
cortex
Renal
medulla
Renal
pelvis
Ureter
-
8/2/2019 Excretion I
3/27
Figure 26.4a, b
Structure of the Kidney
-
8/2/2019 Excretion I
4/27
Nephron
Afferent arteriole
Efferent arteriole
-
8/2/2019 Excretion I
5/27
Blood Supply to Kidney
-
8/2/2019 Excretion I
6/27
Two Capillary system
Glomerular capillary system - high
pressure, filtration system
Peritubular capillaries - low pressure,
absorptive system
-
8/2/2019 Excretion I
7/27
The nephron consists of a renal
corpuscle and renal tubule
The renal corpuscle is composed of
Bowmans capsule and the glomerulus
The renal tubule consists of
Proximal convoluted tubule (PCT)
Loop of Henle: Thin descending limb, Thin ascending limband
Thick ascending limb
Distal convoluted tubule (DCT)
-
8/2/2019 Excretion I
8/27
Cortical nephrons
~85% of all nephrons
Located in the cortex Juxtamedullary nephrons
Closer to renal medulla
Loops of Henle extenddeep into renal pyramids
Two types of nephron
-
8/2/2019 Excretion I
9/27
Urine Formation
-
8/2/2019 Excretion I
10/27
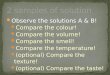
Figure 14.8 (1)
Page 518
Afferent arteriole Efferent arteriole
Glomerulus
Bowmans
capsule
Lumen of
Bowmans
capsule
Outer layer of
Bowmans capsule
Inner layer
of Bowmans capsule
(podocytes)
Proximal convoluted tubule
Lumen of
glomerular
capillary
Endothelial
cell
Basement
membrane
Podocyte
foot process
(see
nextslide)
-
8/2/2019 Excretion I
11/27
Podocyte
foot process
Filtrationslit
Basement
membrane
Capillarypore
(see next slide)3 Layers of Glomerular Capillary Membrane
Endothelial layer of capillaries
Basement membrane
Capsular layer with podocytes
Glomerular ultrafiltration Membrane
-
8/2/2019 Excretion I
12/27
Podocyte
foot process
Filtration
slit
Basement
membrane
Capillary
pore
Endothelial
cell
Lumen of glomerular
capillary
Lumen of
Bowmans capsule
-
8/2/2019 Excretion I
13/27
Mesangial Cells
Intra-mesangial cells liebetween capillary tuft and
provide support for
glomeruli. They secrete a
substance similar to basement
mebrane.
Extra mesnagial cells have
contractile properties in
response to neurohormonal
substance which regulateblood flow in glomerulus.
They are also phagocytic in
nature.
-
8/2/2019 Excretion I
14/27
Glomerular filtration Movement of fluid through the glomerular
capillaries is determined
by capillary pressure (60 mm Hg), colloidal osmotic pressure,
andcapillary permeability.
125 ml of filtrate is formed each minute - (GFR) which can
vary
from a few milliliters per minute to as high as 200
ml/minute.
Constriction of the efferent arteriole increases resistance to
outflowfrom the glomeruli and increases the glomerular pressure and
the
GFR. Constriction of the afferent arteriole causes a reduction
in the
renal blood flow, glomerular filtration pressure, and GFR.
Both, afferent and the efferent arterioles are innervated by
thesympathetic nervous system and are sensitive to vasoactive
hormones, such as angiotensin II.
Strong sympathetic stimulation, such as shock, constriction of
the
afferent arteriole causes a marked decrease in renal blood flow
and
thus glomerular filtration pressure & urine output can be
zero.
-
8/2/2019 Excretion I
15/27
Facilitated diffusion and Passive transport
Primary active transport
Secondary active transport
Cotransport (Symporter)
Countertransport (Antiporter)
Reabsorption in the kidneys
occurs by different mechanisms
R b i i PCT
-
8/2/2019 Excretion I
16/27
Reabsorption in PCT
65% of reabsorption and
secretion occurs in PCT.
Glucose amino acids, lactateand water soluble vitamins,
ions such Na+, Cl-, K+,
HCO3- completely
reabsorbed.
As these solutes move into the
tubular cells, their
concentration in the tubular
lumen decreases, providing a
concentration gradient for theosmotic reabsorption of water
and urea.
PCT secretes H+ and organic
compounds such as penicillin,
aspirin, morphine.
-
8/2/2019 Excretion I
17/27
Reabsorption of Bicarbonate & Na+ &
Secretion of H + Ions
Na+ antiporters reabsorb Na+
and secrete H+
PCT cells produce the H+ &
release bicarbonate ion to theperitubular capillaries
important buffering system
For every H+ secreted into the
tubular fluid, one filtered
bicarbonate eventually returns
to the blood
-
8/2/2019 Excretion I
18/27
Reabsorption in the PCT Na+ symporters help reabsorb
materials from the tubular filtrateand each type of symporter
has an
upper limit on how fast it can
work, called the transport
maximum (Tm).
The maximum amount of
substance that these transport
systems can reabsorb per unit
time is called the transport
maximum.
Tm related elated to the number
of carrier proteins that are
available for transport.
Reabsorption of Nutrients
-
8/2/2019 Excretion I
19/27
Tm determines renal threshold for reabsorption of substances
in
tubular fluid
-
8/2/2019 Excretion I
20/27
Symporters in the Loop of Henle
Thin descending limb is
highly permeable to waterand moderately permeable to
urea, sodium, and other ions
Thick ascending limb is
impermeable to water & hasNa+ K- Cl- symporters that
reabsorb these ions.
About 20% to 25% of the
filtered load of sodium,potassium, and chloride is
reabsorbed in loop of Henle.
-
8/2/2019 Excretion I
21/27
Reabsorption in the DCT & Collecting Duct
DCT is relatively impermeable to water
but removal of Na+ and Cl- (5%)
continues in the DCT by means of Na+
Cl- symporters
Ca++ actively reabsorbed under the
influence of parathyroid hormone and
vitamin D. ADH exerts its action on DCT.
Late part of DCT and collecting duct are
the sites for aldosterone action .
Two types of cells:
- principal cells reabsorb Na+ and secrete
K+ under the influence of aldosterone
- intercalated cells reabsorb HCO3- ions in
exchange for H+
-
8/2/2019 Excretion I
22/27
Formation of Concentrated Urine
Urine can be up to 4 times greater osmolarity than plasma It is
possible for principal cells & ADH to remove water from
urine
to that extent, if interstitial fluid surrounding the loop of
Henle has
high osmolarity
Long loop juxtamedullary nephrons and Na+/K+/Cl- makethat
possible
Two factors contribute to building and maintaining the
osmotic
gradient:
Difference in solute & water reabsorption in
differentsections of the tubule
Countercurrent flow
Urea recycling causes a buildup of urea in the renal medulla
F i f C U i ADH
-
8/2/2019 Excretion I
23/27
Formation of Con. Urine: ADH
Increases water permeability ofprincipal cells so
regulatesfacultative water reabsorption
Stimulates the insertion of
aquaporin-2 channels into themembrane
water molecules move morerapidly
When osmolarity of plasma &interstitial fluid increases,
moreADH is secreted and facultativewater reabsorption
increases.
-
8/2/2019 Excretion I
24/27
Tubular
lumen
filtrate Distal tubular cell
Peritubular
capillary
plasma
Water
channel
Increases permeability of
luminal membrane to H2O
by inserting newwater channels
-
8/2/2019 Excretion I
25/27
Countercurrent Mechanism Descending limb is very permeable to
water
higher osmolarity of interstitial fluid outside thedescending
limb causes water to mover out of the tubuleby osmosis
at hairpin turn, osmolarity can reach 1200 mOsm/liter
Ascending limb is impermeable to water, but symportersremove Na+
and Cl- so osmolarity drops to 100mOsm/liter, but less urine is
left
Vasa recta blood flowing in opposite directions than theloop of
Henle -- provides nutrients & O2 without affectingosmolarity of
interstitial fluid
-
8/2/2019 Excretion I
26/27
Reabsorption within Loop of Henle
-
8/2/2019 Excretion I
27/27























![Excretion [2015]](https://img.pdfslide.us/doc/110x75/55d39c87bb61eb05278b46dd/excretion-2015-55d47f0693bf7.jpg)


