Embed Size (px)
Citation preview

Clinical Trials: Immunotherapy
Exceptional Response to Pembrolizumab in aMetastatic, Chemotherapy/Radiation-ResistantOvarianCancer PatientHarboringaPD-L1-GeneticRearrangementStefania Bellone1, Natalia Buza2, Jungmin Choi3, Luca Zammataro1, Laurie Gay4,Julia Elvin4, David L. Rimm2,Yuting Liu2, Elena S. Ratner1, Peter E. Schwartz1, andAlessandro D. Santin1
Abstract
Purpose: Ovarian carcinoma no longer responsive to surgeryand chemotherapy remains an incurable disease. Alternativetherapeutic options remain desperately needed.
Patients and Methods: We describe a heavily pretreatedpatient with ovarian cancer with recurrent disease experiencinga remarkable clinical response to treatment with the anti-PD1immune checkpoint inhibitor pembrolizumab. The clinical,pathological, and genomic characteristics of this exceptionalovarian cancer responder were carefully investigated usingimmunohistochemistry (IHC), quantitative multiplex fluo-rescence methods (i.e., automated quantitative analysis,AQUA) and whole-exome sequencing (WES) techniques.
Results: The patient harbored a recurrent/metastatic radiationand chemotherapy-resistant high-grade ovarian carcinoma withclear cell features. While progressing on any standard treatmentmodality, she demonstrated a remarkable complete response to theanti-PD1 immune checkpoint inhibitor pembrolizumab. WES
results were notable for the presence a relative low number ofmutations (tumor mutation load/Mb ¼ 4.31, total mutations ¼164) and a peculiar structural variant disrupting the 30 region of thePD-L1 gene causingaberrant PD-L1 surface expressionas confirmedby IHC and AQUA technology. Heavy infiltration of the PD-L1–mutated andPD-L1–overexpressing tumorwith T-cell lymphocytes(i.e., CD4þ/CD8þ TIL), CD68þ macrophages, and CD20þ B cellswas detected in the surgical specimen strongly suggesting immuneevasion as a keymechanismof tumor growthand survival. Patient'scomplete clinical responses remain unchanged at the time of thewritingof this reportwithno significant sideeffects reported todate.
Conclusions: Anti-PD1 inhibitors may represent a novel treat-ment option for recurrent/metastatic human tumors refractoryto salvage treatment harboring PD-L1 gene structural variationscausing aberrant PD-L1 expression. Clin Cancer Res; 24(14); 3282–91.�2018 AACR.
See related commentary by Lheureux, p. 3233
IntroductionOvarian carcinoma remains the cancer with the highest mor-
tality rate among gynecologic tumors. In 2017, 22,440 new casesof ovarian carcinoma are predicted in the United States, with14,080 deaths secondary to this disease (1). While themajority ofpatients with advanced-stage disease (i.e., stages III–IV) initiallyrespond to first-line therapy based on cytoreductive surgery andplatinum-based chemotherapy, ovarian cancer will recur in themajority of cases. Overall, the 5-year survival rate for FIGO(International Federation of Gynecologists and Obstetricians)stage III disease is 20% to 25% and for stage IV disease is only
5% (2). These figures illustrate the dire need for the developmentof novel, more effective approaches for the treatment of chemo-therapy-resistant ovarian cancer.
Next-generation sequencing (NGS) studies from The CancerGenome Atlas (TCGA) network and other research groups haverecently demonstrated that high-grade serous ovarian cancer, themost common histological type of ovarian carcinoma, is charac-terized by TP53 mutations in over 96% of cases, a relative lownumber of single-nucleotide variants (SNVs) when comparedwith other gynecologic and non-gynecologic tumors and a wide-spread copy-number variants (CNVs), a genetic signature corre-lated with high genomic instability (3, 4).
In the last few years, the successful treatment of a variety ofhuman patients with cancer using antibodies against pro-grammed cell death 1 (PD1) and its ligand PD-L1 (CD274) hasdemonstrated the intrinsic immunogenicity of at least a subset ofhuman tumors and the critical importance of the PD-1/PD-L1 axisin tumor immune evasion. In some of these trials, a high muta-tional tumor burden and a high expression of PD-L1 protein onthe surface of human tumors have been identified as predictivebiomarkers for the identification of patients most likely torespond to the immunotherapy treatment (5). However, themechanisms controlling response to current immune checkpointinhibitors remain poorly understood as demonstrated by the factthat some human tumors with low mutation burden and/or
1Department of Obstetrics and Gynecology and Reproductive Sciences, YaleUniversity School of Medicine, New Haven, Connecticut. 2Department of Pathol-ogy, Yale University School of Medicine, New Haven, Connecticut. 3Departmentof Genetics, Yale University School of Medicine, New Haven, Connecticut.4Foundation Medicine, Cambridge, Massachusetts.
Note: Supplementary data for this article are available at Clinical CancerResearch Online (http://clincancerres.aacrjournals.org/).
Corresponding Author: Alessandro D. Santin, Yale University School of Med-icine, 333 Cedar Street, PO Box 208063, New Haven, CT 06520-8063. Phone:203-737-4450; Fax: 203-737-4339; E-mail: [email protected]
doi: 10.1158/1078-0432.CCR-17-1805
�2018 American Association for Cancer Research.
ClinicalCancerResearch
Clin Cancer Res; 24(14) July 15, 20183282
on February 10, 2021. © 2018 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 19, 2018; DOI: 10.1158/1078-0432.CCR-17-1805

lacking expression of PD-L1 may still respond to checkpointblockade (5, 6).
Several studies have recently investigated whether PD-L1expression is associated with tumor-infiltrating T cells (TILs) anda favorable prognosis in patients with ovarian cancer (7–11), andmultiple antibodies directed against PD1 or PD-L1 are currentlybeing tested in clinical trials (for review see ref. 11).Whilemany ofthese studies are currently ongoing or waiting for results tomature, few have been published. For example, Hamanischi andcolleagues (12) treated 20 patients with platinum-resistant ovar-ian cancer with an intravenous infusion of nivolumab every 2weeks at a dose of 1 or 3 mg/kg. The best overall response was15%, which included two patients who had a durable completeresponse (in the 3mg/kg cohort). The disease control rate in all 20patients was 45%. Of interest, complete responses were seen inpatients with ovarian cancer with both serous and clear cellhistology (12). Varga and colleagues reported on the activity ofpembrolizumab in the ovarian cancer cohort of advanced ovarianepithelial, fallopian tube, or primary peritoneal carcinomapatients with PD-L1þ tumors treated within the KEYNOTE-028(NCT02054806) study. Out of the 26 patients enrolled, the bestoverall (confirmed) response was 11.5%with one patient achiev-ing a complete response and two patients experiencing partialresponses (13). Disis and colleagues recently reported on 124patients with recurrent/refractory ovarian cancer treated withavelumab (i.e., anti–PD-L1 humanized antibody;NCT01772004;ref. 14). The overall response rate was 9.7% based on 12 partialresponses (14). Importantly, in all these trials, single-agent anti-PD1 or anti–PD-L1 antibodies showed an acceptable safety pro-file in heavily pretreated patients with ovarian cancer (11–14).
Here, we describe a patient with ovarian cancer treated withneoadjuvant chemotherapy, followed by surgery and progressingon radiation and multiple regimens of chemotherapy, experienc-ing an exceptional clinical response to anti-PD1 therapy (i.e.,pembrolizumab). An analysis of the pathological and genomiccharacteristics of the ovarian tumor demonstrated a low/inter-mediate number ofmutations byWES andaPD-L1 gene structuralvariation causing aberrant PD-L1 surface expression and heavyinfiltration of T lymphocytes in the tumor tissue. These resultsstrongly suggest immune evasion as a key mechanism of tumor
growth and survival for this chemotherapy/radiation resistantovarian cancer.
Patients and MethodsThis studywas conducted in accordancewith recognized ethical
guidelines, after approval by the institutional review board, andafter informed written consent was obtained from the patient.
IHCBriefly, for IHC, 4-mmsections were cut from the formalin-fixed
paraffin embedded (FFPE) blocks of the cancer patient collected atthe time of cytoreductive surgery and 79 additional high-gradeserous ovarian carcinoma from a recently described tissue micro-array ovarian cancer cohort (15), and stained with the followingantibodies according to the manufacturers' instructions: CD8(clone 144B, ready to use, DAKO), CD4 (clone 1F6, 1:40 dilution,Vector), CD3 (clone 2GV6, Ventana), CD56 (clone 1B6, 1:200dilution, Vector), CD68 (clone PG-M1, ready to use, DAKO),CD20 (clone L26, 1:200 dilution, DAKO), TIA-1 (clone TIA1,ready to use, Biocare), CK7 (clone OVTL, Dako), and PD-L1(clone E1L3N, 1:200 Cell Signaling). For antigen retrieval, thesections were pretreated at low pH for PD-L1 and CD8, CD4,CD20, CD56, and CD68. PD-L1 antibody and membranousimmunoreactivity was assessed semiquantitatively in tumor cellsas follows: <1% staining was considered negative, staining in 1%to 50% of tumor cells was scored as focal, and >50% staining wasscored as diffusely positive.
Quantitative multiplex fluorescence analysis of PD-L1expression
PD-L1 (Spring Bioscience; clone SP142; 1:800), CD68 (DAKO;clone PG-M1; 1:200), and CD8 (DAKO; clone C8/144B; 1:250)were used for immunofluorescence multiplex staining using apreviously descried method (16). Simultaneously, cytokeratinand DAPI were stained for detection of tumor and nucleus,respectively. Briefly, the patients' whole tissue section slides anda technical control tumor microarray slides (TMA; ref. 16) weredeparaffinized. Antigen retrieval was performed for 20minutes at97�C in the PT module from LabVision (Thermo Scientific), inEDTA pH8 buffer. Endogenous peroxidases were blocked for 30minutes in 2.5%hydrogenperoxide inmethanol and subsequent-ly blocked by 0.3% BSA in 0.05% tween with 30-minute incu-bation. The mixture of primary antibodies (PD-L1, CD68/CD8)was incubated overnight at 40�C in 0.3%BSA in TBST. For the PD-L1/CD68 multiplex panel, primary antibodies incubation wasfollowed by anti-mouse IgG3 secondary antibody (Abcam;ab97260; 1:1000) incubation in 0.3% BSA in TBST for an hourat room temperature to detect CD68. Signal was amplified withBiotinylated Tyramide (Perkin Elmer) at 1:50 dilution andAlexa750–streptavidin (Life Technologies) at 1:100. Following1-hour incubation, rabbit EnVisionreagent (Dako) was used fordetecting PD-L1 and amplified by Cyanine 5(Cy5) tyramide(Perkin Elmer) at 1:50 dilution. Cytokeratin was detected with1-hour incubation of anti-rabbit cytokeratin (Dako) at 1:100 andgoat anti-rabbit secondary antibody (Life Technologies) at 1:100.ProLongmountingmedium (Molecular Probes)was thefinal stepto stain nuclei with 4,6-diamidino-2-phenylindole (DAPI).Between each step, slides were washed using TBS/Tween and TBS,each for 2 minutes. For the PD-L1/CD8 multiplex panel, primaryantibodies were followed by anti-mouse IgG1 secondary anti-body (eBioscience) at 1:100, and signal was amplified with Plus
Translational Relevance
Patients with ovarian cancer developing chemotherapy-resistant disease have extremely limited therapeutic options.Recent next-generation sequencing (NGS) studies demonstrat-ed rare PD-L1 gene rearrangements, causing aberrant expres-sion of the extracellular domain of PD-L1 in a subset of humancancers. In preclinical models, these PD-L1 variants have beendemonstrated to confer high sensitivity to immune checkpointinhibitors targeting the PD1/PD-L1 axis. Here, we reportthe first clinical demonstration of the exquisite sensitivityto pembrolizumab of a patient with ovarian cancer withrecurrent/progressive disease resistant to surgery, chemother-apy, and radiation and harboring an aberrant PD-L1 expres-sion secondary to a 30-UTR disruption of the PD-L1 gene. Ourresults suggest that PD-L1 rearrangement may be used as agenetic marker to identify patients with cancer who are highlysensitive to anti-PD1 treatment.
Regression of CD274-Mutated Tumor with Pembrolizumab
www.aacrjournals.org Clin Cancer Res; 24(14) July 15, 2018 3283
on February 10, 2021. © 2018 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 19, 2018; DOI: 10.1158/1078-0432.CCR-17-1805

Cyanine 3 (Perkin Elmer) at 1:100. Similar steps were used in thispanel for staining PD-L1, cytokeratin, and DAPI.
Whole-exome sequencingBriefly, DNA was extracted from the patient's peripheral blood
as source of germinal DNA and FFPE tumor samples using aBiOstic FFPE Tissue DNA Isolation Kit (MO BIO Laboratories#12250-50) with a modified protocol. Genomic DNA was cap-tured on the NimbleGen 2.1M human exome array and subjectedto 74 base paired-end reads on the Illumina HiSeq 2000 instru-
ment as described (17). Sequence reads were mapped to thereference genome (hg19) using the ELAND program. Readsoutside the targeted sequences were discarded, and statistics oncoverage were collected from the remaining reads using in-housePerl scripts as previously described (17).
Verification of PD-L1/PLGRKT rearrangement by RT-PCR andSanger sequencing
Briefly, genomic DNA derived from the patient's tumor wastested by real-time PCR using a Custom TaqMan Assay (ID
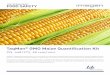
Figure 1.
Representative CAT scans demonstrating activity (i.e., complete response) to pembrolizumab. Left top: Pretreatment images with baseline measurement ofthe representative metastatic tumor deposit (i.e., pelvic/vaginal mass). Right top; stability of the lesion after three pembrolizumab infusions. Left and rightbottom: Complete regression of the metastatic tumor deposits after 16 and 24 weeks from treatment initiation with pembrolizumab.
Bellone et al.
Clin Cancer Res; 24(14) July 15, 2018 Clinical Cancer Research3284
on February 10, 2021. © 2018 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 19, 2018; DOI: 10.1158/1078-0432.CCR-17-1805

APTZ94T, Life Technologies Inc.) designed to specifically amplifythe region of interest. The forward primer (CTTCAAGCAGG-GATTCTCAACCT) was designed on the CD274 sequence whilethe reporter sequence (ATGGAACCCTTTTAGAACCC) and thereverse primer (GCCCCGATACCAGTATGACTTG) were designedto include part of the CD274 sequence and part of the PLGRKTinsertion. The detection of the genetic rearrangement in the tumorsample was confirmed by Sanger sequencing.
HLA typing and class I neoantigen predictionThe patient-specific four-digit HLA class I allele genotype was
assessed by ATHLATES (18) in silico using whole-exome sequenc-ing (WES) data. All somatic mutations including nonsynon-ymousmutations, frameshift insertions, and deletionswere trans-lated into 17-mer polypeptides flanking the mutant aminoacid. The binding affinity of wild-type and mutant nonamers tothe patient-specific HLA class I allele was predicted usingNetMHCcons (19) algorithms. Nonamers with IC50 below orequal to 500 nmol/L were further evaluated for the recognition by
the T-cell receptor using class I immunogenicity (20) resultingin putative neoantigens. The putative neoantigens were thenclassified as a strong binder (IC50 < 50 nmol/L), intermediatebinder (50 nmol/L < IC50 < 150 nmol/L), or weak binder (150nmol/L < IC50 < 500 nmol/L).
ResultsThe patient is an 80-year-old Caucasian woman originally
diagnosed in June 2014 with an advanced-stage, high-grade,ovarian carcinoma with clear cell features. The initial CAT scanrevealed extensive abdominal carcinomatosis, ascites, pelviclymphadenopathy, and a CA125 tumor marker elevated at1,810 U/mL (normal value less than 35 U/mL). After a diagnosticbiopsy she received six cycles of neoadjuvant chemotherapy (i.e.,carboplatin AUC 5 and paclitaxel 175 mg/m2) followed by aradical surgical procedure. Persistent widespread abdominal car-cinomatosis was found at the time of the interval debulkingsurgery with gross residual disease present in the omentum
Figure 2.
WES results. A, Quality assessment and quality control of sequencing data for tumor and matched normal samples. B, Somatic mutation classification.C, The distribution of six different substitution subtypes. D, Potential neoantigen classification. Strong: IC50 � 50 nmol/L, intermediate: 50 nmol/L < IC50
� 150 nmol/L, weak: 150 nmol/L < IC50 � 500 nmol/L. E, Integrative Genomics Viewer (IGV) plots showing genomic rearrangement involving the PD-L1 gene. Theevent consists in a translocation/insertion of a 50 32 nucleotide fragment from the exon 5 of the PLGRKT gene, in the 50 end of the PD-L1 gene, resulting in abreakpoint in exon 7 (30 UTR). Green reads indicate the tandem duplication. Gray reads display normal sequencing reads.
Regression of CD274-Mutated Tumor with Pembrolizumab
www.aacrjournals.org Clin Cancer Res; 24(14) July 15, 2018 3285
on February 10, 2021. © 2018 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 19, 2018; DOI: 10.1158/1078-0432.CCR-17-1805

(nodules up to 2.9 cm), ovaries, fallopian tubes, and pelvic lymphnodes. Final pathology was consistent with the prechemotherapybiopsy and demonstrated a high-grade adenocarcinoma of Mul-lerian origin with clear cell features most likely started in theovaries and treatment effect. Because of symptomatic neuropathy,postoperatively she received six additional cycles of carboplatin(AUC 5) and Topotecan (2mg/kg days 1 and 15) in combinationwith bevacizumab (10 mg/kg, days 1 and 15). The patientremained in remission until March 2015, when an MRI of thepelvic and abdomen followed by a PET/CT imaging revealed thepresence of recurrent disease in the pelvis (i.e., a mass of 2.6 cmabove the vaginal cuff). She was dispositioned to receive vaginalcuff brachytherapy followed by pelvic radiation in the form of 28fractions completed on July 7, 2015. Unfortunately, a PET/CTperformed on October 2015 demonstrated persistent/recurrent
disease with interval increase in size and hypermetabolism of thepelvic lesion involving the superior aspect of the vaginal cuff. Shewas therefore dispositioned to receive dose-dense paclitaxelprotein-bound particles (abraxane), initially at the dose of100 mg/m2 on days 1, 8, and 15 and subsequently dose-reducedto 80mg/m2 of a 28-day cycle in combination with bevacizumab(10 mg/kg, days 1 and 15). She did well until June 2016 when apelvic exam followed by a CAT scan guided biopsy of theenhancing 3.1- � 4.8-cm mass along the superior/cephaladborder of the vaginal cuff confirmed the presence of a metastat-ic/recurrent adenocarcinoma histological consistent with theoriginal high-grade mullerian tumor. On August 2016, she wasenrolled at Yale University within a phase II study of pembro-lizumab entitled "Efficacy and Safety Study of Pembrolizumab(MK-3475) in Women With Advanced Recurrent Ovarian
Figure 3.
WES results. Somatic mutations (SNVs), in cancer or immune-related genes and CNVs in cancer- and immune-related genes.
Bellone et al.
Clin Cancer Res; 24(14) July 15, 2018 Clinical Cancer Research3286
on February 10, 2021. © 2018 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 19, 2018; DOI: 10.1158/1078-0432.CCR-17-1805

Cancer" (MK-3475-100/KEYNOTE-100). Pembrolizumab wasadministered at a flat dose of 200 mg i.v. on day 1 of each 3-week cycle. CA125 tumor marker at this time was found elevatedat 230 U/mL. A CAT scan performed on October 2016 (i.e., afterthree pembrolizumab infusions) demonstrated stable disease(i.e., larger diameter of the pelvic/vaginal mass stable at 5.4 cmvs. 5.6 cm at baseline; Fig. 1, top). Strikingly, at the time of thesecond CAT scan imaging obtained 4 months from study initi-ation (i.e., December 2016, Fig. 1, left bottom), a remarkablecomplete response by RECIST v1.1 criteria was noted to theimmune checkpoint inhibitor. Confirmatory CAT scans obtained8 weeks later (i.e., February 2017, Fig. 1, right bottom) and inApril and June 2017 (data not shown) demonstrated a sustainedcomplete response of the large pelvic/vaginal tumor with no newlesions. The patient continued to improve in her performancestatus during treatment with the normalization of the CA125tumor marker. Per protocol, pembrolizumab treatment has beendiscontinued after the completion of a total of nine cycles oftreatment (24 weeks) and two cycles after the confirmatorycomplete response (i.e., CAT scan imaging). The patient's
remarkable clinical response remains unchanged at the time ofthe writing of this report with no side effects reported to date andthe patient experiencing good quality of life.
To gain additional knowledge in the genetic and pathologiccharacteristics of the patient's tumor demonstrating such exqui-site sensitivity to anti-PD1 treatment, we initially performed NGStesting using a commercially available platform (FoundationOne, FoundationMedicine (FM) Inc., a test sequencing the codingregion of 315 genes plus introns from 28 genes to amedian depthof coverage of greater than 500�; ref. 21) followed by WES(performed at the Center for Genome Analysis at Yale UniversitySchool ofMedicine).We found the ovarian carcinoma to harbor alow/intermediate number of mutations (i.e., tumor mutationburden, TMB ¼ 4.31 mut/Mb, total number of mutations ¼164; Fig. 2) when compared with 316 high-grade ovarian cancersamples previously reported by the Cancer Genome AtlasResearch Network (mean TMB ¼ 1.84 mut/Mb, total numberof mutations ¼ 61; ref. 3) and 114 high-grade ovarian cancersamples recently reported by Patch and colleagues (mean TMB ¼5.64 mut/Mb, total number of mutations ¼ 271; ref. 4). Using
Figure 4.
High-grade ovarian carcinoma withmarked peritumoral inflammatory cellinfiltrate (A). The tumor cells andperitumoral inflammatory cells showmoderate to intense membranousstaining with PD-L1 IHC (B). Tlymphocytes represent thepredominant component among theimmune cells, highlighted by CD4(C) and CD8 (D) immunostains. Blymphocytes (E: CD20 immunostain)and macrophages (F: CD68immunostain) are present in asmaller proportion. CD56 and TIAimmunostains were negative for NKcells (image not shown). (A: H&E stain,B: PD-L1 immunostain, C: CD4immunostain, D: CD8 immunostain,E: CD20 immunostain, F: CD68immunostain; all images at 200�original magnification).
Regression of CD274-Mutated Tumor with Pembrolizumab
www.aacrjournals.org Clin Cancer Res; 24(14) July 15, 2018 3287
on February 10, 2021. © 2018 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 19, 2018; DOI: 10.1158/1078-0432.CCR-17-1805

accurate typing of human leukocyte antigen through exomesequencing, we predicted a total of 40 potential neoantigensharbored in the tumor including 11 strong, nine intermediate,and 20 weak immunogenic antigens (Fig. 2). Somatic mutations(SNV), loss of heterozygosity (LOH), and copy-number variations(CNV) in the whole-exome-sequenced tumor are presentedin Fig. 3. Nonsynonymous mutations (i.e., SNV) in the TP53 andMLH1 genes (the later not causing microsatellite instability, datanot shown) and a stop mutation in TGF-b (a key player cytokineduring host–immune system interaction) amongst other muta-tionswere detected (Fig. 3). Gain of function in knownoncogenes(i.e., the PIK3CA gene on chromosome 3 and in c-MYC onchromosome 8) and in BCL2L1, a gene endowed with antiapop-totic properties and a crucial role in controlling survival duringlymphocyte development and following B- and T-cell activation,was also identified (Fig. 3). Of great interest, both FM and WEStesting demonstrated a peculiar PD-L1 gene rearrangement (i.e.,chr9 duplication event affecting the 50 endofPD-L1, breakpoint inexon 7 [30 untranslated region (30-UTR); Fig. 2E]. As described inthe Materials and Methods section, using primers specific for the
predicted fusion, RT-PCR, and Sanger sequencing, we confirmedthe detection of the genetic rearrangement in the tumor sample(Supplementary Fig. S1). The event consists of a translocation/insertion of a 32 nucleotide fragment from the exon 5 of thePLGRKT gene (plasminogen receptor, C-terminal lysine trans-membrane protein) in chr9:5361091–5361122 of the hg19assembly (Fig. 2E), into 30UTR of the PD-L1 gene. PLGRKT,however, remains intact after the tandemduplication event. Thesegenetic characteristics were found to differ from previously dem-onstrated gain of function of the PD-L1 gene secondary to geneamplification and, importantly, have recently been described in asubset of T-cell leukemia andB-cell lymphoma to lead to amarkedelevation of PD-L1 extracellular domain secondary to the stabi-lization of the PD-L1 transcripts through the truncation of the 30
-UTR of the PD-L1 gene (22). To confirm the potential highexpression of PD-L1 receptor on the surface of the ovarian tumorand thoroughly evaluate the presence or absence of lymphocyticinfiltrationwenext performedPD-L1 IHC testing andquantitativemultiplex fluorescence analysis in the tumor tissue. We foundstrong tumor cell expression for PD-L1 by IHC as well as heavy
Figure 5.
Detection of PD-L1 protein expression in tumor cells using immunofluorescence multiplexing panel. A–F,Multiplex IF panel of PD-L1 (red)/cytokeratin (green)/DAPI(blue)/CD68 (magenta) of the same region. A–D, Representative images of single channels (DAPI, CK, PD-L1, and CD68) of the multiplex IF panel. E,Representativefluorescence image showing the colocalizationof PD-L1 and cytokeratin. CD68þmacrophages donot express PD-L1.F,H&E staining.G–L,Multiplex IFpanel of PD-L1 (red)/cytokeratin (green)/DAPI (blue)/CD8 (magenta) of the same region. G–J, Representative images of single channels (DAPI, CK, PD-L1,CD8) of the multiplex IF panel. K, Representative fluorescence image showing the colocalization of PD-L1 (red) and cytokeratin (green). CD8 (magenta)þ T cells donot express PD-L1. L, H&E staining.
Bellone et al.
Clin Cancer Res; 24(14) July 15, 2018 Clinical Cancer Research3288
on February 10, 2021. © 2018 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 19, 2018; DOI: 10.1158/1078-0432.CCR-17-1805

intratumoral T lymphocytic (i.e., CD8 and CD4) and to a lowerextent B-cell (CD20) and histiocytic infiltration (i.e., CD68) byhematoxylin–eosin (H&E) stain and immunostains (Fig. 4).Using an immunofluorescence multiplexing panel (16), we con-firmed colocalization of PD-L1 with cytokeratin-positive tumorcells and negligible to no PD-L1 expression in infiltrating CD68þ
macrophages and CD8þ T lymphocytes (Fig. 5). Finally, wecompared PD-L1 expression in the patient's tumor with PD-L1expression in 79 cases of high-grade serous ovarian carcinomaavailable to our laboratory from a recently characterized tissuemicroarray (15). As representatively shown in Fig. 6, out of the 79tumors, only 15 (19%) showed focal PD-L1 expression in tumorcells while the remaining 64 cases (81%)were negative for PD-L1.None of the cases present in the TMA showed diffuse immuno-reactivity for PD-L1 as described in Fig. 4 for the patient withovarian cancer harboring the PD-L1–genetic rearrangement.
DiscussionRecurrent ovarian carcinoma resistant to salvage chemotherapy
treatments remains an incurable disease. In the last few years,multiple preclinical and clinical studies have demonstrated thatone mechanism by which multiple human cancers evade hostimmunity is via upregulation of PD1 ligand (PD-L1) and itsinteractionwith the PD1 ligandonantigen specific T-lymphocytes(5, 6). Consistent with this view, a variety of human tumors havedemonstrated sensitivity to immune checkpoint inhibitor anti-
bodies targeting PD1 or PD-L1 in vivo and, accordingly, pembro-lizumab (Merck & Co., Inc.), nivolumab (Bristol-Myers SquibbCompany), and atezulumab (Genentech/Roche) have recentlyreceived approval by the FDA for the treatment ofmultiple humanmalignancies. Unfortunately, however, a large number of patientstreated donot respond to immune checkpoint treatment and littleis currently known about the potential genetic mutations regu-lating response to the blockade of the PD1/PD-L1 axis.
We describe a heavily pretreated patient with ovarian cancerwith recurrent disease experiencing a complete and sustainedresponse to pembrolizumab. Remarkably, this ovarian cancerwas found exquisitely sensitive to the immune checkpoint block-ade regardless to its high resistance to chemotherapy and radia-tion as demonstrated by the complete disappearance of a largerecurrent tumor mass at 16 weeks from treatment initiationconfirmedwithmultiple serial CAT scans. Of interest, WES resultsdemonstrated the tumor to have a relatively low number ofmutations when compared with melanoma, lung cancer, ovariancancer (4), or gynecologic and non-gynecologic tumors charac-terized by high microsatellite instability (i.e., MSI-H endometrialand colorectal tumors; ref. 23). These data combined with ourresults predicting at least 40 potential neoantigens in the WEStumor suggest that a high tumor mutation burden may notrepresent a mandatory requirement for clinical response toimmune checkpoint inhibitors in patients with ovarian cancer.
Of great interest, we found the tumor to harbor a structuralvariation in the PD-L1 gene recently reported in about 27% of
Figure 6.
PD-L1 expression by IHC in representative high-grade ovarian serous carcinomas from the TMA.A, Focal PD-L1 expression (between 1% and 50%) in tumor cells.B–D,No PD-L1 expression is identified in tumor cells. All images at 200� original magnification.
www.aacrjournals.org Clin Cancer Res; 24(14) July 15, 2018 3289
Regression of CD274-Mutated Tumor with Pembrolizumab
on February 10, 2021. © 2018 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 19, 2018; DOI: 10.1158/1078-0432.CCR-17-1805

adult T-cell leukemia/lymphoma, 8% of B-cell lymphomaand 2% of patients with stomach cancer to lead to markedelevation of PD-L1 transcripts secondary to the truncation of the30-UTR of the PD-L1 gene (22). Importantly, this rare PD-L1mutation has recently been reported to provide high sensitivityto immune checkpoint inhibitor in preclinical animalmodels andspeculated to potentially confer high susceptibility to blockade ofthe PD-1/PD-L1 axis in human patients (22). Consistent withthese preclinical data in xenografted animals, we found ourpatient tumor to express high levels of the PD-L1 receptor andto be characterized by a high intratumoral CD8, CD4, and to alower extent CD20 B lymphocytic and macrophage (i.e., CD68)infiltration by IHC staining. Taken together, the relative lowtumor mutation burden, strong PD-L1 surface expression andheavy inflammatory infiltration of this ovarian cancer suggest thePD-L1 structural variation to be the reason of its exquisite sen-sitivity to immune checkpoint treatment. Mutations in otherimmunologically relevant genes such as TGF-beta and CD27werealso detected in the tumor. The possible influence of thesemutations on the exceptional response of this patient to pem-brolizumab are currently unclear.
In conclusion, to our knowledge, this is the first report dem-onstrating a remarkable clinical activity of an immune checkpointinhibitor in a patient harboring a rearrangement in the PD-L1gene.While thePD-L1 structural variationwe found in this patientwithovarian cancer seems tobe a rare event inhuman tumorswithonly 31 cases expressing 30-UTR-truncated PD-L1 transcript out of10,210 cancer samples from 33 tumor panel analyzed by TCGAreported to date (22), the exquisite sensitivity of this patient topembrolizumab suggests that such PD-L1 structural variants mayserve as genetic marker for the identification of human cancersselectively upregulating PD-L1 inorder to evade antitumor immu-nity. More importantly, these peculiar genetic characteristics maybe able to identify human tumors that regardless to their highresistant to surgery, chemotherapy, and radiation and a low
mutation burden may still be highly susceptible to immunecheckpoint PD1 blockade.
Disclosure of Potential Conflicts of InterestL. Gay and J.A. Elvin hold ownership interest (including patents) in Foun-
dation Medicine. D.L. Rimm reports receiving commercial research grants fromNavigate, other commercial research support from Perkin Elmer, and is aconsultant/advisory board member for Cell Signaling Technology. E. Ratneris a consultant/advisory board member for Tesaro. No potential conflicts ofinterest were disclosed by the other authors.
Authors' ContributionsConception and design: Y. Liu, P.E. SchwartzDevelopment of methodology: S. Bellone, Y. LiuAcquisition of data (provided animals, acquired and managed patients,provided facilities, etc.): S. Bellone, N. Buza, Y. Liu, E.S. Ratner, A.D. SantinAnalysis and interpretation of data (e.g., statistical analysis, biostatistics,computational analysis): S. Bellone, N. Buza, J. Choi, L. Zammataro, L. Gay,J. Elvin, D.L. Rimm, Y. Liu, P.E. Schwartz, A.D. SantinWriting, review, and/or revision of the manuscript: S. Bellone, N. Buza,J. Elvin, Y. Liu, P.E. Schwartz, A.D. SantinAdministrative, technical, or material support (i.e., reporting or organizingdata, constructing databases): S. Bellone
AcknowledgmentsThis work was supported in part by grants from NIH U01 CA176067-01A1,
the Deborah Bunn Alley Foundation, the Tina Brozman Foundation, theDiscovery to Cure Foundation, and the Guido Berlucchi Foundation toAlessandro D. Santin. This investigation was also supported by NIH researchgrant CA-16359 from the NCI.
The costs of publication of this article were defrayed in part by thepayment of page charges. This article must therefore be hereby markedadvertisement in accordance with 18 U.S.C. Section 1734 solely to indicatethis fact.
Received June 24, 2017; revised September 22, 2017; accepted January 12,2018; published first January 19, 2018.
References1. Siegel RL, Miller KD, Jemal A. Cancer statistics 2017. CA Cancer J Clin
2017;67:7–30.2. Creasman DiSaia, DiSaia PJ, Creasman WT (eds.). Clinical gynecologic
oncology, 8th ed. Philadelphia, PA: Saunders Elsevier Inc.; 2012.3. Cancer Genome Atlas Research Network. Integrated genomic analyses of
ovarian carcinoma. Nature 2011;474:609–15.4. PatchAM,Christie EL, EtemadmoghadamD,GarsedDW,George J, Fereday
S, et al. Whole-genome characterization of chemoresistant ovarian cancer.Nature 2015;521:489–94.
5. Tumeh PC, Harview CL, Yearley JH, Shintaku IP, Taylor EJ, Robert L, et al.PD-1 blockade induces responses by inhibiting adaptive immune resis-tance. Nature 2014;515:568–71.
6. Postow MA, Callahan CL, Wolchock JD. Immune checkpoint blockade incancer therapy. J Clin Oncol 2015;33:1974–82.
7. Webb JR, Milne K, Kroeger DR, Nelson BH. PD-L1 expression is associatedwith tumor-infiltrating T cells and favorable prognosis in high-grade serousovarian cancer. Gynecol Oncol 2016;141:293–302.
8. Darb-Esfahani S, Kunze CA, Kulbe H, Sehouli J, Wienert S, Lindner J, et al.Prognostic impact of programmed cell death-1 (PD-1) and PD-ligand 1(PD-L1) expression in cancer cells and tumor-infiltrating lymphocytes inovarian high grade serous carcinoma. Oncotarget 2016;7:1486–99.
9. Wang X, Teng F, Kong L, Yu J. PD-L1 expression in human cancers and itsassociation with clinical outcomes. Onco Targets Ther 2016;9:5023–39.
10. Hamanishi J, Mandai M, Iwasaki M, Okazaki T, Tanaka Y, Yamaguchi K,et al. Programmed cell death 1 ligand 1 and tumor-infiltrating CD8þ Tlymphocytes are prognostic factors of human ovarian cancer. Proc NatlAcad Sci U S A 2007;104:3360–5.
11. Gaillard SL, Secord AA,Monk B. The role of immune checkpoint inhibitionin the treatment of ovarian cancer. Gynecol Oncol Res Pract 2016;3:11.
12. Hamanishi J, Mandai M, Ikeda T, Minami M, Kawaguchi A, Murayama T,et al. Safety and antitumor activity of anti-PD-1 antibody, nivolumab, inpatients with platinum-resistant ovarian cancer. J Clin Oncol 2015;33:4015–22.
13. Varga A, Piha-Paul SA, Ott PA, Mehnert JM, Berton-Rigaud D, Johnson EA,et al. Antitumor activity and safety of pembrolizumab inpatients (pts)withPD-L1 positive advanced ovarian cancer: interim results from a phase Ibstudy. J Clin Oncol 2015:33(suppl; abstr 5510).
14. Disis ML, Patel MR, Pant S, Hamilton EP, Lockhart AC, Kelly K, et al.Avelumab (MSB0010718C; anti-PD-L1) in patients with recurrent/refrac-tory ovarian cancer from the JAVELIN solid tumor phase Ib trial: safety andclinical activity. J Clin Oncol 2016:34(suppl; abstr5533).
15. Carvajal-Hausdorf DE, Schalper KA, Bai Y, Black J, Santin AD, Rimm DL.Objective, domain-specific HER2 measurement in uterine and ovarianserous carcinomas and its clinical significance. Gynecol Oncol 2017;145:154–8.
16. Velcheti V, Schalper KA, Carvajal DE, Anagnostou VK, Syrigos KN, SznolM,et al. Programmeddeath ligand-1 expression in non–small cell lung cancer.Lab Invest 2014;94:107–16.
17. Zhao S, ChoiM, Overton JD, Bellone S, Roque D, Cocco E, et al. Landscapeof somatic single-nucleotide and copy-numbermutations in uterine serouscarcinoma. Proc Natl Acad Sci U S A 2013;110:2916–21.
18. Liu C, Yang X, Duffy B, Mohanakumar T, Mitra RD, Zody MC, et al.ATHLATES: accurate typing of human leukocyte antigen through exomesequencing. Nucleic Acids Res 2013;41:e142.
Clin Cancer Res; 24(14) July 15, 2018 Clinical Cancer Research3290
Bellone et al.
on February 10, 2021. © 2018 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 19, 2018; DOI: 10.1158/1078-0432.CCR-17-1805

19. Karosiene E, Lundegaard C, LundO,NielsenM.NetMHCcons: a consensusmethod for the major histocompatibility complex class I predictions.Immunogenetics 2012;64:177–86.
20. Calis JJ,MaybenoM,Greenbaum JA,WeiskopfD,De SilvaAD, Sette A, et al.Properties of MHC class I presented peptides that enhance immunogenic-ity. PLoS Comput Biol 2013;9:e1003266.
21. Frampton GM, Fichtenholtz A, Otto GA, Wang K, Downing SR, He J, et al.Development and validation of a clinical cancer genomic profiling test
based on massively parallel DNA sequencing. Nat Biotechnol 2013;31:1023–31.
22. Kataoka K, Shiraishi Y, Takeda Y, Sakata S, Matsumoto M, Nagano S, et al.Aberrant PD-L1 expression through 30-UTR disruption inmultiple cancers.Nature 2016;534:402–6.
23. Alexandrov LB, Nik-Zainal S, Wedge DC, Aparicio SAJR, Behjati S, BiankinAV, et al. Signatures of mutational processes in human cancer. Nature2013;500:415–21.
www.aacrjournals.org Clin Cancer Res; 24(14) July 15, 2018 3291
Regression of CD274-Mutated Tumor with Pembrolizumab
on February 10, 2021. © 2018 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 19, 2018; DOI: 10.1158/1078-0432.CCR-17-1805

2018;24:3282-3291. Published OnlineFirst January 19, 2018.Clin Cancer Res Stefania Bellone, Natalia Buza, Jungmin Choi, et al. Harboring a PD-L1-Genetic RearrangementChemotherapy/Radiation-Resistant Ovarian Cancer Patient Exceptional Response to Pembrolizumab in a Metastatic,
Updated version
10.1158/1078-0432.CCR-17-1805doi:
Access the most recent version of this article at:
Material
Supplementary
http://clincancerres.aacrjournals.org/content/suppl/2018/01/19/1078-0432.CCR-17-1805.DC1
Access the most recent supplemental material at:
Cited articles
http://clincancerres.aacrjournals.org/content/24/14/3282.full#ref-list-1
This article cites 20 articles, 4 of which you can access for free at:
Citing articles
http://clincancerres.aacrjournals.org/content/24/14/3282.full#related-urls
This article has been cited by 2 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/24/14/3282To request permission to re-use all or part of this article, use this link
on February 10, 2021. © 2018 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 19, 2018; DOI: 10.1158/1078-0432.CCR-17-1805