Embed Size (px)
Citation preview

Excelling in heart failure care
Dr Alex Simms, Consultant Cardiologist
Outline
▪ What is heart failure
▪ Why is it important
▪ Diagnosis
▪ Care in Primary Care
▪ Modern management
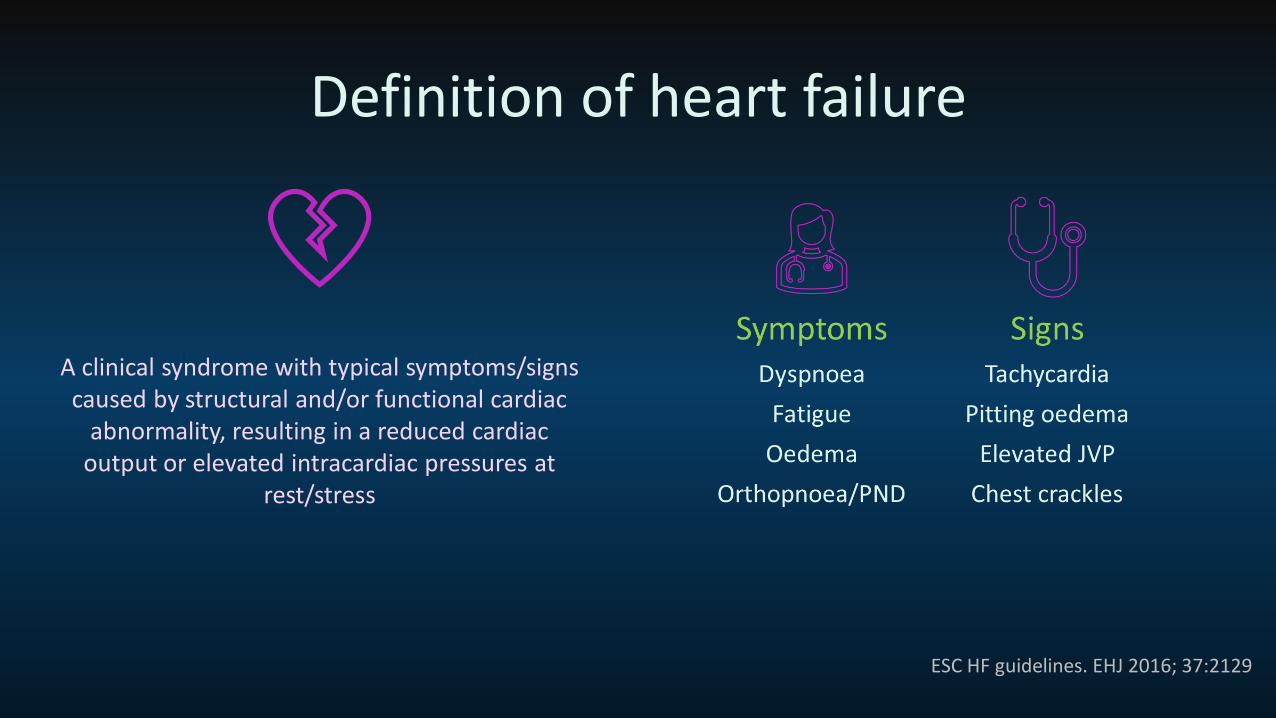
Definition of heart failure
A clinical syndrome with typical symptoms/signs caused by structural and/or functional cardiac
abnormality, resulting in a reduced cardiac output or elevated intracardiac pressures at
rest/stress
ESC HF guidelines. EHJ 2016; 37:2129
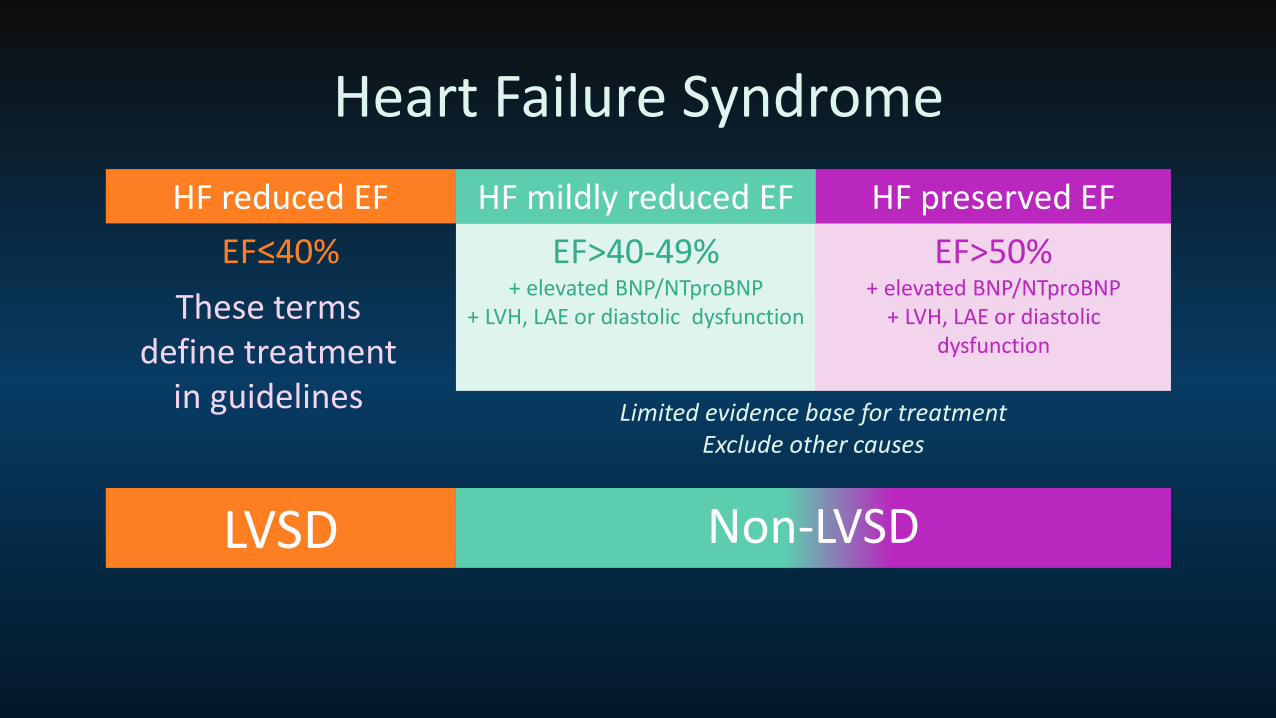
Heart Failure Syndrome
HF reduced EF HF mildly reduced EF HF preserved EF
EF≤40% EF>40-49%+ elevated BNP/NTproBNP
+ LVH, LAE or diastolic dysfunction
EF>50%+ elevated BNP/NTproBNP
+ LVH, LAE or diastolic dysfunction
Limited evidence base for treatmentExclude other causes
These terms define treatment
in guidelines
LVSD Non-LVSD
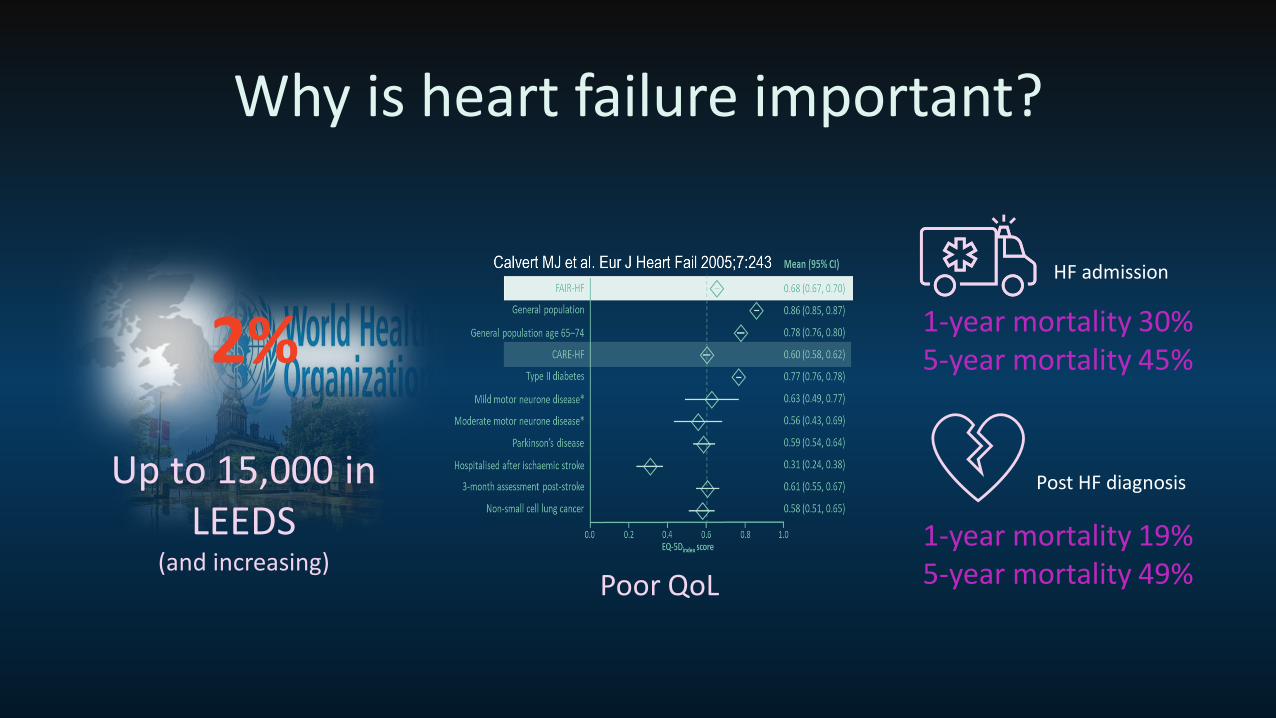
Why is heart failure important?
2%
Up to 15,000 in LEEDS
(and increasing)Poor QoL
1-year mortality 30% 5-year mortality 45%
HF admission
Post HF diagnosis
1-year mortality 19% 5-year mortality 49%
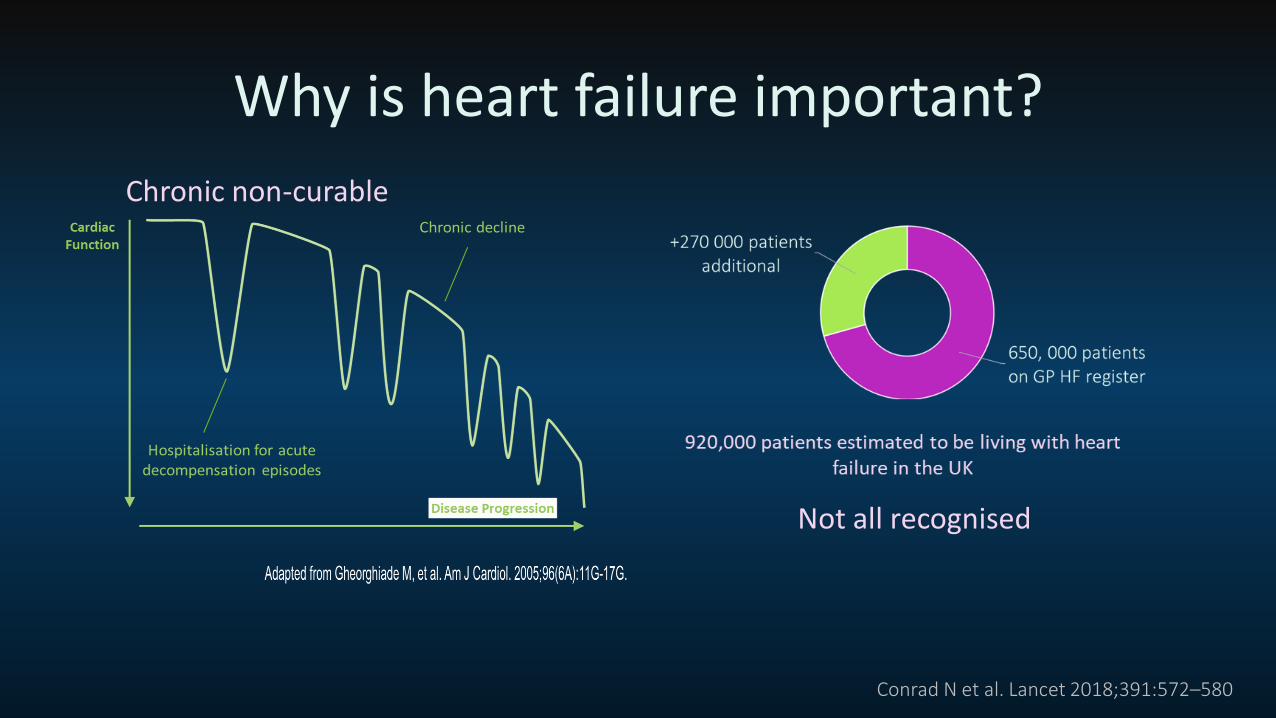
Why is heart failure important?
Conrad N et al. Lancet 2018;391:572–580
Not all recognised
Chronic non-curable
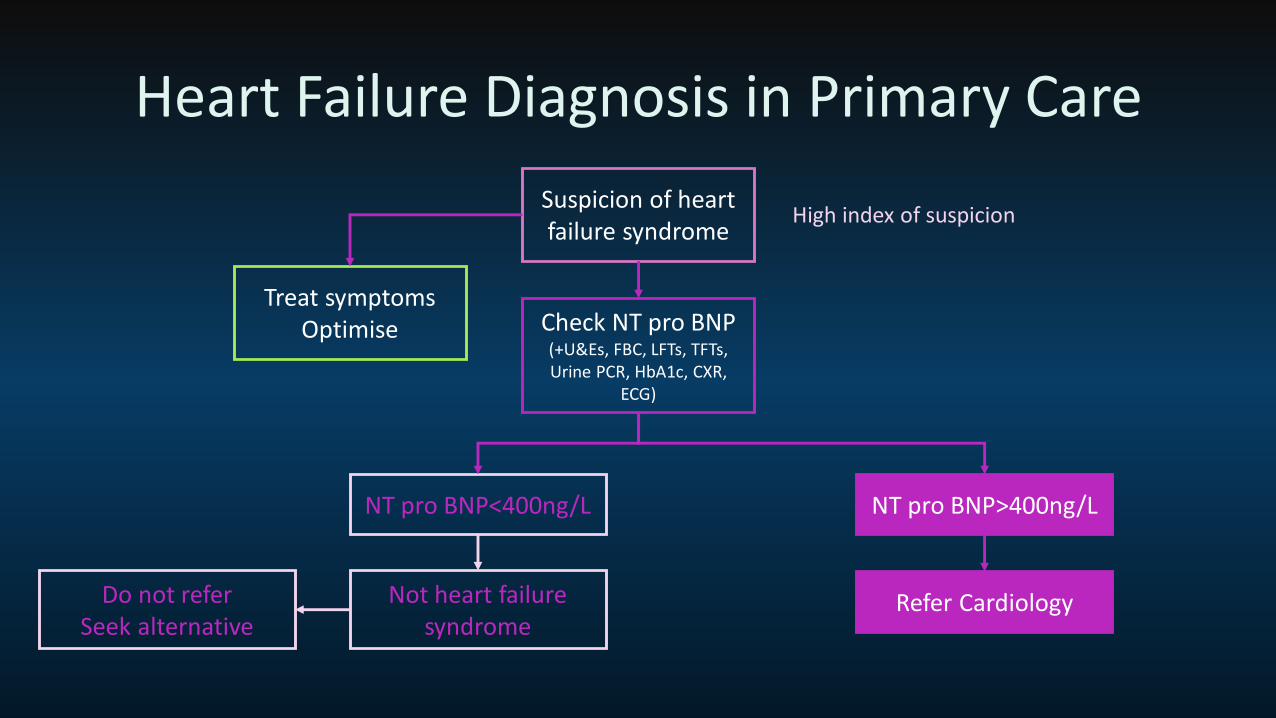
Heart Failure Diagnosis in Primary Care
Suspicion of heart failure syndrome
High index of suspicion
Treat symptomsOptimise Check NT pro BNP
(+U&Es, FBC, LFTs, TFTs, Urine PCR, HbA1c, CXR,
ECG)
NT pro BNP<400ng/L NT pro BNP>400ng/L
Not heart failure syndrome
Do not referSeek alternative
Refer Cardiology

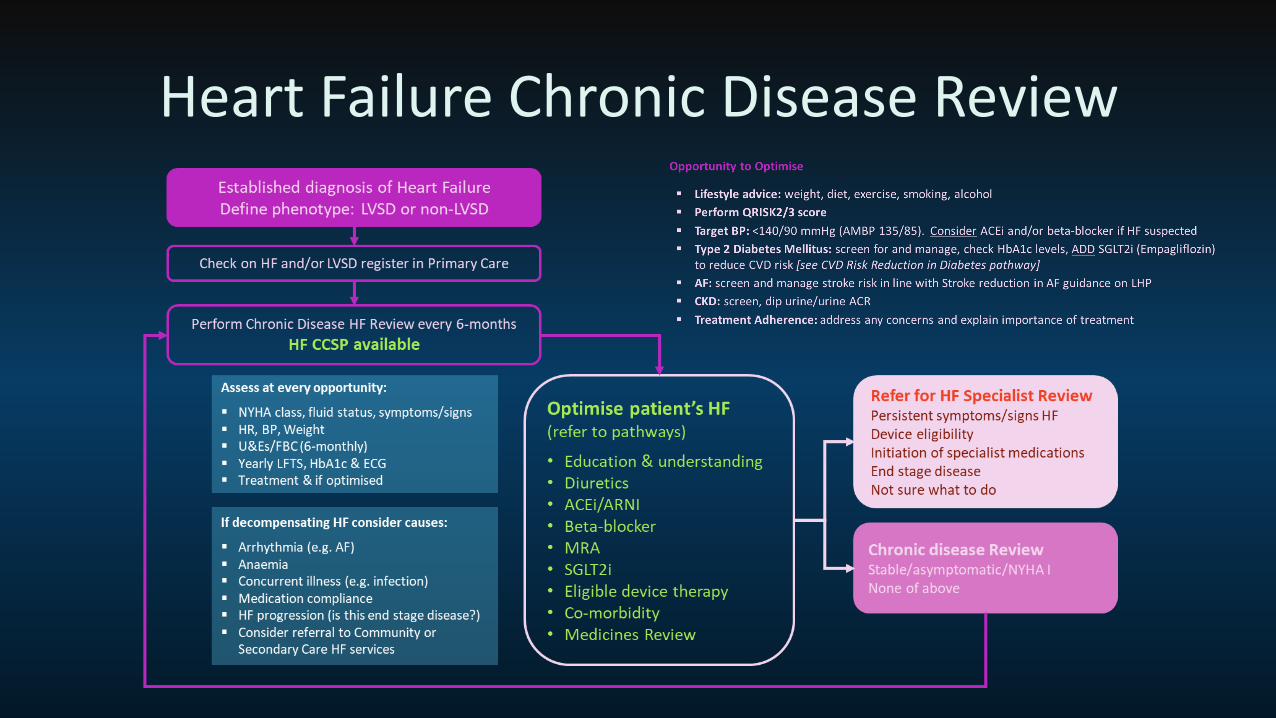
Heart Failure Chronic Disease Review
Can we do better?
Heart Failure Chronic Disease Review
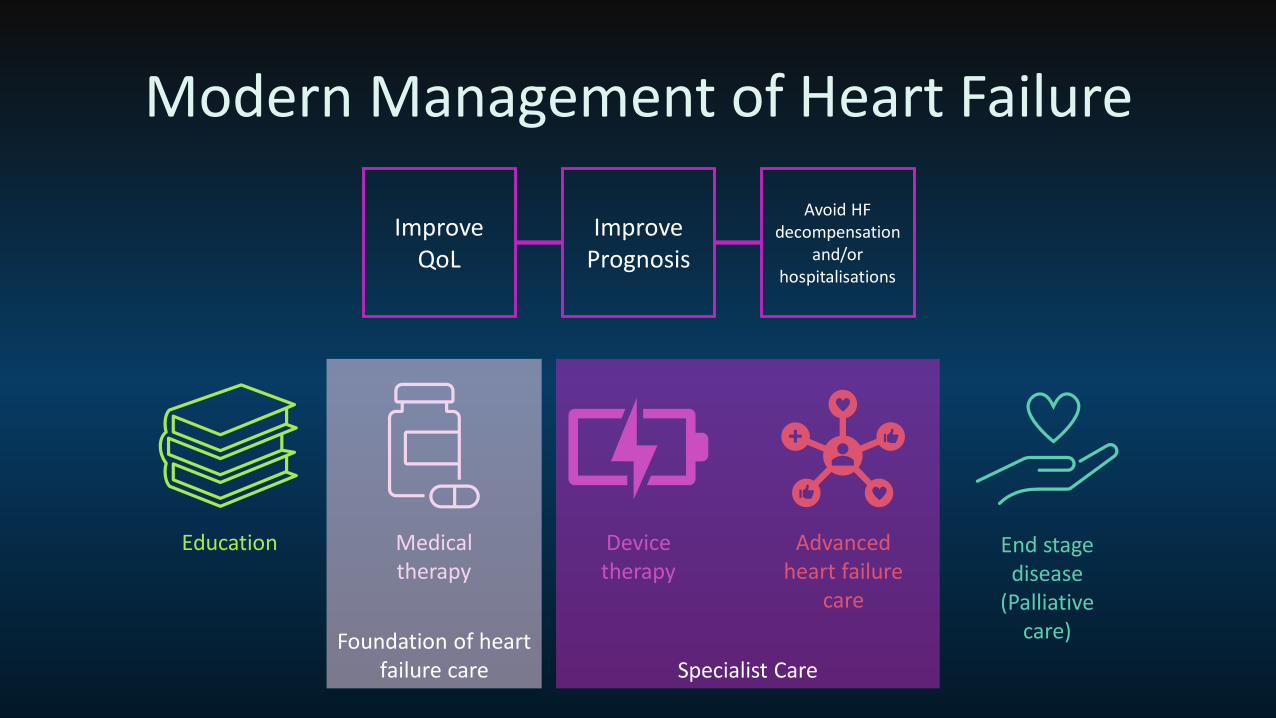
Modern Management of Heart Failure
Improve QoL
Improve Prognosis
Avoid HF decompensation
and/or hospitalisations
Education Medical therapy
Device therapy
Advanced heart failure
care
End stage disease
(Palliative care)Foundation of heart
failure care Specialist Care
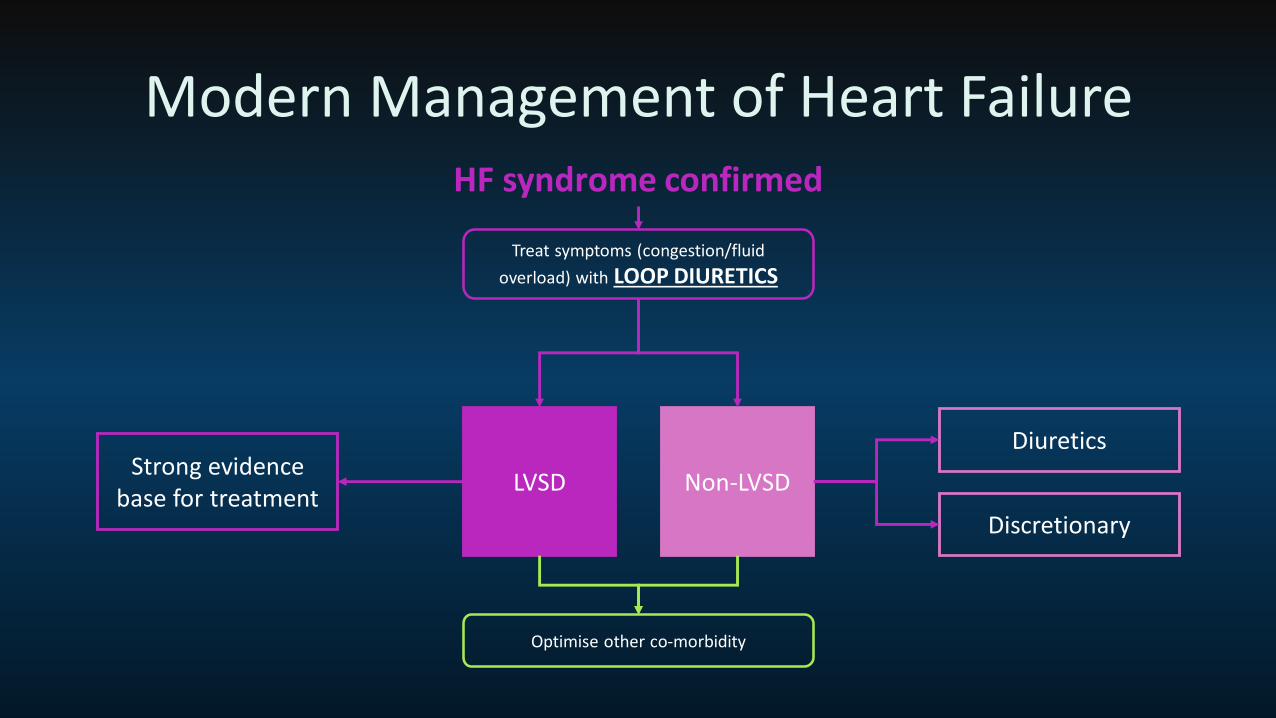
Modern Management of Heart FailureHF syndrome confirmed
Treat symptoms (congestion/fluid
overload) with LOOP DIURETICS
LVSD Non-LVSDStrong evidence
base for treatment
Diuretics
Discretionary
Optimise other co-morbidity
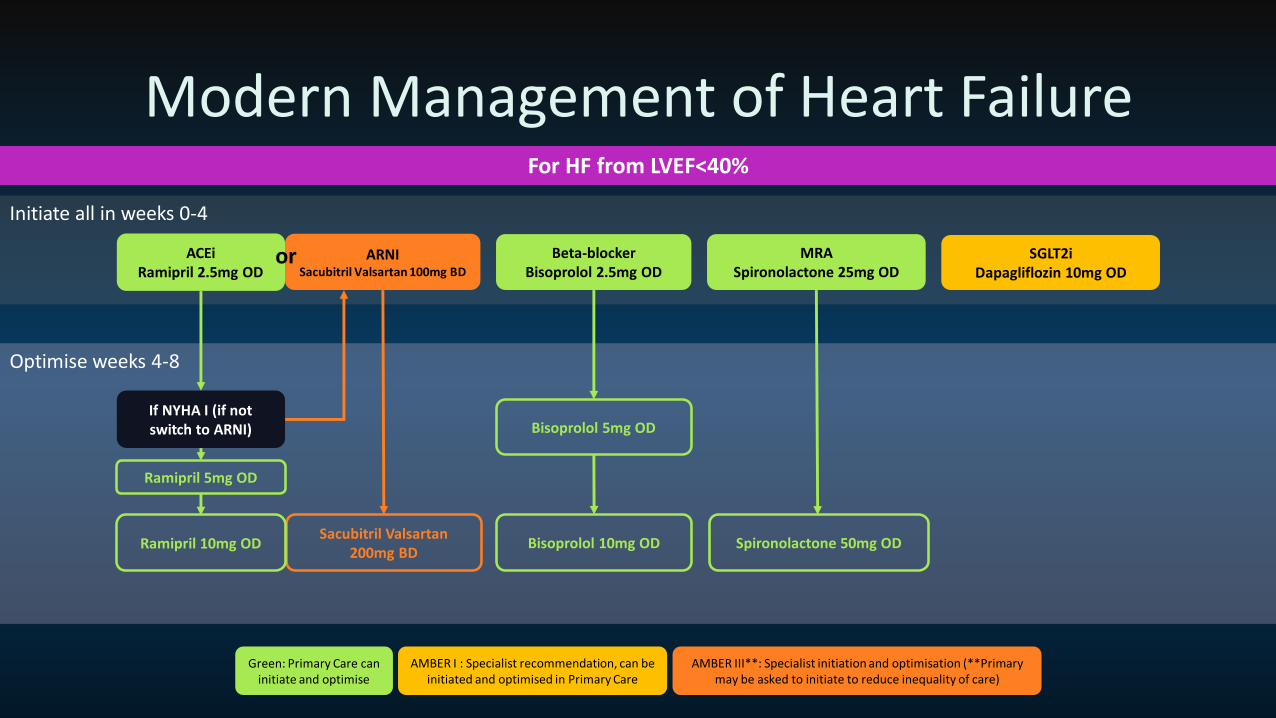
Optimise weeks 4-8
Initiate all in weeks 0-4
Modern Management of Heart FailureFor HF from LVEF<40%
ACEiRamipril 2.5mg OD
Beta-blockerBisoprolol 2.5mg OD
ARNISacubitril Valsartan 100mg BD
or MRASpironolactone 25mg OD
SGLT2iDapagliflozin 10mg OD
Ramipril 5mg OD
Bisoprolol 5mg OD
Sacubitril Valsartan 200mg BD
Spironolactone 50mg OD
If NYHA I (if not switch to ARNI)
Ramipril 10mg OD Bisoprolol 10mg OD
Green: Primary Care can initiate and optimise
AMBER I : Specialist recommendation, can be initiated and optimised in Primary Care
AMBER III**: Specialist initiation and optimisation (**Primary may be asked to initiate to reduce inequality of care)
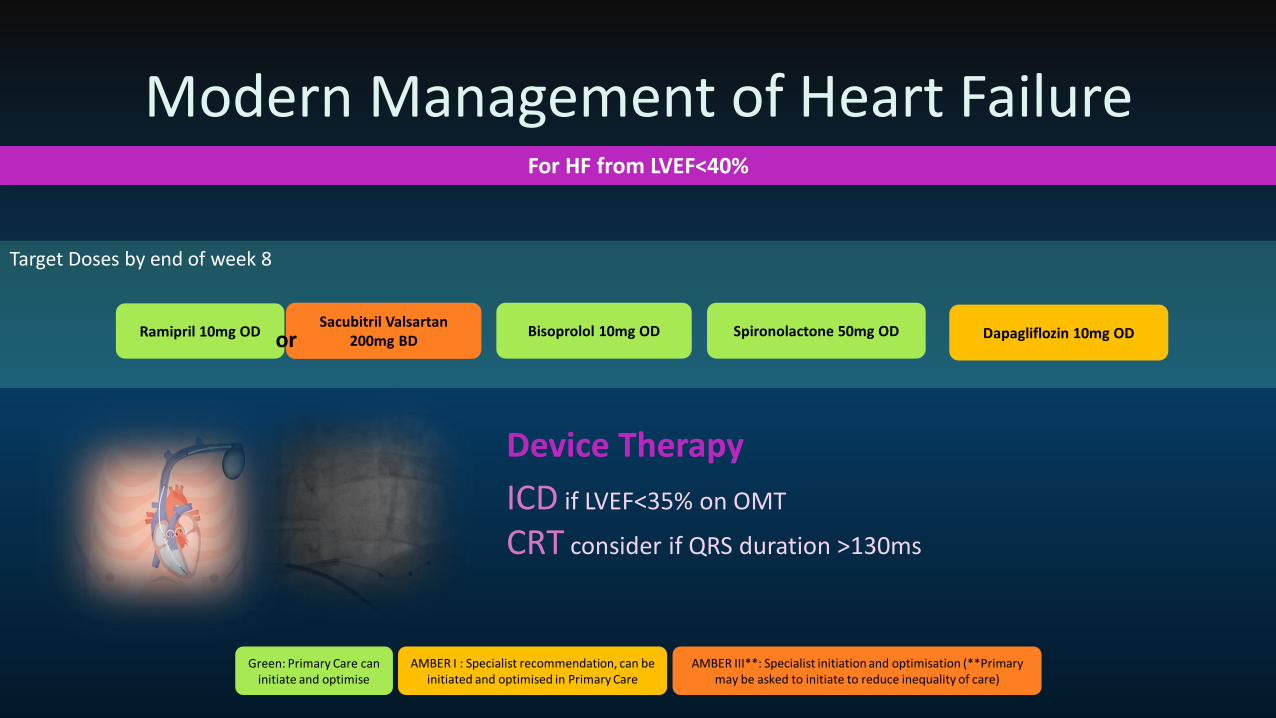
Modern Management of Heart FailureFor HF from LVEF<40%
Target Doses by end of week 8
Sacubitril Valsartan 200mg BD
Spironolactone 50mg ODRamipril 10mg OD Bisoprolol 10mg OD Dapagliflozin 10mg OD
Green: Primary Care can initiate and optimise
AMBER I : Specialist recommendation, can be initiated and optimised in Primary Care
AMBER III**: Specialist initiation and optimisation (**Primary may be asked to initiate to reduce inequality of care)
Device Therapy
ICD if LVEF<35% on OMT
CRT consider if QRS duration >130ms
or
Outline
▪ What is heart failure
▪ Why is it important
▪ Diagnosis
▪ Care in Primary Care
▪ Modern management
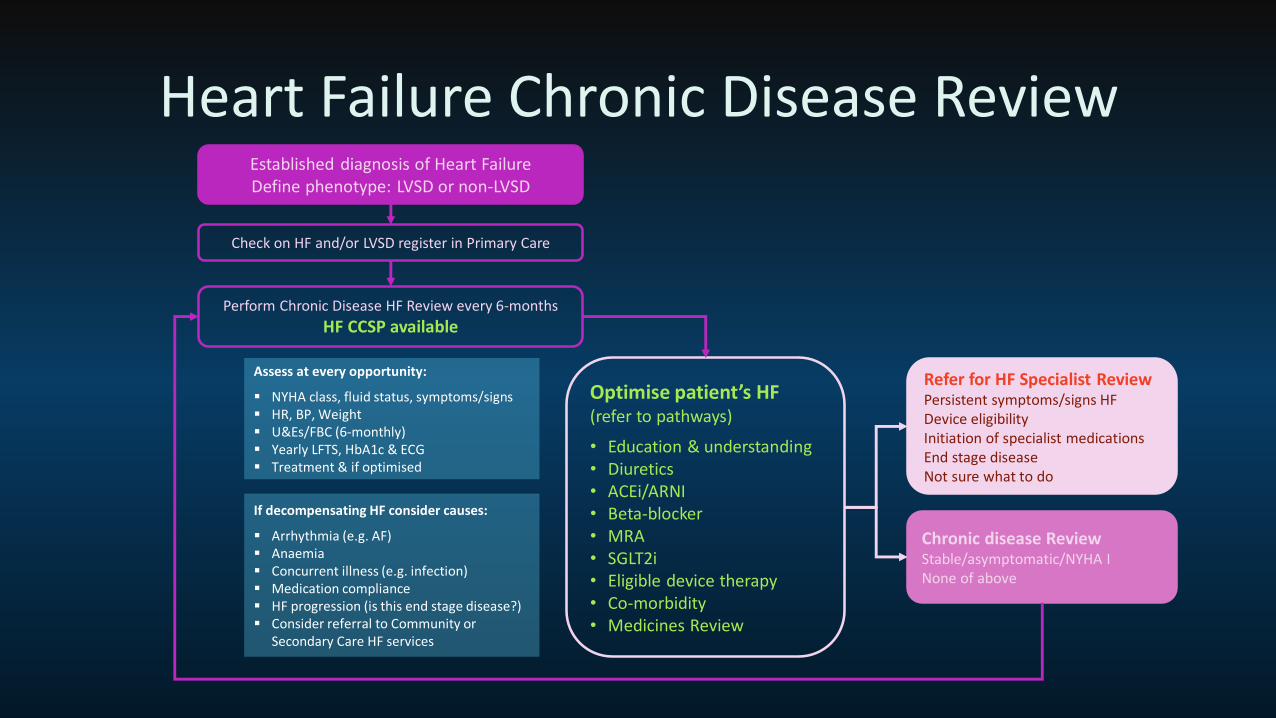
Heart Failure Chronic Disease ReviewEstablished diagnosis of Heart FailureDefine phenotype: LVSD or non-LVSD
Optimise patient’s HF (refer to pathways)
• Education & understanding• Diuretics• ACEi/ARNI• Beta-blocker• MRA• SGLT2i• Eligible device therapy• Co-morbidity• Medicines Review
Chronic disease ReviewStable/asymptomatic/NYHA INone of above
Refer for HF Specialist ReviewPersistent symptoms/signs HFDevice eligibilityInitiation of specialist medicationsEnd stage diseaseNot sure what to do
Perform Chronic Disease HF Review every 6-months
HF CCSP available
Assess at every opportunity:
▪ NYHA class, fluid status, symptoms/signs▪ HR, BP, Weight▪ U&Es/FBC (6-monthly)▪ Yearly LFTS, HbA1c & ECG▪ Treatment & if optimised
If decompensating HF consider causes:
▪ Arrhythmia (e.g. AF)▪ Anaemia▪ Concurrent illness (e.g. infection)▪ Medication compliance▪ HF progression (is this end stage disease?)▪ Consider referral to Community or
Secondary Care HF services
Check on HF and/or LVSD register in Primary Care
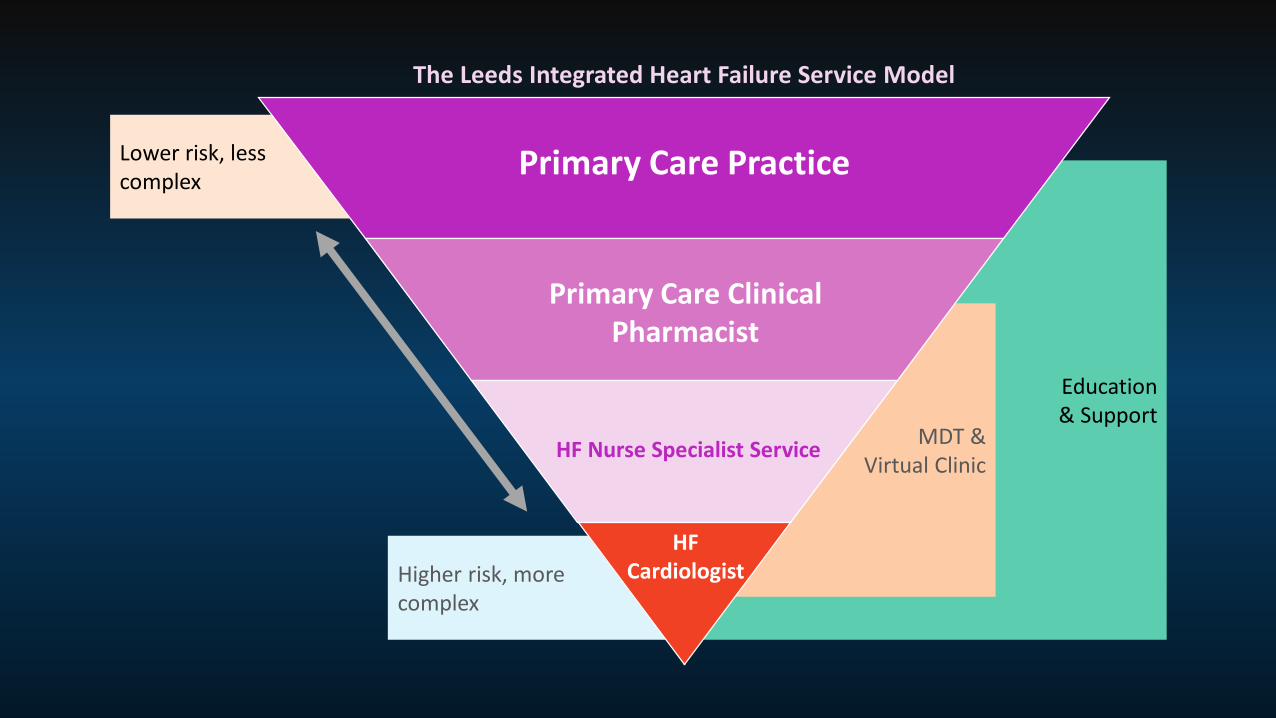
Education & Support
Lower risk, less complex
Higher risk, more complex
MDT & Virtual Clinic
HF Nurse Specialist Service
Primary Care Practice
Primary Care Clinical Pharmacist
HF Cardiologist
The Leeds Integrated Heart Failure Service Model





























