Embed Size (px)
Citation preview

Excellent Clinical Teaching in a Busy Practice:
Make the Most of Your Limited TimeLisa E. Leggio, MD, FAAP
Professor of Pediatrics
Director, Pediatric Student Education
Medical College of Georgia at Augusta University

Disclosures
• I have no disclosures
• All images used in this presentation are my own, in public domain, or marked as not requiring attribution unless otherwise labeled.

OBJECTIVES
Goal: Participants will become better teachers.
By the end of this presentation you will:
1. Ask focused questions to assess knowledge
2. Teach using techniques such as One-Minute Preceptor and SNAPPS
3. Assimilate learners into a busy clinical setting

BACKGROUNDWhy is this important?
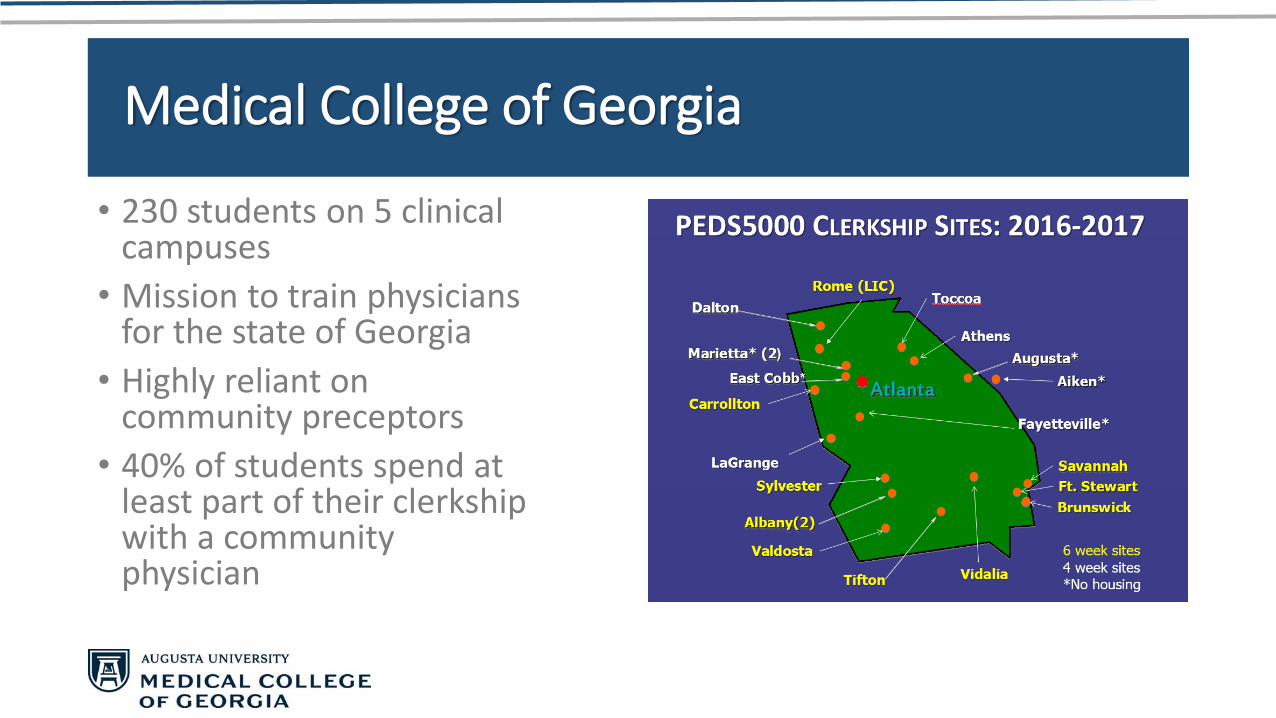
Medical College of Georgia
• 230 students on 5 clinical campuses
• Mission to train physicians for the state of Georgia
• Highly reliant on community preceptors
• 40% of students spend at least part of their clerkship with a community physician
We wear many hats . . .
Takeuchi Seihō [Public domain], via Wikimedia Commons
Balance
Patients
Students

Willliam Osler, MD
"I desire no other epitaph … than the statement that I taught medical students in the wards, as I regard this as by far the most useful and important work I have been called upon to do."

Clinical Teaching
• Teaching in context of ongoing patient care
• Involvement of and teaching about patients
• Diagnose and treat• Patient
• Student
Bannister et al. Pediatrics 2010
HOW MUCH TIME DOES IT TAKE?
• Less Time per Patient • Charting and gathering history
• More Time per Patient: • Listening to presentations and teaching
• Bottom line is about 1 minute per patient or about one hour per day
You can minimize the impact!
Usatine. Acad Med 2000

Time-Efficient Strategies
Planning and
Preparing
TeachingEvaluating
and Reflecting
Ferenchick. Acad Med 1997, Irby. Clin Teach 2004

Plan/PrepareStrategies for Efficient Teaching

Prepare Your Staff
• Involve them in Orientation meetings
• Ask them how students can help
• Listen to their concerns about having a student in the office
• Strategize how to best incorporate a student
• Let them help you• Orient the student
• Maintain patient flow
• Teach the student procedures (vital signs, immunizations, phlebotomy)

How Can Students Help?
• Before visit• Pre-visit planning• Meet patients in hospital prior• Goal-setting before visit• Review social history
• During visit• Help families complete forms• Take patient to room• Document in EHR
• Update problem and med lists• Write/pend orders, Rx• Write notes (ROS, PMH, FH, SH)
• Medication Reconciliation• Patient Education
• After visit• Answer questions from patients• Communicate lab results• Follow-up calls• Help coordinate care
• Other:• Work with front desk/nurse/lab• Work on quality improvement• Create patient handouts• Bookmark patient education sites• Answer clinical questions
www.teachingphysician.org

Wave Scheduling
Ferenchick. Acad Med 1997, Usatine. Acad Med 2000, Lehner. J Physician Assist Educ 2016
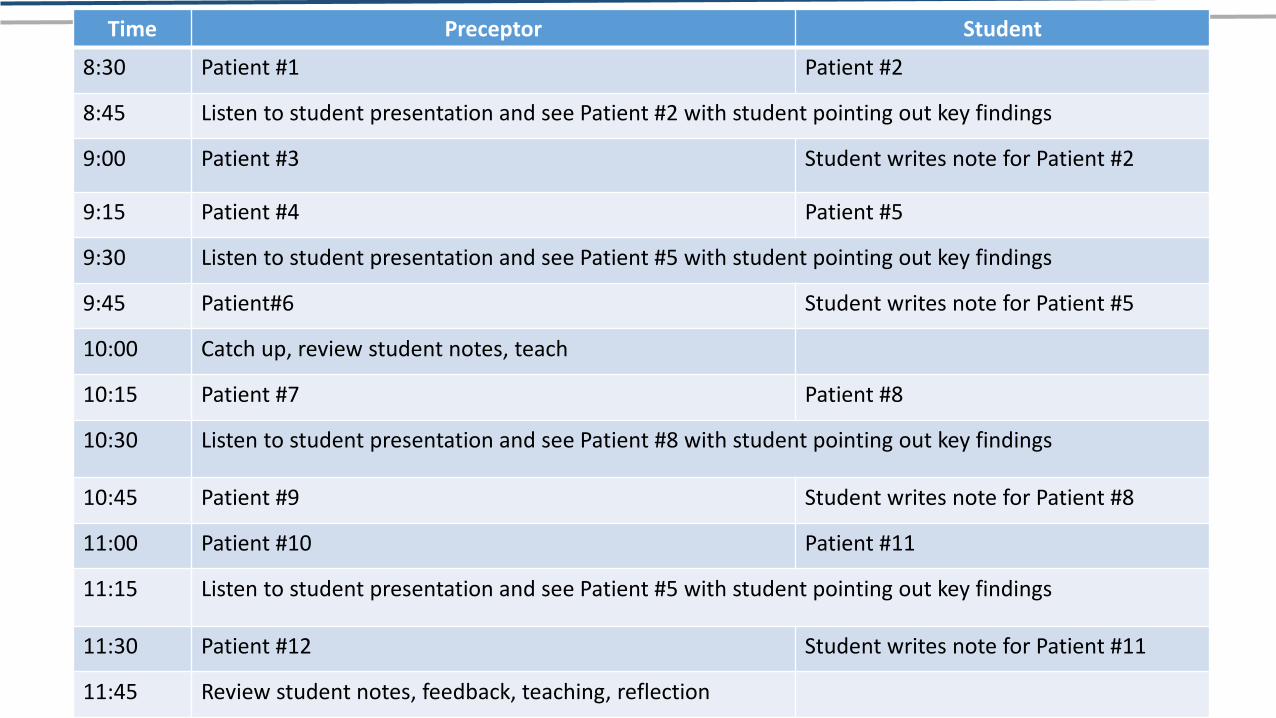
Ferenchick 1997, Usatine 2000
Time Preceptor Student
8:30 Patient #1 Patient #2
8:45 Listen to student presentation and see Patient #2 with student pointing out key findings
9:00 Patient #3 Student writes note for Patient #2
9:15 Patient #4 Patient #5
9:30 Listen to student presentation and see Patient #5 with student pointing out key findings
9:45 Patient#6 Student writes note for Patient #5
10:00 Catch up, review student notes, teach
10:15 Patient #7 Patient #8
10:30 Listen to student presentation and see Patient #8 with student pointing out key findings
10:45 Patient #9 Student writes note for Patient #8
11:00 Patient #10 Patient #11
11:15 Listen to student presentation and see Patient #5 with student pointing out key findings
11:30 Patient #12 Student writes note for Patient #11
11:45 Review student notes, feedback, teaching, reflection

Orient Your Learner

Orientation - Mechanics
Raszka. Pediatrics 2010
Orientation - Mechanics
Raszka. Pediatrics 2010

Orientation - Mechanics
Raszka. Pediatrics 2010
Orientation - Mechanics
Raszka. Pediatrics 2010

Orientation - Process
• Awareness of Goals, Objectives, Competencies
• Awareness of student (rotations done, career goals, learning style)
• Set personally relevant education goals
• Support student’s self-reflections
• Listening to and acting on student requests – conveys respect
• Clearly define expectations and goals
Raszka. Pediatrics 2010

TeachStrategies for Efficient Teaching
WHAT MAKES A GREAT TEACHER
Cognitive
• Knowledgeable
• Clinical Skills
• Organized
• Clear expectations
• Explains concepts
• Communication skills
• Direct supervision
• Gives feedback
Non-Cognitive
• Enthusiastic
• Stimulating
• Professional
• Positive learning environment
• Encouraging
• Focus on student needs
• Listening
Bannister. Pediatrics 2010
Child vs Adult
Child
• Accumulate knowledge and skills that might be useful later in life
• Subject-centered
Adult
• Accumulate knowledge and skills they can apply right away
• Problem-centered or performance-centered
Knowles
ADULT LEARNING THEORY
• Adults will learn what is relevant
• Adults learn better if they are involved in the process
• Adults learn with practice
• Adults need feedback
• Adults need opportunity for reflection
Vella, Learning to Listen, Learning to Teach: The
Power of Dialogue in Educating Adults 2002
FOCUSED QUESTIONS
• Diagnose the learner
• What do you think is going on?
• Why do you think that is so?
• Allows focused teaching
• Don’t waste time telling something they know
• Make your teaching relevant

ONE MINUTE PRECEPTOR
Five Steps
1. Get a commitment
2. Probe for evidence
3. Teach 1-2 points related to the case
4. Reinforce what was done well
5. Correct errors
Examples
1. What do you think is going on?
2. Why do you think that?
3. Whenever you see . . . you should think about . . .
4. You gave good evidence to support your diagnosis
5. In the future, you should avoid . . .
Preceptor driven
Ferenchick. Acad Med 1997, Aagaard. Acad Med 2004, Irby. Acad Med 2004, Bannister. Pediatrics 2011
Problem Representations
• Synthesize the entire patient story into one “big picture” statement.
• Uses semantic qualifiers• Acute/chronic
• Unilateral/bilateral
• Bilious/nonbilious
Fleming. Pediatrics 2012
Problem Representation - Example
A previously healthy 5 week old first-born male presents with non-bilious projectile emesis. He is afebrile, well-appearing, and on exam has an olive-shaped mass in the right upper quadrant.
Fleming. Pediatrics 2012
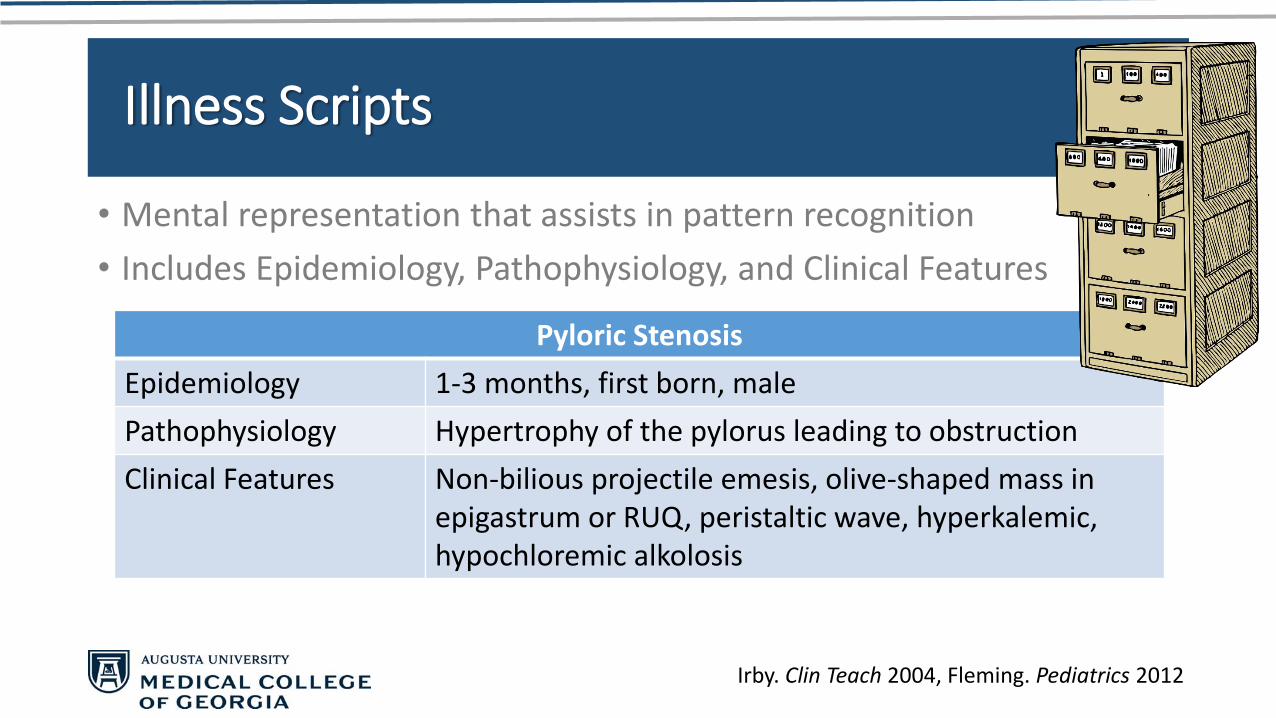
Illness Scripts
• Mental representation that assists in pattern recognition
• Includes Epidemiology, Pathophysiology, and Clinical Features
Irby. Clin Teach 2004, Fleming. Pediatrics 2012
Pyloric Stenosis
Epidemiology 1-3 months, first born, male
Pathophysiology Hypertrophy of the pylorus leading to obstruction
Clinical Features Non-bilious projectile emesis, olive-shaped mass in epigastrum or RUQ, peristaltic wave, hyperkalemic, hypochloremic alkolosis

Teaching Scripts
• 3-5 points with illustrations
• Appreciate common errors learners typically make
• Effective way to help beginners build their own “illness scripts”
Irby. Clin Teach 2004

Horizontal Learning
• Compare several diagnoses side by side to easily see differences
• 3 week old with cough
Pneumococcal PNA Chlamydia PNA Pertussis
Presentation recent URI, fever, grunting, rtxs, flaring, hypoxia
“staccato”; happy tachypneic, h/oconjunctivitis; maternal STI
“paroxysmal”; post-tussive emesis; contactwith chronic cough
Labs Bandemia Eosinophilia Lymphocytosis
CXR findings Lobar Interstitial Interstitial
Treatment Ampicillin Erythromycin Erythromycin
SNAPPS
Steps
1. Summarize the case
2. Narrow the differential
3. Analyze the possibilities
4. Probe the preceptor about uncertainties
5. Plan management for the patient
6. Select case-related issues for self-study (self-directed learning)
Prepare the Student
• Orient everyone
• Cards
• Posters
• Keep track of learning topics
Learner Driven
Bannister. Pediatrics 2011, Wolpaw. Acad Med 2012
Preceptors were “ready to teachat the drop of a question”.
Other Teaching Strategies
• Role model (history, exam, thought process)
• Think aloud as you make decisions
• Make brief handouts of most commonly seen illnesses
• Give mini-lectures to the student on medical topics
• Observe a history and physical exam and give feedback

Evaluate/ReflectStrategies for Efficient Teaching

Evaluate
• Provide feedback
Irby. Clin Teach 2004

FEEDBACK SHOULD BE
• Timely
• Given in an appropriate location
• Descriptive, non-judgmental
• Based on direct observations
• Be formative, use verbs and nouns
• Reinforce what is done right
• Correct errors
• Be given on a regular basis• “Feedback Fridays”
• Specific, Timely, Objective, Plan
• Feedback Video
Gigante. Pediatrics 2011; Ende. JAMA 1983
Ask
Tell
Ask

Evaluate
• Provide feedback
• Specific comments on learner strengths
• Recommendations for improvement
• Referenced to required competencies
Irby. Clin Teach 2004

PRIME+ Model for Evaluation
• Professional – remark on professionalism
• Reporter – history and exam skills, presentations, documentation
• Interpreter – data interpretation, prioritization, diff dx
• Manager – diagnostic/therapeutic plans; procedures; managing time
• Educator – self-directed learning, response to feedback, interpreting literature, teaching others
• + - suggested areas for improvement
Holmes. Pediatrics 2014

PRIME+ Model for Evaluation
• Professional – everyone should be professional
• Reporter – expected level of 2nd year or early 3rd year med students
• Interpreter – expected level of most 3rd year medical students
• Manager – expected for late 3rd year, 4th year, and residents
• Educator – expected for 4th year and residents
• + - suggested areas for improvement

Reflect

Reflect - Learner
• Have the learner reflect on one thing they learned today
• What went well
• What could be done better
Ferenchick. Acad Med 1997, Irby. Clin Teach 2004
Reflect - Teacher
• Take 1 min to identify a teaching approach that was effective or ineffective
• Why was the approach (in)effective?
• What if anything would you do differently next time, and why?
Ferenchick. Acad Med 1997, Irby. Clin Teach 2004

WHAT WHY
Ask the
student to
make a
commitment
or decision
Probe for
evidence to
support the
commitment
or decision
Summarize the
case in a single
sentence
Diagnose the Patient
• Orient the Student to Your Practice / Clinic
• EstablishPerformanceExpectations
• Allow the student to play an active role in patient care
Teach the Learner
Identify a key point of emphasis from
the case
Link the key point of emphasis to a
generalizable, relevant teaching point for the
student to learn, based upon the student’s
learning needs.
&
Provide
feedback for
specific,
observed
behaviors
Reinforce
positive
behaviors
Correct
mistakes or
misconceptions
Diagnose the Learner
Slide used with permission from Christopher B. White, MD
An Efficient & Effective Clinical Teacher

Willliam Osler, MD
"No bubble is so iridescent or floats longer than that blown by the successful teacher."

OBJECTIVES
Goal: Participants will become better teachers.
By the end of this presentation you will:
1. Ask focused questions to assess knowledge
2. Teach using techniques such as One-Minute Preceptor and SNAPPS
3. Assimilate learners into a busy clinical setting

REFERENCES
1. Aagaard E, Teherani A, Irby D. Effectiveness of the One-Minute Preceptor Model for Diagnosing the Patient and the Learner: Proof of Concept. Acad Med 2004 79:1 42-49.
2. Bannister S, Hanson J, Maloney C, and Raszka W. Using the Student Case Presentation to Enhance Diagnostic Reasoning. Pediatrics 2011; 128:2 211-213
3. Bannister S, Raszka W, and Maloney C. What Makes a Great Clinical Teacher in Pediatrics? Lessons Learned From the Literature. Pediatrics 2010; 125:5 863-865
4. Ende J. Feedback in Clinical Medical Education. JAMA 1983; 250: 777-781
5. Ferenchick G, Simpson D, Blackman J, DaRosa D, Dunnington G. Strategies for Efficient and Effective Teaching in the Ambulatory Care Setting. Acad Med 1997. 72: 277-280.
6. Fleming A, Cutrer W, Reimschisel T, and Gigante J. You Too Can Teach Clinical Reasoning. Pediatrics 2012; 130:5 795-797

REFERENCES
7. Gigante J, Dell M and Sharkey A. Getting Beyond “Good Job”: How to Give Effective Feedback. Pediatrics 2011; 127:2 205-207
8. Holmes AV, Peltier CB, Hanson JL, Lopreiato JO. Writing medical student and resident performance evaluations: beyond "performed as expected Pediatrics. 2014 May;133(5):766-8. doi: 10.1542/peds.2014-0418. Epub 2014 Apr 14.
9. Irby D, Aagaard E, Teherani A. Teaching Points Identified by Preceptors Observing One-Minute Preceptor and Traditional Preceptor Encounters. Acad Med 2004; 79: 50-55.
10. Irby D, Bowen J. Time Efficient Strategies for Learning and Performance. Clin Teach 2004; Vol 1: No 1: 23-28.
11. Lehner V, Smith D. Wave Scheduling: Efficient Precepting in the Outpatient Setting. J Physician Assist Educ 2016. 27:4. 200-202.
12. Mutnik A. Ask-Tell-Ask Feedback Process developed at Columbia - Video https://www.youtube.com/watch?v=SYXgMobMU8U

REFERENCES
13. Raszka W, Maloney C, Hanson J. Getting Off to a Good Start: Discussing Goals and Expectations with Medical Students. Pediatrics 2010. 126:2 193-195.
14. Usatine R, Tremoulet T, and Irby D. Time-efficient Preceptors in Ambulatory Care Settings. Acad Med 2000. 75:6 639-642
15. Vella, J. Learning to Listen, Learning to Teach: The Power of Dialogue in Educating Adults. John Wiley and Sons, Inc., 2002
16. Wolpaw TM, Cote L, Papp KK, Bordage G. Student Uncertainties Drive Teaching During Case Presentations: More So with SNAPPS. Acad Med2012; 87: 1210-1217.
17. www.teachingphysician.org/become-a-preceptor/How-Students-Can-Add-Value-to-Your-Office

QUESTIONS?